
A New Perspective for Potential Organ Damage Due to Iron-Mediated Oxidation in Thalassemia Major Patients
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Origa, R. Beta-Thalassemia. Genet. Med. Off. J. Am. Coll. Med. Genet. 2017, 19, 609–619. [Google Scholar] [CrossRef] [Green Version]
- Al, I.O.; Ayçiçek, A.; Ersoy, G.; Bayram, C.; Neselioglu, S.; Erel, Ö. Thiol Disulfide Homeostasis and Ischemia-modified Albumin Level in Children With Beta-Thalassemia. J. Pediatr. Hematol./Oncol. 2019, 41, e463–e466. [Google Scholar]
- Canatan, D. Türkiye’de hemoglobinopatilerin epidemiyolojisi. Hematolog 2014, 4, 11–22. [Google Scholar]
- Fibach, E.; Dana, M. Oxidative Stress in beta-Thalassemia. Mol. Diagn. Ther. 2019, 23, 245–261. [Google Scholar] [CrossRef]
- Meral, A.; Tuncel, P.; Sürmen-Gür, E.; Özbek, R.; Öztürk, E.; GÜnay, Ü. Lipid peroxidation and antioxidant status in ß-thalassemia. Pediatr. Hematol. Oncol. 2000, 17, 687–693. [Google Scholar] [CrossRef]
- Fibach, E.; Rachmilewitz, E. The role of oxidative stress in hemolytic anemia. Curr. Mol. Med. 2008, 8, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Centis, F.; Tabellini, L.; Lucarelli, G.; Buffi, O.; Tonucci, P.; Persini, B.; Annibali, M.; Emiliani, R.; Iliescu, A.; Rapa, S. The importance of erythroid expansion in determining the extent of apoptosis in erythroid precursors in patients with β-thalassemia major. Blood J. Am. Soc. Hematol. 2000, 96, 3624–3629. [Google Scholar]
- Thein, S.L. 3 β-Thalassaemia. Baillière’s Clin. Haematol. 1998, 11, 91–126. [Google Scholar]
- Patpan, N.; Banjerdpongchai, R.; Tantiworawit, A.; Poofery, J.; Komonrit, P.; Fanhchaksai, K.; Rattanathammethee, T.; Chai-Adisaksopha, C.; Rattarittamrong, E.; Norasetthada, L. The Effect of Transfusion-Dependent Thalassemia Patient’s Serum on Peripheral Blood Mononuclear Cell Viability. J. Cell Death 2019, 12, 1179066018823534. [Google Scholar] [CrossRef] [Green Version]
- Erel, O.; Neselioglu, S. A novel and automated assay for thiol/disulphide homeostasis. Clin. Biochem. 2014, 47, 326–332. [Google Scholar] [CrossRef]
- Erel, O.; Erdoğan, S. Thiol-disulfide homeostasis: An integrated approach with biochemical and clinical aspects. Turk. J. Med. Sci. 2020, 50, 1728–1738. [Google Scholar] [PubMed]
- Finkel, T.; Holbrook, N.J. Oxidants, oxidative stress and the biology of ageing. Nature 2000, 408, 239–247. [Google Scholar] [CrossRef]
- Erel, O. A new automated colorimetric method for measuring total oxidant status. Clin. Biochem. 2005, 38, 1103–1111. [Google Scholar] [CrossRef] [PubMed]
- Awadallah, S.M.; Nimer, N.A.; Atoum, M.F.; Saleh, S.A. Association of haptoglobin phenotypes with ceruloplasmin ferroxidase activity in β-thalassemia major. Clin. Chim. Acta 2011, 412, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Awadallah, S.M.; Atoum, M.F.; Nimer, N.A.; Saleh, S.A. Ischemia modified albumin: An oxidative stress marker in β-thalassemia major. Clin. Chim. Acta 2012, 413, 907–910. [Google Scholar] [PubMed]
