
Ocular Manifestations of Takayasu’s Arteritis—A Case-Based Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
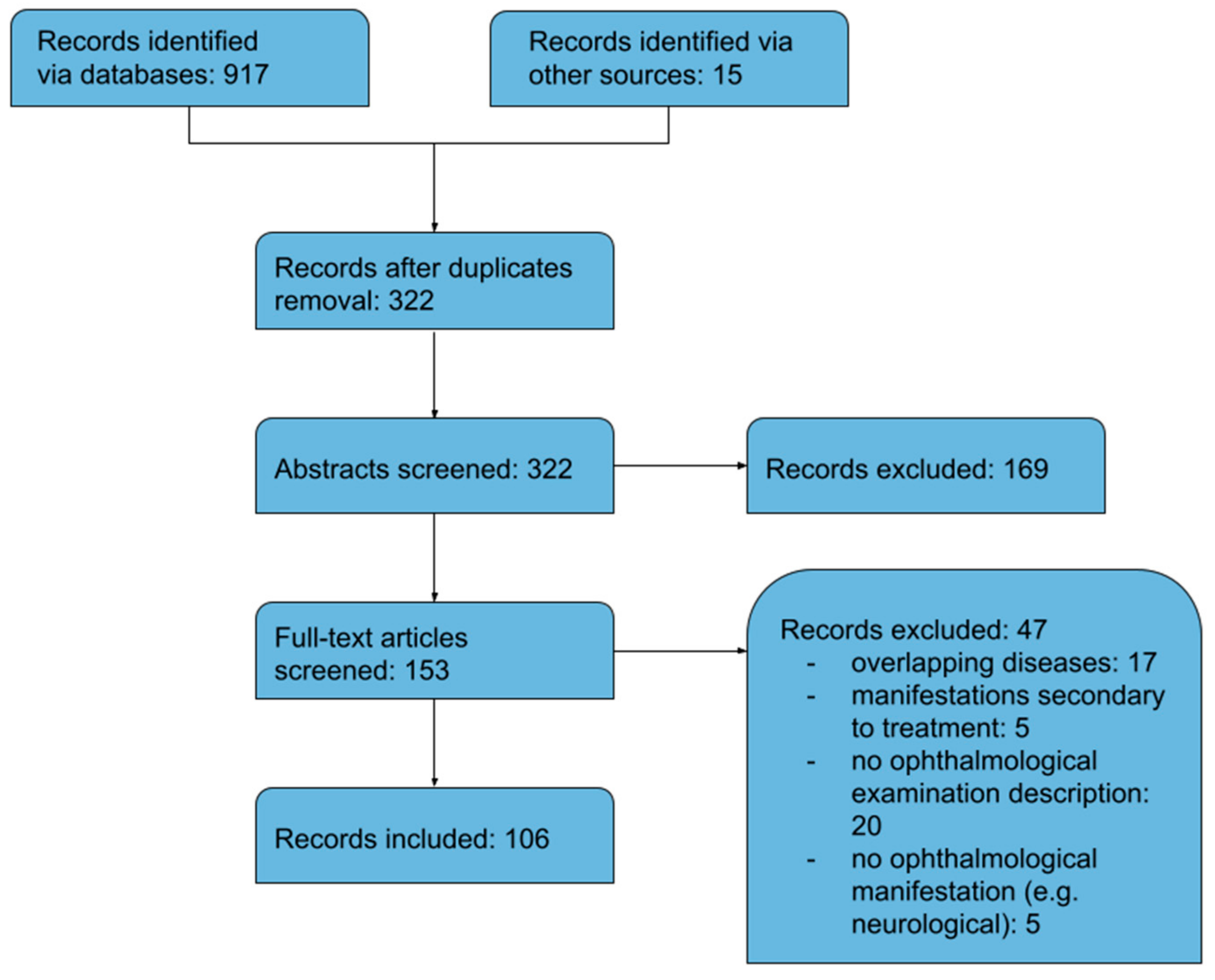
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Turk, M.A.; Hayworth, J.L.; Nevskaya, T.; Pope, J.E. Ocular Manifestations in Rheumatoid Arthritis, Connective Tissue Disease, and Vasculitis: A Systematic Review and Metaanalysis. J. Rheumatol. 2021, 48, 25–34. [Google Scholar] [CrossRef]
- Turk, M.A.; Hayworth, J.L.; Nevskaya, T.; Pope, J.E. Ocular manifestations of Behçet’s disease in children and adults: A systematic review and meta-analysis. Clin. Exp. Rheumatol. 2021, 132, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Trinidad, B.; Surmachevska, N.; Lala, V. Takayasu Arteritis. [Updated 8 August 2022]. StatPearls Publishing. 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459127/ (accessed on 5 December 2022).
- Mayo Clinic. Takayasu’s Arteritis. Available online: https://www.mayoclinic.org/diseases-conditions/takayasus-arteritis/symptoms-causes/syc-20351335 (accessed on 5 December 2022).
