
Clinical Features of Anti-Synthetase Syndrome Associated with Prognosis in Patients with Dermatomyositis and Polymyositis


Abstract
:1. Introduction
2. Materials and Methods
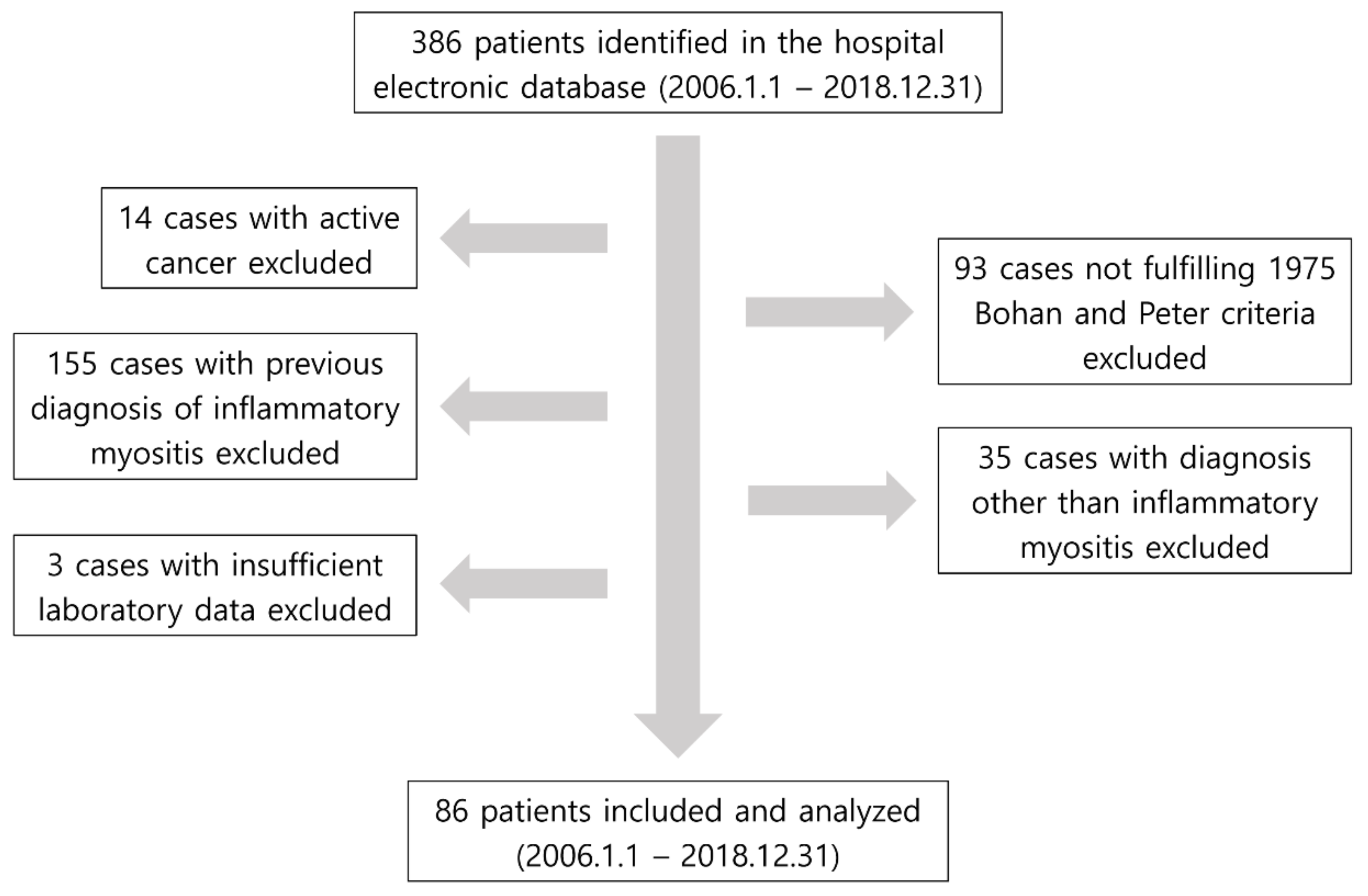
2.1. Study Design and Patient Selection
2.2. Collection of Baseline Patient Data
2.3. Clinical Features of Anti-Synthetase Syndrome, Definition of Clinical Outcomes and Treatment
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
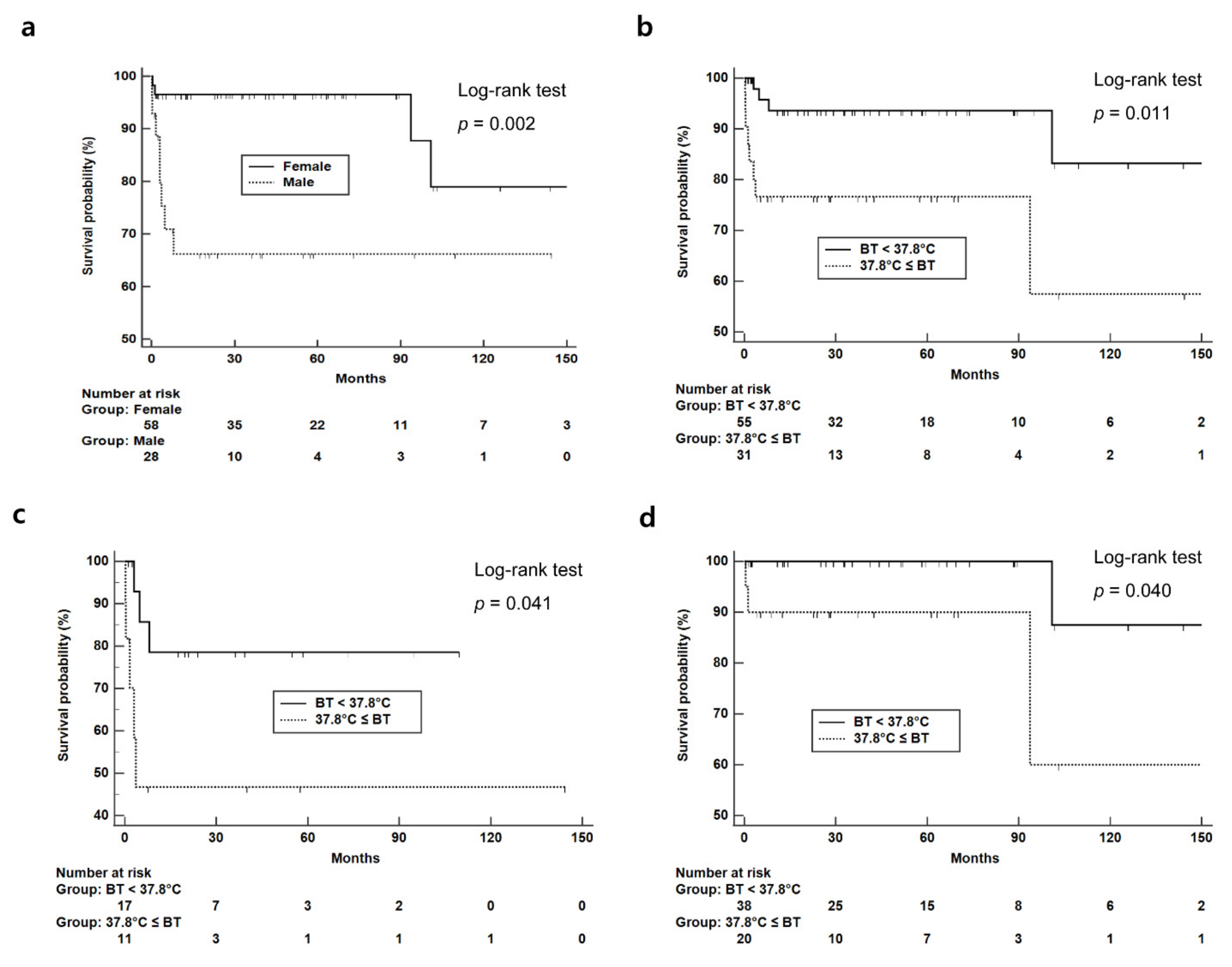
3.2. Clinical Outcomes Based on the Presence of Fever, Interstitial Lung Disease and Anti-Jo-1 Antibody
3.3. Clinical and Laboratory Features Associated with All-Cause Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chatterjee, S.; Prayson, R.; Farver, C. Antisynthetase syndrome: Not just an inflammatory myopathy. Cleve Clin. J. Med. 2013, 80, 655–666. [Google Scholar] [CrossRef] [PubMed]
- Connors, G.R.; Christopher-Stine, L.; Oddis, C.V.; Danoff, S.K. Interstitial lung disease associated with the idiopathic inflammatory myopathies: What progress has been made in the past 35 years? Chest 2010, 138, 1464–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witt, L.J.; Curran, J.J.; Strek, M.E. The Diagnosis and Treatment of Antisynthetase Syndrome. Clin. Pulm. Med. 2016, 23, 218–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, S.; Kronzer, V.L.; Dellaripa, P.F.; Deane, K.D.; Bolster, M.B.; Nagaraja, V.; Khanna, D.; Doyle, T.J.; Sparks, J.A. Rheumatoid arthritis-associated interstitial lung disease: Current update on prevalence, risk factors, and pharmacologic treatment. Curr. Treatm. Opt. Rheumatol. 2020, 6, 337–353. [Google Scholar] [CrossRef]
- Reiseter, S.; Gunnarsson, R.; Mogens Aaløkken, T.; Lund, M.B.; Mynarek, G.; Corander, J.; Haydon, J.; Molberg, Ø. Progression and mortality of interstitial lung disease in mixed connective tissue disease: A long-term observational nationwide cohort study. Rheumatology 2018, 57, 255–262. [Google Scholar] [CrossRef] [Green Version]
- Katsumata, Y.; Kawaguchi, Y.; Yamanaka, H. Interstitial Lung Disease with ANCA-associated Vasculitis. Clin. Med. Insights Circ. Respir. Pulm. Med. 2015, 9 (Suppl. S1), 51–56. [Google Scholar] [CrossRef]
