


Association between Serum Ferritin and Prognosis in Patients with Ischemic Heart Disease in Intensive Care Units


Abstract
:1. Introduction
2. Methods
2.1. The Data Source
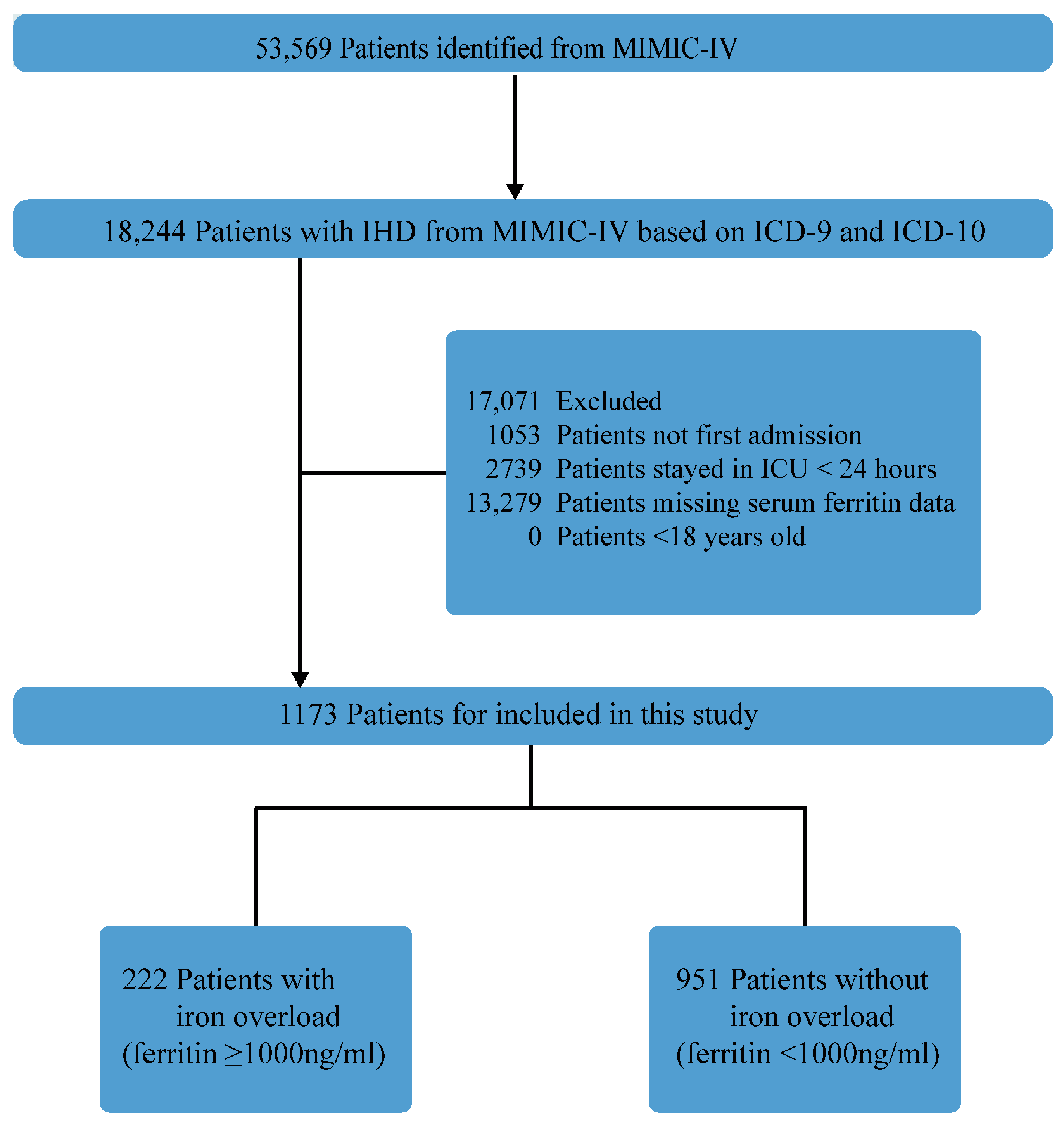
2.2. Study Population
2.3. Data Extraction and Variables
2.4. Primary Outcome and Secondary Outcomes
2.5. Statistical Methods
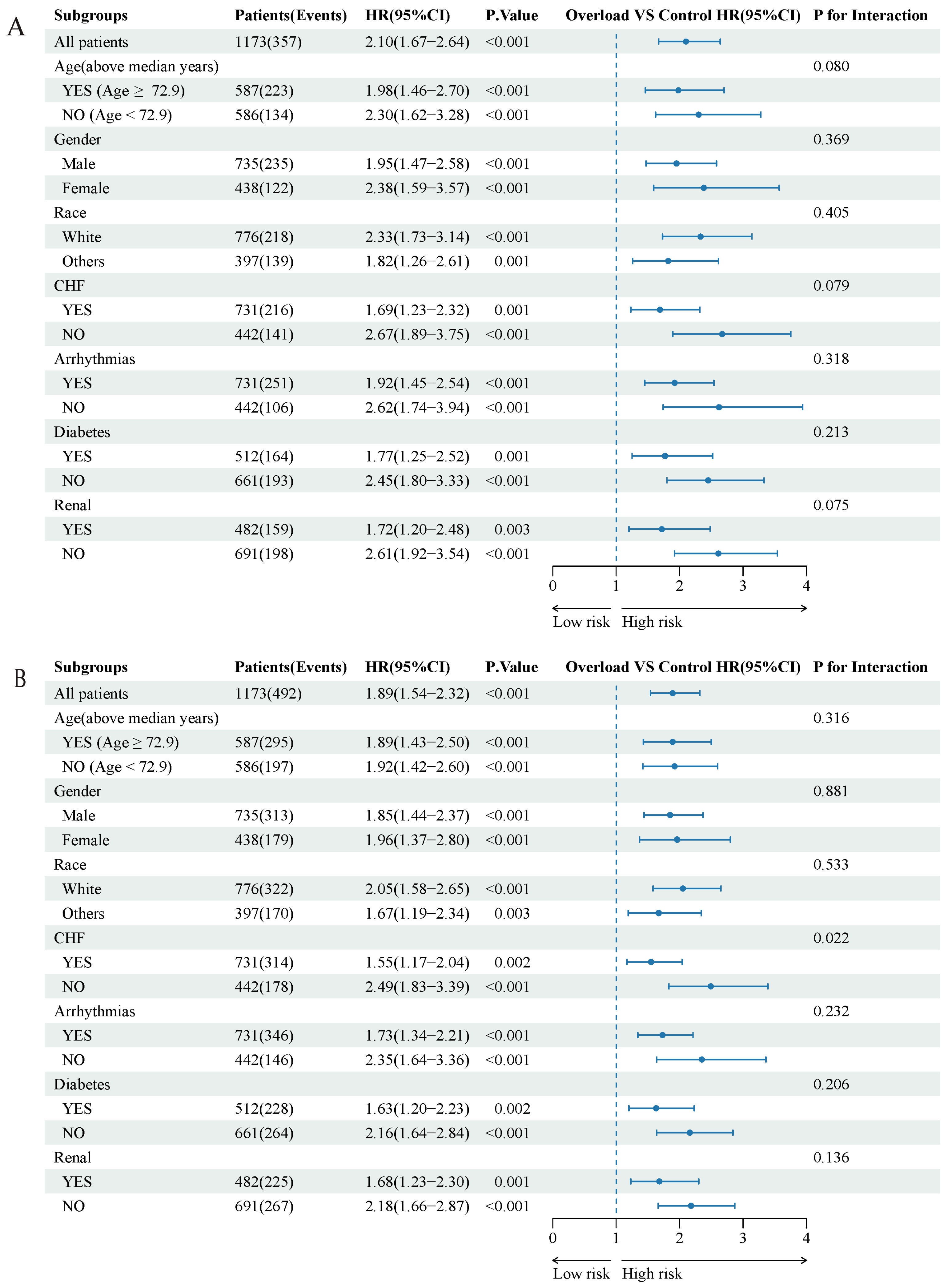
2.6. Sensitivity Analyses and Exploratory Subgroup Analyses
3. Results
3.1. Study Population and Baseline Characteristics
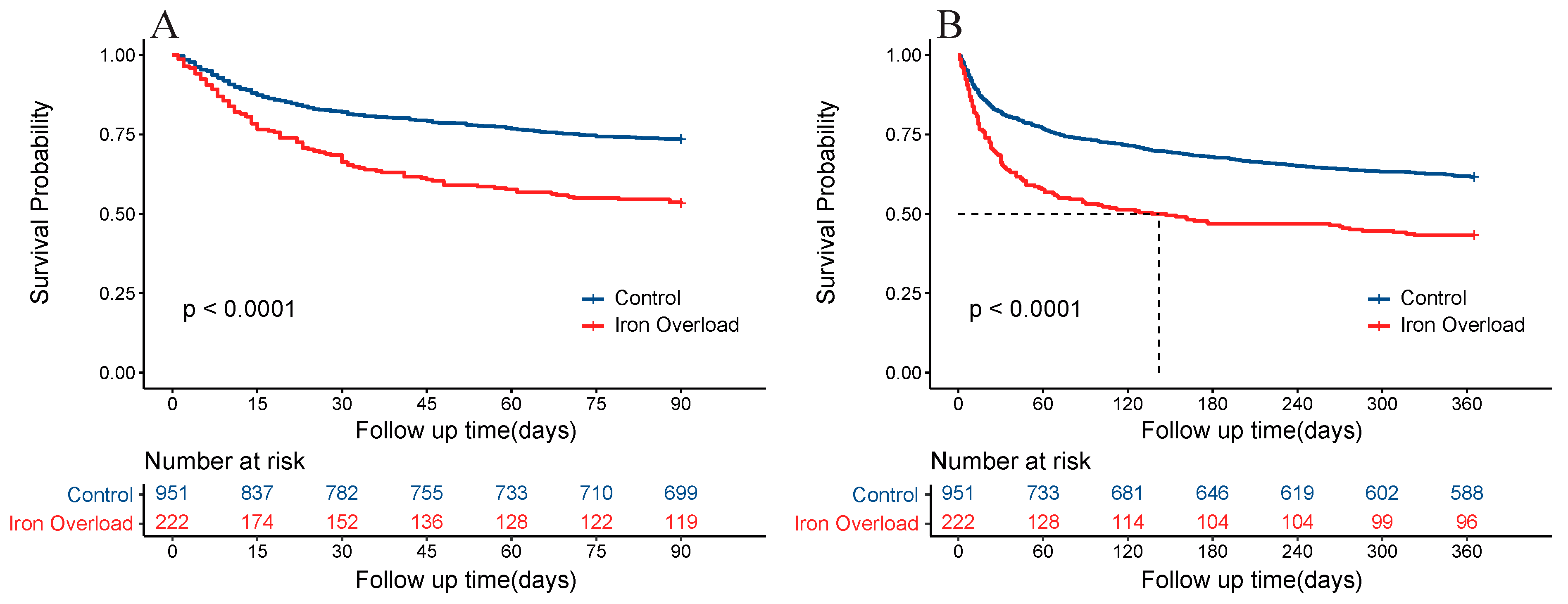
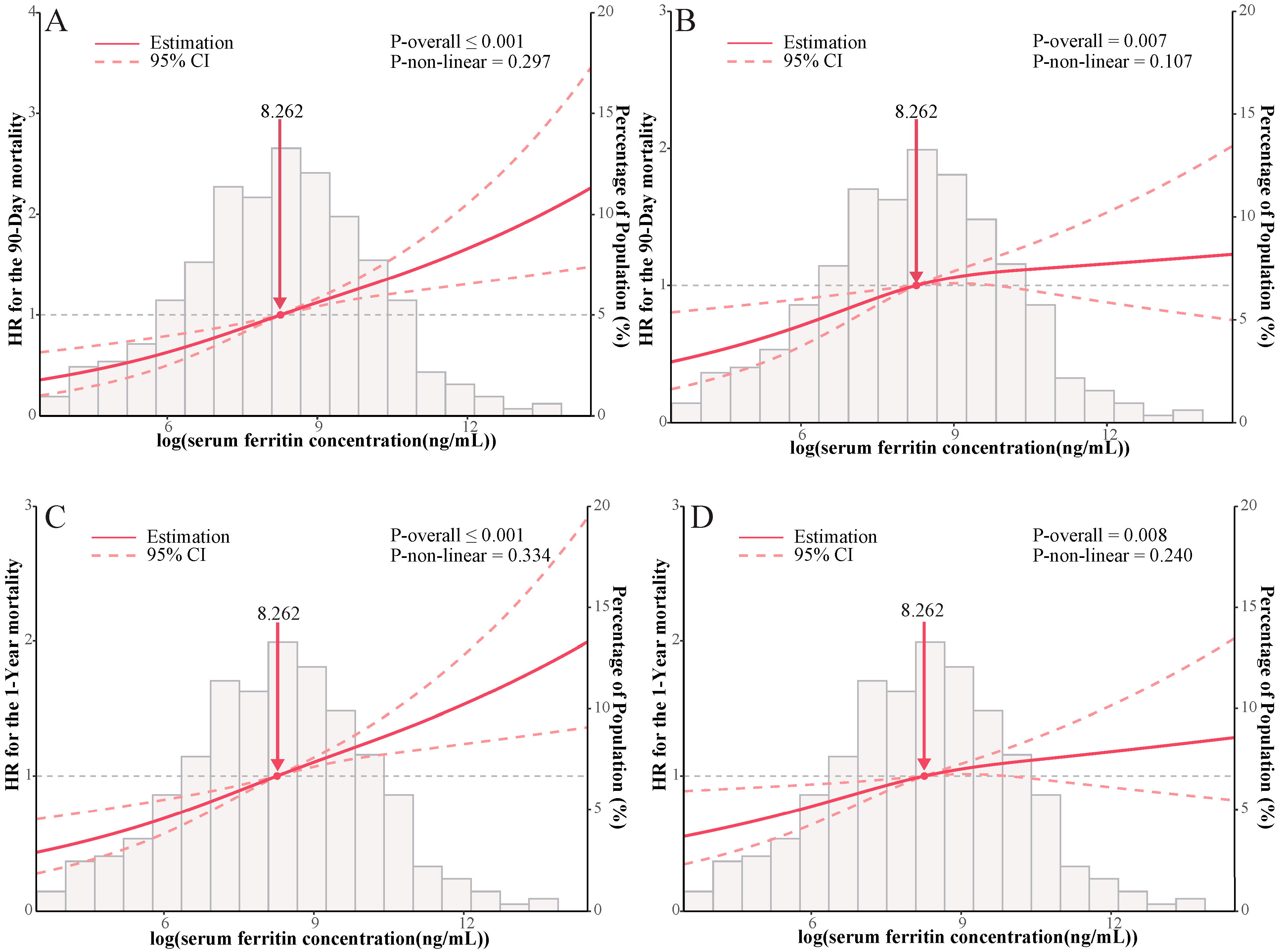
3.2. Primary Analysis
3.3. Secondary Analysis
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ICU | Intensive care unit |
| MIMIC-IV | Medical Information Mart for Intensive Care IV |
| ICD | International Classification of Diseases |
| IHD | ischemic heart disease |
| AIC | Akaike Information Criterion |
| SMDs | standardized mean differences |
| HR | hazard ratio |
| CIs | confidence intervals |
| BMI | body mass index |
| SAPSII Score | simplified acute physiology score |
| SOFA Score | sequential organ failure assessment score |
| GCS Score | glasgow coma scale score |
| MBP | mean blood pressure |
| CHF | congestive heart failure |
| PVD | peripheral vascular disease |
| COPD | chronic pulmonary disease |
| PCI | percutaneous coronary intervention |
| CABG | coronary artery bypass grafting |
| Spo2 | partial pressure of oxygen |
| WBC | white blood cell |
| ALT | alanine aminotransferase |
| AST | aspartate aminotransferase |
| BUN | blood urea nitrogen |
| INR | international normalized ratio |
| BNP | B-type natriuretic peptide |
References
- Diseases, G.B.D.; Injuries, C. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart Disease and Stroke Statistics-2023 Update: A Report from the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar] [CrossRef] [PubMed]
- Badal, S.; Thapa Bajgain, K.; Badal, S.; Thapa, R.; Bajgain, B.B.; Santana, M.J. Prevalence, clinical characteristics, and outcomes of pediatric COVID-19: A systematic review and meta-analysis. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2021, 135, 104715. [Google Scholar] [CrossRef] [PubMed]