- Onen, F.; Akkoc, N. Epidemiology of Takayasu arteritis. Presse Med. 2017, 46, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Keser, G.; Aksu, K.; Direskeneli, H. Takayasu arteritis: An update. Turk. J. Med. Sci. 2018, 48, 681–697. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, J.L.; Ai, S.; Matsumura, I. New Insights on the Pathogenesis of Takayasu Arteritis: Revisiting the Microbial Theory. Pathogens 2018, 6, 73. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Akhtar, S.; Babar, S.; Lightman, S.; Mason, J.C. Adalimumab-induced remission of anterior scleritis: A very rare late manifestation of Takayasu arteritis. Rheumatology 2015, 54, 2288–2290. [Google Scholar] [CrossRef]
- Amer, R.; Rankin, R.; Mackenzie, J.; Olson, J. Posterior scleritis: An ominous sign of occult Takayasu’s arteritis. Br. J. Ophthalmol. 2007, 91, 1568–1569. [Google Scholar] [CrossRef]
- Anguita, R.; Nazar, C.; Kobus, R.; Salinas, A.; Astete, M. Bilateral ocular ischemic syndrome as a manifestation of Takayasu arteritis in children. Can. J. Ophthalmol. 2019, 54, 105–108. [Google Scholar] [CrossRef]
- Arya, S.K.; Nahar, R.; Narang, S.; Jain, R.; Kalra, N.; Sood, S. Sclerokeratitis in Takayasu’s arteritis: A case report. Jpn. J. Ophthalmol. 2005, 49, 548–550. [Google Scholar] [CrossRef]
- Austen, W.G.; Shaw, R.S. Surgical Treatment of Pulseless (Takayasu’s) Disease. N. Engl. J. Med. 1964, 270, 1228–1231. [Google Scholar] [CrossRef]
- Babu, K.; Parameswarappa, D.C. Atypical Tolosa Hunt syndrome with bilateral sclerokeratitis and optic atrophy in Takayasu’s arteritis. Am. J. Ophthalmol. Case Rep. 2016, 5, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Bajgai, P.; Singh, R. Retinal Vasculitis in Takayasu’s Arteritis. N. Engl. J. Med. 2018, 378, 28. [Google Scholar] [CrossRef]
- Balaskas, K.; Potamitou, D.; Spastri, A. Occlusion de branche artérielle rétinienne comme manifestation oculaire isolée d’une maladie de Takayasu Branch retinal artery occlusion as the sole ocular manifestation of Takayasu arteritis. J. Fr. Ophtalmol. 2010, 33, 50.e1–50.e3. [Google Scholar] [CrossRef]
- Bapat, V.N.; Tendolkar, A.G. Turning a blind eye. Lancet 1997, 349, 1740. [Google Scholar] [CrossRef] [PubMed]
- Batliwala, S.Y.; Perez, M.; Aston, W.; Chavala, S.H. Peripheral Retinal Telangiectasia and Ischemia in Takayasu Arteritis. Arthritis Rheumatol. 2016, 68, 2350. [Google Scholar] [CrossRef]
- Becker, R.W.; Sohn, R.L.; Poulik, J.M.; Berguer, R. Takayasu’s arteritis presenting as uveitis in a 5-year-old girl. Ann. Vasc. Surg. 2005, 19, 258–262. [Google Scholar] [CrossRef]
- Bodker, F.S.; Tessler, H.H.; Shapiro, M.J. Ocular complications of Takayasu’s disease in a Hispanic woman. Am. J. Ophthalmol. 1993, 115, 676–677. [Google Scholar] [CrossRef]
- Bouzas, E.A.; Karadimas, P.; Alexandrou, A.; Panagopoulos, I. Epiretinal membrane in association with Takayasu disease. Acta Ophthalmol. Scand. 1999, 77, 483–484. [Google Scholar] [CrossRef] [PubMed]
- Caccamise, W.C.; Whitman, J.F. Pulse-less disease; a preliminary case report. Am. Heart J. 1952, 44, 628–633. [Google Scholar]
- Chaudhary, M.; Shah, D.N.; Chaudhary, R.P. Scleritis and Takayasu’s disease—Rare combined presentation. Nepal. J. Ophthalmol. 2017, 9, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Chawla, M.; Longe, A.C.; Keshav, B.R.; Arya, B.Y.T. Takayasu’s Disease: Report of a Case with Severe Neurological and Ocular Complications. Ann. Saudi Med. 2019, 17, 629–631. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, M.E.; O’Carroll, C.B.; Kumar, G.; Larsen, B.T.; Dumitrascu, O.M. Transcranial Doppler Evaluation in Takayasu Arteritis with Oculo-Cerebrovascular Complications. Neurologist 2019, 24, 17–21. [Google Scholar] [CrossRef]
- Conrath, J.; Hadjadj, E.; Serratrice, J.; Ridings, B. Occlusion de branche veineuse rétinienne révélatrice d’une maladie de Takayasu Branch retinal vein occlusion reveals Takayasu’s arteritis. J. Fr. Ophtalmol. 2004, 27, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Das, B.; Pandharpurkar, M. A rare disease with a rarer presentation: Nodular episcleritis in Takayasu’s arteritis. Indian J. Ophthalmol. 2022, 70, 2675–2677. [Google Scholar] [CrossRef]
- Demir, M.N.; Hazirolan, D.; Altiparmak, U.E.; Acar, M.A.; Unlü, N.; Ornek, F. Takayasu’s disease and secondary ocular ischemic syndrome. J. Pediatr. Ophthalmol. Strabismus 2010, 47, 54–57. [Google Scholar] [CrossRef]