- Sikora, K.A.; Grom, A.A. Update on the pathogenesis and treatment of systemic idiopathic arthritis. Curr. Opin. Pediatr. 2011, 23, 640–646. [Google Scholar] [CrossRef] [Green Version]
- Ahn, S.S.; Yoo, B.W.; Jung, S.M.; Lee, S.W.; Park, Y.B.; Song, J.J. In-hospital mortality in febrile lupus patients based on 2016 EULAR/ACR/PRINTO classification criteria for macrophage activation syndrome. Semin. Arthritis Rheum. 2017, 47, 216–221. [Google Scholar] [CrossRef]
- Cook, R.J.; Gladman, D.D.; Pericak, D.; Urowitz, M.B. Prediction of short term mortality in systemic lupus erythematosus with time dependent measures of disease activity. J. Rheumatol. 2000, 27, 1892–1895. [Google Scholar]
- Dalakas, M.C. Inflammatory muscle diseases. N. Engl. J. Med. 2015, 372, 1734–1747. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.H.; Chang, C.; Lian, Z.X. Polymyositis and dermatomyositis—Challenges in diagnosis and management. J. Transl. Autoimmun. 2019, 2, 100018. [Google Scholar] [CrossRef]
- Bronner, I.M.; van der Meulen, M.F.; de Visser, M.; Kalmijn, S.; van Venrooij, W.J.; Voskuyl, A.E.; Dinant, H.J.; Linssen, W.H.J.P.; Wokke, J.H.J.; Hoogendijk, J.E. Long-term outcome in polymyositis and dermatomyositis. Ann. Rheum. Dis. 2006, 65, 1456–1461. [Google Scholar] [CrossRef] [Green Version]
- Airio, A.; Kautiainen, H.; Hakala, M. Prognosis and mortality of polymyositis and dermatomyositis patients. Clin. Rheumatol. 2006, 25, 234–239. [Google Scholar] [CrossRef]
- Marie, I.; Hachulla, E.; Hatron, P.Y.; Hellot, M.F.; Levesque, H.; Devulder, B.; Courtois, H. Polymyositis and dermatomyositis: Short term and longterm outcome, and predictive factors of prognosis. J. Rheumatol. 2001, 28, 2230–2237. [Google Scholar] [CrossRef]
- Schiopu, E.; Phillips, K.; MacDonald, P.M.; Crofford, L.J.; Somers, E.C. Predictors of survival in a cohort of patients with polymyositis and dermatomyositis: Effect of corticosteroids, methotrexate and azathioprine. Arthritis Res. Ther. 2012, 14, R22. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Hao, Y.; Zhang, X.; Geng, Y.; Ji, L.; Li, G.; Zhang, Z. Mortality of Chinese patients with polymyositis and dermatomyositis. Clin. Rheumatol. 2020, 39, 1569–1579. [Google Scholar] [CrossRef]
- Marie, I. Morbidity and mortality in adult polymyositis and dermatomyositis. Curr. Rheumatol. Rep. 2012, 14, 275–285. [Google Scholar] [CrossRef]
