
Aerobic and Muscle-Strengthening Physical Activity, Television Viewing, and Nonalcoholic Fatty Liver Disease: The CARDIA Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
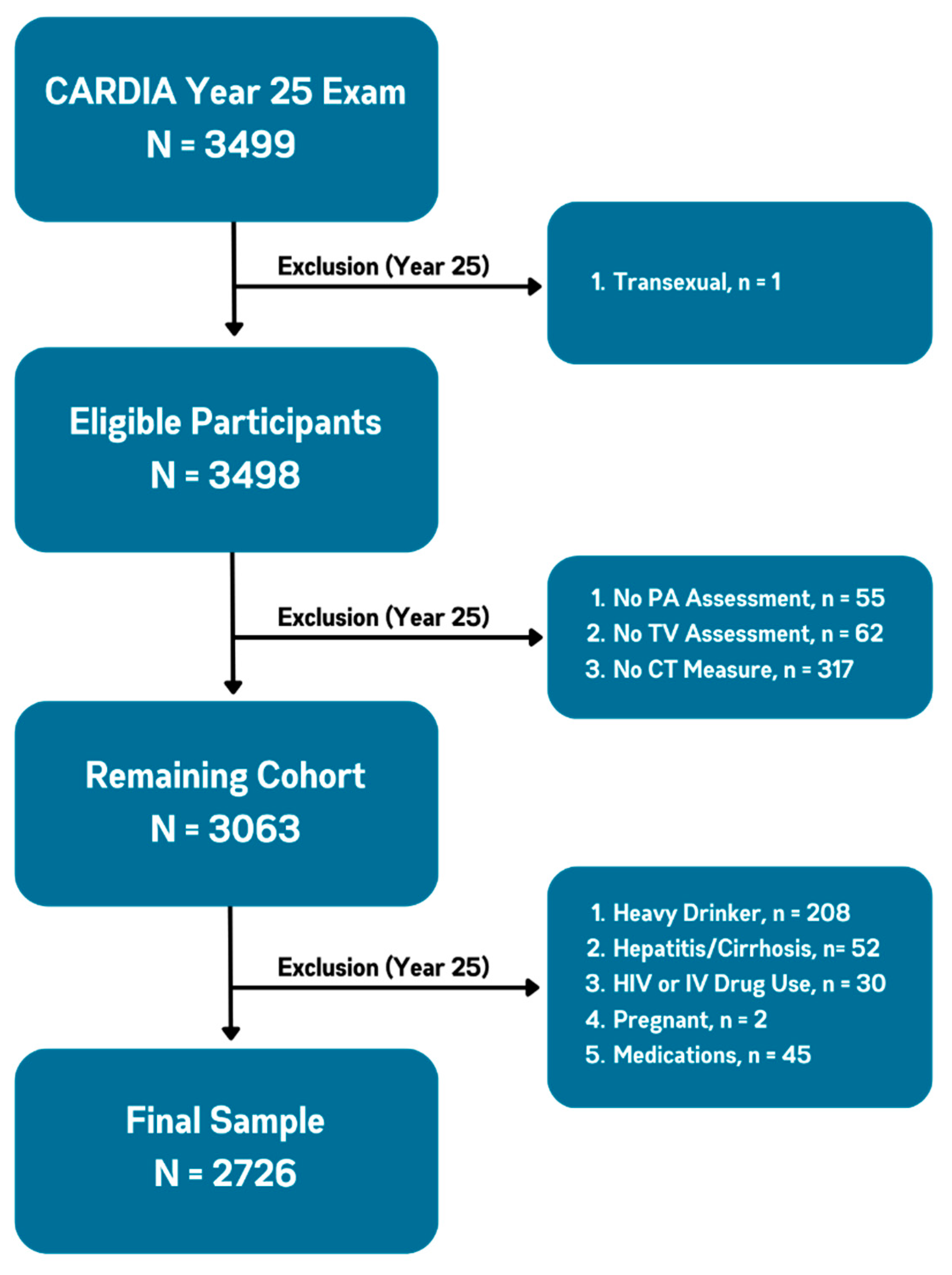
2.1. Study Sample
2.2. Measures
2.2.1. Physical Activity and Television Viewing
2.2.2. Liver Attenuation
2.3. Covariates
2.4. Statistical Analyses

{kind=link}
{kind=link}
| Analysis | Model 1 Adjustments | Model 2 Adjustments | Model 3 Exploratory Adjustment | Model 3b Exploratory Adjustment |
|---|---|---|---|---|
| Table 2 Primary, Continuous Analysis | Age, race, sex, study center | Model 1 + diet quality, alcohol consumption, education, and smoking status | Model 2 + BMI | Model 2 + waist circumference |
| Table 3 Categorical Analysis to Elucidate Dose–response Associations | Age, race, sex, study center | Model 1 + diet quality, alcohol consumption, education, and smoking status | Model 2 + waist circumference | N/A. (BMI adjustment omitted given lack of attenuation of vigorous physical activity and television viewing in our primary analyses |
| Figure 2 Summary Index Model to Examine Additivity of the 3 Exposures | Adjusted for Model 2 (above). Not adjusted for exploratory adiposity confounders (BMI or waist circumference) | |||
| Variable | Overall (n = 2726) | Liver Attenuation | |
|---|---|---|---|
| NAFLD <51 HU (n = 648) | No NAFLD ≥51 HU (n = 2078) | ||
| Liver Attenuation (HU), mean ± SD | 55.6 ± 11.6 | 39.7 ± 10.9 | 60.6 ± 5.9 |
| Age (years), mean ± SD | 50.1 ± 3.6 | 50.3 ± 3.6 | 49.9 ± 3.6 |
| Sex, n (%) | |||
| Male | 1163 (42.7) | 359 (55.5) | 804 (38.7) |
| Female | 1562 (57.3) | 288 (44.5) | 1274 (61.3) |
| Race n (%) | |||
| Black | 1325 (48.6) | 303 (46.8) | 1022 (49.2) |
| White | 1401 (51.4) | 345 (53.2) | 1056 (50.8) |
| Education (years), mean ± SD | 15.1 ± 2.6 | 15.1 ± 2.7 | 14.9 ± 2.6 |
| Diet Quality Score (std.), mean ± SD | 5.4 ± 1.0 | 5.4 ± 1.0 | 5.3 ± 0.9 |
| Smoking, n (%) | |||
| Never | 1717 (63.0) | 373 (57.6) | 1344 (64.7) |
| Former | 590 (21.6) | 167 (25.8) | 423 (20.4) |
| Current | 419 (15.4) | 208 (16.7) | 311 (15.0) |
| Alcohol (drinks/week), mean ± SD | 7.4 ± 10.7 | 7.9 ± 11.7 | 7.3 ± 10.4 |
| BMI (kg/m2), mean ± SD | 30.4 ± 7.2 | 35.2 ± 7.3 | 28.9 ± 6.4 |
| Waist Circumference (cm), mean ± SD | 94.7 ± 15.8 | 108.4 ± 14.5 | 90.4 ± 13.6 |
| Variable | Model 1 | Model 2 | Model 3 | Model 3b |
|---|---|---|---|---|
| Aerobic PA | ||||
| Moderate (IQR = 4.33, h/wk) | 1.08 (0.95–1.23) | 1.10 (0.97–1.26) | 1.14 (1.00–1.31) | 1.16 (1.01–1.32) |
| Vigorous (IQR = 1.91, h/wk) | 0.71 (0.63–0.81) | 0.72 (0.63–0.82) | 0.83 (0.73–0.94) | 0.89 (0.79–1.02) |
| Muscle-Strengthening PA (IQR = 3.33, h/wk) | 0.89 (0.79–1.00) | 0.89 (0.80–1.01) | 0.93 (0.83–1.05) | 0.95 (0.84–1.07) |
| Television Viewing (IQR = 14.0, h/wk) | 1.11 (1.05–1.18) | 1.12 (1.05–1.19) | 1.07 (1.01–1.14) | 1.06 (0.99–1.14) |
3. Results
3.1. Participant Characteristics
3.2. Primary Analysis
3.3. Categorical (Dose–Response) Analysis
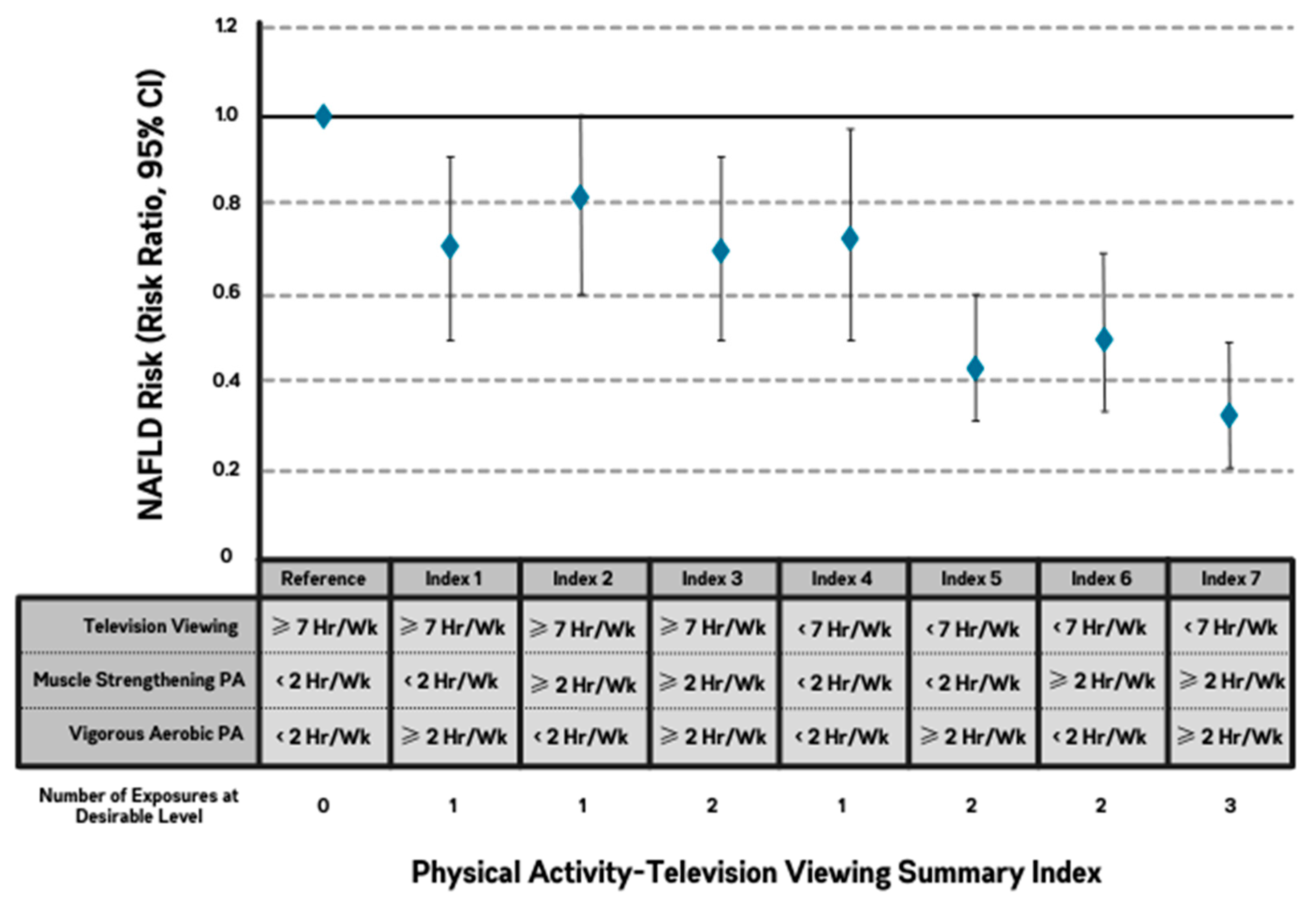
3.4. Summary Index
