

The Impact of Overweight and Obesity on Reduced-Port Laparoscopic Distal Gastrectomy for Gastric Cancer Patients: A Propensity Score Matching Analysis of a Single-Institution Data

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Data Collection and Definition
2.3. Surgical Technique
2.4. PSM
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Operative Results
3.3. Hospital Course and Postoperative Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Viñuela, E.F.; Gonen, M.; Brennan, M.F.; Coit, D.G.; Strong, V.E. Laparoscopic versus open distal gastrectomy for gastric cancer: A meta-analysis of randomized controlled trials and high-quality nonrandomized studies. Ann. Surg. 2012, 255, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Takiguchi, S.; Fujiwara, Y.; Yamasaki, M.; Miyata, H.; Nakajima, K.; Sekimoto, M.; Mori, M.; Doki, Y. Laparoscopy-assisted distal gastrectomy versus open distal gastrectomy. A prospective randomized single-blind study. World J. Surg. 2013, 37, 2379–2386. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Ha, M.H.; Seo, J.E.; Kim, J.E.; Choi, M.G.; Sohn, T.S.; Bae, J.M.; Kim, S.; Lee, J.H. Comparison of Reduced Port Totally Laparoscopic Distal Gastrectomy (Duet TLDG) and Conventional Laparoscopic-Assisted Distal Gastrectomy. Ann. Surg. Oncol. 2015, 22, 2567–2572. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.G.; Kim, D.Y.; Jeong, O. Transition from Conventional to Reduced-Port Laparoscopic Gastrectomy to Treat Gastric Carcinoma: A Single Surgeon’s Experience from a Small-Volume Center. J. Gastric Cancer 2018, 18, 172–181. [Google Scholar] [CrossRef]
- Kunisaki, C.; Makino, H.; Yamaguchi, N.; Izumisawa, Y.; Miyamato, H.; Sato, K.; Hayashi, T.; Sugano, N.; Suzuki, Y.; Ota, M.; et al. Surgical advantages of reduced-port laparoscopic gastrectomy in gastric cancer. Surg. Endosc. 2016, 30, 5520–5528. [Google Scholar] [CrossRef]
- Kim, S.M.; Ha, M.H.; Seo, J.E.; Kim, J.E.; Choi, M.G.; Sohn, T.S.; Bae, J.M.; Kim, S.; Lee, J.H. Comparison of single-port and reduced-port totally laparoscopic distal gastrectomy for patients with early gastric cancer. Surg. Endosc. 2016, 30, 3950–3957. [Google Scholar] [CrossRef]
- Kunisaki, C.; Miyamoto, H.; Sato, S.; Tanaka, Y.; Sato, K.; Izumisawa, Y.; Yukawa, N.; Kosaka, T.; Akiyama, H.; Saigusa, Y.; et al. Surgical Outcomes of Reduced-Port Laparoscopic Gastrectomy Versus Conventional Laparoscopic Gastrectomy for Gastric Cancer: A Propensity-Matched Retrospective Cohort Study. Ann. Surg. Oncol. 2018, 25, 3604–3612. [Google Scholar] [CrossRef]