- Abrams, J.Y.; Oster, M.E.; Godfred-Cato, S.E.; Bryant, B.; Datta, S.D.; Campbell, A.P.; Leung, J.W.; Tsang, C.A.; Pierce, T.J.; Kennedy, J.L.; et al. Factors linked to severe outcomes in multisystem inflammatory syndrome in children (MIS-C) in the USA: A retrospective surveillance study. Lancet. Child Adolesc. Health 2021, 5, 323–331. [Google Scholar] [CrossRef]
- Mahroum, N.; Alghory, A.; Kiyak, Z.; Alwani, A.; Seida, R.; Alrais, M.; Shoenfeld, Y. Ferritin—From iron, through inflammation and autoimmunity, to COVID-19. J. Autoimmun. 2022, 126, 102778. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Liu, Q.; Shan, X.; Gao, W.; Chen, Q. ATM orchestrates ferritinophagy and ferroptosis by phosphorylating NCOA4. Autophagy 2023, 19, 2062–2077. [Google Scholar] [CrossRef]
- Sun, W.C.; Wang, N.N.; Li, R.; Sun, X.C.; Liao, J.W.; Yang, G.; Liu, S. Ferritinophagy activation and sideroflexin1-dependent mitochondrial iron overload contribute to patulin-induced cardiac inflammation and fibrosis. Sci. Total Environ. 2023, 892, 164472. [Google Scholar] [CrossRef]
- Anandhan, A.; Dodson, M.; Shakya, A.; Chen, J.; Liu, P.; Wei, Y.; Tan, H.; Wang, Q.; Jiang, Z.; Yang, K.; et al. NRF2 controls iron homeostasis and ferroptosis through HERC2 and VAMP8. Sci. Adv. 2023, 9, eade9585. [Google Scholar] [CrossRef]
- Sharif, K.; Vieira Borba, V.; Zandman-Goddard, G.; Shoenfeld, Y. Eppur Si Muove: Ferritin is essential in modulating inflammation. Clin. Exp. Immunol. 2018, 191, 149–150. [Google Scholar] [CrossRef]
- Arosio, P.; Elia, L.; Poli, M. Ferritin, cellular iron storage and regulation. IUBMB Life 2017, 69, 414–422. [Google Scholar] [CrossRef]
- Kell, D.B.; Pretorius, E. Serum ferritin is an important inflammatory disease marker, as it is mainly a leakage product from damaged cells. Met. Integr. Biometal Sci. 2014, 6, 748–773. [Google Scholar] [CrossRef] [PubMed]
- Depalma, R.G.; Hayes, V.W.; Chow, B.K.; Shamayeva, G.; May, P.E.; Zacharski, L.R. Ferritin levels, inflammatory biomarkers, and mortality in peripheral arterial disease: A substudy of the Iron (Fe) and Atherosclerosis Study (FeAST) Trial. J. Vasc. Surg. 2010, 51, 1498–1503. [Google Scholar] [CrossRef]
- Hayıroğlu, M.; Çınar, T.; Çinier, G.; Pay, L.; Yumurtaş, A.; Tezen, O.; Eren, S.; Kolak, Z.; Çetin, T.; Çiçek, V.; et al. Evaluating systemic immune-inflammation index in patients with implantable cardioverter defibrillator for heart failure with reduced ejection fraction. Pacing Clin. Electrophysiol. PACE 2022, 45, 188–195. [Google Scholar] [CrossRef]