- Do Vale, M.A.B.; Brito, P.; Ribeiro, M.P.; Bulhões, M.A. Síndrome ocular isquêmica secundária à arterite de Takayasu: Relato de caso Ocular ischemic syndrome secondary to Takayasu’s arteritis: Case report. Arq. Bras. Oftalmol. 2002, 65, 107–110. [Google Scholar] [CrossRef]
- Dowling, J.L., Jr.; Smith, T.R. An ocular study of pulseless disease. Arch. Ophthalmol. 1960, 64, 236–243. [Google Scholar] [CrossRef]
- Elizalde, J.; Capella, M.J. Takayasu’s retinopathy. Int. Ophthalmol. 2011, 3, 533–537. [Google Scholar] [CrossRef]
- Escano, M.F.; Ino-ue, M.; Azumi, A.; Yamada, Y.; Yamamoto, M. Colour Doppler imaging in Takayasu’s arteritis. Br. J. Ophthalmol. 1998, 82, 1091–1092. [Google Scholar] [CrossRef]
- Font, R.L.; Naumann, G. Ocular histopathology in pulseless disease. Arch. Ophthalmol. 1969, 82, 784–788. [Google Scholar] [CrossRef] [PubMed]
- Gaur, N.; Sharma, P.; Takkar, B.; Singh, J. Bilateral ischaemic optic neuropathy and retinopathy along with cortical infarct in a case of Takayasu disease. Case Rep. 2017, 2017, bcr-2017-220970. [Google Scholar] [CrossRef] [PubMed]
- Genç, B.O.; Genç, E.; Açik, L.; Ilhan, S.; Paksoy, Y. Acquired ocular motor apraxia from bilateral frontoparietal infarcts associated with Takayasu arteritis. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1651–1652. [Google Scholar] [CrossRef] [PubMed]
- Gong, Q.; Qian, T.; Chen, F.; Xu, X.; Wang, W. A case of anti-VEGF therapy application in Takayasu arteries with retinopathy. Am. J. Ophthalmol. Case Rep. 2020, 19, 100706. [Google Scholar] [CrossRef]
- Guclu, H.; Gurlu, V.P.; Ozal, S.A.; Guclu, O. Central Retinal Artery Occlusion in Takayasu’s Arteritis as the First Presentation of the Disease. Case Rep. Ophthalmol. Med. 2016, 2016, 6492513. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Luthra, S.; Shrinkhal, N.; Sinha, S. Takayasu’s arteritis: A unique ophthalmic presentation with CRAO and BRVO. BMJ Case Rep. 2019, 12, e228909. [Google Scholar] [CrossRef]
- Harada, M.; Yoshida, H.; Mitsuyama, K.; Sakamoto, M.; Koga, H.; Matsuo, K.; Teshima, Y.; Ikeda, E.; Sakisaka, S.; Sata, M.; et al. Aortitis syndrome (Takayasu’s arteritis) with cataract and elevated serum level of vascular endothelial growth factor. Scand. J. Rheumatol. 1998, 27, 78–79. [Google Scholar]
- Hayasaka, S.; Matsui, H.; Noda, S.; Setogawa, T. Electroretinographic responses in patients with pulseless disease vary with head and body positions. Graefes Arch. Clin. Exp. Ophthalmol. 1991, 229, 508–511. [Google Scholar] [CrossRef]
- Herath, H.M.M.T.B.; Pahalagamage, S.P.; Withana, D.; Senanayake, S. Complete ophthalmoplegia, complete ptosis and dilated pupil due to internal carotid artery dissection: As the first manifestation of Takayasu arteritis. BMC Cardiovasc. Disord. 2017, 17, 201. [Google Scholar] [CrossRef]
- Ibrahim, H.; D’souza, S.; Agorogiannis, E.; Ali, A.; Bashar, N.; Pearce, I.; Madhusudhan, S. Lessons of the month 2: Retinal vasculitis: A first presentation of Takayasu’s arteritis. Clin. Med. 2021, 21, 673–676. [Google Scholar] [CrossRef]
- Jain, I.S.; Grover, A.D. Pulsless Disease. Br. J. Ophthalmol. 1963, 47, 304–307. [Google Scholar] [CrossRef]
- Jain, R.; Ionides, A.; Pavesio, C.; Russell, A.; Haskard, D. Scleritis as a presenting feature of Takayasu’s disease. Br. J. Ophthalmol. 2000, 84, 801. [Google Scholar] [CrossRef] [PubMed]
- Jain, V.K.; Pal, S.; Singh, V.; Saha, R.; Sharma, K. Visual outcome after endovascular intervention in Takayasu arteritis. Taiwan J. Ophthalmol. 2022, 12, 206–208. [Google Scholar] [PubMed]
- Kaliaperumal, S.; Gupta, A.; Sengupta, S.; Srinivasan, R. Unilateral hemorrhagic keratouveitis as the initial presentation of Takayasu’s arteritis. Indian J. Ophthalmol. 2007, 55, 397–398. [Google Scholar]
- Kancherla, H.; Konduri, G.; Bollam, A.; Atla, K.; Injeti, N. Takayasu Arteritis: A Case Report. J. Young Pharm. 2022, 14, 130–132. [Google Scholar] [CrossRef]
- Kannan, N.B.; Kohli, P.; Ramachandran, N.O. Abnormal Retinal Vasculature in a Young Child: A Diagnostic Dilemma. Ocul. Immunol. Inflamm. 2021, 29, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Kapran, Z.; Atmaca, L.S.; Albayrak, Z.; Uyar, M.; Eltutar, K. Bilateral glaucomatous optic neuropathy in Takayasu’s disease without cervical arterial stenosis. Eur. J. Ophthalmol. 2001, 11, 93–96. [Google Scholar] [CrossRef]
