
The Effect of Epidural Analgesia on Labour and Neonatal and Maternal Outcomes in 1, 2a, 3, and 4a Robson’s Classes: A Propensity Score-Matched Analysis

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Methods
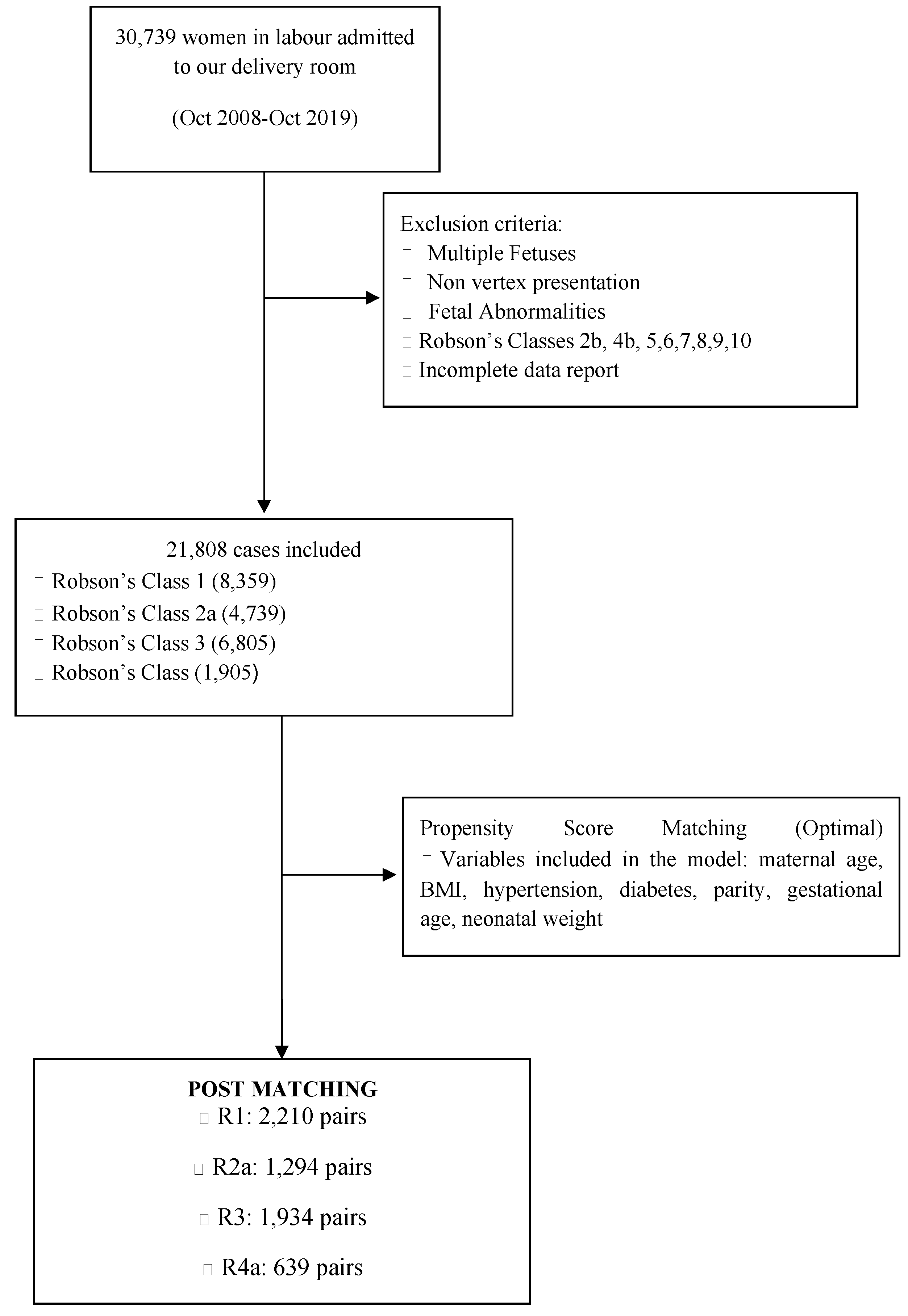
2.1. Study Population
2.2. Data Collection
2.3. Epidural Analgesia Method
2.4. Statistical Analysis
3. Results
3.1. Labour Length
3.2. Neonatal and Maternal Outcomes
4. Discussion
- -
- EA prolongs the second stage of labour in nulliparous and multiparous women with and without labour induction.
- -
- A longer labour length is not correlated with any adverse neonatal outcomes.
