

Electrocardiographic Markers of Adverse Left Ventricular Remodeling and Myocardial Fibrosis in Severe Aortic Stenosis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
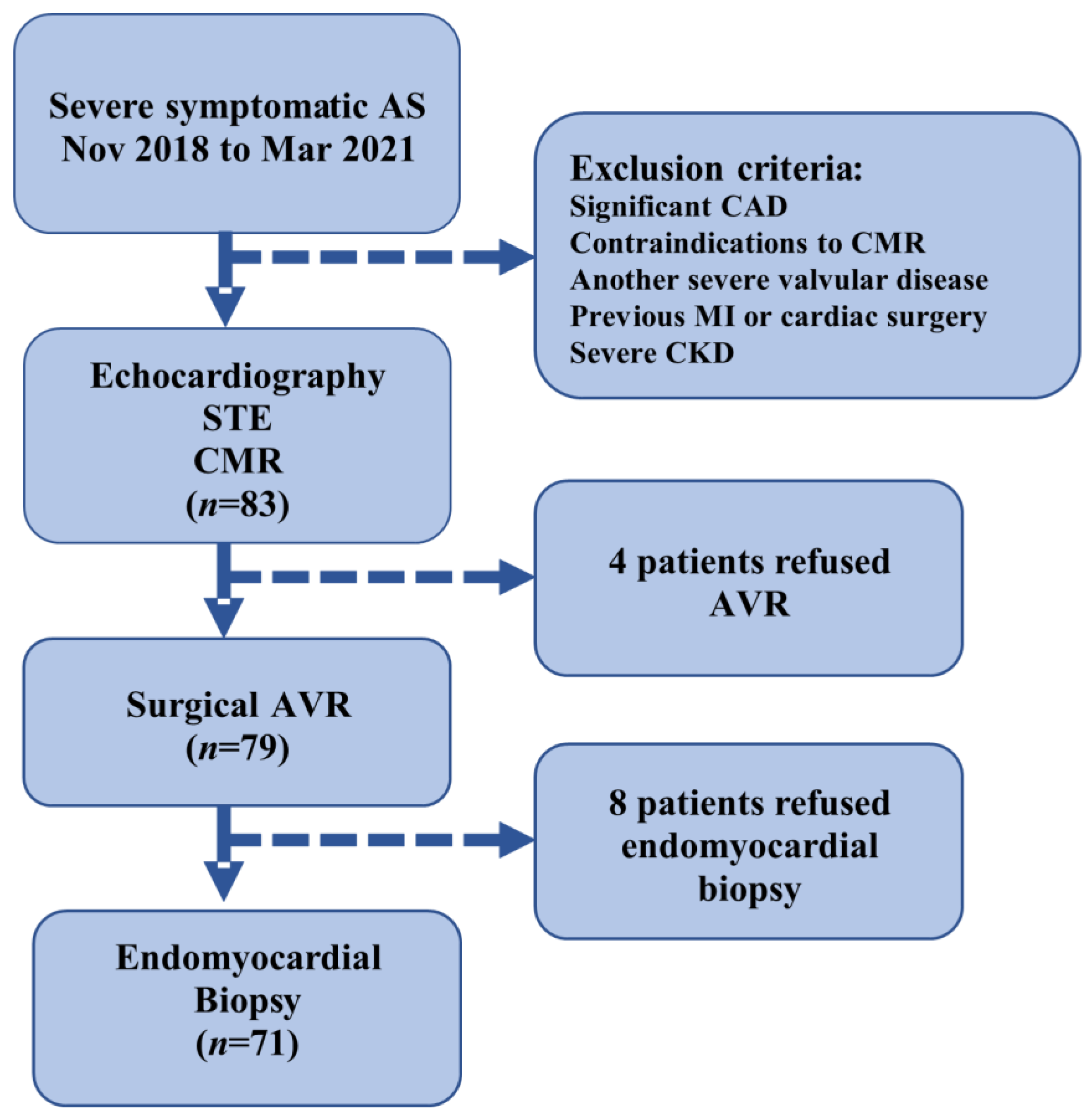
2.1. Study Design and Population
2.2. Inclusion/Exclusion Criteria
2.3. Cardiac Imaging
2.3.1. ECG Analysis
2.3.2. Echocardiography
2.3.3. CMR Protocol
2.4. Histological Analysis
2.5. Statistical Analysis
3. Results
3.1. ECG Strain and LV Remodeling
3.2. ECG Strain and Myocardial Fibrosis
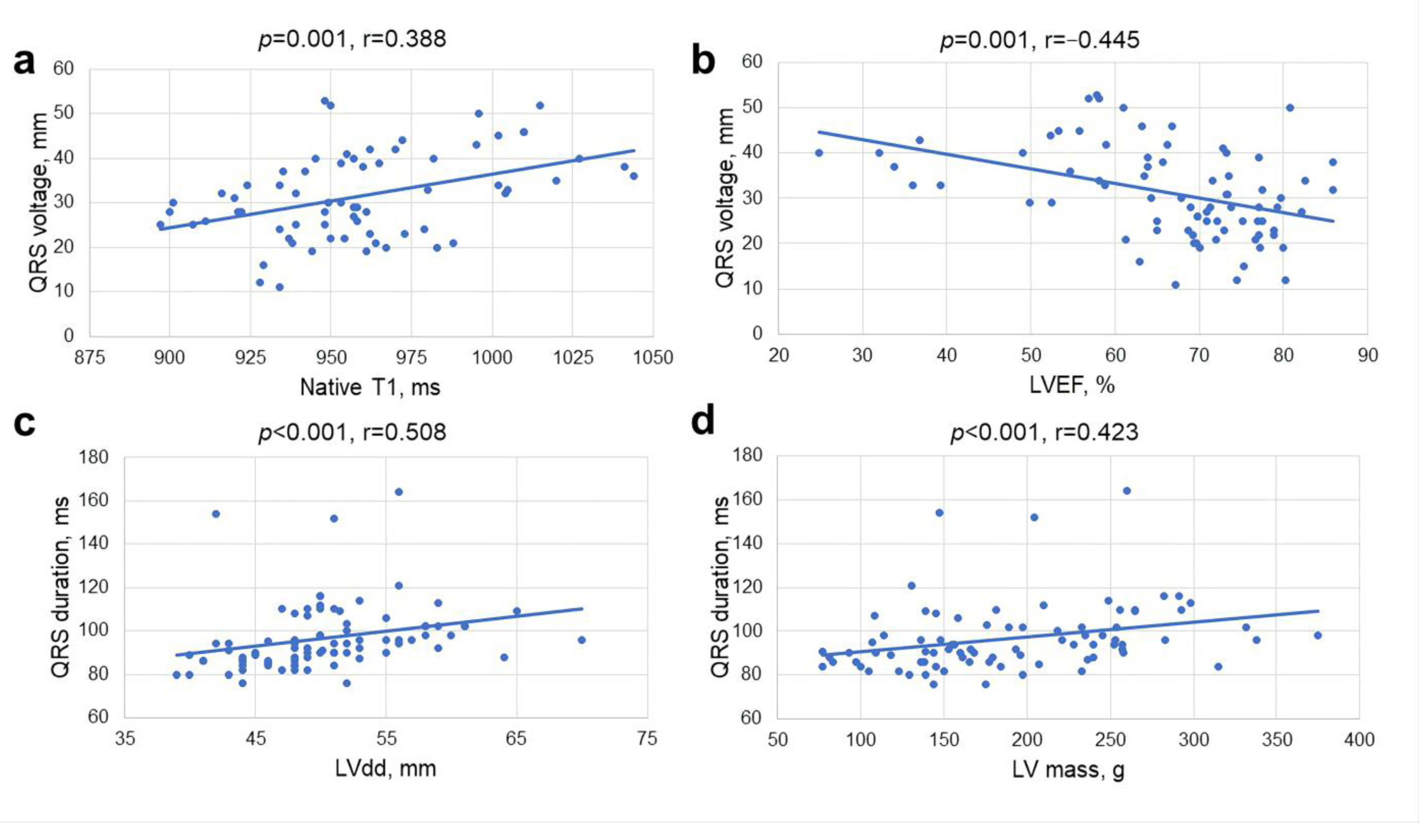
3.3. Analysis of Associations
3.4. ECG Parameters as Independent Prognostic Factors
3.5. ECG Changes at Follow-Up
4. Discussion
4.1. ECG Strain and LV Remodeling
4.2. ECG Strain and Myocardial Fibrosis
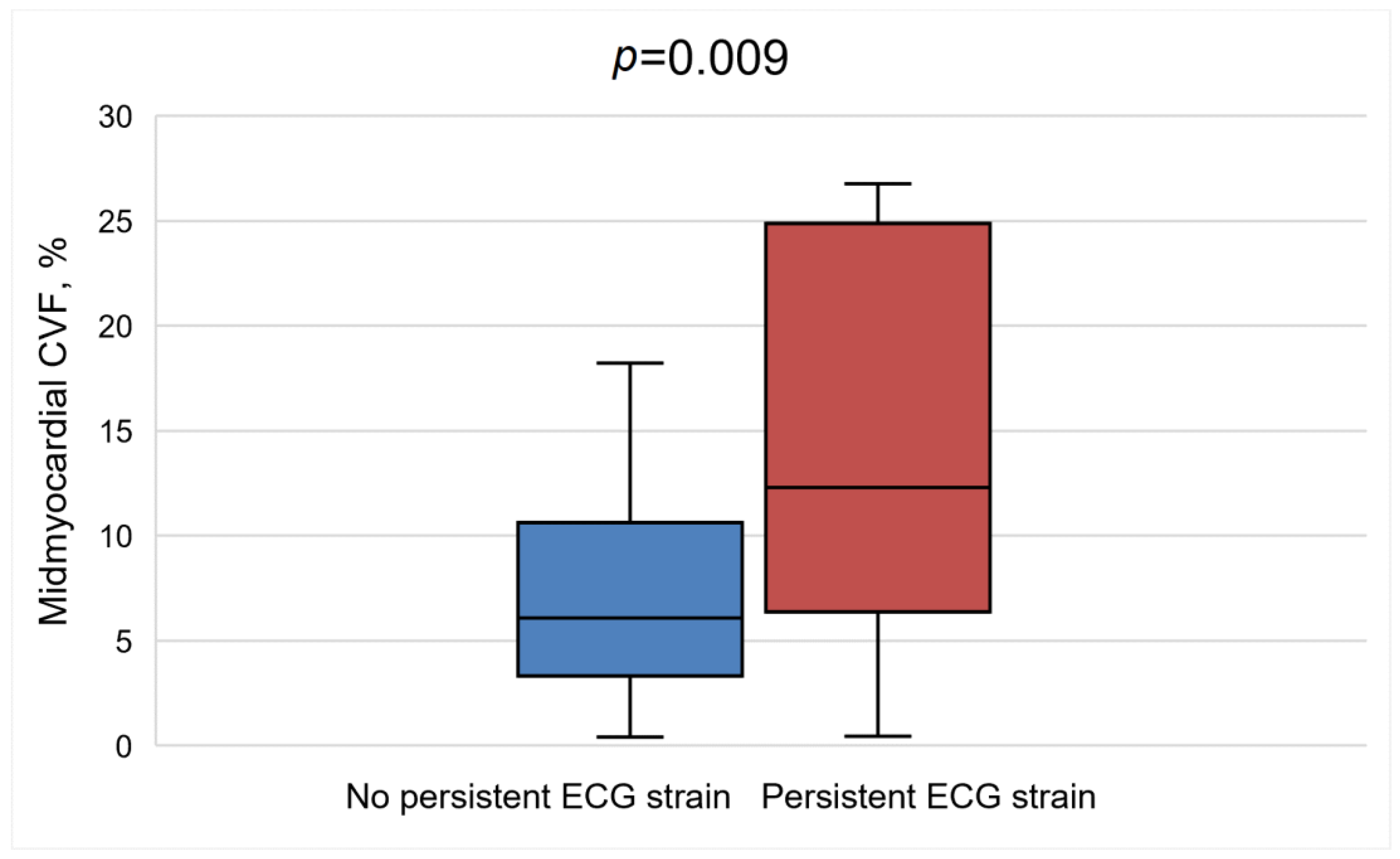
4.3. ECG Strain at Follow-Up
4.4. Prognostic Value of ECG Strain
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AS | aortic stenosis |
| AVA | aortic valve area |
| AV | aortic valve |
| AVR | aortic valve replacement |
| BNP | brain natriuretic peptide |
| CAD | coronary artery disease |
| CMR | cardiovascular magnetic resonance |
| CVF | collagen volume fraction |
| ECG | electrocardiography |
| ECV | extracellular volume |
| GLS | global longitudinal strain |
| Hs-Tn-I | high-sensitivity troponin I |
| LGE | late gadolinium enhancement |
| LV | left ventricle |
| LVEF | left ventricular ejection fraction |
| TAVI | transcatheter aortic valve implantation |
References
- Gladding, P.A.; Hewitt, W.; Schlegel, T.T. Going Deep with ECG and Aortic Stenosis: Touchdown or Incomplete Pass? J. Am. Heart Assoc. 2020, 9, e016193. [Google Scholar] [CrossRef]
- Açıkgöz, E.; Yaman, B.; Açıkgöz, S.K.; Topal, S.; Tavil, Y.; Boyacı, N.B. Fragmented QRS can predict severity of aortic stenosis. Ann. Noninvasive Electrocardiol. 2015, 20, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Dweck, M.R.; Joshi, S.; Murigu, T.; Gulati, A.; Alpendurada, F.; Jabbour, A.; Maceira, A.; Roussin, I.; Northridge, D.B.; Kilner, P.J.; et al. Left ventricular remodeling and hypertrophy in patients with aortic stenosis: Insights from cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2012, 14, 50. [Google Scholar] [CrossRef] [PubMed]
- Everett, R.J.; Tastet, L.; Clavel, M.-A.; Chin, C.W.; Capoulade, R.; Vassiliou, V.S.; Kwiecinski, J.; Gomez, M.; van Beek, E.J.; White, A.C.; et al. Progression of Hypertrophy and Myocardial Fibrosis in Aortic Stenosis: A Multicenter Cardiac Magnetic Resonance Study. Circ. Cardiovasc. Imaging 2018, 11, e007451. [Google Scholar] [CrossRef]
- Conrad, C.H.; Brooks, W.W.; Hayes, J.A.; Sen, S.; Robinson, K.G.; Bing, O.H. Myocardial fibrosis and stiffness with hypertrophy and heart failure in the spontaneously hypertensive rat. Circulation 1995, 91, 161–170. [Google Scholar] [CrossRef]
- Capasso, J.M.; Robinson, T.F.; Anversa, P. Alterations in collagen cross-linking impair myocardial contractility in the mouse heart. Circ. Res. 1989, 65, 1657–1664. [Google Scholar] [CrossRef] [PubMed]
