


Immediate and Long-Term Effectiveness of Proprioceptive Neuromuscular Facilitation and Static Stretching on Joint Range of Motion, Flexibility, and Electromyographic Activity of Knee Muscles in Older Adults

 , , ,
, , ,
Abstract
:1. Introduction
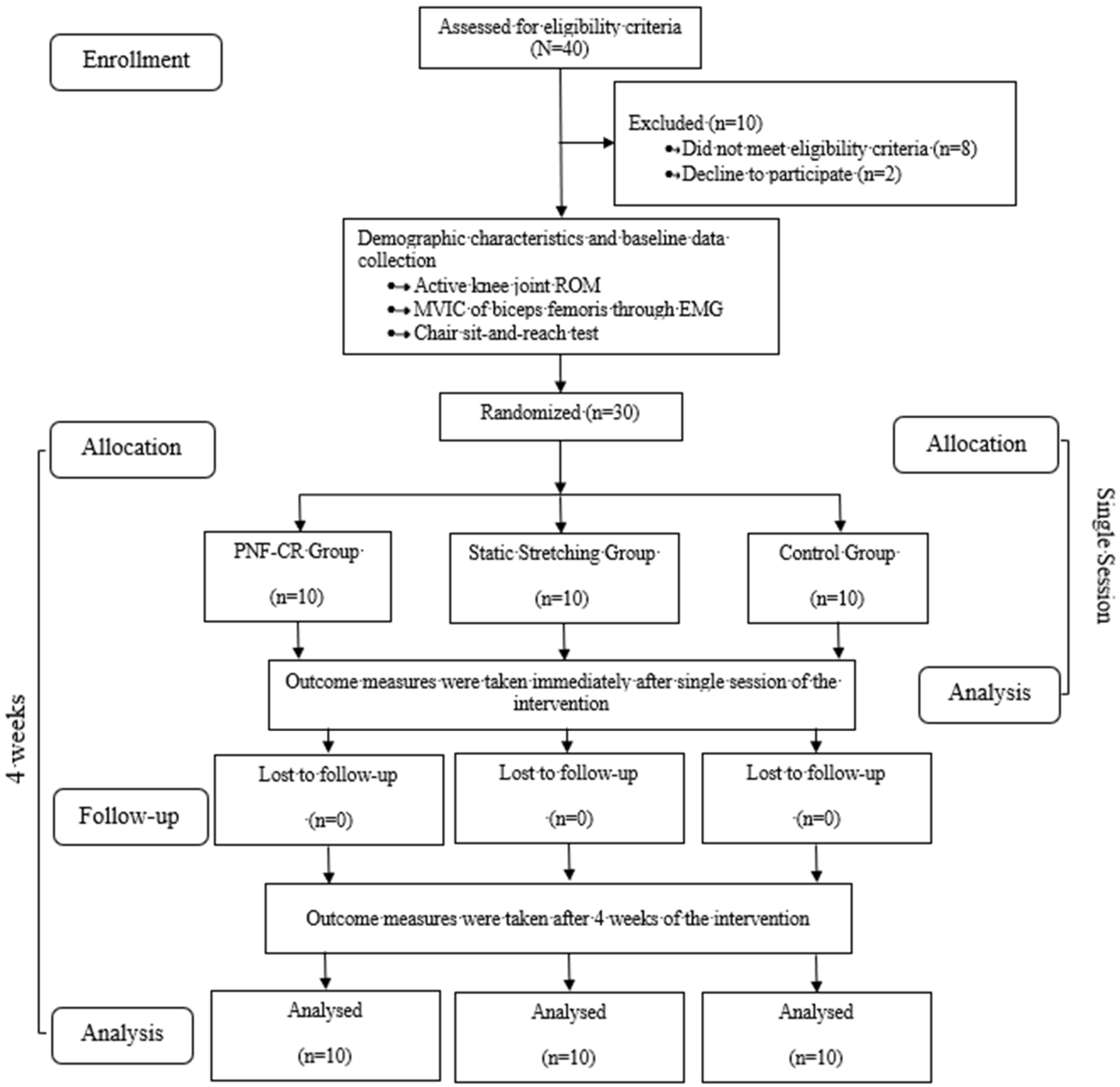
2. Methods
2.1. Sample Size Calculation
2.2. Participants
2.3. Study Design
2.4. Procedure
2.5. Intervention
2.5.1. PNF-CR Group
2.5.2. Static Stretching Group
2.6. Outcome Measures
2.6.1. Maximal Voluntary Isometric Contraction for Biceps Femoris
2.6.2. Active Knee Joint ROM Measurement
2.6.3. Chair Sit-and-Reach Test (CART)
2.7. Data Analysis
3. Result
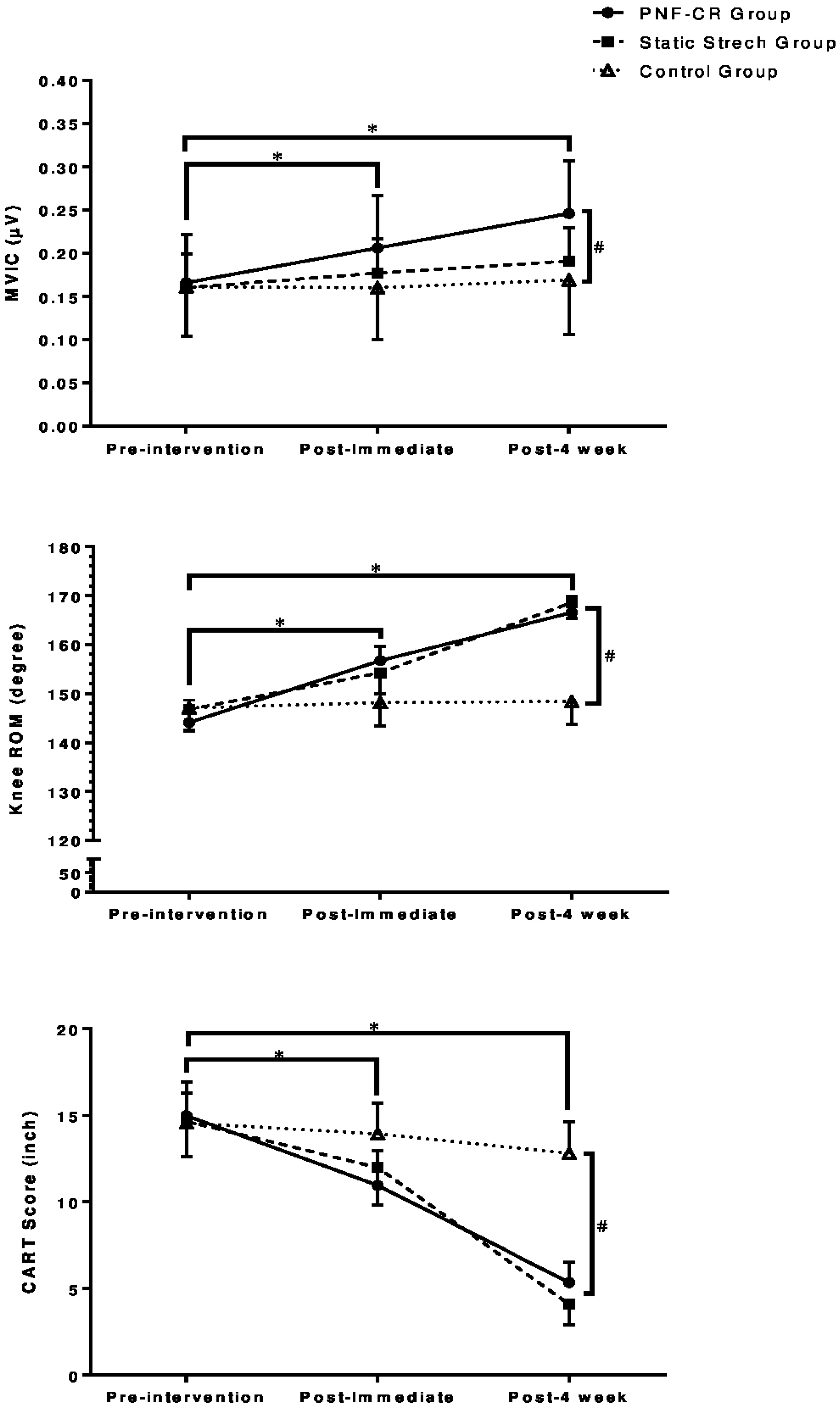
3.1. EMG Activity of Biceps Femoris Muscle
3.2. Active Knee Joint ROM
3.3. Chair Sit-and-Reach Test (CART)
4. Discussion
Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bryanton, M.; Bilodeau, M. The role of thigh muscular efforts in limiting sit-to-stand capacity in healthy young and older adults. Aging Clin. Exp. Res. 2017, 29, 1211–1219. [Google Scholar] [CrossRef] [PubMed]
- Ferber, R.; Osternig, L.R.; Gravelle, D.C. Effect of PNF stretch techniques on knee flexor muscle EMG activity in older adults. J. Electromyogr. Kinesiol. 2002, 12, 391–397. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, G.; Kirschner, J.; Prather, H.; Goldman, D.; Rozanski, A. Musculoskeletal exercise: Its role in promoting health and longevity. Prog. Cardiovasc. Dis. 2023. [Google Scholar] [CrossRef]
- Phu, S.; Sturnieks, D.L.; Lord, S.R.; Okubo, Y. Impact of ageing, fall history and exercise on postural reflexes following unpredictable perturbations: A systematic review and meta-analyses. Mech. Ageing Dev. 2022, 203, 111634. [Google Scholar] [CrossRef] [PubMed]
- Siebert, T.; Donath, L.; Borsdorf, M.; Stutzig, N. Effect of Static Stretching, Dynamic Stretching, and Myofascial Foam Rolling on Range of Motion During Hip Flexion: A Randomized Crossover Trial. J. Strength Cond. Res. 2022, 36, 680–685. [Google Scholar] [CrossRef]