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diehl, A.M.; Day, C. Cause, pathogenesis, and treatment of nonalcoholic steatohepatitis. N. Engl. J. Med. 2017, 377, 2063–2072. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Golabi, P.; Paik, J.M.; Henry, A.; Van Dongen, C.; Henry, L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): A systematic review. Hepatology 2023, 77, 1335–1347. [Google Scholar] [CrossRef]
- Estes, C.; Razavi, H.; Loomba, R.; Younossi, Z.; Sanyal, A.J. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology 2018, 67, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Faasse, S.; Braun, H.; Vos, M. The role of NAFLD in cardiometabolic disease: An update. F1000Res 2018, 7, 170. [Google Scholar] [CrossRef]
- Mantovani, A.; Csermely, A.; Petracca, G.; Beatrice, G.; E Corey, K.; Simon, T.G.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: An updated systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 903–913. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Tampi, R.; Priyadarshini, M.; Nader, F.; Younossi, I.M.; Racila, A. Burden of illness and economic model for patients with nonalcoholic steatohepatitis in the United States. Hepatology 2019, 69, 564–572. [Google Scholar] [CrossRef]
- Than, N.N.; Newsome, P.N. A concise review of non-alcoholic fatty liver disease. Atherosclerosis 2015, 239, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Sheka, A.C.; Adeyi, O.; Thompson, J.; Hameed, B.; Crawford, P.A.; Ikramuddin, S. Nonalcoholic steatohepatitis: A review. JAMA 2020, 323, 1175–1183. [Google Scholar] [CrossRef]
- Koutoukidis, D.A.; Astbury, N.M.; Tudor, K.E.; Morris, E.; Henry, J.A.; Noreik, M.; Jebb, S.A.; Aveyard, P. Association of weight loss interventions with changes in biomarkers of nonalcoholic fatty liver disease: A systematic review and meta-analysis. JAMA Intern Med. 2019, 179, 1262–1271. [Google Scholar] [CrossRef]
- van der Windt, D.J.; Sud, V.; Zhang, H.; Tsung, A.; Huang, H. The effects of physical exercise on fatty liver disease. Gene Expr. 2018, 18, 89–101. [Google Scholar] [CrossRef]
- Johnson, N.A.; Sachinwalla, T.; Walton, D.W.; Smith, K.; Armstrong, A.; Thompson, M.W.; George, J. Aerobic exercise training reduces hepatic and visceral lipids in obese individuals without weight loss. Hepatology 2009, 50, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.C.; Suh, S.; Park, S.E.; Rhee, E.J.; Park, C.Y.; Oh, K.W.; Park, S.W.; Kim, S.W.; Hur, K.Y.; Kim, J.H.; et al. Regular exercise is associated with a reduction in the risk of NAFLD and decreased liver enzymes in individuals with NAFLD independent of obesity in Korean adults. PLoS ONE 2012, 7, e46819. [Google Scholar] [CrossRef] [PubMed]
- Hannukainen, J.C.; Nuutila, P.; Ronald, B.; Kaprio, J.; Kujala, U.M.; Janatuinen, T.; Heinonen, O.J.; Kapanen, J.; Viljanen, T.; Haaparanta, M.; et al. Increased physical activity decreases hepatic free fatty acid uptake: A study in human monozygotic twins. J Physiol. 2007, 578 Pt 1, 347–358. [Google Scholar] [CrossRef]