- Schewel, J.; Kuck, K.H.; Frerker, C.; Schmidt, T.; Schewel, D. Outcome of aortic stenosis according to invasive cardiac damage staging after transcatheter aortic valve replacement. Clin. Res. Cardiol. 2021, 110, 699–710. [Google Scholar] [CrossRef]
- Mino, T.; Kimura, S.; Kitaura, A.; Iwamoto, T.; Yuasa, H.; Chiba, Y.; Nakao, S. Can left ventricular hypertrophy on electrocardiography detect severe aortic valve stenosis? PLoS ONE 2020, 15, e0241591. [Google Scholar] [CrossRef]
- Dweck, M.R.; Joshi, S.; Murigu, T.; Alpendurada, F.; Jabbour, A.; Melina, G.; Banya, W.; Gulati, A.; Roussin, I.; Raza, S.; et al. Midwall fibrosis is an independent predictor of mortality in patients with aortic stenosis. J. Am. Coll. Cardiol. 2011, 58, 1271–1279. [Google Scholar] [CrossRef]
- Yamabe, S.; HERO (Hiroshima Heart Study Group) Investigators; Dohi, Y.; Higashi, A.; Kinoshita, H.; Sada, Y.; Hidaka, T.; Kurisu, S.; Shiode, N.; Kihara, Y. Clinical value of regression of electrocardiographic left ventricular hypertrophy after aortic valve replacement. Heart Vessel. 2016, 31, 1497–1503. [Google Scholar] [CrossRef]
- Kurisu, S.; Inoue, I.; Kawagoe, T.; Ishihara, M.; Shimatani, Y.; Nakama, Y.; Maruhashi, T.; Kagawa, E.; Dai, K.; Matsushita, J.; et al. The decrease in QRS amplitude after aortic valve replacement in patients with aortic valve stenosis. J. Electrocardiol. 2009, 42, 410–413. [Google Scholar] [CrossRef] [PubMed]
- Musa, T.A.; Treibel, T.A.; Vassiliou, V.S.; Captur, G.; Singh, A.; Chin, C.; Dobson, L.E.; Pica, S.; Loudon, M.; Malley, T.; et al. Myocardial Scar and Mortality in Severe Aortic Stenosis. Circulation 2018, 138, 1935–1947. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Rev. Esp. Cardiol. (Engl. Ed.) 2022, 75, 524. [Google Scholar] [CrossRef] [PubMed]
- Heger, J.; Trimaille, A.; Kibler, M.; Marchandot, B.; Peillex, M.; Carmona, A.; Matsushita, K.; Trinh, A.; Reydel, A.; Zeyons, F.; et al. Electrocardiographic Strain Pattern Is a Major Determinant of Rehospitalization for Heart Failure after Transcatheter Aortic Valve Replacement. J. Am. Heart Assoc. 2021, 10, e014481. [Google Scholar] [CrossRef]
- Chin, C.W.; Semple, S.; Malley, T.; White, A.C.; Mirsadraee, S.; Weale, P.J.; Prasad, S.; Newby, D.E.; Dweck, M.R. Optimization and comparison of myocardial T1 techniques at 3T in patients with aortic stenosis. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 556–565. [Google Scholar] [CrossRef] [PubMed]
- Barone-Rochette, G.; Piérard, S.; de Ravenstein, C.D.M.; Seldrum, S.; Melchior, J.; Maes, F.; Pouleur, A.-C.; Vancraeynest, D.; Pasquet, A.; Vanoverschelde, J.-L.; et al. Prognostic significance of LGE by CMR in aortic stenosis patients undergoing valve replacement. J. Am. Coll. Cardiol. 2014, 64, 144–154. [Google Scholar] [CrossRef]