- Sharman, M.J.; Cresswell, A.G.; Riek, S. Proprioceptive Neuromuscular Facilitation Stretching: Mechanisms and Clinical Implications. Sports Med. 2006, 36, 929–939. [Google Scholar] [CrossRef]
- Fukaya, T.; Konrad, A.; Sato, S.; Kiyono, R.; Yahata, K.; Yasaka, K.; Onuma, R.; Yoshida, R.; Nakamura, M. Comparison Between Contract–Relax Stretching and Antagonist Contract–Relax Stretching on Gastrocnemius Medialis Passive Properties. Front. Physiol. 2022, 12, 764792. [Google Scholar] [CrossRef]
- Feland, J.B.; Myrer, J.W.; Schulthies, S.S.; Fellingham, G.W.; Measom, G.W. The effect of duration of stretching of the hamstring muscle group for increasing range of motion in people aged 65 years or older. Phys. Ther. 2001, 81, 1110–1117. [Google Scholar] [CrossRef]
- Yuktasir, B.; Kaya, F. Investigation into the long-term effects of static and PNF stretching exercises on range of motion and jump performance. J. Bodyw. Mov. Ther. 2009, 13, 11–21. [Google Scholar] [CrossRef]
- Higgs, F.; Winter, S.L. The Effect of a Four-Week Proprioceptive Neuromuscular Facilitation Stretching Program on Isokinetic Torque Production. J. Strength Cond. Res. 2009, 23, 1442–1447. [Google Scholar] [CrossRef] [Green Version]
- O’Hora, J.; Cartwright, A.; Wade, C.D.; Hough, A.D.; Shum, G.L. Efficacy of Static Stretching and Proprioceptive Neuromuscular Facilitation Stretch on Hamstrings Length After a Single Session. J. Strength Cond. Res. 2011, 25, 1586–1591. [Google Scholar] [CrossRef]
- Rowlands, A.V.; Marginson, V.F.; Lee, J. Chronic Flexibility Gains: Effect of Isometric Contraction Duration during Proprioceptive Neuromuscular Facilitation Stretching Techniques. Res. Q. Exerc. Sport 2003, 74, 47–51. [Google Scholar] [CrossRef]
- Konrad, A.; Gad, M.; Tilp, M. Effect of PNF stretching training on the properties of human muscle and tendon structures: Effect of PNF stretching training. Scand. J. Med. Sci. Sports 2015, 25, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Ghram, A.; Damak, M.; Rhibi, F.; Marchetti, P.H. The contract-relax proprioceptive neuromuscular facilitation (PNF) stretching can affect the dynamic balance in healthy men. Med. Express 2016, 3, 4. [Google Scholar] [CrossRef]