- -
- Increases in OVDs are statistically significant among patients who received EA in all four groups.
- -
- There is an increased risk of CS for R2a and R3 patients with EA.
- -
- Episiotomy rates are reduced among nulliparous women with EA, with no statistically significant difference in atony or pelvic laceration rates.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anim-Somuah, M.; Smyth, R.M.; Cyna, A.M.; Cuthbert, A. Epidural versus non-epidural or no analgesia for pain management in labour. Cochrane Database Syst Rev. 2018, 5, CD000331. [Google Scholar] [CrossRef] [PubMed]
- Shmueli, A.; Salman, L.; Orbach-Zinger, S.; Aviram, A.; Hiersch, L.; Chen, R.; Gabbay-Benziv, R. The impact of epidural analgesia on the duration of the second stage of labor. Birth 2018, 45, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.W.; Shaffer, B.L.; Nicholson, J.M.; Caughey, A.B. Second stage of labor and epidural use: A larger effect than previously suggested. Obstet. Gynecol. 2014, 123, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Naito, Y.; Ida, M.; Yamamoto, R.; Tachibana, K.; Kinouchi, K. The effect of labor epidural analgesia on labor, delivery, and neonatal outcomes: A propensity score-matched analysis in a single Japanese institute. JA Clin. Rep. 2019, 5, 40. [Google Scholar] [CrossRef]
- Wang, T.T.; Sun, S.; Huang, S.Q. Effects of Epidural Labor Analgesia with Low Concentrations of Local Anesthetics on Obstetric Outcomes: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Anesth. Analg. 2017, 124, 1571–1580. [Google Scholar] [CrossRef]
- Shen, X.; Li, Y.; Xu, S.; Wang, N.; Fan, S.; Qin, X.; Zhou, C.; Hess, P.E. Epidural Analgesia during the Second Stage of Labor: A Randomized Controlled Trial. Obstet. Gynecol. 2017, 130, 1097–1103. [Google Scholar] [CrossRef]
- The American College of Obstetricians and Gynecologists. Obstetris Care Consensus—Safe prevention of the Primary Cesarean Delivery. Cochrane Database Syst. Rev. 2016, 2, 7. [Google Scholar]
- Zhang, J.; Landy, H.J.; Ware Branch, D.; Burkman, R.; Haberman, S.; Gregory, K.D.; Hatjis, C.G.; Ramirez, M.M.; Bailit, J.L.; Gonzalez-Quintero, V.H.; et al. Contemporary patterns of spontaneous labor with normal neonatal outcomes. Obstet. Gynecol. 2010, 116, 1281–1287. [Google Scholar] [CrossRef] [Green Version]
- Gimovsky, A.C.; Berghella, V. Randomized controlled trial of prolonged second stage: Extending the time limit vs. usual guidelines. Am. J. Obstet. Gynecol. 2016, 214, 361.e1–361.e6. [Google Scholar] [CrossRef] [Green Version]
- Committee on Obstetric Practice. ACOG Committee Opinion No. 766: Approaches to Limit Intervention during Labor and Birth. Obstet. Gynecol. 2019, 133, e164–e173. [Google Scholar] [CrossRef]
- O’Connell, M.P.; Hussain, J.; Maclennan, F.A.; Lindow, S.W. Factors associated with a prolonged second state of labour—A case-controlled study of 364 nulliparous labours. J. Obstet. Gynaecol. 2003, 23, 255–257. [Google Scholar] [CrossRef]
- Carlhall, S.; Kallen, K.; Blomberg, M. Maternal body mass index and duration of labor. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 171, 49–53. [Google Scholar] [CrossRef]
- Bregand-White, J.M.; Kominiarek, M.; Hibbard, J.U.; Consortium on Safe Labor. OS030. Hypertension and labor duration: Does it take longer? Pregnancy Hypertens. 2012, 2, 192. [Google Scholar] [CrossRef]