- Weidemann, F.; Herrmann, S.; Störk, S.; Niemann, M.; Frantz, S.; Lange, V.; Beer, M.; Gattenlöhner, S.; Voelker, W.; Ertl, G.; et al. Impact of myocardial fibrosis in patients with symptomatic severe aortic stenosis. Circulation 2009, 120, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Saeed, S.; Wasim, D.; Mohamed Ali, A.; Bleie, Ø.; Chambers, J.B. The electrocardiogram: Still a useful marker for LV fibrosis in aortic stenosis. J. Electrocardiol. 2021, 65, 82–87. [Google Scholar] [CrossRef]
- Shah, A.S.; Chin, C.W.; Vassiliou, V.; Cowell, S.J.; Doris, M.; Kwok, T.C.; Semple, S.; Zamvar, V.; White, A.C.; McKillop, G.; et al. Left ventricular hypertrophy with strain and aortic stenosis. Circulation 2014, 130, 1607–1616. [Google Scholar] [CrossRef]
- Guinot, B.; Magne, J.; Le Guyader, A.; Bégot, E.; Bourgeois, A.; Piccardo, A.; Marsaud, J.-P.; Mohty, D.; Aboyans, V. Usefulness of Electrocardiographic Strain to Predict Survival after Surgical Aortic Valve Replacement for Aortic Stenosis. Am. J. Cardiol. 2017, 120, 1359–1365. [Google Scholar] [CrossRef]
- Greve, A.M.; Boman, K.; Gohlke-Baerwolf, C.; Kesäniemi, Y.A.; Nienaber, C.; Ray, S.; Egstrup, K.; Rossebø, A.B.; Devereux, R.B.; Køber, L.; et al. Clinical Implications of Electrocardiographic Left Ventricular Strain and Hypertrophy in Asymptomatic Patients with Aortic Stenosis. Circulation 2012, 125, 346–353. [Google Scholar] [CrossRef]
- Coisne, A.; Ninni, S.; Pontana, F.; Aghezzaf, S.; Janvier, F.; Mouton, S.; Ridon, H.; Ortmans, S.; Seunes, C.; Wautier, M.; et al. Clinical significance of electrocardiographic markers of myocardial damage prior to aortic valve replacement. Int. J. Cardiol. 2020, 307, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Sokolow, M.; Lyon, T.P. The ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Am. Heart J. 1949, 37, 161–186. [Google Scholar] [CrossRef] [PubMed]
- Hancock, E.W.; Deal, B.J.; Mirvis, D.M.; Okin, P.; Kligfield, P.; Gettes, L.S.; Bailey, J.J.; Childers, R.; Gorgels, A.; Josephson, M.; et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: Part V: Electrocardiogram changes associated with cardiac chamber hypertrophy: A scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. J. Am. Coll. Cardiol. 2009, 53, 992–1002. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Edvardsen, T.; Goldstein, S.; Lancellotti, P.; LeFevre, M.; Miller, F.; Otto, C.M. Recommendations on the echocardiographic assessment of aortic valve stenosis: A focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 254–275. [Google Scholar] [CrossRef]
- Voigt, J.-U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1–11. [Google Scholar] [CrossRef]
- Taylor, A.J.; Salerno, M.; Dharmakumar, R.; Jerosch-Herold, M. T1 Mapping: Basic Techniques and Clinical Applications. JACC Cardiovasc. Imaging 2016, 9, 67–81. [Google Scholar] [CrossRef]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reson. 2017, 19, 75. [Google Scholar] [CrossRef]