- Çinier, G.; Hayıroğlu, M.; Pay, L.; Yumurtaş, A.; Tezen, O.; Eren, S.; Kolak, Z.; Çetin, T.; Özcan, S.; Türkkan, C.; et al. Prognostic nutritional index as the predictor of long-term mortality among HFrEF patients with ICD. Pacing Clin. Electrophysiol. PACE 2021, 44, 490–496. [Google Scholar] [CrossRef]
- Çinier, G.; Hayıroğlu, M.; Kolak, Z.; Tezen, O.; Yumurtaş, A.; Pay, L.; Eren, S.; Çetin, T.; Özcan, S.; Türkkan, C.; et al. The value of C-reactive protein-to-albumin ratio in predicting long-term mortality among HFrEF patients with implantable cardiac defibrillators. Eur. J. Clin. Investig. 2021, 51, e13550. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.K.; Yun, B.H.; Chon, S.J.; Lee, Y.J.; Han, E.J.; Park, J.H.; Cho, S.; Choi, Y.S.; Lee, B.S. Association of serum ferritin levels with metabolic syndrome and subclinical coronary atherosclerosis in postmenopausal Korean women. Clin. Chim. Acta Int. J. Clin. Chem. 2015, 438, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Liu, T.; Jia, C. Joint effects of serum ferritin and body mass index on the risk of coronary artery disease: A case-control study. BMJ Open 2013, 3, e003695. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Ortegon, M.F.; McLachlan, S.; Fernandez-Real, J.M.; Tuomainen, T.P.; Aregbesola, A.; Wild, S.H. Serum ferritin and incident cardiometabolic diseases in Scottish adults. Cardiovasc. Diabetol. 2022, 21, 26. [Google Scholar] [CrossRef]
- Egbuche, O.; Millard, H.R.; Renelus, B.; Maihemuti, A.; Musani, S.K.; Fox, E.R.; Liu, J.; Taylor, H.A.; Bidulescu, A. Serum Ferritin Levels in Blacks Without Known Cardiovascular Disease (from the Jackson Heart Study). Am. J. Cardiol. 2017, 120, 1533–1540. [Google Scholar] [CrossRef]
- Friedrich, N.; Milman, N.; Volzke, H.; Linneberg, A.; Jorgensen, T. Is serum ferritin within the reference range a risk predictor of cardiovascular disease? A population-based, long-term study comprising 2874 subjects. Br. J. Nutr. 2009, 102, 594–600. [Google Scholar] [CrossRef]
- Johnson, A.; Bulgarelli, L.; Pollard, T.; Horng, S.; Celi, L.A.; Mark, R. MIMIC-IV (version 2.0). PhysioNet 2022. [Google Scholar] [CrossRef]