- Roxborough, H.E.; Mercer, C.; McMaster, D.; Maxwell, A.P.; Young, I.S. The ferroxidase activity of caeruloplasmin is reduced in haemodialysis patients. Nephron 2000, 84, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Bar–Or, D.; Lau, E.; Winkler, J.V. A novel assay for cobalt-albumin binding and its potential as a marker for myocardial ischemia—A preliminary report. J. Emerg. Med. 2000, 19, 311–315. [Google Scholar] [CrossRef]
- Erel, O. A novel automated direct measurement method for total antioxidant capacity using a new generation, more stable ABTS radical cation. Clin. Biochem. 2004, 37, 277–285. [Google Scholar] [CrossRef]
- Neselioglu, S.; Ergin, M.; Erel, O. A new kinetic, automated assay to determine the ferroxidase activity of ceruloplasmin. Anal. Sci. 2017, 33, 1339–1344. [Google Scholar] [CrossRef] [Green Version]
- Guzelcicek, A.; Cakirca, G.; Erel, O.; Solmaz, A. Assessment of thiol/disulfide balance as an oxidative stress marker in children with β-thalassemia major. Pak. J. Med. Sci. 2019, 35, 161. [Google Scholar]
- Vichinsky, E.; Butensky, E.; Fung, E.; Hudes, M.; Theil, E.; Ferrell, L.; Williams, R.; Louie, L.; Lee, P.D.; Harmatz, P. Comparison of organ dysfunction in transfused patients with SCD or β thalassemia. Am. J. Hematol. 2005, 80, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Birben, E.; Sahiner, U.M.; Sackesen, C.; Erzurum, S.; Kalayci, O. Oxidative stress and antioxidant defense. World Allergy Organ. J. 2012, 5, 9–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clemens, M.R. Antioxidant therapy in hematological disorders. Antioxid. Ther. Prev. Med. 1990, 264, 423–433. [Google Scholar]
- Kattamis, C.; Kattamis, A.C. Oxidative stress disturbances in erythrocytes of ß-thalassemia. Pediatr. Hematol. Oncol. 2001, 18, 85–88. [Google Scholar] [CrossRef]
- Tekin, M.; Akar, N.; Egin, Y.; Cin, S. Serum superoxide dismutase levels of beta thalassemia patients and effects of high dosage of intravenous desferrioxamine treatment on superoxide dismutase levels. Pediatr. Hematol. Oncol. 1998, 15, 371–374. [Google Scholar] [CrossRef]
- Waseem, F.; Khemomal, K.A.; Sajid, R. Antioxidant status in beta thalassemia major: A single-center study. Indian J. Pathol. Microbiol. 2011, 54, 761. [Google Scholar]
- Cakmak, A.; Soker, M.; Koc, A.; Aksoy, N. Prolidase activity and oxidative status in patients with thalassemia major. J. Clin. Lab. Anal. 2010, 24, 6–11. [Google Scholar] [CrossRef]
- Awadallah, S.; Al Arrayed, K.; Bahareth, E.; Saeed, Z. Total antioxidant capacity and ischemia modified albumin in beta thalassemia. Clin. Lab. 2013, 59, 687–691. [Google Scholar] [CrossRef]