- Ugander, M.; Oki, A.J.; Hsu, L.-Y.; Kellman, P.; Greiser, A.; Aletras, A.H.; Sibley, C.T.; Chen, M.Y.; Bandettini, W.P.; Arai, A.E. Extracellular volume imaging by magnetic resonance imaging provides insights into overt and sub-clinical myocardial pathology. Eur. Heart J. 2012, 33, 1268–1278. [Google Scholar] [CrossRef]
- Horai, Y.; Mizukawa, M.; Nishina, H.; Nishikawa, S.; Ono, Y.; Takemoto, K.; Baba, N. Quantification of histopathological findings using a novel image analysis platform. J. Toxicol. Pathol. 2019, 32, 319–327. [Google Scholar] [CrossRef]
- Ogah, O.; Oladapo, O.; Adebiyi, A.; Salako, B.; Falase, A.; Adebayo, A.; Aje, A.; Ojji, D. Electrocardiographic left ventricular hypertrophy with strain pattern: Prevalence, mechanisms and prognostic implications. Cardiovasc. J. Afr. 2008, 19, 39–45. [Google Scholar] [PubMed]
- Greve, A.M.; Gerdts, E.; Boman, K.; Gohlke-Baerwolf, C.; Rossebø, A.B.; Hammer-Hansen, S.; Køber, L.; Willenheimer, R.; Wachtell, K. Differences in cardiovascular risk profile between electrocardiographic hypertrophy versus strain in asymptomatic patients with aortic stenosis (from SEAS data). Am. J. Cardiol. 2011, 108, 541–547. [Google Scholar] [CrossRef]
- Al-Hijji, M.; Alkhouli, M.; Alqahtani, F.; Nkomo, V.T.; Greason, K.L.; Holmes, D.R. Prognostic Implication of Electrocardiographic Left Ventricular Strain in Patients Who Underwent Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2018, 122, 1042–1046. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, T.; Shiomi, H.; Kosuge, M.; Morimoto, T.; Nakatsuma, K.; Nishiga, M.; Sasa, T.; Saito, N.; Kimura, T. Prognostic Significance of ST-Segment Elevation in Leads V₁–₂ in Patients with Severe Aortic Stenosis. Circ. J. 2016, 80, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Greve, A.M.; Dalsgaard, M.; Bang, C.N.; Egstrup, K.; Rossebø, A.B.; Boman, K.; Cramariuc, D.; Nienaber, C.A.; Ray, S.; Gohlke-Baerwolf, C.; et al. Usefulness of the electrocardiogram in predicting cardiovascular mortality in asymptomatic adults with aortic stenosis (from the Simvastatin and Ezetimibe in Aortic Stenosis Study). Am. J. Cardiol. 2014, 114, 751–756. [Google Scholar] [CrossRef]
- Maanja, M.; Wieslander, B.; Schlegel, T.T.; Bacharova, L.; Abu Daya, H.; Fridman, Y.; Wong, T.C.; Schelbert, E.B.; Ugander, M. Diffuse Myocardial Fibrosis Reduces Electrocardiographic Voltage Measures of Left Ventricular Hypertrophy Independent of Left Ventricular Mass. J. Am. Heart Assoc. 2017, 6, e003795. [Google Scholar] [CrossRef]
- Balčiūnaitė, G.; Besusparis, J.; Palionis, D.; Žurauskas, E.; Skorniakov, V.; Janušauskas, V.; Zorinas, A.; Zaremba, T.; Valevičienė, N.; Šerpytis, P.; et al. Exploring myocardial fibrosis in severe aortic stenosis: Echo, CMR and histology data from FIB-AS study. Int. J. Cardiovasc. Imaging 2022, 38, 1555–1568, ahead of print. [Google Scholar] [CrossRef]
- Cameli, M.; Mondillo, S.; Righini, F.M.; Lisi, M.; Dokollari, A.; Lindqvist, P.; Maccherini, M.; Henein, M. Left Ventricular Deformation and Myocardial Fibrosis in Patients with Advanced Heart Failure Requiring Transplantation. J. Card. Fail. 2016, 22, 901–907. [Google Scholar] [CrossRef]