- Leitch, H.A.; Buckstein, R.; Zhu, N.; Nevill, T.J.; Yee, K.W.L.; Leber, B.; Keating, M.M.; St Hilaire, E.; Kumar, R.; Delage, R.; et al. Iron overload in myelodysplastic syndromes: Evidence based guidelines from the Canadian consortium on MDS. Leuk. Res. 2018, 74, 21–41. [Google Scholar] [CrossRef] [PubMed]
- Cullis, J.O.; Fitzsimons, E.J.; Griffiths, W.J.; Tsochatzis, E.; Thomas, D.W.; British Society for Haematology. Investigation and management of a raised serum ferritin. Br. J. Haematol. 2018, 181, 331–340. [Google Scholar] [CrossRef]
- Van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Li, F.; Thomas, L.E.; Li, F. Addressing Extreme Propensity Scores via the Overlap Weights. Am. J. Epidemiol. 2019, 188, 250–257. [Google Scholar] [CrossRef]
- Feng, Y.; Wang, Q.; Chen, G.; Ye, D.; Xu, W. Impaired renal function and abnormal level of ferritin are independent risk factors of left ventricular aneurysm after acute myocardial infarction: A hospital-based case-control study. Medicine 2018, 97, e12109. [Google Scholar] [CrossRef]
- Duarte, T.; Goncalves, S.; Sa, C.; Rodrigues, R.; Marinheiro, R.; Fonseca, M.; Seixo, F.; Caria, R. Prognostic Impact of Iron Metabolism Changes in Patients with Acute Coronary Syndrome. Arq. Bras. Cardiol. 2018, 111, 144–150. [Google Scholar] [CrossRef]
- Silvestre, O.M.; Gonçalves, A.; Nadruz, W., Jr.; Claggett, B.; Couper, D.; Eckfeldt, J.H.; Pankow, J.S.; Anker, S.D.; Solomon, S.D. Ferritin levels and risk of heart failure—The Atherosclerosis Risk in Communities Study. Eur. J. Heart Fail. 2017, 19, 340–347. [Google Scholar] [CrossRef]
- Fuernau, G.; Traeder, F.; Lele, S.S.; Rajapurkar, M.M.; Mukhopadhyay, B.; de Waha, S.; Desch, S.; Eitel, I.; Schuler, G.; Adams, V.; et al. Catalytic iron in acute myocardial infarction complicated by cardiogenic shock—A biomarker substudy of the IABP-SHOCK II-trial. Int. J. Cardiol. 2017, 227, 83–88. [Google Scholar] [CrossRef]
- Ponikowska, B.; Suchocki, T.; Paleczny, B.; Olesinska, M.; Powierza, S.; Borodulin-Nadzieja, L.; Reczuch, K.; von Haehling, S.; Doehner, W.; Anker, S.D.; et al. Iron status and survival in diabetic patients with coronary artery disease. Diabetes Care 2013, 36, 4147–4156. [Google Scholar] [CrossRef]