- Hashida, R.; Kawaguchi, T.; Bekki, M.; Omoto, M.; Matsuse, H.; Nago, T.; Takano, Y.; Ueno, T.; Koga, H.; George, J.; et al. Aerobic vs. resistance exercise in non-alcoholic fatty liver disease: A systematic review. J. Hepatol. 2017, 66, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Babu, A.F.; Csader, S.; Lok, J.; Gómez-Gallego, C.; Hanhineva, K.; El-Nezami, H.; Schwab, U. Positive Effects of exercise intervention without weight loss and dietary changes in NAFLD-related clinical parameters: A systematic review and meta-analysis. Nutrients 2021, 13, 3135. [Google Scholar] [CrossRef]
- Bacchi, E.; Negri, C.; Targher, G.; Faccioli, N.; Lanza, M.; Zoppini, G.; Zanolin, E.; Schena, F.; Bonora, E.; Moghetti, P. Both resistance training and aerobic training reduce hepatic fat content in type 2 diabetic subjects with nonalcoholic fatty liver disease (the RAED2 Randomized Trial). Hepatology 2013, 58, 1287–1295. [Google Scholar] [CrossRef]
- Oh, S.; Shida, T.; Yamagishi, K.; Tanaka, K.; So, R.; Tsujimoto, T.; Shoda, J. Moderate to vigorous physical activity volume is an important factor for managing nonalcoholic fatty liver disease: A retrospective study. Hepatology 2015, 61, 1205–1215. [Google Scholar] [CrossRef]
- Blanc, S.; Normand, S.; Pachiaudi, C.; Fortrat, J.O.; Laville, M.; Gharib, C. Fuel homeostasis during physical inactivity induced by bed rest. J. Clin. Endocrinol. Metab. 2000, 85, 2223–2233. [Google Scholar] [CrossRef]
- van der Ploeg, H.P.; Hillsdon, M. Is sedentary behaviour just physical inactivity by another name? Int. J. Behav. Nutr. Phys. Act. 2017, 14, 142. [Google Scholar] [CrossRef]
- Dempsey, P.C.; Matthews, C.E.; Dashti, S.G.; Doherty, A.R.; Bergouignan, A.; van Roekel, E.H.; Dunstan, D.W.; Wareham, N.J.; Yates, T.E.; Wijndaele, K.; et al. Sedentary behavior and chronic disease: Mechanisms and future directions. J. Phys. Act. Health. 2020, 17, 52–61. [Google Scholar] [CrossRef]
- Dempsey, P.C.; Matthews, C.E.; Dashti, S.G.; Doherty, A.R.; Bergouignan, A.; van Roekel, E.H.; Dunstan, D.W.; Wareham, N.J.; Yates, T.E.; Wijndaele, K.; et al. Relationship of sitting time and physical activity with non-alcoholic fatty liver disease. J. Hepatol. 2015, 63, 1229–1237. [Google Scholar]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Friedman, G.D.; Cutter, G.R.; Donahue, R.P.; Hughes, G.H.; Hulley, S.B.; Jacobs, D.R.; Liu, K.; Savage, P.J. CARDIA: Study design, recruitment, and some characteristics of the examined subjects. J. Clin. Epidemiol. 1988, 41, 1105–1116. [Google Scholar] [CrossRef] [PubMed]
- VanWagner, L.B.; Wilcox, J.E.; Colangelo, L.A.; Lloyd-Jones, D.M.; Carr, J.J.; Lima, J.A.; Lewis, C.E.; Rinella, M.E.; Shah, S.J. Association of nonalcoholic fatty liver disease with subclinical myocardial remodeling and dysfunction: A population-based study. Hepatology 2015, 62, 773–783. [Google Scholar] [CrossRef] [PubMed]
- VanWagner, L.B.; Ning, H.; Lewis, C.E.; Shay, C.M.; Wilkins, J.; Carr, J.J.; Terry, J.G.; Lloyd-Jones, D.M.; Jacobs, D.R.; Carnethon, M.R. Associations between nonalcoholic fatty liver disease and subclinical atherosclerosis in middle-aged adults: The Coronary Artery Risk Development in Young Adults Study. Atherosclerosis 2014, 235, 599–605. [Google Scholar] [CrossRef]
- Pereira, M.; FitzerGerald, S.; Gregg, E. A collection of physical activity questionnaires for health-related research. Med. Sci. Sports Exerc. 1997, 29 (Suppl. S6), S1–S205. [Google Scholar]