- Karam, E.Z.; Muci-Mendoza, R.; Hedges, T.R., 3rd. Retinal findings in Takayasu’s arteritis. Acta Ophthalmol. Scand. 1999, 77, 209–213. [Google Scholar] [CrossRef]
- Karwatowski, W.S.; Jampol, L.M.; Mani, H.; Weinreb, R.N. Neovascular glaucoma in Takayasu’s disease: A case report. Retina 1995, 15, 353–354. [Google Scholar] [CrossRef]
- Kaushik, S.; Gupta, A.; Gupta, V.; Jain, S.; Lal, V. Retinal arterial occlusion in Takayasu’s arteritis. Indian J. Ophthalmol. 2005, 53, 194–196. [Google Scholar]
- Kausman, J.Y.; Walker, A.; Piper, S. Acute panuveitis and Takayasu’s arteritis. Arch. Dis. Child. 2003, 88, 938–939. [Google Scholar] [CrossRef] [PubMed]
- Kavitha, R.; Sakthi, A.; Kunjumoidu, N.; Bakyaraj, S.; Vishnuram, P.; Karuppusamy, N.; Natarajan, K.; Kala, C.J.; Hemanandini, M. Takayasu Arteritis with Atrial Septal Defect Presenting as Sterile Corneal Melt. J. Assoc. Physicians India 2019, 67, 80–81. [Google Scholar] [PubMed]
- Kim, I.T.; Park, S.K.; Shim, S.D. Unilateral anterior ischemic optic neuropathy caused by Takayasu’s arteritis. Neuro-Ophthalmology 1999, 22, 107–113. [Google Scholar] [CrossRef]
- Kimura, H.; Masai, H.; Kashii, S. Anterior ischemic optic neuropathy associated with pulseless disease. Ophthalmologica 1995, 209, 346–348. [Google Scholar] [CrossRef]
- Kinoshita, N.; Yanagi, Y.; Tamaki, Y.; Obata, R.; Takahashi, H. Sequential change of ophthalmic findings after bypass graft surgery in Takayasu disease. Retina 2005, 25, 225–227. [Google Scholar] [CrossRef]
- Koz, O.G.; Ates, A.; Numan Alp, M.; Gultan, E.; Karaaslan, Y.; Kural, G. Bilateral ocular ischemic syndrome as an initial manifestation of Takayasu’s arteritis associated with carotid steal syndrome. Rheumatol. Int. 2007, 27, 299–302. [Google Scholar] [CrossRef]
- Kumar, G.; Kumar, A.; Menon, V. Ophthalmic manifestations of pulseless disease: A case report. Indian J. Ophthalmol. 1995, 43, 79–81. [Google Scholar]
- Kuwahara, C.; Imamura, Y.; Okamura, N.; Sakai, R.; Ikeda, T. Severe proliferative retinopathy progressing to blindness in a japanese woman with takayasu disease. Am. J. Ophthalmol. 2003, 135, 722–723. [Google Scholar] [CrossRef]
- Larrazabal, R.B.; Chiu, H.H.C.; Magbitang-Santiago, A.T. Takayasu Arteritis Presenting as Bilateral Ocular Ischemic Syndrome. Vasc. Spec. Int. 2020, 36, 163–169. [Google Scholar] [CrossRef]
- Lee, G.I.; Bae, K.; Kim, J.M.; Kang, S.W. A Case Report of Takayasu’s Arteritis with Traction Retinal Detachment. J. Korean Ophthalmol. Soc. 2017, 58, 600–605. [Google Scholar] [CrossRef]
- Lee, J.C.; Wang, M.Y.; Damodar, D.; Sadun, A.A.; Sadda, S. Headache and whiteout vision as the presenting symptoms in a case of Takayasu retinopathy. Retin. Cases Brief Rep. 2014, 8, 273–275. [Google Scholar] [CrossRef] [PubMed]
- Leonard, T.J.; Sanders, M.D. Ischaemic optic neuropathy in pulseless disease. Br. J. Ophthalmol. 1983, 67, 389–392. [Google Scholar] [CrossRef]
- Lewis, J.R.; Glaser, J.S.; Schatz, N.J.; Hutson, D.G. Pulseless (Takayasu) disease with ophthalmic manifestations. J. Neuro-Ophthalmol. 1993, 13, 242–249. [Google Scholar]
- Lim, J.W.; Lee, S.U.; Lee, S.J.; Nam, K.Y. A Case of Branch Retinal Artery Occlusion Associated with Takayasu’s Arteritis. J. Korean Ophthalmol. Soc. 2016, 57, 1312–1315. [Google Scholar] [CrossRef]
- Mahajan, S.; Behera, U.C.; Pravabati, S.L.; Shah MPadhy, S.K.; Kelgaonkar, A. Pulseless and blindness—An ophthalmologist’s role in diagnosing Takayasu arteritis: Case series and brief review of literature. Eur. J. Ophthalmol. 2021, 31, 3525–3531. [Google Scholar] [CrossRef]
- Mahendradas, P.; Vala, R.; Kawali, A.; Akkali, M.C.; Shetty, R. Adaptive Optics Imaging in Retinal Vasculitis. Ocul. Immunol. Inflamm. 2018, 26, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Mashru, P.; Sagdeo, P.; Gattimallanahali, Y.; Mangat, G. Atypical eye complication in Takayasu’s arteritis. Case Rep. 2016, 2016, bcr2016215018. [Google Scholar] [CrossRef] [PubMed]
- Matalia, J.; Kasturi, N.; Anaspure, H.D.; Shetty, B.K. Tonic pupil, anterior ischemic optic neuropathy in a teenager with Takayasu arteritis. Can. J. Ophthalmol. 2013, 48, 159–163. [Google Scholar] [CrossRef]
- Matsumoto-Otake, A.; Hirota, K.; Koto, T.; Inoue, M.; Hirakata, A. Thickened retinal ganglion cell complex in patient with severe Takayasu retinopathy at early stage. Retin. Cases Brief Rep. 2015, 9, 41–44. [Google Scholar] [CrossRef]