- Gurgoze, M.T.; Kardys, I.; Akkerhuis, K.M.; Oemrawsingh, R.M.; Groot, H.E.; van der Harst, P.; Umans, V.A.; Kietselaer, B.; Ronner, E.; Lenderink, T.; et al. Relation of Iron Status to Prognosis After Acute Coronary Syndrome. Am. J. Cardiol. 2022, 168, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Barywani, S.B.; Ostgard Thunstrom, E.; Mandalenakis, Z.; Hansson, P.O. Body iron stores had no impact on coronary heart disease outcomes: A middle-aged male cohort from the general population with 21-year follow-up. Open Heart 2022, 9, e001928. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Kawasaki, N.K.; Min, J.; Matsui, T.; Wang, F. Ferroptosis in heart failure. J. Mol. Cell. Cardiol. 2022, 173, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Qiao, Y.; Wang, D.; Tang, C.; Yan, G. Ferritinophagy and ferroptosis in cardiovascular disease: Mechanisms and potential applications. Biomed. Pharmacother. Biomed. Pharmacother. 2021, 141, 111872. [Google Scholar] [CrossRef]
- Mancardi, D.; Mezzanotte, M.; Arrigo, E.; Barinotti, A.; Roetto, A. Iron Overload, Oxidative Stress, and Ferroptosis in the Failing Heart and Liver. Antioxidants 2021, 10, 1864. [Google Scholar] [CrossRef]
- Ajoolabady, A.; Aslkhodapasandhokmabad, H.; Libby, P.; Tuomilehto, J.; Lip, G.Y.H.; Penninger, J.M.; Richardson, D.R.; Tang, D.; Zhou, H.; Wang, S.; et al. Ferritinophagy and ferroptosis in the management of metabolic diseases. Trends Endocrinol. Metab. TEM 2021, 32, 444–462. [Google Scholar] [CrossRef]
- Fang, X.; Ardehali, H.; Min, J.; Wang, F. The molecular and metabolic landscape of iron and ferroptosis in cardiovascular disease. Nat. Rev. Cardiol. 2023, 20, 7–23. [Google Scholar] [CrossRef]
- Valenti, L.; Corradini, E.; Adams, L.A.; Aigner, E.; Alqahtani, S.; Arrese, M.; Bardou-Jacquet, E.; Bugianesi, E.; Fernandez-Real, J.M.; Girelli, D.; et al. Consensus Statement on the definition and classification of metabolic hyperferritinaemia. Nat. Rev. Endocrinol. 2023, 19, 299–310. [Google Scholar] [CrossRef]
- Hayıroğlu, M.; Altay, S. The Role of Artificial Intelligence in Coronary Artery Disease and Atrial Fibrillation. Balk. Med. J. 2023, 40, 151–152. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable Name | Unmatched | After Propensity Score Weighting | ||||
|---|---|---|---|---|---|---|
| Control | Iron Overload | SMD | Control | Iron Overload | SMD | |
| No. | 951 | 222 | 951 | 222 | ||
| Log2(Ferritin) (mean (SD)) | 7.60 (1.52) | 11.20 (1.43) | 2.434 | 7.81 (1.45) | 11.06 (1.25) | 2.402 |