- Jacobs, D.R.; Ainsworth, B.E.; Hartman, T.J.; Leon, A.S. A simultaneous evaluation of 10 commonly used physical activity questionnaires. Med. Sci. Sports Exerc. 1993, 25, 81–91. [Google Scholar] [CrossRef]
- Jacobs, D.R.; Hahn, L.P.; Haskell, W.L.; Pirie, P.; Sidney, S. Validity and reliability of short physical activity history: CARDIA and the Minnesota Heart Health Program. J. Cardiopulm. Rehabil. 1989, 9, 448–459. [Google Scholar] [CrossRef]
- Pettee Gabriel, K.; Sidney, S.; Jacobs, D.R., Jr.; Whitaker, K.M.; Carnethon, M.R.; Lewis, C.E.; Schreiner, P.J.; Malkani, R.I.; Shikany, J.M.; Reis, J.P.; et al. Ten-year changes in accelerometer-based physical activity and sedentarytime during midlife: The CARDIA study. Am. J. Epidemiol. 2018, 187, 2145–2150. [Google Scholar] [CrossRef]
- Sternfeld, B.; Gabriel, K.P.; Jiang, S.-F.; Whitaker, K.M.; Jacobs, D.R.; Quesenberry, C.P.; Carnethon, M.; Sidney, S. Risk estimates for diabetes and hypertension with different physical activity methods. Med. Sci. Sports Exerc. 2019, 51, 2498–2505. [Google Scholar] [CrossRef]
- Sidney, S.; Jacobs, D.R.; Haskell, W.L.; Armstrong, M.A.; Dimicco, A.; Oberman, A.; Savage, P.J.; Slattery, M.L.; Sternfeld, B.; Van Hom, L. Comparison of two methods of assessing physical activity in the Coronary Artery Risk Development in Young Adults (CARDIA) Study. Am. J. Epidemiol. 1991, 133, 1231–1245. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, K.M.; Pereira, M.A.; Jacobs, D.R.; Sidney, S.; Odegaard, A.O. Sedentary behavior, physical activity, and abdominal adipose tissue deposition. Med. Sci. Sports Exerc. 2017, 49, 450–458. [Google Scholar] [CrossRef]
- Norman, G.J.; Schmid, B.A.; Sallis, J.F.; Calfas, K.J.; Patrick, K. Psychosocial and environmental correlates of adolescent sedentary behaviors. Pediatrics 2005, 116, 908–916. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.N. Reducing children’s television viewing to prevent obesity: A randomized controlled trial. JAMA 1999, 282, 1561–1567. [Google Scholar] [CrossRef]
- Marshall, A.L.; Miller, Y.D.; Burton, N.W.; Brown, W.J. Measuring total and domain-specific sitting: A study of reliability and validity. Med. Sci. Sports Exerc. 2010, 42, 1094–1102. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, D.E.; Norman, G.J.; Wagner, N.; Patrick, K.; Calfas, K.J.; Sallis, J.F. Reliability and validity of the Sedentary Behavior Questionnaire (SBQ) for adults. J. Phys. Act. Health. 2010, 7, 697–705. [Google Scholar] [CrossRef]
- Carr, J.J.; Nelson, J.C.; Wong, N.D.; McNitt-Gray, M.; Arad, Y.; Jacobs, D.R.; Sidney, S.; Bild, D.E.; Williams, O.D.; Detrano, R.C. Calcified coronary artery plaque measurement with cardiac CT in population-based studies: Standardized protocol of Multi-Ethnic Study of Atherosclerosis (MESA) and Coronary Artery Risk Development in Young Adults (CARDIA) study. Radiology 2005, 234, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Carr, J.J.; Jacobs, D.R.; Terry, J.G.; Shay, C.M.; Sidney, S.; Liu, K.; Schreiner, P.J.; Lewis, C.E.; Shikany, J.M.; Reis, J.P.; et al. Association of coronary artery calcium in adults aged 32 to 46 Years with incident coronary heart disease and death. JAMA Cardiol. 2017, 2, 391–399. [Google Scholar] [CrossRef]