- McDonald, M.A.; Ojaimi, E.; Favilla, I. Anterior uveitis in a child with Takayasu’s arteritis. Clin. Exp. Ophthalmol. 2004, 32, 336–339. [Google Scholar] [CrossRef]
- Milea, D.; Cassoux, N.; Lehoang, P.; Gerber, S.; Marsault, C.; Piette, J.C.; Amoura, Z.; Kieffer, E.; Lehoang, P. Neovascular glaucoma after bypass surgery in Takayasu’s disease. Eye 1999, 13, 786–789. [Google Scholar] [CrossRef]
- Moncada, G.; Kobayashi, Y.; Kaneko, E.; Nishiwaki, Y.; Kishi, Y.; Numano, F. Subclavian steal syndrome secondary to Takayasu arteritis. Int. J. Cardiol. 1998, 66, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Nithyanandam, S.; Mohan, A.; Sheth, U. Anterior ischemic optic neuropathy in a case of Takayasu’s arteritis. Oman J. Ophthalmol. 2010, 3, 94–95. [Google Scholar] [CrossRef] [PubMed]
- Noel, N.; Butel, N.; Le Hoang, P.; Koskas, F.; Costedoat-Chalumeau, N.; Wechsler, B.; Amoura, Z.; Bodaghi, B.; Cacoub, P.; Saadoun, D. Small vessel involvement in Takayasu’s arteritis. Autoimmun. Rev. 2013, 12, 355–362. [Google Scholar] [CrossRef]
- Ostler, H.B. Pulseless disease (Takayasu’s disease). Am. J. Ophthalmol. 1957, 43, 583–589. [Google Scholar] [CrossRef]
- Padhy, S.K.; Chawla, R. Novel ultrawide field fundus fluorescein angiographic findings in a patient of Takayasu arteritis on immunosuppression. Indian J. Ophthalmol. 2020, 68, 238–240. [Google Scholar] [CrossRef]
- Pahwa, J.M.; Pandey, M.P.; Gupta, D.P. Pulseless disease, or Takayasu’s disease. Case Rep. Br. Med. J. 1959, 2, 1439–1442. [Google Scholar]
- Pallangyo, P.; Epafra, E.; Nicholaus, P.; Lyimo, F.; Kazahura, P.; Janabi, M. Bilateral ocular ischemia-induced blindness as a presenting manifestation of Takayasu arteritis: A case report. J. Med. Case Rep. 2017, 11, 153. [Google Scholar] [CrossRef]
- Paterson, M.W. Ocular changes in the pulseless disease (Takayasu’s disease: The aortic arch syndrome). Scott. Med. J. 1957, 2, 57–65. [Google Scholar] [CrossRef]
- Paul, A.K. Ocular manifestations of pulseless disease. Indian J. Ophthalmol. 1975, 23, 36–38. [Google Scholar]
- Pelegrín, L.; Mesquida, M.; Rey, A.; Sánchez-Dalmau, B.; Frohman, L. Blind runner. Surv. Ophthalmol. 2012, 57, 486–494. [Google Scholar] [CrossRef]
- Peter, J.; Joseph, G.; David, S.; Danda, D. Regression of takayasu retinopathy after revascularization of occluded branches of the aortic arch by percutaneous angioplasty. Retin. Cases Brief Rep. 2013, 7, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Peter, J.; David, S.; Joseph, G.; Horo, S.; Danda, D. Hypoperfusive and hypertensive ocular manifestations in Takayasu arteritis. Clin. Ophthalmol. 2010, 4, 1173–1176. [Google Scholar] [CrossRef] [PubMed]
- Rainer, K.; Eshtehardi, P.; Bercu, Z.L.; Navarrete, J.E.; Gandiga, P.C.; Yeh, S.; Wells, B.J. New-Onset Uncontrolled Hypertension and Renal Failure in a Young Woman. Case Rep. 2020, 2, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Abd Rahman, S.A.; Mohd Khialdin, S.; Muda, R. Stage 4 Takayasu Retinopathy with Persistent Neovascularization. Cureus 2021, 13, e16640. [Google Scholar] [CrossRef] [PubMed]
- Rajshri, H.; Krishnappa, N.C.; Arthi, M. Blinding vasculitis: Bilateral severe vision loss as a presenting feature of undiagnosed Takayasu arteritis. BMJ Case Rep. 2022, 15, e251366. [Google Scholar] [CrossRef]
- Ramteke, V.V.; Gokhale, Y.A.; Kamdar, P.A.; Maniar, V.; Shrivastava, M.; Singh, N.; Krishna, B.A. Sudden mono-ocular blindness with recurrent transient diplopia and ptosis in a middle-aged woman. Case Rep. 2011, 2011, bcr1020103414. [Google Scholar] [CrossRef]
- Reddy, S.; Tyagi, M.; Suresh, A.; Dogra, A. Multimodal imaging in bilateral ocular ischaemic syndrome with anterior ischaemic optic neuropathy in a case of Takayasu arteritis. BMJ Case Rep. 2020, 13, e236351. [Google Scholar] [CrossRef]
- Rodriguez, A.R.; Rebello, R.; Khalidi, N. Hypertensive Retinopathy in Takayasu Arteritis. Neuro-Ophthalmology 2013, 37, 157–158. [Google Scholar] [CrossRef]
- Sakthiswary, R.; Syazarina, S.O.; Shaharir, S.S.; Said, M.S.; Hanom, F. Blindness in a pulseless young woman: Lessons learned. Ocul. Immunol. Inflamm. 2012, 20, 309–311. [Google Scholar] [CrossRef]
- Santhanam, S.; Sankaralingam, R.; Tamilselvam, T.N.; Mani, M. Bilateral visual loss as presenting manifestation—Takayasu arteritis. Indian J. Rheumatol. 2015, 10, 172–173. [Google Scholar] [CrossRef]