- Lee, H.H.; Jeong, O.; Seo, H.S.; Choi, M.G.; Ryu, S.Y.; Sohn, T.S.; Bae, J.M.; Kim, S.; Lee, J.H. Long-Term Oncological Outcomes of Reduced Three-Port Laparoscopic Gastrectomy for Early-Stage Gastric Carcinoma: A Retrospective Large-Scale Multi-Institutional Study. J. Gastric Cancer 2021, 21, 93–102. [Google Scholar] [CrossRef]
- Yamada, H.; Kojima, K.; Inokuchi, M.; Kawano, T.; Sugihara, K. Effect of obesity on technical feasibility and postoperative outcomes of laparoscopy-assisted distal gastrectomy—Comparison with open distal gastrectomy. J. Gastrointest. Surg. 2008, 12, 997–1004. [Google Scholar] [CrossRef]
- Yasuda, K.; Inomata, M.; Shiraishi, N.; Izumi, K.; Ishikawa, K.; Kitano, S. Laparoscopy-assisted distal gastrectomy for early gastric cancer in obese and nonobese patients. Surg. Endosc. 2004, 18, 1253–1256. [Google Scholar] [CrossRef]
- Inagawa, S.; Adachi, S.; Oda, T.; Kawamoto, T.; Koike, N.; Fukao, K. Effect of fat volume on postoperative complications and survival rate after D2 dissection for gastric cancer. Gastric Cancer 2000, 3, 141–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer 2017, 20, 113–153. [Google Scholar] [CrossRef] [Green Version]
- Mayhew, D.; Mendonca, V.; Murthy, B.V.S. A review of ASA physical status—Historical perspectives and modern developments. Anaesthesia 2019, 74, 373–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, S.E.; Seo, J.E.; An, J.Y.; Choi, M.G.; Sohn, T.S.; Bae, J.M.; Kim, S.; Lee, J.H. Compliance with D2 lymph node dissection in reduced-port totally laparoscopic distal gastrectomy in patients with gastric cancer. Sci. Rep. 2021, 11, 3658. [Google Scholar] [CrossRef]
- Kang, D.Y.; Kim, H.G.; Kim, D.Y. Reduced-port laparoscopic distal gastrectomy in obese gastric cancer patients. PLoS ONE 2021, 16, e0255855. [Google Scholar] [CrossRef]
- Noshiro, H.; Shimizu, S.; Nagai, E.; Ohuchida, K.; Tanaka, M. Laparoscopy-assisted distal gastrectomy for early gastric cancer: Is it beneficial for patients of heavier weight? Ann. Surg. 2003, 238, 680–685. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, M.; Kinoshita, T.; Shibasaki, H.; Kato, Y.; Gotohda, N.; Takahashi, S.; Konishi, M. Short-term outcome of total laparoscopic distal gastrectomy for overweight and obese patients with gastric cancer. Surg. Endosc. 2013, 27, 4291–4296. [Google Scholar] [CrossRef]