- VanWagner, L.B.; Terry, J.G.; Chow, L.S.; Alman, A.C.; Kang, H.; Ingram, K.H.; Shay, C.; Lewis, C.E.; Bryan, R.N.; Launer, L.J.; et al. Nonalcoholic fatty liver disease and measures of early brain health in middle-aged adults: The CARDIA study. Obesity 2017, 25, 642–651. [Google Scholar] [CrossRef]
- Kodama, Y.; Ng, C.S.; Wu, T.T.; Ayers, G.D.; Curley, S.A.; Abdalla, E.K.; Vauthey, J.N.; Charnsangavej, C. Comparison of CT methods for determining the fat content of the liver. AJR Am. J. Roentgenol. 2007, 188, 1307–1312. [Google Scholar] [CrossRef]
- Meyer, K.A.; Sijtsma, F.P.; Nettleton, J.A.; Steffen, L.M.; Van Horn, L.; Shikany, J.M.; Gross, M.D.; Mursu, J.; Traber, M.G.; Jacobs, D.R. Dietary patterns are associated with plasma F2-isoprostanes in an observational cohort study of adults. Free Radic. Biol. Med. 2013, 57, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Sargeant, J.A.; Gray, L.J.; Bodicoat, D.H.; Willis, S.A.; Stensel, D.J.; Nimmo, M.A.; Aithal, G.P.; King, J.A. The effect of exercise training on intrahepatic triglyceride and hepatic insulin sensitivity: A systematic review and meta-analysis. Obes. Rev. 2018, 19, 1446–1459. [Google Scholar] [CrossRef]
- Katsagoni, C.N.; Georgoulis, M.; Papatheodoridis, G.V.; Panagiotakos, D.B.; Kontogianni, M.D. Effects of lifestyle interventions on clinical characteristics of patients with non-alcoholic fatty liver disease: A meta-analysis. Metabolism 2017, 68, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Smart, N.A.; King, N.; McFarlane, J.R.; Graham, P.L.; Dieberg, G. Effect of exercise training on liver function in adults who are overweight or exhibit fatty liver disease: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 834–843. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.J.; He, J.; Pan, L.L.; Ma, Z.M.; Han, C.K.; Chen, C.S.; Chen, Z.; Han, H.W.; Chen, S.; Sun, Q.; et al. Effects of moderate and vigorous exercise on nonalcoholic fatty liver disease: A randomized clinical trial. JAMA Intern. Med. 2016, 176, 1074–1082. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Vazquez-Montesino, L.M.; Li, A.A.; Cholankeril, G.; Ahmed, A. Inadequate physical activity and sedentary behavior are independent predictors of nonalcoholic fatty liver disease. Hepatology 2020, 72, 1556–1568. [Google Scholar] [CrossRef]
- Tsunoda, K.; Kitano, N.; Kai, Y.; Jindo, T.; Uchida, K.; Arao, T. Dose-response relationships of accelerometer-measured sedentary behaviour and physical activity with non-alcoholic fatty liver disease. Aliment Pharmacol. Ther. 2021, 54, 1330–1339. [Google Scholar] [CrossRef]
- Zelber-Sagi, S.; Nitzan-Kaluski, D.; Goldsmith, R.; Webb, M.; Zvibel, I.; Goldiner, I.; Blendis, L.; Halpern, Z.; Oren, R. Role of leisure-time physical activity in nonalcoholic fatty liver disease: A population-based study. Hepatology 2008, 48, 1791–1798. [Google Scholar] [CrossRef]
- Berzigotti, A.; Saran, U.; Dufour, J.F. Physical activity and liver diseases. Hepatology 2016, 63, 1026–1040. [Google Scholar] [CrossRef]