- Grabowska, W.; Burton, W.; Kowalski, M.H.; Vining, R.; Long, C.R.; Lisi, A.; Hausdorff, J.M.; Manor, B.; Muñoz-Vergara, D.; Wayne, P.M. A systematic review of chiropractic care for fall prevention: Rationale, state of the evidence, and recommendations for future research. BMC Musculoskelet. Disord. 2022, 23, 844. [Google Scholar] [CrossRef] [PubMed]
- Borges, M.O.; Medeiros, D.M.; Minotto, B.B.; Lima, C.S. Comparison between static stretching and proprioceptive neuromuscular facilitation on hamstring flexibility: Systematic review and meta-analysis. Eur. J. Physiother. 2018, 20, 12–19. [Google Scholar] [CrossRef]
- Lempke, L.; Wilkinson, R.; Murray, C.; Stanek, J. The Effectiveness of PNF Versus Static Stretching on Increasing Hip-Flexion Range of Motion. J. Sport Rehabil. 2018, 27, 289–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Medical Association. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull. World Health Organ. 2001, 79, 373–374. [Google Scholar]
- Jakobsen, T.L.; Christensen, M.; Christensen, S.S.; Olsen, M.; Bandholm, T. Reliability of knee joint range of motion and circumference measurements after total knee arthroplasty: Does tester experience matter? Physiother. Res. Int. 2010, 15, 126–134. [Google Scholar] [CrossRef]
- Shamsi, M.; Mirzaei, M.; Khabiri, S.S. Universal goniometer and electro-goniometer intra-examiner reliability in measuring the knee range of motion during active knee extension test in patients with chronic low back pain with short hamstring muscle. BMC Sports Sci. Med. Rehabil. 2019, 11, 4. [Google Scholar] [CrossRef]
- Epskamp, S.; Dibley, H.; Ray, E.; Bond, N.; White, J.; Wilkinson, A.; Chapple, C.M. Range of motion as an outcome measure for knee osteoarthritis interventions in clinical trials: An integrated review. Phys. Ther. Rev. 2020, 25, 462–481. [Google Scholar] [CrossRef]