- Setty, H.S.N.; Reddy, B.; Srinivas, B.C.; Raghu, T.R.; Kharge, J.; Patil, R.; Raj, S.; Nagesh, C.M.; Manjunath, C.N. Young lady presented with sudden loss of vision. Xiangya Med. 2019, 4, 13. [Google Scholar] [CrossRef]
- Shailaja, S.; Vivek, G.; Shetty, R.; Kamath, Y. Eye is a window to the pulse: Bilateral ocular ischaemic syndrome as a presenting manifestation of Takayasu arteritis. Case Rep. 2013, 2013, bcr2013009461. [Google Scholar] [CrossRef]
- Shrestha, R.; Pandit, A.; Kharel, G. Takayasu Arteritis Presenting As Epileptic Seizure: A Case Report. Cureus 2022, 14, e26520. [Google Scholar] [CrossRef] [PubMed]
- Shukla, E.; Desai, A.; Malkan, N.; Gokhale, Y. Nodular scleritis as a presenting feature of Takayasu’s arteritis. Indian J. Ophthalmol. 2016, 64, 312–314. [Google Scholar] [CrossRef]
- Smith, J.R.; Rosenbaum, J.T. Case reports and small case series: Scleritis occurring in association with Takayasu disease. Arch. Ophthalmol. 2001, 119, 778–779. [Google Scholar]
- Stone, J.H.; Nousari, H.C.; Jabs, D.A.; Griffith, L.S. Takayansu’s Arteritis Associated with Anterior Uveitis and Cutaneous Extravascular Necrotizing Granuloma. J. Clin. Rheumatol. 1998, 4, 319–322. [Google Scholar] [CrossRef]
- Strauss, D.S.; Barbazetto, I. Takayasu retinopathy presenting as amaurosis fugax in a young patient. Retin. Cases Brief Rep. 2013, 7, 1–4. [Google Scholar] [CrossRef]
- Subirà, O.; Muñoz, S.; Sánchez, J.J.; Puyalto, P.; Lee, A.G. Painless bilateral visual loss in a 33-year-old woman with severe arterial hypotension. Surv. Ophthalmol. 2018, 63, 125–131. [Google Scholar] [CrossRef]
- Suematsu, R.; Tashiro, S.; Ono, N.; Koarada, S.; Ohta, A.; Tada, Y. Successful golimumab therapy in four patients with refractory Takayasu’s arteritis. Mod. Rheumatol. 2018, 28, 712–715. [Google Scholar] [CrossRef]
- Suh, S.Y.; Lee, S.M.; So, M.W.; Lee, S.G.; Park, S.W.; Byon, I.S. Bilateral Central Retinal Vein Occlusion in a Patient with Takayasu Arteritis. J. Korean Ophthalmol. Soc. 2020, 61, 1380–1385. [Google Scholar] [CrossRef]
- Sureja, N.P.; Kalyan, S.; Patel, M.R. Recurrent scleritis as a presenting manifestation of asymptomatic occult Takayasu arteritis. Rheumatol. Adv. Pract. 2021, 5, rkaa065. [Google Scholar] [CrossRef]
- Tani, T.; Takahashi, A.; Nagaoka, T.; Yoshida, A. Abnormality of retinal arterial velocity profiles using Doppler Fourier-domain optical coherence tomography in a case of Takayasu’s arteritis with aortic regurgitation. Am. J. Ophthalmol. Case Rep. 2016, 30, 134–136. [Google Scholar] [CrossRef] [PubMed]
- Taylan, A.; Karakas, B.; Gulcu, A.; Birlik, M. Bilateral orbital pseudotumor in a patient with Takayasu arteritis: A case report and review of the literature. Rheumatol. Int. 2016, 36, 743–746. [Google Scholar] [CrossRef] [PubMed]
- Tian, G.; Chen, Q.; Wang, W. Takayasu arteritis presenting as isolated anterior ischemic optic neuropathy. Int. Ophthalmol. 2018, 38, 823–828. [Google Scholar] [CrossRef]
- Topcuoğlu, M.Ş.; Yaliniz, H.; Tokcan, A.; Bozdemir, H.; Sarica, Y. Cerebral Circulation via Right Vertebral Artery in Takayasu’s Arteritis. Asian Cardiovasc. Thorac. Ann. 2000, 8, 268–270. [Google Scholar] [CrossRef]
- Torun, E.S.; Koca, N.; Yalçınkaya, Y.; Artım Esen, B.; Gül, A.; İnanç, M.A. Case of Takayasu Arteritis with Thrombotic Microangiopathy Secondary to Malignant Hypertension Due to Bilateral Renal Artery Stenosis. Open Access Rheumatol. Res. Rev. 2022, 14, 39–42. [Google Scholar] [CrossRef]
- Ueno, A.; Awane, Y.; Wakabayashi, A.; Shimizu, K. Successfully operated obliterative brachiocephalic arteritis (Takayasu) associated with the elongated coarctation. Jpn. Heart J. 1967, 8, 538–544. [Google Scholar] [CrossRef]
- Wu, S.Y.; Chen, C.H.; Cheng, C.C.; Fan, H.C. Takayasu’s Arteritis Presenting as Monocular Visual Loss. Pediatr. Neonatol. 2015, 56, 435–438. [Google Scholar] [CrossRef]
- Zahaf, A.; Anchour, B.B.; Lajmi, H.; Lahdhiri MHHmaied, W. Unusual ocular manifestation revealing Takayasu’s Arteritis. PAMJ-Clin. Med. 2020, 3, 117. [Google Scholar] [CrossRef]
- Zeng, Y.; Duan, J.; Ge, G.; Zhang, M. Therapeutic Management of Ocular Ischemia in Takayasu’s Arteritis: A Case-Based Systematic Review. Front. Immunol. 2022, 12, 5854. [Google Scholar] [CrossRef] [PubMed]
- Numano, F. The story of Takayasu arteritis. Rheumatology 2022, 41, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Uyama, M.; Asayma, K. Retinal vascular changes in Takayasu’s disease (Pulseless disease), occurrence and evolution of the lesion. Doc. Ophthalmol. Proc. Ser. 1976, 9, 549–554. [Google Scholar]