- Boudrahem-Addour, N.; Izem-Meziane, M.; Bouguerra, K.; Nadjem, N.; Zidani, N.; Belhani, M.; Djerdjouri, B. Oxidative status and plasma lipid profile in β-thalassemia patients. Hemoglobin 2015, 39, 36–41. [Google Scholar] [CrossRef]
- Kalpravidh, R.W.; Siritanaratkul, N.; Insain, P.; Charoensakdi, R.; Panichkul, N.; Hatairaktham, S.; Srichairatanakool, S.; Phisalaphong, C.; Rachmilewitz, E.; Fucharoen, S. Improvement in oxidative stress and antioxidant parameters in β-thalassemia/Hb E patients treated with curcuminoids. Clin. Biochem. 2010, 43, 424–429. [Google Scholar] [CrossRef]
- Floris, G.; Medda, R.; Padiglia, A.; Musci, G. The physiopathological significance of ceruloplasmin: A possible therapeutic approach. Biochem. Pharmacol. 2000, 60, 1735–1741. [Google Scholar] [CrossRef] [PubMed]
- Valko, M.; Leibfritz, D.; Moncol, J.; Cronin, M.T.; Mazur, M.; Telser, J. Free radicals and antioxidants in normal physiological functions and human disease. Int. J. Biochem. Cell Biol. 2007, 39, 44–84. [Google Scholar] [CrossRef]
- Camiolo, G.; Tibullo, D.; Giallongo, C.; Romano, A.; Parrinello, N.L.; Musumeci, G.; Di Rosa, M.; Vicario, N.; Brundo, M.V.; Amenta, F. α-Lipoic acid reduces iron-induced toxicity and oxidative stress in a model of iron overload. Int. J. Mol. Sci. 2019, 20, 609. [Google Scholar] [CrossRef] [Green Version]
- Jamshidi, K.; Abdollahzad, H.; Nachvak, M.; Rezaei, M.; Golpayegani, M.R.; Zahabi, E.S. Effects of alpha-lipoic acid supplementation on cardiovascular disease risk factors in β-thalassemia major patients: A clinical trial crossover study. J. Blood Med. 2020, 11, 131. [Google Scholar] [PubMed]
- Ali, Y.F.; Desouky, O.S.; Selim, N.S.; Ereiba, K.M. Assessment of the role of α-lipoic acid against the oxidative stress of induced iron overload. J. Radiat. Res. Appl. Sci. 2015, 8, 26–35. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
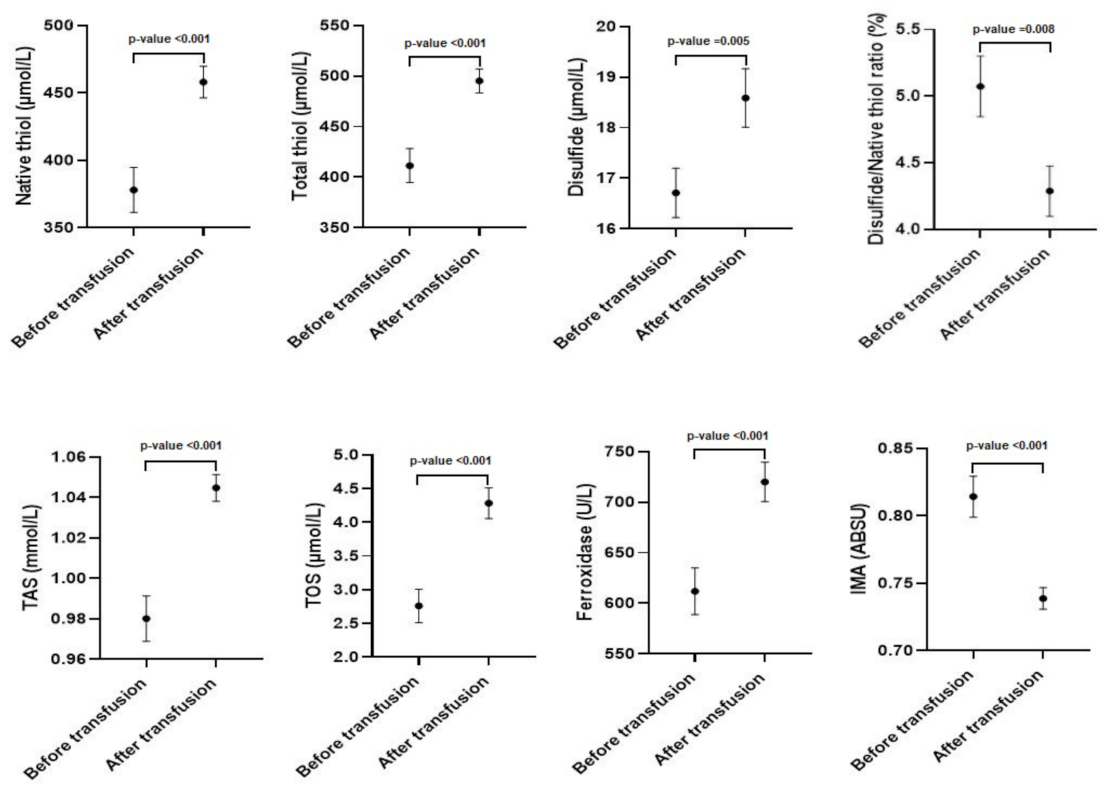
| Parameters | Before Transfusion | After Transfusion | p-Values |
|---|---|---|---|
| Native thiol (µmol/L) | 378.0 ± 150.2 | 458.0 ± 105.6 | <0.001 * |
| Total thiol (µmol/L) | 411.4 ± 152.1 | 495.2 ± 107.7 | <0.001 * |
| Disulfide (µmol/L) | 16.7 ± 3.4 | 18.5 ± 4.2 | =0.005 * |
| Disulfide/Native thiol ratio (%) | 5.1 ± 1.1 | 4.3 ± 0.7 | =0.008 * |
| TAS (mmol/L) | 0.98 ± 0.05 | 1.04 ± 0.06 | <0.001 * |
| Ferroxidase (U/L) | 611.8 ± 208.1 | 720.1 ± 176.9 | <0.001 * |
| IMA (ABSU) | 0.76 (0.14) | 0.73 (0.06) | <0.001 ** |
| TOS (µmol/L) | 2.14 (0.89) | 3.7 (2.15) | <0.001 ** |
| Parameters | Ferroxidase | TAS | TOS | IMA | |
|---|---|---|---|---|---|
| Native thiol | r | 0.704 | 0.492 | 0.438 | −0.775 |
| p | <0.001 * | <0.001 * | <0.001 * | <0.001 * | |