- Jones, C.J.; Rikli, R.E.; Max, J.; Noffal, G. The Reliability and Validity of a Chair Sit-and-Reach Test as a Measure of Hamstring Flexibility in Older Adults. Res. Q. Exerc. Sport 1998, 69, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Konrad, A.; Stafilidis, S.; Tilp, M. Effects of acute static, ballistic, and PNF stretching exercise on the muscle and tendon tissue properties. Scand. J. Med. Sci. Sports 2017, 27, 1070–1080. [Google Scholar] [CrossRef] [PubMed]
- Puentedura, E.J.; Huijbregts, P.A.; Celeste, S.; Edwards, D.; In, A.; Landers, M.R.; Fernandez-de-las-Penas, C. Immediate effects of quantified hamstring stretching: Hold-relax proprioceptive neuromuscular facilitation versus static stretching. Phys. Ther. Sport 2011, 12, 122–126. [Google Scholar] [CrossRef]
- Funk, D.C.; Swank, A.M.; Mikla, B.M.; Fagan, T.A.; Farr, B.K. Impact of Prior Exercise on Hamstring Flexibility: A Comparison of Proprioceptive Neuromuscular Facilitation and Static Stretching. J. Strength Cond. Res. 2003, 17, 489. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.-I.; Nam, H.-C.; Jung, K.-S. Effects on Hamstring Muscle Extensibility, Muscle Activity, and Balance of Different Stretching Techniques. J. Phys. Ther. Sci. 2014, 26, 209–213. [Google Scholar] [CrossRef] [Green Version]
- Beltrão, N.; Ritti-Dias, R.; Pitangui, A.; De Araújo, R. Correlation between Acute and Short-Term Changes in Flexibility Using Two Stretching Techniques. Int. J. Sports Med. 2014, 35, 1151–1154. [Google Scholar] [CrossRef]
- Minshull, C.; Eston, R.; Bailey, A.; Rees, D.; Gleeson, N. The differential effects of PNF versus passive stretch conditioning on neuromuscular performance. Eur. J. Sport Sci. 2014, 14, 233–241. [Google Scholar] [CrossRef]
- Davis, D.S.; Ashby, P.E.; McCale, K.L.; McQuain, J.A.; Wine, J.M. The Effectiveness of 3 Stretching Techniques on Hamstring Flexibility Using Consistent Stretching Parameters. J. Strength Cond. Res. 2005, 19, 27. [Google Scholar] [CrossRef]