- Ghi, T.; Maroni, E.; Youssef, A.; Morselli-Labate, A.M.; Paccapelo, A.; Montaguti, E.; Rizzo, N.; Pilu, G. Sonographic pattern of fetal head descent: Relationship with duration of active second stage of labor and occiput position at delivery. Ultrasound Obstet. Gynecol. 2014, 44, 82–89. [Google Scholar] [CrossRef]
- Moraloglu, O.; Kansu-Celik, H.; Tasci, Y.; Karakaya, B.K.; Yilmaz, Y.; Cakir, E.; Yakut, H.I. The influence of different maternal pushing positions on birth outcomes at the second stage of labor in nulliparous women. J. Matern. Fetal Neonatal Med. 2017, 30, 245–249. [Google Scholar] [CrossRef]
- Cheng, Y.W.; Hopkins, L.M.; Laros, R.K., Jr.; Caughey, A.B. Duration of the second stage of labor in multiparous women: Maternal and neonatal outcomes. Am. J. Obstet. Gynecol. 2007, 196, 585.e1–585.e6. [Google Scholar] [CrossRef]
- Gimovsky, A.C.; Guarente, J.; Berghella, V. Prolonged second stage in nulliparous with epidurals: A systematic review. J. Matern. Fetal Neonatal Med. 2017, 30, 461–465. [Google Scholar] [CrossRef]
- Bannister-Tyrrell, M.; Ford, J.B.; Morris, J.M.; Roberts, C.L. Epidural analgesia in labour and risk of caesarean delivery. Paediatr. Perinat. Epidemiol. 2014, 28, 400–411. [Google Scholar] [CrossRef] [Green Version]
- Zha, Y.; Gong, X.; Yang, C.; Deng, D.; Feng, L.; Luo, A.; Wan, L.; Qiao, F.; Zeng, W.; Chen, S.; et al. Epidural analgesia during labor and its optimal initiation time-points: A real-world study on 400 Chinese nulliparas. Medicine 2021, 100, e24923. [Google Scholar] [CrossRef]
- Ravelli, A.C.J.; Eskes, M.; de Groot, C.J.M.; Abu-Hanna, A.; van der Post, J.A.M. Intrapartum epidural analgesia and low Apgar score among singleton infants born at term: A propensity score matched study. Acta Obstet. Gynecol. Scand. 2020, 99, 1155–1162. [Google Scholar] [CrossRef]
- Laughon, S.K.; Berghella, V.; Reddy, U.M.; Sundaram, R.; Lu, Z.; Hoffman, M.K. Neonatal and maternal outcomes with prolonged second stage of labor. Obstet. Gynecol. 2014, 124, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Robson, M.S. Classification of caesarean sections. Fetal Matern. Med. Rev. 2001, 12, 23–39. [Google Scholar] [CrossRef]
- World Health Organization. WHO Statement on Caesarean Section Rates; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Ye, Y.; Song, X.; Liu, L.; Shi, S.Q.; Garfield, R.E.; Zhang, G.; Liu, H. Effects of Patient-Controlled Epidural Analgesia on Uterine Electromyography During Spontaneous Onset of Labor in Term Nulliparous Women. Reprod. Sci. 2015, 22, 1350–1357. [Google Scholar] [CrossRef]
- Wang, Q.; Zheng, S.X.; Ni, Y.F.; Lu, Y.Y.; Zhang, B.; Lian, Q.Q.; Hu, M.P. The effect of labor epidural analgesia on maternal-fetal outcomes: A retrospective cohort study. Arch. Gynecol. Obstet. 2018, 298, 89–96. [Google Scholar] [CrossRef] [PubMed]
- La Camera, G.; La Via, L.; Murabito, P.; Pitino, S.; Dezio, V.; Interlandi, A.; Minardi, C.; Astuto, M. Epidural analgesia during labour and stress markers in the newborn. J. Obstet. Gynaecol. 2021, 41, 690–692. [Google Scholar] [CrossRef]
- de Barros Duarte, L.; Moisés, E.C.; Carvalho Cavalli, R.; Lanchote, V.L.; Duarte, G.; da Cunha, S.P. Distribution of fentanyl in the placental intervillous space and in the different maternal and fetal compartments in term pregnant women. Eur. J. Clin. Pharmacol. 2009, 65, 803–808. [Google Scholar] [CrossRef]