- Chen, K.; Pan, Y.; Zhai, S.-T.; Cai, J.-Q.; Chen, Q.-L.; Chen, D.-W.; Zhu, Y.-P.; Zhang, Y.; Zhang, Y.-P.; Maher, H.; et al. Laparoscopic gastrectomy in obese gastric cancer patients: A comparative study with non-obese patients and evaluation of difference in laparoscopic methods. BMC Gastroenterol. 2017, 17, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Japanese Gastric Cancer, A. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer 2011, 14, 101–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, D.J.; Lee, E.J.; Kim, G.Y. Evaluation of Reduced Port Laparoscopic Distal Gastrectomy Performed by a Novice Surgeon. J. Gastric Cancer 2021, 21, 179–190. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total Set (n = 211) | PSM Set (n = 136) | |||||
|---|---|---|---|---|---|---|
| NOG (n = 143) | OG (n = 68) | p-Value | NOG (n = 68) | OG (n = 68) | p-Value | |
| Body mass index (kg/m2) | 22.07 ± 2.00 | 27.85 ± 2.75 | <0.001 | 21.97 ± 2.11 | 27.85 ± 2.75 | <0.001 |
| Age (years) | 66.18 ± 11.11 | 62.85 ± 11.03 | 0.043 | 63.21 ± 10.88 | 62.85 ± 11.03 | 0.851 |
| Sex (male) | 101 (70.6) | 47 (69.1) | 0.823 | 49 (72.1) | 47 (69.1) | 0.707 |
| Abdominal surgery history | 11 (7.7) | 7 (10.3) | 0.527 | 6 (8.8) | 7 (10.3) | 0.771 |
| Comorbidity | 78 (54.6) | 50 (73.5) | 0.008 | 52 (76.5) | 50 (73.5) | 0.692 |
| Hypertension | 51 (35.7) | 38 (55.9) | 0.005 | 40 (58.8) | 38 (55.9) | 0.729 |
| Diabetes mellitus | 28 (19.6) | 16 (23.5) | 0.509 | 15 (22.1) | 16 (23.5) | 0.838 |
| Ischemic heart disease | 6 (4.2) | 5 (7.4) | 0.335 | 4 (5.9) | 5 (7.4) | 0.73 |
| Obstructive pulmonary disease | 8 (5.6) | 2 (2.9) | 0.397 | 2 (2.9) | 2 (2.9) | 1 |
| Cerebrovascular disease | 4 (2.8) | 0 (0.0) | 0.164 | 2 (2.9) | 0 (0.0) | 0.154 |
| Liver cirrhosis | 2 (1.4) | 1 (1.5) | 0.967 | 1 (1.5) | 1 (1.5) | 1 |
| Renal disease | 1 (0.7) | 1 (1.5) | 0.589 | 1 (1.5) | 1 (1.5) | 1 |
| ASA score | <0.001 | 0.568 | ||||
| 1 | 75 (52.4) | 13 (19.1) | 17 (25.0) | 13 (19.1) | ||
| 2 | 62 (43.4) | 51 (75.0) | 45 (66.2) | 51 (75.0) | ||
| 3 | 5 (3.5) | 4 (5.9) | 5 (7.3) | 4 (5.9) | ||
| 4 | 1 (0.7) | 0 (0.0) | 1 (1.5) | 0 (0.0) | ||
| Tumor size (mm) | 22.10 ± 22.53 | 21.43 ± 9.17 | 0.15 | 20.54 ± 12.30 | 21.43 ± 9.17 | 0.282 |
| Histological grade | 0.793 | 0.72 | ||||