- Bohan, A.; Peter, J.B. Polymyositis and dermatomyositis (first of two parts). N. Engl. J. Med. 1975, 292, 344–347. [Google Scholar] [CrossRef]
- Bohan, A.; Peter, J.B. Polymyositis and dermatomyositis (second of two parts). N. Engl. J. Med. 1975, 292, 403–407. [Google Scholar] [CrossRef] [Green Version]
- Fathi, M.; Lundberg, I.E. Interstitial lung disease in polymyositis and dermatomyositis. Curr. Opin. Rheumatol. 2005, 17, 701–706. [Google Scholar] [CrossRef] [Green Version]
- Marie, I.; Hatron, P.Y.; Cherin, P.; Hachulla, E.; Diot, E.; Vittecoq, O.; Menard, J.-F.; Jouen, F.; Dominique, S. Functional outcome and prognostic factors in anti-Jo1 patients with antisynthetase syndrome. Arthritis Res. Ther. 2013, 15, R149. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, E.; Gono, T.; Kuwana, M.; Terai, C. Predictive factors for sustained remission with stratification by myositis-specific autoantibodies in adult polymyositis/dermatomyositis. Rheumatology 2020, 59, 586–593. [Google Scholar] [CrossRef]
- Lee, L.W.; Narang, N.S.; Postolova, A.; Seminara, N.; Kantor, M.A. Anti-MDA5-Positive Dermatomyositis Presenting as Fever of Unknown Origin. J. Gen. Intern. Med. 2016, 31, 1530–1536. [Google Scholar] [CrossRef] [Green Version]
- Nakashima, R. Clinical significance of myositis-specific autoantibodies. Immunol. Med. 2018, 41, 103–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Opinc, A.H.; Makowska, J.S. Antisynthetase syndrome—Much more than just a myopathy. Semin. Arthritis Rheum. 2020, 51, 72–83. [Google Scholar] [CrossRef]
- Douglas, W.W.; Tazelaar, H.D.; Hartman, T.E.; Hartman, R.P.; Decker, P.A.; Schroeder, D.R.; Ryu, J. Polymyositis-dermatomyositis-associated interstitial lung disease. Am. J. Respir. Crit. Care Med. 2001, 164, 1182–1185. [Google Scholar] [CrossRef]
- Aggarwal, R.; Cassidy, E.; Fertig, N.; Koontz, D.C.; Lucas, M.; Ascherman, D.P.; Oddis, C.V. Patients with non-Jo-1 anti-tRNA-synthetase autoantibodies have worse survival than Jo-1 positive patients. Ann. Rheum. Dis. 2014, 73, 227–232. [Google Scholar] [CrossRef]