- Zhang, L.; Xu, C.; Li, Y. Impact of epidural labor analgesia using sufentanil combined with low-concentration ropivacaine on maternal and neonatal outcomes: A retrospective cohort study. BMC Anesthesiol. 2021, 21, 229. [Google Scholar] [CrossRef]
- Antonakou, A.; Papoutsis, D. The Effect of Epidural Analgesia on the Delivery Outcome of Induced Labour: A Retrospective Case Series. Obstet. Gynecol. Int. 2016, 2016, 5740534. [Google Scholar] [CrossRef]
- Srebnik, N.; Barkan, O.; Rottenstreich, M.; Ioscovich, A.; Farkash, R.; Rotshenker-Olshinka, K.; Samueloff, A.; Grisaru-Granovsky, S. The impact of epidural analgesia on the mode of delivery in nulliparous women that attain the second stage of labor. J. Matern. Fetal Neonatal Med. 2020, 33, 2451–2458. [Google Scholar] [CrossRef]
- Simic, M.; Cnattingius, S.; Petersson, G.; Sandström, A.; Stephansson, O. Duration of second stage of labor and instrumental delivery as risk factors for severe perineal lacerations: Population-based study. BMC Pregnancy Childbirth 2017, 17, 72. [Google Scholar] [CrossRef] [Green Version]
- MacDougall, M.; Waugh, J.; Morland, D. Epidural analgesia may be protective against third and fourth degree perineal trauma. Arch. Dis. Child. Fetal Neonatal 2011, 96, Fa75. [Google Scholar] [CrossRef]
- Fritel, X.; Schaal, J.P.; Fauconnier, A.; Bertrand, V.; Levet, C.; Pigné, A. Pelvic floor disorders 4 years after first delivery: A comparative study of restrictive versus systematic episiotomy. BJOG 2008, 115, 247–252. [Google Scholar] [CrossRef] [Green Version]
- Webb, D.A.; Culhane, J. Hospital variation in episiotomy use and the risk of perineal trauma during childbirth. Birth 2002, 29, 132–136. [Google Scholar] [CrossRef]


{kind=link}
| Robson 1 | Robson 2a | Robson 3 | Robson 4a | |||||
|---|---|---|---|---|---|---|---|---|
| EA (n = 5226) | NEA (n = 3133) | EA (n= 2996) | NEA (n= 1743) | EA (n = 2612) | NEA (n = 4193) | EA (n = 791) | NEA (n = 1114) | |
| Maternal age (years) | 32 ± 5 | 30 ± 6 | 33 ± 5 | 31 ± 5 | 34 ± 4 | 33 ± 5 | 35 ± 5 | 34 ± 5 |
| BMI (kg/m2) | 22 ± 3.6 | 22.3 ± 4.1 | 22.9 ± 4.3 | 23.4 ± 4.9 | 22.6 ± 3.6 | 23 ± 4.1 | 23.8 ± 5.2 | 24.1 ± 5.1 |
| Parity (n) | 0 | 0 | 0 | 0 | 1.2 ± 0.5 | 1.4 ± 0.9 | 1.2 ± 0.5 | 1.3 ± 0.7 |
| Gravidity (n) | 1.3 ± 0.6 | 1.3 ± 0.7 | 1.3 ± 0.7 | 1.3 ± 0.7 | 2.6 ± 1 | 2.9 ± 1.3 | 2.7 ± 1 | 2.9 ± 1.3 |
| Foetal weight (g) | 3287 ± 380 | 3227 ± 416 | 3284 ± 423 | 3209 ± 451 | 3410 ± 407 | 3370 ± 429 | 3385 ± 446 | 3315 ± 464 |
| Gestational age (week) | 40.3 ± 1.1 | 40.1 ± 1.1 | 40.1 ± 1.2 | 40.1 ± 1.2 | 40.2 ± 1 | 40.1 ± 1.1 | 40.1 ± 1.2 | 40 ± 1.2 |
| Hypertension | 95 (1.8) | 69 (2.2) | 183 (6.1) | 125 (7.2) | 30 (1.1) | 73 (1.7) | 55 (7) | 90 (8.1) |
| Diabetes | 260 (5) | 186 (5.9) | 429 (14.3) | 297 (17) | 111 (4.2) | 252 (6) | 152 (19.2) | 213 (19.1) |
| Robson 1 (2210 Pairs) | Robson 2a (1294 Pairs) | Robson 3 (1934 Pairs) | Robson 4a (639 Pairs) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EA | NEA | p-Value | EA | NEA | p-Value | EA | NEA | p-Value | EA | NEA | p-Value | |
| Stage I, active phase (min) | 213 ± 143 | 137 ± 128 | <0.001 | 205 ± 154 | 141 ± 141 | <0.001 | 129 ± 90 | 84 ± 83 | <0.001 | 120 ± 95 | 87 ± 86 | <0.001 |