| Differentiated | 92 (64.3) | 45 (66.2) | 43 (63.2) | 45 (66.2) | ||
| Undifferentiated | 51 (35.7) | 23 (33.8) | 25 (36.8) | 23 (33.8) | ||
| Lymphovascular invasion | 11 (7.7) | 3 (4.4) | 0.371 | 5 (7.4) | 3 (4.4) | 0.466 |
| Perineural invasion | 7 (4.9) | 3 (4.4) | 0.877 | 3 (4.4) | 3 (4.4) | 1 |
| Depth of invasion | 0.73 | 0.799 | ||||
| pTis | 3 (2.1) | 2 (2.9) | 2 (2.9) | 2 (2.9) | ||
| pT1 | 130 (90.9) | 64 (94.1) | 63 (92.7) | 64 (94.1) | ||
| pT2 | 7 (4.9) | 2 (2.9) | 2 (2.9) | 2 (2.9) | ||
| pT3 | 1 (0.7) | 0 (0.0) | 1 (1.5) | 0 (0.0) | ||
| pT4 | 2 (1.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Nodal metastasis | 0.46 | 0.242 | ||||
| pN0 | 129 (90.2) | 63 (92.7) | 60 (88.2) | 63 (92.7) | ||
| pN1 | 11 (7.7) | 2 (2.9) | 7 (10.3) | 2 (2.9) | ||
| pN2 | 1 (0.7) | 1 (1.5) | 0 (0.0) | 1 (1.5) | ||
| pN3 | 2 (1.4) | 2 (2.9) | 1 (1.5) | 2 (2.9) | ||
| Total Set (n = 211) | PSM Set (n = 136) | |||||
|---|---|---|---|---|---|---|
| NOG (n = 143) | OG (n = 68) | p-Value | NOG (n = 68) | OG (n = 68) | p-Value | |
| Operation time (min) | 199.51 ± 39.71 | 208.68 ± 29.15 | 0.014 | 200.59 ± 40.39 | 208.68 ± 29.15 | 0.044 |
| Estimated bleeding volume (mL) | 42.59 ± 37.04 | 58.01 ± 45.82 | <0.001 | 40.96 ± 35.40 | 58.01 ± 45.82 | 0.001 |
| Approach | 0.081 | 0.259 | ||||
| Intracorporeal | 120 (83.9) | 63 (92.7) | 59 (86.8) | 63 (92.7) | ||
| Extracorporeal | 23 (16.1) | 5 (7.3) | 9 (13.2) | 5 (7.3) | ||
| Reconstruction | 0.06 | 0.13 | ||||
| Billroth I | 18 (12.6) | 2 (2.9) | 8 (11.8) | 2 (2.9) | ||
| Billroth II | 118 (82.5) | 61 (89.7) | 57 (83.8) | 61 (89.7) | ||
| Roux-en-Y | 7 (4.9) | 5 (7.4) | 3 (4.4) | 5 (7.4) | ||
| Nodal dissection | 0.172 | 0.167 | ||||
| D1+ | 74 (51.8) | 42 (61.8) | 34 (50.0) | 42 (61.8) | ||
| D2 | 69 (48.2) | 26 (38.2) | 34 (50.0) | 26 (38.2) | ||
| No. harvested lymph nodes | 39.13 ± 15.88 | 32.13 ± 16.59 | 0.027 | 36.81 ± 16.45 | 32.13 ± 16.59 | 0.039 |
| No. metastatic lymph nodes | 0.40 ± 2.13 | 0.59 ± 2.99 | 0.607 | 0.41 ± 2.10 | 0.59 ± 2.99 | 0.425 |
| Omentectomy | 0.511 | 0.645 | ||||
| Complete | 130 (90.9) | 63 (92.7) | 61 (89.7) | 63 (92.7) | ||
| Bursectomy | 4 (2.8) | 3 (4.4) | 2 (2.9) | 3 (4.4) | ||
| Partial | 9 (6.3) | 2 (2.9) | 5 (7.4) | 2 (2.9) | ||
| Proximal margin (mm) | 53.03 ± 34.30 | 58.53 ± 89.44 | 0.662 | 57.28 ± 35.40 | 58.53 ± 89.44 | 0.205 |