- Le, T.-T.; Huang, W.; Singh, G.K.; Toh, D.-F.; Ewe, S.H.; Tang, H.C.; Loo, G.; Bryant, J.A.; Ang, B.; Tay, E.L.-W.; et al. Echocardiographic Global Longitudinal Strain Is Associated with Myocardial Fibrosis and Predicts Outcomes in Aortic Stenosis. Front. Cardiovasc. Med. 2021, 8, 750016. [Google Scholar] [CrossRef]
- Rank, N.; Stoiber, L.; Nasser, M.; Tanacli, R.; Stehning, C.; Knierim, J.; Schoenrath, F.; Pieske, B.; Falk, V.; Kuehne, T.; et al. Assessment of 10-Year Left-Ventricular-Remodeling by CMR in Patients Following Aortic Valve Replacement. Front. Cardiovasc. Med. 2021, 8, 645693. [Google Scholar] [CrossRef] [PubMed]
- Treibel, T.A.; Kozor, R.; Schofield, R.; Benedetti, G.; Fontana, M.; Bhuva, A.N.; Sheikh, A.; López, B.; González, A.; Manisty, C.; et al. Reverse Myocardial Remodeling Following Valve Replacement in Patients with Aortic Stenosis. J. Am. Coll. Cardiol. 2018, 71, 860–871. [Google Scholar] [CrossRef]
- Izumi, C.; Kitai, T.; Kume, T.; Onishi, T.; Yuda, S.; Hirata, K.; Yamashita, E.; Kawata, T.; Nishimura, K.; Takeuchi, M.; et al. Effect of Left Ventricular Reverse Remodeling on Long-term Outcomes after Aortic Valve Replacement. Am. J. Cardiol. 2019, 124, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Gavina, C.; Falcão-Pires, I.; Pinho, P.; Manso, M.-C.; Gonçalves, A.; Rocha-Gonçalves, F.; Leite-Moreira, A. Relevance of residual left ventricular hypertrophy after surgery for isolated aortic stenosis. Eur. J. Cardiothorac. Surg. 2016, 49, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, A.; Weber, M.; von Depka, A.; Tabata, N.; Shamekhi, J.; Al-Kassou, B.; Nickenig, G.; Werner, N.; Sinning, J.-M.; Sedaghat, A. Outcomes of myocardial fibrosis in patients undergoing transcatheter aortic valve replacement. EuroIntervention 2020, 15, 1417–1423. [Google Scholar] [CrossRef]
- Minamino-Muta, E.; Kato, T.; Morimoto, T.; Taniguchi, T.; Shiomi, H.; Nakatsuma, K.; Shirai, S.; Ando, K.; Kanamori, N.; Murata, K.; et al. Causes of Death in Patients with Severe Aortic Stenosis: An Observational study. Sci. Rep. 2017, 7, 14723. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 83) | No ECG Strain (n = 47) | ECG Strain (n = 36) | p-Value |
|---|---|---|---|---|
| Age, yrs | 66.5 ± 8.6 | 67.2 ± 8.3 | 65.4 ± 9.1 | 0.357 |
| Male gender | 35 (42.2) | 13 (27.7) | 22 (61.1) | 0.002 |
| BSA, m2 | 1.9 ± 0.2 | 1.9 ± 0.2 | 2 ± 0.2 | 0.165 |
| Systolic BP, mm Hg | 149.6 ± 24.8 | 157.7 ± 23.7 | 139.0 ± 22.3 | <0.001 |
| Diastolic BP, mm Hg | 84.0 ± 11.7 | 88.4 ± 10.1 | 78.2 ± 11.2 | <0.001 |
| Comorbidities | ||||
| Hypertension | 73 (88) | 42 (89.4) | 31 (86.1) | 0.740 |
| Dyslipidemia | 67 (80.7) | 40 (85.1) | 27 (75) | 0.247 |
| Unobstructive CAD | 39 (47) | 20 (42.6) | 19 (52.8) | 0.355 |
| Diabetes mellitus | 15 (18.1) | 10 (21.3) | 5 (13.9) | 0.389 |
| Risk scores | ||||
| STS-PROM, % | 1.6 (1.2–2.4) | 1.8 (1.4–2.5) | 1.3 (1.0–1.9) | 0.004 |