| Demographic | ||||||
| Age (mean (SD)) | 72.27 (12.51) | 69.77 (12.45) | 0.200 | 71.39 (12.25) | 70.50 (12.54) | 0.072 |
| Gender (Female %) | 366 (38.5) | 72 (32.4) | 0.127 | 46.4 (36.8) | 39.3 (31.2) | 0.118 |
| BMI (mean (SD)) | 29.04 (7.32) | 28.96 (8.28) | 0.010 | 29.08 (7.30) | 29.04 (8.56) | 0.005 |
| Race (White %) | 640 (67.3) | 136 (61.3) | 0.126 | 82.7 (65.6) | 76.4 (60.7) | 0.103 |
| Severity of Illness | ||||||
| SAPSII Score (mean (SD)) | 40.04 (13.04) | 45.93 (13.51) | 0.444 | 43.60 (13.78) | 44.14 (12.74) | 0.041 |
| SOFA Score (mean (SD)) | 6.05 (3.67) | 8.34 (4.04) | 0.594 | 7.31 (3.94) | 7.77 (3.82) | 0.117 |
| Charlson Comorbidity Score (mean (SD)) | 7.52 (2.57) | 8.00 (2.67) | 0.185 | 7.78 (2.67) | 7.90 (2.69) | 0.043 |
| GCS Score (mean (SD)) | 13.74 (2.63) | 13.75 (2.37) | 0.006 | 13.60 (2.76) | 13.81 (2.23) | 0.084 |
| MBP (1st 24 h) (mean (SD)) | 56.49 (12.31) | 54.56 (13.63) | 0.148 | 55.18 (12.78) | 55.19 (13.91) | 0.001 |
| Heart Rate (1st 24 h) (mean (SD)) | 102.49 (21.10) | 110.92 (24.97) | 0.365 | 105.48 (21.72) | 108.92 (23.63) | 0.152 |
| Spo2 (mean (SD)) | 91.77 (6.59) | 90.99 (6.52) | 0.118 | 91.13 (7.92) | 91.00 (6.16) | 0.019 |
| Comorbidities | ||||||
| CHF (%) | 611 (64.2) | 120 (54.1) | 0.209 | 77.9 (61.9) | 69.7 (55.3) | 0.133 |
| Arrhythmias (%) | 596 (62.7) | 135 (60.8) | 0.038 | 79.3 (62.9) | 78.0 (62.0) | 0.02 |
| PVD (%) | 205 (21.6) | 43 (19.4) | 0.054 | 26.4 (21.0) | 23.4 (18.6) | 0.059 |
| Stroke (%) | 138 (14.5) | 35 (15.8) | 0.035 | 20.2 (16.0) | 21.0 (16.7) | 0.019 |
| COPD (%) | 329 (34.6) | 76 (34.2) | 0.008 | 43.1 (34.2) | 44.3 (35.2) | 0.020 |
| Diabetes (%) | 420 (44.2) | 92 (41.4) | 0.055 | 56.0 (44.4) | 52.4 (41.6) | 0.058 |
| Liver (%) | 121 (12.7) | 47 (21.2) | 0.227 | 21.9 (17.3) | 21.7 (17.2) | 0.004 |
| Renal (%) | 392 (41.2) | 90 (40.5) | 0.014 | 53.2 (42.2) | 50.2 (39.8) | 0.048 |
| Malignancy (%) | 90 (9.5) | 49 (22.1) | 0.351 | 17.7 (14.0) | 23.1 (18.4) | 0.118 |
| Interventions | ||||||
| PCI (%) | 93 (9.8) | 19 (8.6) | 0.042 | 11.7 (9.2) | 10.8 (8.6) | 0.023 |
| CABG (%) | 100 (10.5) | 17 (7.7) | 0.100 | 11.0 (8.7) | 11.2 (8.9) | 0.005 |
| Sedative Use (1st 24 h) (%) | 392 (41.2) | 109 (49.1) | 0.159 | 60.3 (47.9) | 60.5 (48.0) | 0.003 |