- Fathi, M.; Vikgren, J.; Boijsen, M.; Tylen, U.; Jorfeldt, L.; Tornling, G.; Lundberg, I.E. Interstitial lung disease in polymyositis and dermatomyositis: Longitudinal evaluation by pulmonary function and radiology. Arthritis Rheum. 2008, 59, 677–685. [Google Scholar] [CrossRef]
- Conti, B.; Tabarean, I.; Andrei, C.; Bartfai, T. Cytokines and fever. Front. Biosci. 2004, 9, 1433–1449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schultz, R.M. Interleukin 1 and interferon-gamma: Cytokines that provide reciprocal regulation of macrophage and T cell function. Toxicol. Pathol. 1987, 15, 333–337. [Google Scholar] [CrossRef]
- Moran, E.M.; Mastaglia, F.L. Cytokines in immune-mediated inflammatory myopathies: Cellular sources, multiple actions and therapeutic implications. Clin. Exp. Immunol. 2014, 178, 405–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Clinical Characteristics | Values |
|---|---|
| Demographics | |
| Age | 51.0 (29.0) |
| Male sex | 28 (32.6) |
| Diagnosis | |
| Polymyositis | 38 (44.2) |
| Dermatomyositis | 37 (43.0) |
| Juvenile dermatomyositis | 11 (12.8) |
| Previous comorbidities present ‡ | |
| Hypertension | 19 (22.1) |
| Diabetes mellitus | 13 (15.1) |
| Dyslipidemia | 5 (5.8) |
| Laboratory results | |
| White blood cell count (/mm3) | 7375.0 (3330.0) |
| Neutrophil count (/mm3) | 4340.0 (2867.5) |
| Platelet count (×1000/mm3) | 274.5 (130.0) |
| Erythrocyte sedimentation rate (mm/h) | 32.0 (34.0) |
| C-reactive protein (mg/L) (n = 81) | 2.6 (8.1) |
| Aspartate aminotransferase (IU/L) | 115.0 (192.0) |
| Alanine aminotransferase (IU/L) | 88.5 (144.0) |
| Creatinine kinase (IU/L) | 1884.0 (6684.0) |
| Anti-Jo-1 antibody positivity (n = 67) † | 20 (29.9) |
| Clinical features of anti-synthetase syndrome present | |
| Fever | 31 (36.0) |
| Raynaud’s phenomenon | 9 (10.5) |
| Mechanic’s hand | 5 (5.8) |
| Arthritis | 11 (12.8) |
| Interstitial lung disease | 23 (26.7) |
| Outcomes | |
| All-cause mortality | 12 (14.0) |
| Intensive care unit admission | 11 (12.8) |
| Remission at 1 year (n = 58) ¶ | 33 (56.9) |
| Follow-up duration (months) | 34.2 (61.1) |
| Anti-Jo-1 Antibody (+) Group (n = 20) | Anti-Jo-1 Antibody (−) Group (n = 47) | p-Value | |
|---|---|---|---|
| Fever | 9 (45.0) | 20 (42.6) | 0.854 |
| Raynaud’s phenomenon | 4 (20.0) | 4 (8.5) | 0.226 |
| Mechanic’s hand | 2 (10.0) | 3 (6.4) | 0.631 |