- Gerber, L.; Otgonsuren, M.; Mishra, A.; Escheik, C.; Birerdinc, A.; Stepanova, M.; Younossi, Z.M. Non-alcoholic fatty liver disease (NAFLD) is associated with low level of physical activity: A population-based study. Aliment. Pharmacol. Ther. 2012, 36, 772–781. [Google Scholar] [CrossRef]
- Helajärvi, H.; Pahkala, K.; Heinonen, O.J.; Juonala, M.; Oikonen, M.; Tammelin, T.; Hutri-Kähönen, N.; Kähönen, M.; Lehtimäki, T.; Mikkilä, V.; et al. Television viewing and fatty liver in early midlife. The Cardiovascular Risk in Young Finns Study. Annals. Med. 2015, 47, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Chen, K.; Yin, S.; Qian, M.; Liu, C. Association of leisure sedentary behavior and physical activity with the risk of nonalcoholic fatty liver disease: A two-sample Mendelian randomization study. Front. Nutr. 2023, 10, 1158810. [Google Scholar] [CrossRef] [PubMed]
- Prenner, S.; Rinella, M.E. Moderate exercise for nonalcoholic fatty liver disease. JAMA Intern. Med. 2016, 176, 1083–1084. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Andreato, L.V.; Esteves, J.V.; Coimbra, D.R.; Moraes, A.J.P.; de Carvalho, T. The influence of high-intensity interval training on anthropometric variables of adults with overweight or obesity: A systematic review and network meta-analysis. Obes. Rev. 2019, 20, 142–155. [Google Scholar] [CrossRef]
- Atakan, M.M.; Guzel, Y.; Shrestha, N.; Kosar, S.N.; Grgic, J.; A Astorino, T.; Turnagol, H.H.; Pedisic, Z. Effects of high-intensity interval training (HIIT) and sprint interval training (SIT) on fat oxidation during exercise: A systematic review and meta-analysis. Br. J. Sports Med. 2022, 56, 988–996. [Google Scholar] [CrossRef]
- Khalafi, M.; Malandish, A.; Rosenkranz, S.K.; Ravasi, A.A. Effect of resistance training with and without caloric restriction on visceral fat: A systemic review and meta-analysis. Obes. Rev. 2021, 22, e13275. [Google Scholar] [CrossRef]
- Maillard, F.; Pereira, B.; Boisseau, N. Effect of high-intensity interval training on total, abdominal and visceral fat mass: A meta-analysis. Sports Med. 2018, 48, 269–288. [Google Scholar] [CrossRef]
- Pang, Q.; Zhang, J.-Y.; Song, S.-D.; Qu, K.; Xu, X.-S.; Liu, S.-S.; Liu, C. Central obesity and nonalcoholic fatty liver disease risk after adjusting for body mass index. World J. Gastroenterol. 2015, 21, 1650–1662. [Google Scholar] [CrossRef]
- Utzschneider, K.M.; Kahn, S.E. Review: The role of insulin resistance in nonalcoholic fatty liver disease. J. Clin. Endocrinol. Metab. 2006, 91, 4753–4761. [Google Scholar] [CrossRef]
- Palma, R.; Pronio, A.; Romeo, M.; Scognamiglio, F.; Ventriglia, L.; Ormando, V.M.; Lamazza, A.; Pontone, S.; Federico, A.; Dallio, M. The role of insulin resistance in fueling NAFLD pathogenesis: From molecular mechanisms to clinical implications. J. Clin. Med. 2022, 11, 3649. [Google Scholar] [CrossRef]
- Bird, S.R.; Hawley, J.A. Update on the effects of physical activity on insulin sensitivity in humans. BMJ Open Sport Exerc. Med. 2016, 2, e000143. [Google Scholar] [CrossRef]