| EuroSCORE II, % | 1 (0.7–1.6) | 1.1 (0.8–1.6) | 1 (0.7–1.7) | 0.695 |
| Functional status | ||||
| NYHA f. cl. * | ||||
| I–II | 40 (48.2) | 26 (55.3) | 14 (38.9) | 0.138 * |
| III–IV | 43 (51.8) | 21 (44.7) | 22 (61.1) | |
| MLHFQ score | 32.5 (18.5–52.8) | 40.5 (19–56) | 30 (17–40.8) | 0.306 |
| 6 MWT, m | 369 (300–420) | 360 (294.8–420) | 388.5 (322.5–420) | 0.489 |
| Blood tests | ||||
| eGFR, ml/min/1.73 m2 | 85 (69–90) | 85 (69–90) | 85 (67.5–90) | 0.875 |
| Hs-Tn-I, pg/L | 9.1 (5–18.7) | 6 (4–13) | 15.5 (9–29) | <0.001 |
| BNP, pg/L | 130 (65.2–361.9) | 80.2 (46.5–163.2) | 297.2 (117.7–812.8) | <0.001 |
| ECG parameters | ||||
| Heart rate, beats/min | 75 (65–86) | 75 (68–86) | 75.5 (64.3–87.5) | 0.890 |
| PQ duration, ms | 165 (153.5–180) | 162 (150–176) | 168 (160–184) | 0.067 |
| QRS duration, ms | 94 (86–102) | 90 (85–98) | 96 (90.3–108.5) | 0.016 |
| S-L, mm | 30.9 ± 9.9 | 25.3 ± 7.3 | 38.1 ± 8.1 | <0.001 |
| S-L ≥ 35 mm, % | 28 (33.7) | 6 (12.8) | 22 (61.1) | <0.001 |
| All Patients (n = 83) | No ECG Strain (n = 47) | ECG Strain (n = 36) | p-Value | |
|---|---|---|---|---|
| Echocardiography Data | ||||
| AVA, cm2 | 0.84 ± 0.2 | 0.85 ± 0.2 | 0.83 ± 0.2 | 0.612 |
| AVA index, cm2/m2 | 0.45 (0.35–0.53) | 0.47 (0.4–0.53) | 0.41 (0.33–0.53) | 0.230 |
| Peak AV velocity, m/s | 4.9 (4.4–5.3) | 4.5 (4.2–5.2) | 5.0 (4.7–5.5) | 0.008 |
| Mean AV gradient, mm Hg | 54.9 (44.4–70.0) | 49 (42.0–64.0) | 60.5 (52.5–77.9) | 0.003 |
| IVSd, mm | 13 (12–14) | 12 (11–13) | 13.5 (13–15) | <0.001 |
| PWd, mm | 11.5 (10–12) | 11 (10–12) | 12 (11–13) | <0.001 |
| LVdd, mm | 51.2 ± 5.4 | 49.4 ± 4.2 | 53.6 ± 5.9 | <0.001 |
| LVsd, mm | 32.7 ± 5.9 | 30.5 ± 4.5 | 35.7 ± 6.3 | <0.001 |
| LV mass, g | 130.2 ± 30.7 | 116.4 ± 20.7 | 148.3 ± 32.4 | <0.001 |
| E/A | 1.1 ± 0.4 | 1.2 ± 0.4 | 1.1 ± 0.5 | 0.132 |
| E/e’ septal | 16.4 (12.7–20.9) | 15 (11.6–18.3) | 17 (13.4–25) | 0.011 |
| E/e’ lateral | 13 (10.3–17) | 12.5 (9.7–17.6) | 13.4 (10.4–16.5) | 0.388 |
| E/e’ mean | 14.4 (11.6–18.3) | 14 (10.8–18.3) | 15 (12.2–19) | 0.107 |
| LA volume index, mL/m2 | 47.3 (40.6–55.3) | 43.5 (38.3–53) | 51.4 (44.8–56.9) | 0.004 |
| Estimated PASP, mm Hg | 33 (29–43) | 33 (29.3–39.5) | 35 (29–65) | 0.272 |
| GLS, % * | −18 ± 5 | −20.1 ± 3.8 | −15.2 ± 4.9 | <0.001 |
| CMR data | ||||
| IVSd, mm | 13.3 ± 2 | 12.7 ± 1.9 | 14.2 ± 1.9 | <0.001 |
| PWd, mm | 10.5 ± 1.9 | 9.8 ± 1.7 | 11.5 ± 1.8 | <0.001 |
| LVdd, mm | 50.4 ± 6.1 | 48.8 ± 5.2 | 52.4 ± 6.7 | 0.008 |
| LVsd, mm | 33.7 ± 8.1 | 30.9 ± 6.6 | 37.2 ± 8.6 | <0.001 |
| LVEDV index, mL/m2 | 70.6 (61.5–80.6) | 63.1 (54.9–74.6) | 78.9 (70.4–99.8) | <0.001 |
| LVESV index, mL/m2 | 20.6 (14.9–30.8) | 16 (12.9–21.7) | 29.8 (18.4–45.3) | <0.001 |
| LVEF, % | 66.7 ± 12.8 | 71.5 ± 7.7 | 60.6 ± 15.4 | <0.001 |
| LVEF < 50%, n (%) | 9 (10.8) | 1 (2.1) | 8 (22.2) | 0.009 |
| LV mass, g | 189.9 ± 68.1 | 152.3 ± 45.1 | 237.9 ± 62.2 | <0.001 |