- Arend, W.P.; Michel, B.A.; Bloch, D.A.; Hunder, G.G.; Calabrese, L.H.; Edworthy, S.M.; Fauci, A.S.; Leavitt, R.Y.; Lie, J.T.; Lightfoot, R.W., Jr. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum. 1990, 33, 1129–1134. [Google Scholar] [CrossRef]
- Bolek, E.C.; Kaya Akca, U.; Sari, A.; Sag, E.; Demir, S.; Kilic, L.; Sener, Y.Z.; Aykan, H.H.; Kaya, E.B.; Bilginer, Y.; et al. Is Takayasu’s arteritis more severe in children? Clin. Exp. Rheumatol. 2021, 39, 32–38. [Google Scholar] [CrossRef]
- Clemente, G.; Silva, C.A.; Sacchetti, S.B.; Ferriani, V.P.L.; Oliveira, S.K.; Sztajnbok, F.; Bica, B.E.R.G.; Cavalcanti, A.; Robazzi, T.; Bandeira, M.; et al. Takayasu arteritis in childhood: Misdiagnoses at disease onset and associated diseases. Rheumatol. Int. 2018, 38, 1089–1094. [Google Scholar] [CrossRef]
- Hellmich, B.; Agueda, A.; Monti, S.; Buttgereit, F.; de Boysson, H.; Brouwer, E.; Cassie, R.; Cid, M.C.; Dasgupta, B.; Dejaco, C.; et al. 2018 Update of the EULAR recommendations for the management of large vessel vasculitis. Ann. Rheum. Dis. 2020, 79, 19–30. [Google Scholar] [CrossRef]


{kind=link}
| First Author | Age | Sex | Patient’s Origin (Continent) | New Diagnosis of TA |
|---|---|---|---|---|
| Akhtar [9] | 35 | M | - | No |
| Amer [10] | 26 | M | - | No |
| Anguita [11] | 12 | F | South America | Yes |
| Arya [12] | 45 | F | - | No |
| Austen [13] | 28 | F | Asia | Yes |
| Babu [14] | 31 | F | - | Yes |
| Bajgai [15] | 25 | F | - | Yes |
| Balaskas [16] | 35 | F | Europe | No |
| Bapat [17] | 24 | M | - | Yes |
| Batliwala [18] | 18 | F | Europe | No |
| Becker [19] | 5 | F | - | Yes |
| Bodker [20] | 22 | F | South America | Yes |
| Bouzas [21] | 45 | F | Europe | No |
| Caccamise [22] | 19 | F | - | Yes |
| Chaudhary [23] | 44 | F | South America | Yes |
| Chawla [24] | 28 | M | Asia | Yes |
| Christiansen [25] | 19 | F | Asia | Yes |
| Conrath [26] | 28 | F | Africa | Yes |
| Das [27] | 37 | F | - | Yes |
| Demir [28] | 14 | F | - | Yes |
| Do Vale [29] | 46 | F | - | Yes |
| Dowling [30] | 54 | - | - | Yes |
| Elizalde [31] | 63 | F | - | No |
| Escano [32] | 34 | M | - | No |
| Font [33] | 35 | F | Asia | Yes |
| Gaur [34] | 27 | F | - | Yes |
| Genc [35] | 52 | M | - | Yes |
| Gong [36] | 18 | F | Asia | Yes |
| Guclu [37] | 48 | F | - | Yes |
| Gupta [38] | 18 | M | - | Yes |
| Harada [39] | 34 | F | Asia | Yes |
| Hayasaka [40] | 33 | F | Asia | No |
| Hayasaka [40] | 19 | F | Asia | Yes |
| Herath [41] | 38 | F | Asia | Yes |
| Ibrahim [42] | 39 | F | - | No |
| Jain [43] | 40 | F | Asia | Yes |
| Jain [44] | 39 | F | Asia | Yes |
| Jain [45] | 15 | F | - | No |
| Kaliaperumal [46] | 35 | F | - | Yes |
| Kancherla [47] | 27 | F | - | Yes |
| Kannan [48] | 13 | M | Asia | Yes |
| Kapran [49] | 29 | M | - | Yes |
| Karam [50] | 28 | F | - | Yes |
| Karam [50] | 24 | F | - | Yes |
| Karam [50] | 27 | F | - | Yes |
| Karam [50] | 24 | F | - | Yes |
| Karam [50] | 21 | F | - | Yes |
| Karam [50] | 8 | F | - | Yes |
| Karam [50] | 30 | F | - | Yes |
| Karwatowski [51] | 66 | F | Asia | No |
| Kaushik [52] | 40 | F | - | Yes |
| Kausman [53] | 12 | M | Asia | Yes |
| Kavitha [54] | 40 | F | - | Yes |
| Kim [55] | 25 | F | Asia | Yes |
| Kimura [56] | 41 | M | - | No |
| Kinoshita [57] | 28 | F | - | No |
| Koz [58] | 45 | M | - | Yes |
| Kumar [59] | 65 | M | - | Yes |
| Kuwahara [60] | 57 | F | Asia | No |
| Larrazabal [61] | 26 | F | - | Yes |
| Lee [62] | 23 | F | - | Yes |
| Lee [63] | 28 | F | Asia | Yes |
| Leonard [64] | 37 | F | - | Yes |
| Lewis [65] | 59 | F | - | Yes |
| Lim [66] | 53 | F | - | No |
| Mahajan [67] | 36 | F | - | Yes |
| Mahajan [67] | 14 | F | - | Yes |
| Mahajan [67] | 34 | F | - | Yes |
| Mahajan [67] | 25 | F | - | Yes |
| Mahajan [67] | 30 | F | - | Yes |
| Mahendradas [68] | 18 | F | - | No |
| Mashru [69] | 31 | F | - | Yes |
| Matalia [70] | 16 | F | - | Yes |
| Matsumoto-Otake [71] | 31 | F | - | Yes |
| McDonald [72] | 12 | M | Asia | Yes |
| Milea [73] | 32 | F | Africa | No |
| Moncada [74] | 32 | F | Asia | Yes |
| Nithyanandam [75] | 30 | F | - | No |
| Noel [76] | 58 | F | - | Yes |
| Noel [76] | 48 | M | - | No |
| Noel [76] | 58 | F | - | No |
| Ostler [77] | 47 | M | - | Yes |
| Padhy [78] | 35 | M | - | No |