- Ibañez, J.; Izquierdo, M.; Argüelles, I.; Forga, L.; Larrión, J.L.; García-Unciti, M.; Idoate, F.; Gorostiaga, E.M. Twice-weekly progressive resistance training decreases abdominal fat and improves insulin sensitivity in older men with type 2 diabetes. Diabetes Care 2005, 28, 662–667. [Google Scholar] [CrossRef]
- Spriet, L.L.; Howlett, R.A.; Heigenhauser, G.J. An enzymatic approach to lactate production in human skeletal muscle during exercise. Med. Sci. Sports Exerc. 2000, 32, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, T.; Hussien, R.; Oommen, S.; Gohil, K.; Brooks, G.A. Lactate sensitive transcription factor network in L6 cells: Activation of MCT1 and mitochondrial biogenesis. FASEB J. 2007, 21, 2602–2612. [Google Scholar] [CrossRef] [PubMed]
- Scheiman, J.; Luber, J.M.; Chavkin, T.A.; MacDonald, T.; Tung, A.; Pham, L.-D.; Wibowo, M.C.; Wurth, R.C.; Punthambaker, S.; Tierney, B.T.; et al. Meta-omics analysis of elite athletes identifies a performance-enhancing microbe that functions via lactate metabolism. Nat. Med. 2019, 25, 1104–1109. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K. Muscle as a secretory organ. Compr. Physiol. 2013, 3, 1337–1362. [Google Scholar]
- Febbraio, M.A.; Hiscock, N.; Sacchetti, M.; Fischer, C.P.; Pedersen, B.K. Interleukin-6 is a novel factor mediating glucose homeostasis during skeletal muscle contraction. Diabetes 2004, 53, 1643–1648. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Lee, H.J.; So, B.; Son, J.S.; Yoon, D.; Song, W. Effect of aerobic training and resistance training on circulating irisin level and their association with change of body composition in overweight/obese adults: A pilot study. Physiol Res. 2016, 65, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, P.M.; Touchberry, C.D.; Teson, K.; McCabe, E.; Tehel, M.; Wacker, M.J. Effects of an acute bout of resistance exercise on fiber-type specific to GLUT4 and IGF-1R expression. Appl. Physiol. Nutr. Metab. 2013, 38, 581–586. [Google Scholar] [CrossRef]
- Oh, Y.S.; Kim, H.J.; Ryu, S.J.; Cho, K.A.; Park, Y.S.; Park, H.; Kim, M.; Kim, C.K. Exercise type and muscle fiber specific induction of caveolin-1 expression for insulin sensitivity of skeletal muscle. Exp. Mol. Med. 2007, 39, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.J.; Sherman, W.M.; Ivy, J.L. Effect of strength training on glucose tolerance and post-glucose insulin response. Med. Sci. Sports Exerc. 1984, 16, 539–543. [Google Scholar] [CrossRef]
- Donahoo, W.T.; Levine, J.A.; Melanson, E.L. Variability in energy expenditure and its components. Curr. Opin. Clin. Nutr. Metab. Care 2004, 7, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Børsheim, E.; Bahr, R. Effect of exercise intensity, duration and mode on post-exercise oxygen consumption. Sports Med. 2003, 33, 1037–1060. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.O.; Wyatt, H.R.; Reed, G.W.; Peters, J.C. Obesity and the environment: Where do we go from here? Science 2003, 299, 853–855. [Google Scholar] [CrossRef]
- Ramadan, F.A.; Bea, J.W.; Garcia, O.D.; Ellingson, K.D.; A Canales, R.; Raichlen, A.D.; Klimentidis, Y.C. Association of sedentary and physical activity behaviours with body composition: A genome-wide association and Mendelian randomisation study. BMJ Open Sport Exerc. Med. 2022, 8, e001291. [Google Scholar] [CrossRef] [PubMed]