| LV mass index, g/m2 | 92.5 (76.8–119.3) | 79.3 (61.8–90.9) | 119.8 (109.7–137.3) | <0.001 |
| LGE prevalence | 61 (73.5) | 31 (66) | 30 (83.3) | 0.075 |
| Native T1, ms # | 959.6 ± 33.7 | 946.5 ± 28.2 | 974.8 ± 33.6 | <0.001 |
| ECV, % # | 23.1 (20.8–24.9) | 23 (20.7–24.9) | 23.3 (21.2–25.2) | 0.821 |
| Histology data (n = 71) | ||||
| CVF total, % & | 16.1 ± 9.4 | 15.7 ± 8.7 | 16.6 ± 10.2 | 0.679 |
| CVF midmyocardial, % & | 7 (3.8–11.9) | 5.9 (3.6–9.1) | 8.8 (4–12.6) | 0.155 |
| CVF subendocardial, % & | 21.6 ± 12.3 | 21.4 ± 10.9 | 21.8 ± 13.8 | 0.872 |
| Variable | LV Mass Index | Native T1 | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Male sex | 3.67 (1.39–9.69) | 0.009 | 2.91 (0.89–9.56) | 0.078 | 1.07 (0.33–3.45) | 0.914 | - | - |
| Age, yrs | 0.95 (0.90–1.00) | 0.053 | - | - | 0.96 (0.90–1.03) | 0.268 | - | - |
| Hs-Tn-I, pg/L | 1.00 (0.99–1.00) | 0.497 | - | - | 1.00 (0.99–1.00) | 0.697 | - | - |
| BNP, pg/L | 1.00 (1.00–1.01) | 0.009 | 1.00 (1.00–1.01) | 0.309 | 1.00 (1.00–1.00) | 0.600 | - | - |
| LVEF, % | 0.91 (0.86–0.97) | 0.001 | 0.94 (0.87–1.02) | 0.110 | 0.945 (0.90–0.99) | 0.016 | 1.00 (0.92–1.08) | 0.931 |
| GLS, % | 0.73 (0.62–0.87) | <0.001 | - | - | 0.86 (0.75–0.99) | 0.036 | 0.93 (0.74–1.17) | 0.546 |
| QRS voltage | 1.09 (1.03–1.15) | 0.002 | 0.98 (0.91–1.06) | 0.679 | 1.10 (1.03–1.18) | 0.006 | 1.08 (0.99–1.18) | 0.093 |
| PQ duration, ms | 1.01 (0.99–1.03) | 0.262 | - | - | 1.00 (0.98–1.02) | 0.885 | - | - |
| QRS duration, ms | 1.02 (0.99–1.05) | 0.296 | - | - | 1.03 (0.99–1.07) | 0.129 | - | - |
| ECG strain | 12.89 (3.90–42.55) | <0.001 | 7.10 (1.46–34.48) | 0.015 | 4.40 (1.23–15.72) | 0.023 | 1.34 (0.26–7.03) | 0.726 |
| Variables | Baseline (n = 83) | 3-Month Follow-Up (n = 76) | 12-Month Follow-Up (n = 59) |
|---|---|---|---|
| PQ duration, ms | 165 (153.5–180) | 164 (145.5–184) | 163 (144.5–191.5) |
| QRS duration, ms | 94 (86–102) | 98.5 (88–115.5) * | 96 (86–108) |
| S-L, mm | 30 (23–39) | 23 (18.5–27) * | 19.5 (16–24) * |
| ECG strain, n (%) | 36 (43.4) | 26 (34.2) | 10 (16.9) * |
| Variable | Patients without Persistent ECG Strain (n = 73) | Patients with Persistent ECG Strain (n = 10) | p-Value |
|---|---|---|---|
| Blood Tests | |||
| eGFR, ml/min/1.73 m2 | 86 (73.5–90) | 67.5 (60.3–80.8) | 0.019 |
| Hs-Tn-I, pg/L | 9 (5–16) | 17 (11.3–36.3) | 0.065 |
| BNP, pg/L | 118.8 (60.7–285) | 772.4 (148.3–1128.9) | 0.005 |
| Echocardiography data | |||
| AVA, cm2 | 0.9 ± 0.2 | 0.7 ± 0.1 | 0.069 |
| AVA index, cm2/m2 | 0.45 ± 0.1 | 0.40 ± 0.1 | 0.220 |
| Peak AV velocity, m/s | 4.9 ± 0.6 | 4.6 ± 0.6 | 0.122 |
| Mean AV gradient, mm Hg | 59.2 ± 17.4 | 52.6 ± 13.4 | 0.249 |
| IVSd, mm | 13 (12–15) | 13 (11–14.3) | 0.949 |
| PWd, mm | 11 (10–12) | 12 (10.5–13.5) | 0.553 |
| LVdd, mm | 50 (47–53) | 56.5 (51.3–58) | 0.014 |
| LVsd, mm | 31.8 ± 5 | 39.1 ± 8.3 | <0.001 |
| LV mass, g | 127.7 ± 29.6 | 153.4 ± 32.1 | 0.023 |
| E/A | 1.2 ± 0.4 | 1 ± 0.6 | 0.299 |
| E/e’ septal | 16.3 (12.7–20.4) | 16.7 (11.7–23.2) | 0.994 |