| Stage II (min) | 77 ± 59 | 55 ± 49 | <0.001 | 85 ± 63 | 55 ± 49 | <0.001 | 32 ± 30 | 22 ± 18 | <0.001 | 34 ± 35 | 20 ± 21 | <0.001 |
| Robson 1 (n= 2210 Pairs) | Robson 2a (n = 1294) | Robson 3 (n = 1934) | Robson 4a (n = 639) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EA | NEA | p-Value | EA | NEA | p-Value | EA | NEA | p-Value | EA | NEA | p-Value | |
| Apgar 1 min < 7 | 52 (2.4) | 34 (1.5) | 0.064 | 27 (2.1) | 37 (2.9) | 0.255 | 20 (1) | 24 (1.2) | 0.649 | 8 (1.3) | 8 (1.3) | >0.999 |
| Apgar 5 min < 7 | 4 (0.2) | 7 (0.3) | 0.548 # | 1 (0.1) | 9 (0.7) | 0.021 * | 3 (0.2) | 2 (0.1) | >0.999 # | 0 (0) | 5 (0.8) | 0.062 # |
| Resuscitation | 53 (2.4) | 53 (2.4) | >0.999 | 31 (2.4) | 27 (2.1) | 0.69 | 22 (1.1) | 34 (1.8) | 0.139 | 10 (1.6) | 13 (2) | 0.674 |
| Robson 1 (n = 2210 Pairs) | Robson 2a (n = 1294) | Robson 3 (n = 1934) | Robson 4a (n = 639) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EA | NEA | p-Value | EA | NEA | p-Value | EA | NEA | p-Value | EA | NEA | p-Value | |
| Uterine atony | 121 (5.5) | 142 (6.4) | 0.203 | 102 (7.9) | 117 (9) | 0.323 | 78 (4) | 98 (5.1) | 0.143 | 47 (7.4) | 49 (7.6) | 0.915 |
| III–IV laceration | 11 (0.5) | 11 (0.5) | 1 | 6 (0.5) | 11 (0.9) | 0.33 | 3 (0.2) | 4 (0.2) | 1 # | 2 (0.3) | 2 (0.3) | 1 # |
| Episiotomy | 1227 (55.5) | 1352 (61.2) | <0.001 | 655 (50.6) | 736 (56.9) | 0.002 | 753 (38.9) | 806 (41.7) | 0.088 | 221 (0.3) | 228 (35.7) | 0.725 |
| Caesarean section | 47 (2.1) | 42 (1.9) | 0.668 | 46 (3.6) | 28 (2.2) | 0.045 | 12 (0.6) | 2 (0.1) | 0.013 # | 8 (1.3) | 3 (0.5) | 0.225 # |
| Operative vaginal delivery | 293 (13.3) | 151 (6.8) | <0.001 | 201 (15.5) | 117 (9) | <0.001 | 33 (1.7) | 30 (1.6) | 0.783 | 18 (2.8) | 11 (1.7) | 0.251 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanfini, B.A.; Catarci, S.; Vassalli, F.; Laurita Longo, V.; Biancone, M.; Carducci, B.; Frassanito, L.; Lanzone, A.; Draisci, G. The Effect of Epidural Analgesia on Labour and Neonatal and Maternal Outcomes in 1, 2a, 3, and 4a Robson’s Classes: A Propensity Score-Matched Analysis. J. Clin. Med. 2022, 11, 6124. https://doi.org/10.3390/jcm11206124
Zanfini BA, Catarci S, Vassalli F, Laurita Longo V, Biancone M, Carducci B, Frassanito L, Lanzone A, Draisci G. The Effect of Epidural Analgesia on Labour and Neonatal and Maternal Outcomes in 1, 2a, 3, and 4a Robson’s Classes: A Propensity Score-Matched Analysis. Journal of Clinical Medicine. 2022; 11(20):6124. https://doi.org/10.3390/jcm11206124
Chicago/Turabian StyleZanfini, Bruno Antonio, Stefano Catarci, Francesco Vassalli, Valentina Laurita Longo, Matteo Biancone, Brigida Carducci, Luciano Frassanito, Antonio Lanzone, and Gaetano Draisci. 2022. "The Effect of Epidural Analgesia on Labour and Neonatal and Maternal Outcomes in 1, 2a, 3, and 4a Robson’s Classes: A Propensity Score-Matched Analysis" Journal of Clinical Medicine 11, no. 20: 6124. https://doi.org/10.3390/jcm11206124
APA StyleZanfini, B. A., Catarci, S., Vassalli, F., Laurita Longo, V., Biancone, M., Carducci, B., Frassanito, L., Lanzone, A., & Draisci, G. (2022). The Effect of Epidural Analgesia on Labour and Neonatal and Maternal Outcomes in 1, 2a, 3, and 4a Robson’s Classes: A Propensity Score-Matched Analysis. Journal of Clinical Medicine, 11(20), 6124. https://doi.org/10.3390/jcm11206124