| Distal margin (mm) | 54.98 ± 29.71 | 72.38 ± 63.05 | 0.158 | 54.81 ± 31.13 | 72.38 ± 63.05 | 0.176 |
| Total Set (n = 211) | PSM Set (n = 136) | |||||
|---|---|---|---|---|---|---|
| NOG (n = 143) | OG (n = 68) | p-Value | NOG (n = 68) | OG (n = 68) | p-Value | |
| Time to first flatus (d) | 3.13 ± 0.95 | 3.07 ± 0.89 | 0.666 | 3.04 ± 0.89 | 3.07 ± 0.89 | 0.847 |
| Time to diet resumption (d) | 1.99 ± 0.19 | 2.06 ± 0.49 | 0.4 | 2.01 ± 0.12 | 2.06 ± 0.49 | 0.992 |
| Length of hospital stay (d) | 7.87 ± 3.60 | 8.15 ± 4.83 | 0.895 | 7.79 ± 3.80 | 8.15 ± 4.83 | 0.824 |
| Fever | 11 (7.7) | 9 (13.2) | 0.199 | 6 (8.8) | 9 (13.2) | 0.412 |
| Transfusion | 2 (1.4) | 1 (1.5) | 1 | 2 (2.9) | 1 (1.5) | 1 |
| Severity of medical complication | 3 (2.1) | 2 (2.9) | 0.658 | 2 (2.9) | 2 (2.9) | 1 |
| Mild | 1 (0.7) | 0 (0.0) | 1 (1.5) | 0 (0.0) | ||
| moderate | 1 (0.7) | 2 (2.9) | 1 (1.5) | 2 (2.9) | ||
| Severe | 1 (0.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Severity of surgical complication | 19 (13.3) | 9 (13.2) | 0.992 | 9 (13.2) | 9 (13.2) | 1 |
| mild | 16 (11.2) | 5 (7.3) | 7 (10.2) | 5 (7.3) | ||
| moderate | 1 (0.7) | 3 (4.4) | 1 (1.5) | 3 (4.4) | ||
| severe | 1 (0.7) | 1 (1.5) | 1 (1.5) | 1 (1.5) | ||
| Total Set (n = 211) | PSM Set (n = 136) | |||||
|---|---|---|---|---|---|---|
| NOG (n = 143) | OG (n = 68) | p-Value | NOG (n = 68) | OG (n = 68) | p-Value | |
| Clavien-Dindo grade | 0.117 | 0.592 | ||||
| I | 17 (11.9) | 5 (7.3) | 8 (11.8) | 5 (7.3) | ||
| II | 2 (1.4) | 5 (7.3) | 2 (2.9) | 5 (7.3) | ||
| III | 2 (1.4) | 1 (1.5) | 1 (1.5) | 1 (1.5) | ||
| IV | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Medical complications | 0.100 | 0.333 | ||||
| Cardiovascular | 0 (0.0) | 1 (1.5) | 0 (0.0) | 1 (1.5) | ||
| Pulmonary | 3 (2.1) | 0 (0.0) | 2 (2.9) | 0 (0.0) | ||
| Renal | 0 (0.0) | 1 (1.5) | 0 (0.0) | 1 (1.5) | ||
| Surgical complications | 0.822 | 0.772 | ||||
| Ascites (Lymphorrhea) | 1 (0.7) | 2 (2.9) | 1 (1.5) | 2 (2.9) | ||
| Chyle leakage | 1 (0.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Gastric stasis | 5 (3.5) | 1 (1.5) | 1 (1.5) | 1 (1.5) | ||
| Ileus | 6 (4.2) | 4 (5.9) | 5 (7.3) | 4 (5.9) | ||
| Intraabdominal infection | 3 (2.1) | 2 (2.9) | 0 (0.0) | 2 (2.9) | ||
| Pancreatitis | 1 (0.7) | 0 (0.0) | 1 (1.5) | 0 (0.0) | ||
| Wound infection | 1 (0.7) | 0 (0.0) | 1 (1.5) | 0 (0.0) | ||
| Total | 21 (14.7) | 11 (16.2) | 0.778 | 11 (16.2) | 11 (16.2) | 1 |