| Pahwa [79] | 27 | F | Asia | No |
| Pallangyo [80] | 24 | F | Africa | Yes |
| Paterson [81] | 25 | F | - | Yes |
| Paul [82] | 30 | F | Asia | No |
| Pelegrin [83] | 42 | M | Asia | Yes |
| Peter [84] | 37 | F | - | Yes |
| Peter [85] | 25 | F | - | No |
| Peter [85] | 29 | F | - | Yes |
| Peter [85] | 13 | F | - | Yes |
| Peter [85] | 28 | M | - | No |
| Rainer [86] | 30 | F | - | Yes |
| Rahman [87] | 22 | F | Asia | No |
| Rajshri [88] | 50’s | M | - | Yes |
| Ramteke [89] | 48 | F | - | Yes |
| Reddy [90] | 27 | F | - | No |
| Rodriguez [91] | 26 | F | - | Yes |
| Sakthiswary [92] | 20 | F | - | Yes |
| Santhanam [93] | 19 | F | - | Yes |
| Setty [94] | 23 | F | - | Yes |
| Setty [94] | 23 | F | - | Yes |
| Shailaja [95] | 22 | F | - | Yes |
| Shrestha [96] | 20 | F | - | Yes |
| Shukla [97] | 44 | F | Asia | Yes |
| Smith [98] | 36 | F | Asia | Yes |
| Stone [99] | 13 | F | North America | Yes |
| Strauss [100] | 25 | F | Asia | Yes |
| Subira [101] | 32 | F | - | Yes |
| Suematsu [102] | 34 | F | - | Yes |
| Suh [103] | 52 | F | - | Yes |
| Sureja [104] | 48 | F | - | Yes |
| Tani [105] | 42 | M | - | Yes |
| Taylan [106] | 40 | F | - | Yes |
| Tian [107] | 23 | F | Asia | Yes |
| Topcuoglu [108] | 42 | F | - | Yes |
| Torun [109] | 20 | F | - | No |
| Ueno [110] | 17 | F | Asia | No |
| Wu [111] | 13 | F | - | Yes |
| Zahaf [112] | 20 | F | - | Yes |
| Zeng [113] | 29 | F | Asia | No |
| Ophthalmological Symptoms | Number of Cases | % of Cases |
|---|---|---|
| Amaurosis fugax | 31 | 25.4 |
| Diplopia | 2 | 1.6 |
| Orbital pain | 4 | 3.3 |
| Ocular pain | 21 | 17.2 |
| Gradual visual acuity decrease | 64 | 52.5 |
| Sudden visual acuity decrease/loss | 28 | 23.0 |
| Ocular redness | 16 | 13.1 |
| Photophobia | 10 | 8.2 |
| Metamophopsia | 1 | 0.8 |
| Xanthopsia | 1 | 0.8 |
| No eye movement | 1 | 0.8 |
| Ocular Manifestation | Number of Cases | % of Cases |
|---|---|---|
| Retinal ischemia | 70 | 57.4 |
| Hypertensive retinopathy | 7 | 5.7 |
| Scleritis | 9 | 7.4 |
| Keratitis | 3 | 2.5 |
| Atypical Tolosa Hunt syndrome | 1 | 0.8 |
| Retinal artery occlusion | 15 | 12.3 |
| Cataract | 18 | 14.8 |
| Uveitis | 5 | 4.1 |
| Epiretinal membrane | 1 | 0.8 |
| Episcleritis | 1 | 0.8 |
| Optic neuropathy | 22 | 18.0 |
| Facial nerve palsy | 2 | 1.6 |
| Acquired ocular motor apraxia | 1 | 0.8 |
| Retinal vein occlusion | 4 | 3.3 |
| Ptosis | 2 | 1.6 |
| Ophthalmoplegia | 1 | 0.8 |
| Retinal vasculitis | 5 | 4.1 |
| Sterile corneal melt | 1 | 0.8 |
| Multiple evanescent white dot syndrome | 1 | 0.8 |
| Orbital pseudotumor | 1 | 0.8 |
| Exudative retinal detachment | 1 | 0.8 |
| Systemic Treatment | Number of Cases | % of Cases |
|---|---|---|
| Systemic steroids | 84 | 68.9 |
| Vascular procedure | 39 | 32.0 |
| Mycophenolate mofetil | 6 | 4.9 |
| Azathioprine | 8 | 6.6 |
| Cyclophosphamide | 7 | 5.7 |
| Methotrexate | 33 | 27.0 |
| Leflunomide | 1 | 0.8 |
| Acetylsalicylic acid | 22 | 18.0 |
| Monoclonal antibody | 9 | 7.4 |
| Antiplatelet drugs | 9 | 7.4 |
| Anticoagulants | 9 | 7.4 |
| Antihypertensives | 12 | 9.8 |
| Age Range | Number of Patients | % of Patients |
|---|---|---|
| 0–10 | 2 | 1.6 |
| 11–20 | 24 | 19.7 |
| 21–30 | 41 | 33.6 |
| 31–40 | 28 | 23.0 |
| 41–50 | 15 | 12.3 |
| 51–60 | 9 | 7.4 |
| 61–70 | 3 | 2.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szydełko-Paśko, U.; Przeździecka-Dołyk, J.; Nowak, Ł.; Małyszczak, A.; Misiuk-Hojło, M. Ocular Manifestations of Takayasu’s Arteritis—A Case-Based Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 3745. https://doi.org/10.3390/jcm12113745
Szydełko-Paśko U, Przeździecka-Dołyk J, Nowak Ł, Małyszczak A, Misiuk-Hojło M. Ocular Manifestations of Takayasu’s Arteritis—A Case-Based Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(11):3745. https://doi.org/10.3390/jcm12113745
Chicago/Turabian StyleSzydełko-Paśko, Urszula, Joanna Przeździecka-Dołyk, Łukasz Nowak, Artur Małyszczak, and Marta Misiuk-Hojło. 2023. "Ocular Manifestations of Takayasu’s Arteritis—A Case-Based Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 11: 3745. https://doi.org/10.3390/jcm12113745
APA StyleSzydełko-Paśko, U., Przeździecka-Dołyk, J., Nowak, Ł., Małyszczak, A., & Misiuk-Hojło, M. (2023). Ocular Manifestations of Takayasu’s Arteritis—A Case-Based Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(11), 3745. https://doi.org/10.3390/jcm12113745