| Arthritis | 3 (15.0) | 7 (14.9) | 0.999 |
| Interstitial lung disease | 10 (50.0) | 12 (25.5) | 0.053 |
| All Patients (n = 86) | Fever (n = 86) | Interstitial Lung Disease (n = 86) | Anti-Jo-1 Antibody (n = 67) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes (n = 31) | No (n = 55) | p-Value | Yes (n = 23) | No (n = 63) | p-Value | Yes (n = 20) | No (n = 47) | p-Value | |
| All-cause mortality (+) | 8 (25.8) | 4 (7.3) | 0.024 | 6 (26.1) | 6 (9.5) | 0.051 | 5 (25.0) | 6 (12.8) | 0.220 |
| All-cause mortality (−) | 23 (74.2) | 51 (92.7) | 17 (73.9) | 57 (90.5) | 15 (75.0) | 41 (87.2) | |||
| Intensive care unit admission (+) | 7 (22.6) | 4 (7.3) | 0.051 | 5 (21.7) | 6 (9.5) | 0.136 | 5 (25.0) | 5 (10.6) | 0.134 |
| Intensive care unit admission (−) | 24 (77.4) | 51 (92.7) | 18 (78.3) | 57 (90.5) | 15 (75.0) | 42 (89.4) | |||
| Patients with follow-up ≥1 year (n = 58) | Fever (n = 58) | Interstitial lung disease (n = 58) | Anti-Jo-1 antibody (n = 48) | ||||||
| Yes (n = 17) | No (n = 41) | p-value | Yes (n = 13) | No (n = 45) | p-value | Yes (n = 13) | No (n = 35) | p-value | |
| Remission at 1 year (+) † (n = 58) | 14 (82.4) | 19 (46.3) | 0.019 | 5 (38.5) | 28 (62.2) | 0.131 | 4 (30.8) | 22 (62.9) | 0.059 |
| Remission at 1 year (−) † (n = 58) | 3 (17.6) | 22 (53.7) | 8 (61.5) | 17 (37.8) | 9 (69.2) | 13 (37.1) | |||
| Patients with Interstitial Lung Disease (n = 23) | Patients without Interstitial Lung Disease (n = 63) | p-Value | |
|---|---|---|---|
| Glucocorticoid | 23 (100.0) | 63 (100.0) | 0.999 |
| Methotrexate | 7 (30.4) | 36 (57.1) | 0.029 |
| Azathioprine | 13 (56.5) | 16 (25.4) | 0.007 |
| Intravenous immunoglobulin | 8 (34.8) | 19 (30.2) | 0.684 |
| Rituximab | 1 (4.3) | 4 (6.3) | 0.999 |
| Hydroxychloroquine | 5 (21.7) | 20 (31.7) | 0.369 |
| Cyclophosphamide | 3 (13.0) | 5 (7.9) | 0.436 |
| Tacrolimus | 3 (13.0) | 3 (4.8) | 0.336 |
| Mycophenolate mofetil | 2 (8.7) | 4 (6.3) | 0.656 |
| Patients with Mortality (n = 12) | Patients without Mortality (n = 74) | p-Value | |
|---|---|---|---|
| Glucocorticoid | 12 (100.0) | 74 (100.0) | 0.999 |
| Methotrexate | 3 (25.0) | 40 (54.1) | 0.117 |
| Azathioprine | 3 (25.0) | 26 (35.1) | 0.743 |
| Intravenous immunoglobulin | 5 (41.7) | 22 (29.7) | 0.411 |