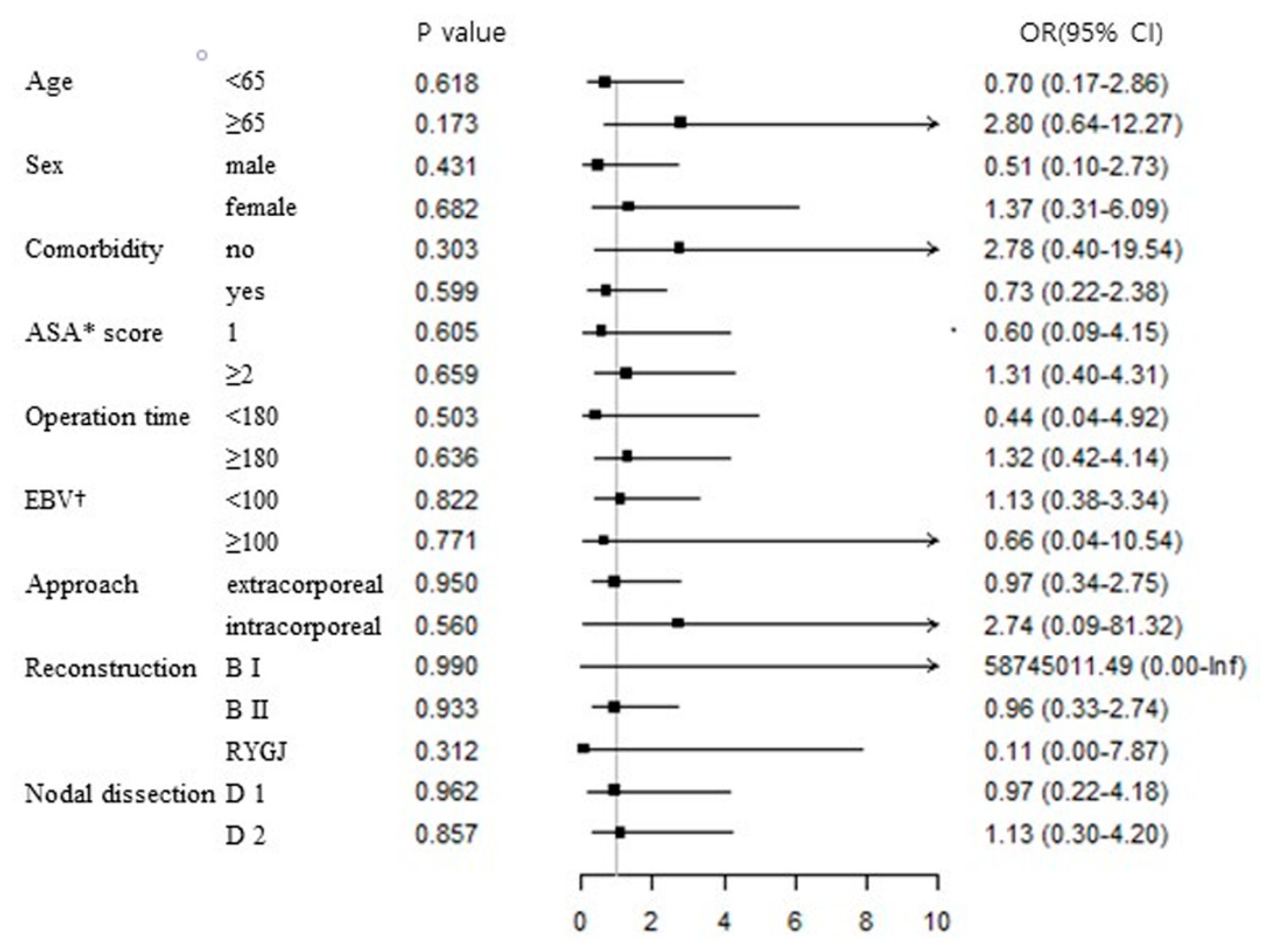
| PSM Set (n = 136) | ||||
|---|---|---|---|---|
| Univariate | Multivariate | |||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age (≥65 years) | 0.96 (0.38–2.40) | 0.929 | 1.35 (0.49–3.74) | 0.563 |
| Sex (female) | 0.88 (0.32–2.45) | 0.81 | 0.85 (0.29–2.53) | 0.775 |
| Body mass index (≥25 kg/m2) | 1.00 (0.40–2.49) | 1 | 1.05 (0.39–2.87) | 0.92 |
| Comorbidity | 0.67 (0.25–1.80) | 0.422 | 1.10 (0.28–4.32) | 0.89 |
| ASA score (≥2) | 0.54 (0.20–1.48) | 0.233 | 0.55 (0.14–2.07) | 0.374 |
| Operation time (≥3 h) | 0.86 (0.29–2.57) | 0.787 | 0.73 (0.22–2.38) | 0.6 |
| Estimated bleeding volume (≥100 cc) | 1.13 (0.30–4.31) | 0.86 | 1.20 (0.27–5.28) | 0.805 |
| Approach | ||||
| Intracorporeal | 1 | 1 | ||
| Extracorporeal | 1.48 (0.38–5.80) | 0.575 | 4.03 (0.37–43.65) | 0.251 |
| Reconstruction | ||||
| Billroth I | 1 | 1 | ||
| Billroth II | 1.73 (0.21–14.44) | 0.614 | 4.76 (0.19–119.10) | 0.342 |
| Roux-en-Y | 3.00 (0.22–40.93) | 0.41 | 6.94 (0.29–167.53) | 0.233 |
| Nodal dissection | ||||
| D1+ | 1 | 1 | ||
| D2 | 2.06 (0.81–5.21) | 0.127 | 2.01 (0.74–5.49) | 0.171 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-G.; Kang, D.-Y.; Kim, D.-Y. The Impact of Overweight and Obesity on Reduced-Port Laparoscopic Distal Gastrectomy for Gastric Cancer Patients: A Propensity Score Matching Analysis of a Single-Institution Data. J. Clin. Med. 2022, 11, 6453. https://doi.org/10.3390/jcm11216453
Kim H-G, Kang D-Y, Kim D-Y. The Impact of Overweight and Obesity on Reduced-Port Laparoscopic Distal Gastrectomy for Gastric Cancer Patients: A Propensity Score Matching Analysis of a Single-Institution Data. Journal of Clinical Medicine. 2022; 11(21):6453. https://doi.org/10.3390/jcm11216453
Chicago/Turabian StyleKim, Ho-Goon, Dong-Yeon Kang, and Dong-Yi Kim. 2022. "The Impact of Overweight and Obesity on Reduced-Port Laparoscopic Distal Gastrectomy for Gastric Cancer Patients: A Propensity Score Matching Analysis of a Single-Institution Data" Journal of Clinical Medicine 11, no. 21: 6453. https://doi.org/10.3390/jcm11216453
APA StyleKim, H. -G., Kang, D. -Y., & Kim, D. -Y. (2022). The Impact of Overweight and Obesity on Reduced-Port Laparoscopic Distal Gastrectomy for Gastric Cancer Patients: A Propensity Score Matching Analysis of a Single-Institution Data. Journal of Clinical Medicine, 11(21), 6453. https://doi.org/10.3390/jcm11216453