| E/e’ lateral | 13.3 (10.4–17.1) | 10.8 (9–22.2) | 0.558 |
| E/e’ mean | 14.5 (11.8–18.3) | 12.7 (11.1–22) | 0.716 |
| LA volume index, mL/m2 | 46.2 (29.6–55) | 54.5 (48.6–56.8) | 0.118 |
| Estimated PASP, mm Hg | 33 (29.5–40.5) | 54 (26–70) | 0.250 |
| GLS, % * | 18.6 ± 4.4 | 12.8 ± 6.7 | <0.001 |
| CMR data | |||
| IVSd, mm | 13.3 ± 2.1 | 13.6 ± 1.9 | 0.648 |
| PWd, mm | 10 (9–12) | 10 (9.5–11.4) | 0.861 |
| LVdd, mm | 49 (46–52.5) | 55.5 (50.8–58.8) | 0.013 |
| LVsd, mm | 32.6 ± 7.5 | 41.4 ± 8.8 | <0.001 |
| LVEDV index, mL/m2 | 70.5 (61.1–78.2) | 99.2 (63.7–129) | 0.010 |
| LVESV index, mL/m2 | 18.7 (14.7–28.5) | 52.7 (18.9–83.8) | 0.003 |
| LVEF, % | 68.9 ± 10.3 | 51 ± 18.2 | <0.001 |
| LVEF < 50%, n (%) | 4 (5.5) | 5 (50) | <0.001 |
| LV mass, g | 167 (138.3–239) | 236 (185.8–255) | 0.072 |
| LV mass index, g/m2 | 86.4 (75.5–118.5) | 119.8 (101.5–131.9) | 0.052 |
| RVEDV, mL | 124.3 ± 31.5 | 132.5 ± 28.6 | 0.440 |
| RVESV, mL | 43.5 (35–58.6) | 57.7 (50.2–71.5) | 0.020 |
| RVEF, % | 62.1 ± 7.5 | 52.5 ± 16.3 | 0.002 |
| LGE prevalence | 53 (72.6) | 8 (80) | 1.000 |
| Native T1, ms # | 955 (934.5–976) | 965 (943–1004.3) | 0.374 |
| ECV, % # | 22.6 ± 3.7 | 23.7 ± 2.6 | 0.401 |
| Histology data (n = 71) | |||
| CVF total, % & | 15.6 ± 8.4 | 19 ± 14.2 | 0.293 |
| CVF midmyocardial, % & | 7.3 ± 4.7 | 12.5 ± 9.9 | 0.009 |
| CVF subendocardial, % & | 21.4 ± 11.5 | 22.6 ± 16.6 | 0.770 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balčiūnaitė, G.; Rudinskaitė, I.; Palionis, D.; Besusparis, J.; Žurauskas, E.; Janušauskas, V.; Zorinas, A.; Valevičienė, N.; Ručinskas, K.; Sogaard, P.; et al. Electrocardiographic Markers of Adverse Left Ventricular Remodeling and Myocardial Fibrosis in Severe Aortic Stenosis. J. Clin. Med. 2023, 12, 5588. https://doi.org/10.3390/jcm12175588
Balčiūnaitė G, Rudinskaitė I, Palionis D, Besusparis J, Žurauskas E, Janušauskas V, Zorinas A, Valevičienė N, Ručinskas K, Sogaard P, et al. Electrocardiographic Markers of Adverse Left Ventricular Remodeling and Myocardial Fibrosis in Severe Aortic Stenosis. Journal of Clinical Medicine. 2023; 12(17):5588. https://doi.org/10.3390/jcm12175588
Chicago/Turabian StyleBalčiūnaitė, Giedrė, Ieva Rudinskaitė, Darius Palionis, Justinas Besusparis, Edvardas Žurauskas, Vilius Janušauskas, Aleksejus Zorinas, Nomeda Valevičienė, Kęstutis Ručinskas, Peter Sogaard, and et al. 2023. "Electrocardiographic Markers of Adverse Left Ventricular Remodeling and Myocardial Fibrosis in Severe Aortic Stenosis" Journal of Clinical Medicine 12, no. 17: 5588. https://doi.org/10.3390/jcm12175588
APA StyleBalčiūnaitė, G., Rudinskaitė, I., Palionis, D., Besusparis, J., Žurauskas, E., Janušauskas, V., Zorinas, A., Valevičienė, N., Ručinskas, K., Sogaard, P., & Glaveckaitė, S. (2023). Electrocardiographic Markers of Adverse Left Ventricular Remodeling and Myocardial Fibrosis in Severe Aortic Stenosis. Journal of Clinical Medicine, 12(17), 5588. https://doi.org/10.3390/jcm12175588