| Vasopressor Use (1st 24 h) (%) | 383 (40.3) | 114 (51.4) | 0.224 | 60.0 (47.7) | 61.8 (49.1) | 0.028 |
| Mechanical Ventilation Use (1st 24 h) (%) | 283 (29.8) | 86 (38.7) | 0.190 | 44.9 (35.7) | 47.9 (38.0) | 0.049 |
| Laboratory Tests | ||||||
| Lactate (mean (SD)) | 2.53 (2.08) | 3.29 (3.18) | 0.281 | 2.87 (2.44) | 2.98 (2.65) | 0.041 |
| WBC (mean (SD)) | 13.96 (9.46) | 15.27 (8.96) | 0.143 | 14.97 (11.04) | 15.07 (9.05) | 0.010 |
| Hemoglobin (mean (SD)) | 9.28 (2.08) | 8.95 (2.26) | 0.153 | 9.18 (2.10) | 9.11 (2.24) | 0.029 |
| Platelet (mean (SD)) | 191.63 (100.62) | 174.87 (110.71) | 0.158 | 182.24 (110.48) | 180.92 (105.51) | 0.012 |
| ALT (mean (SD)) | 109.17 (381.26) | 310.63 (914.97) | 0.287 | 180.37 (540.80) | 213.87 (668.90) | 0.055 |
| AST (mean (SD)) | 166.09 (641.56) | 547.70 (1732.55) | 0.292 | 280.69 (898.54) | 350.47 (1203.38) | 0.066 |
| Total Bilirubin (mean (SD)) | 1.16 (1.94) | 2.69 (5.79) | 0.353 | 1.57 (2.76) | 1.88 (4.29) | 0.085 |
| BUN (mean (SD)) | 40.38 (29.23) | 46.53 (33.98) | 0.194 | 45.11 (32.85) | 45.39 (34.09) | 0.008 |
| Creatinine (mean (SD)) | 2.05 (2.19) | 2.98 (2.90) | 0.362 | 2.56 (3.18) | 2.75 (2.88) | 0.065 |
| Glucose (mean (SD)) | 184.07 (106.79) | 202.19 (111.74) | 0.166 | 194.39 (118.00) | 202.39 (118.02) | 0.068 |
| Cholesterol (tested) (%) | 160 (16.8) | 32 (14.4) | 0.066 | 19.1 (15.2) | 19.0 (15.1) | 0.002 |
| Sodium (mean (SD)) | 139.39 (5.15) | 139.88 (4.82) | 0.097 | 139.45 (5.31) | 139.83 (4.79) | 0.075 |
| Potassium (mean (SD)) | 4.72 (0.86) | 4.82 (0.98) | 0.110 | 4.81 (0.95) | 4.83 (0.97) | 0.018 |
| Calcium (mean (SD)) | 8.43 (1.48) | 8.37 (1.32) | 0.041 | 8.41 (1.43) | 8.38 (1.35) | 0.019 |
| Bicarbonate (mean (SD)) | 21.34 (5.20) | 19.58 (5.65) | 0.324 | 20.20 (5.32) | 19.99 (5.45) | 0.039 |
| Chloride (mean (SD)) | 104.57 (6.77) | 104.41 (6.55) | 0.024 | 104.74 (6.98) | 104.66 (6.35) | 0.013 |
| Anion Gap (mean (SD)) | 17.25 (4.84) | 19.72 (6.19) | 0.444 | 18.41 (5.34) | 18.85 (5.50) | 0.081 |
| INR (mean (SD)) | 1.70 (1.13) | 1.88 (1.49) | 0.137 | 1.81 (1.36) | 1.76 (1.25) | 0.042 |
| Iron (mean (SD)) | 46.70 (42.93) | 70.23 (62.37) | 0.440 | 47.41 (45.43) | 64.21 (53.40) | 0.339 |
| Creatinine Kinase (tested) (%) | 612 (64.4) | 158 (71.2) | 0.146 | 86.0 (68.2) | 85.9 (68.2) | 0.001 |
| Creatinine Kinase-MB (tested) (%) | 622 (65.4) | 159 (71.6) | 0.134 | 86.8 (68.9) | 89.7 (71.2) | 0.051 |