- Coleman, C.J.; McDonough, D.J.; Pope, Z.C.; Pope, C.A. Dose-response association of aerobic and muscle-strengthening physical activity with mortality: A national cohort study of 416 420 US adults. Br. J. Sports Med. 2022. Online ahead of print. [Google Scholar] [CrossRef]


| Variable | Model 1 | aP | Model 2 | aP | Model 3b | aP |
|---|---|---|---|---|---|---|
| Aerobic PA | ||||||
| Moderate (h/wk) ≤1.7, (n = 697) 1.71–3.8, (n = 682) 3.81–6, (n = 671) >6, (n = 676) | - 1.03 (0.83–1.30) 1.10 (0.87–1.30) 1.14 (0.89–1.45) | 0.27 | - 1.05 (0.83–1.32) 1.14 (0.90–1.44) 1.17 (0.91–1.51) | 0.18 | - 1.04 (0.82–1.31) 1.19 (0.94–1.51) 1.21 (0.94–1.57) | 0.09 |
| Vigorous (h/wk) 0, (n = 946) 0–0.5, (n = 456) 0.51–1.99, (n = 635) ≥2, (n = 676) | - 0.94 (0.75–1.17) 0.82 (0.66–1.01) 0.56 (0.44–0.71) | <0.001 | - 0.96 (0.76–1.20) 0.83 (0.67–1.03) 0.57 (0.44–0.73) | <0.001 | - 1.14 (0.90–1.43) 1.06 (0.85–1.33) 0.89 (0.69–1.16) | 0.11 |
| Muscle-Strengthening PA (h/wk) 0, (n = 840) 0–1.99, (n = 682) 2–3.99, (n = 671) ≥4.0, (n = 676) | - 0.87 (0.71–1.07) 0.78 (0.59–1.03) 0.80 (0.63–1.01) | 0.04 | - 0.87 (0.71–1.08) 0.78 (0.59–1.03) 0.81 (0.63–1.03) | 0.04 | - 0.99 (0.81–1.24) 0.92 (0.70–1.22) 0.95 (0.74–1.21) | 0.57 |
| Television Viewing (h/wk) <7, (n = 882) 7–13.99, (n = 750) 14–20.99, (n = 437) ≥21, (n = 574) | - 1.39 (1.12–1.73) 1.82 (1.43–2.32) 1.75 (1.37–2.24) | <0.001 | - 1.38 (1.10–1.73) 1.83 (1.43–2.33) 1.75 (1.36–2.25) | <0.001 | - 1.19 (0.95–1.49) 1.27 (0.99–1.63) 1.37 (1.07–1.77) | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McDonough, D.J.; Mathew, M.; Pope, Z.C.; Schreiner, P.J.; Jacobs, D.R., Jr.; VanWagner, L.B.; Carr, J.J.; Terry, J.G.; Gabriel, K.P.; Reis, J.P.; et al. Aerobic and Muscle-Strengthening Physical Activity, Television Viewing, and Nonalcoholic Fatty Liver Disease: The CARDIA Study. J. Clin. Med. 2023, 12, 5603. https://doi.org/10.3390/jcm12175603
McDonough DJ, Mathew M, Pope ZC, Schreiner PJ, Jacobs DR Jr., VanWagner LB, Carr JJ, Terry JG, Gabriel KP, Reis JP, et al. Aerobic and Muscle-Strengthening Physical Activity, Television Viewing, and Nonalcoholic Fatty Liver Disease: The CARDIA Study. Journal of Clinical Medicine. 2023; 12(17):5603. https://doi.org/10.3390/jcm12175603
Chicago/Turabian StyleMcDonough, Daniel J., Mahesh Mathew, Zachary C. Pope, Pamela J. Schreiner, David R. Jacobs, Jr., Lisa B. VanWagner, John Jeffrey Carr, James G. Terry, Kelley Pettee Gabriel, Jared P. Reis, and et al. 2023. "Aerobic and Muscle-Strengthening Physical Activity, Television Viewing, and Nonalcoholic Fatty Liver Disease: The CARDIA Study" Journal of Clinical Medicine 12, no. 17: 5603. https://doi.org/10.3390/jcm12175603
APA StyleMcDonough, D. J., Mathew, M., Pope, Z. C., Schreiner, P. J., Jacobs, D. R., Jr., VanWagner, L. B., Carr, J. J., Terry, J. G., Gabriel, K. P., Reis, J. P., & Pereira, M. A. (2023). Aerobic and Muscle-Strengthening Physical Activity, Television Viewing, and Nonalcoholic Fatty Liver Disease: The CARDIA Study. Journal of Clinical Medicine, 12(17), 5603. https://doi.org/10.3390/jcm12175603