| Rituximab | 2 (16.7) | 3 (4.1) | 0.141 |
| Hydroxychloroquine | 2 (16.7) | 23 (31.1) | 0.496 |
| Cyclophosphamide | 2 (16.7) | 6 (8.1) | 0.309 |
| Tacrolimus | 1 (8.3) | 5 (6.8) | 0.999 |
| Mycophenolate mofetil | 1 (8.3) | 5 (6.8) | 0.999 |
| Univariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | 1.04 | 1.01, 1.08 | 0.02 | |||
| Male sex | 5.54 | 1.66, 18.56 | <0.01 | 5.53 | 1.65, 18.49 | <0.01 |
| Hypertension | 1.99 | 0.60, 6.62 | 0.26 | |||
| Diabetes mellitus | 3.57 | 1.07, 11.93 | 0.04 | |||
| Dyslipidemia ¶ | n/a | |||||
| White blood cell count | 1.00 | 1.00, 1.00 | 0.30 | |||
| Neutrophil count | 1.00 | 1.00, 1.00 | 0.96 | |||
| Platelet count | 1.00 | 1.00, 1.00 | 0.95 | |||
| Erythrocyte sedimentation rate | 1.02 | 1.00, 1.03 | 0.04 | |||
| Aspartate aminotransferase | 1.00 | 1.00, 1.00 | 0.77 | |||
| Alanine aminotransferase | 1.00 | 0.99, 1.00 | 0.37 | |||
| Creatinine kinase | 1.00 | 1.00, 1.00 | 0.68 | |||
| Fever | 4.20 | 1.26, 13.97 | 0.02 | 4.20 | 1.26, 14.01 | 0.02 |
| Raynaud’s phenomenon | 0.87 | 0.11, 6.76 | 0.90 | |||
| Mechanic’s hand ¶ | n/a | |||||
| Arthritis | 0.49 | 0.06, 3.79 | 0.49 | |||
| Interstitial lung disease | 3.06 | 0.98, 9.49 | 0.05 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, S.S.; Park, Y.-B.; Lee, S.-W. Clinical Features of Anti-Synthetase Syndrome Associated with Prognosis in Patients with Dermatomyositis and Polymyositis. J. Clin. Med. 2022, 11, 2052. https://doi.org/10.3390/jcm11072052
Ahn SS, Park Y-B, Lee S-W. Clinical Features of Anti-Synthetase Syndrome Associated with Prognosis in Patients with Dermatomyositis and Polymyositis. Journal of Clinical Medicine. 2022; 11(7):2052. https://doi.org/10.3390/jcm11072052
Chicago/Turabian StyleAhn, Sung Soo, Yong-Beom Park, and Sang-Won Lee. 2022. "Clinical Features of Anti-Synthetase Syndrome Associated with Prognosis in Patients with Dermatomyositis and Polymyositis" Journal of Clinical Medicine 11, no. 7: 2052. https://doi.org/10.3390/jcm11072052
APA StyleAhn, S. S., Park, Y. -B., & Lee, S. -W. (2022). Clinical Features of Anti-Synthetase Syndrome Associated with Prognosis in Patients with Dermatomyositis and Polymyositis. Journal of Clinical Medicine, 11(7), 2052. https://doi.org/10.3390/jcm11072052