| Total thiol | r | 0.710 | 0.505 | 0.438 | −0.785 |
| p | <0.001 * | <0.001 * | <0.001 * | <0.001 * | |
| Disulfide | r | 0.256 | 0.328 | 0.099 | −0.331 |
| p | 0.02 * | 0.003 * | 0.377 | 0.002 * | |
| Disulfide/Native thiol | r | −0.567 | −0.376 | −0.298 | 0.692 |
| p | <0.001 * | <0.001 * | 0.007 * | <0.001 * | |
| Ferroxidase | r | 1 | 0.479 | 0.378 | −0.659 |
| p | <0.001 * | <0.001 * | <0.001 * | ||
| TAS | r | 0.479 | 1 | 0.186 | −0.703 |
| p | <0.001 * | 0.094 | <0.001 * | ||
| TOS | r | 0.378 | 0.186 | 1 | −0.291 |
| p | <0.001 * | 0.094 | 0.008 * | ||
| IMA | r | −0.659 | −0.703 | −0.291 | 1 |
| p | <0.001 * | <0.001 * | 0.008 * | ||
| Parameters | Ferroxidase | TAS | TOS | IMA | |
|---|---|---|---|---|---|
| Native thiol | r | 0.421 | 0.164 | 0.300 | −0.679 |
| p | <0.001 * | 0.140 | 0.006 * | <0.001 * | |
| Total thiol | r | 0.419 | 0.174 | 0.319 | −0.677 |
| p | <0.001 * | 0.118 | 0.003 * | <0.001 * | |
| Disulfide | r | 0.089 | 0.133 | 0.252 | −0.132 |
| p | 0.429 | 0.235 | 0.022 * | 0.238 | |
| Disulfide/Native thiol | r | −0.286 | −0.139 | 0.007 | 0.547 |
| p | 0.009 * | 0214 | 0.951 | <0.001 * | |
| Ferroxidase | r | 1 | 0.106 | 0.260 | −0.361 |
| p | 0.341 | 0.018 * | 0.001 * | ||
| TAS | r | 0.106 | 1 | 0.185 | −0.140 |
| p | 0.341 | 0.096 | 0.209 | ||
| TOS | r | 0.260 | 0.185 | 1 | −0.158 |
| p | 0.018 * | 0.096 | 0.155 | ||
| IMA | r | −0.361 | −0.140 | −0.158 | 1 |
| p | 0.001 * | 0.209 | 0.155 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eren, F.; Koca Yozgat, A.; Firat Oğuz, E.; Neşelioğlu, S.; Firat, R.; Gürlek Gökçebay, D.; Yarali, H.N.; Özbek, N.Y.; Erel, Ö. A New Perspective for Potential Organ Damage Due to Iron-Mediated Oxidation in Thalassemia Major Patients. J. Clin. Med. 2023, 12, 2422. https://doi.org/10.3390/jcm12062422
Eren F, Koca Yozgat A, Firat Oğuz E, Neşelioğlu S, Firat R, Gürlek Gökçebay D, Yarali HN, Özbek NY, Erel Ö. A New Perspective for Potential Organ Damage Due to Iron-Mediated Oxidation in Thalassemia Major Patients. Journal of Clinical Medicine. 2023; 12(6):2422. https://doi.org/10.3390/jcm12062422
Chicago/Turabian StyleEren, Funda, Ayça Koca Yozgat, Esra Firat Oğuz, Salim Neşelioğlu, Rıdvan Firat, Dilek Gürlek Gökçebay, Hüsniye Neşe Yarali, Namık Yaşar Özbek, and Özcan Erel. 2023. "A New Perspective for Potential Organ Damage Due to Iron-Mediated Oxidation in Thalassemia Major Patients" Journal of Clinical Medicine 12, no. 6: 2422. https://doi.org/10.3390/jcm12062422
APA StyleEren, F., Koca Yozgat, A., Firat Oğuz, E., Neşelioğlu, S., Firat, R., Gürlek Gökçebay, D., Yarali, H. N., Özbek, N. Y., & Erel, Ö. (2023). A New Perspective for Potential Organ Damage Due to Iron-Mediated Oxidation in Thalassemia Major Patients. Journal of Clinical Medicine, 12(6), 2422. https://doi.org/10.3390/jcm12062422