| Troponin (tested) (%) | 594 (62.5) | 158 (71.2) | 0.186 | 84.3 (66.9) | 89.8 (71.3) | 0.095 |
| BNP (tested) (%) | 278 (29.2) | 60 (27.0) | 0.049 | 32.5 (25.8) | 31.6 (25.1) | 0.016 |
| Primary Analysis | ||||
|---|---|---|---|---|
| 90-Day Mortality | ||||
| Cox Regression | HR | CIL | CIU | p value |
| Model 1 | 2.03 | 1.62 | 2.55 | <0.001 |
| Model 2 | 2.10 | 1.67 | 2.64 | <0.001 |
| Model 3 | 1.63 | 1.27 | 2.09 | <0.001 |
| Cox Analysis after Weighting | 1.50 | 1.17 | 1.93 | 0.001 |
| 1-Year Mortality | ||||
| Cox Regression | HR | CIL | CIU | p value |
| Model 1 | 1.79 | 1.46 | 2.20 | <0.001 |
| Model 2 | 1.89 | 1.54 | 2.32 | <0.001 |
| Model 3 | 1.49 | 1.19 | 1.86 | <0.001 |
| Cox Analysis after Weighting | 1.35 | 1.08 | 1.69 | 0.008 |
| Secondary Analysis | ||||
|---|---|---|---|---|
| Length of Stay in ICU | ||||
| Linear Regression | Coef. | S.E. | t-value | p value |
| Model 1 | 2.58 | 0.65 | 3.99 | <0.001 |
| Model 2 | 2.42 | 0.65 | 3.72 | <0.001 |
| Model 3 | 0.96 | 0.61 | 1.58 | 0.115 |
| In-Hospital Mortality | ||||
| Logistic Regression | OR | CIL | CIU | p value |
| Model 1 | 2.61 | 1.86 | 3.65 | <0.001 |
| Model 2 | 2.70 | 1.91 | 3.80 | <0.001 |
| Model 3 | 1.88 | 1.24 | 2.81 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, S.; Chen, M.; Tang, L.; Li, X.; Zhou, S. Association between Serum Ferritin and Prognosis in Patients with Ischemic Heart Disease in Intensive Care Units. J. Clin. Med. 2023, 12, 6547. https://doi.org/10.3390/jcm12206547
Liu S, Chen M, Tang L, Li X, Zhou S. Association between Serum Ferritin and Prognosis in Patients with Ischemic Heart Disease in Intensive Care Units. Journal of Clinical Medicine. 2023; 12(20):6547. https://doi.org/10.3390/jcm12206547
Chicago/Turabian StyleLiu, Shun, Mingxian Chen, Liang Tang, Xuping Li, and Shenghua Zhou. 2023. "Association between Serum Ferritin and Prognosis in Patients with Ischemic Heart Disease in Intensive Care Units" Journal of Clinical Medicine 12, no. 20: 6547. https://doi.org/10.3390/jcm12206547
APA StyleLiu, S., Chen, M., Tang, L., Li, X., & Zhou, S. (2023). Association between Serum Ferritin and Prognosis in Patients with Ischemic Heart Disease in Intensive Care Units. Journal of Clinical Medicine, 12(20), 6547. https://doi.org/10.3390/jcm12206547