- Shadmehr, A.; Hadian, M.R.; Naiemi, S.S.; Jalaie, S. Hamstring flexibility in young women following passive stretch and muscle energy technique. BMR 2009, 22, 143–148. [Google Scholar] [CrossRef]
- Hill, K.J.; Robinson, K.P.; Cuchna, J.W.; Hoch, M.C. Immediate Effects of Proprioceptive Neuromuscular Facilitation Stretching Programs Compared with Passive Stretching Programs for Hamstring Flexibility: A Critically Appraised Topic. J. Sport Rehabil. 2017, 26, 567–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cayco, C.S.; Labro, A.V.; Gorgon, E.J.R. Hold-relax and contract-relax stretching for hamstrings flexibility: A systematic review with meta-analysis. Phys. Ther. Sport 2019, 35, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Gunn, L.J.; Stewart, J.C.; Morgan, B.; Metts, S.T.; Magnuson, J.M.; Iglowski, N.J.; Fritz, S.L.; Arnot, C. Instrument-assisted soft tissue mobilization and proprioceptive neuromuscular facilitation techniques improve hamstring flexibility better than static stretching alone: A randomized clinical trial. J. Man. Manip. Ther. 2019, 27, 15–23. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | PNF-CR Group (n = 10) | Static Stretching Group (n = 10) | Control Group (n = 10) | One-Way ANOVA |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | p-Value | |
| Age | 59.20 ± 3.15 | 59 ± 3.83 | 58.7 ± 3.02 | 0.94 |
| Weight | 67.10 ± 6.35 | 68.6 ± 3.53 | 68.5 ± 4.9 | 0.76 |
| Height | 1.64 ± 0.08 | 1.67 ± 0.46 | 1.67 ± 0.07 | 0.52 |
| BMI | 24.88 ± 2.37 | 24.37 ± 1.01 | 24.56 ± 2.03 | 0.82 |
| MVIC | 0.16 ± 0.56 | 0.16 ± 0.04 | 0.161 ± 0.05 | 0.96 |
| Knee ROM | 146.1 ± 4.57 | 146.73 ± 4.2 | 147.06 ± 4.72 | 0.88 |
| CART | 14.98 ± 1.94 | 14.66 ± 2.03 | 14.56 ± 1.72 | 0.87 |
| Variables | PNF-CR Group (n = 10) | Static Stretching Group (n = 10) | Control Group (n = 10) | Time (T) Effect | Group (G) Effect | G × T Interaction |
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | ηp2 (p-Value) | ηp2 (p-Value) | ηp2 (p-Value) | |
| MVIC | 0.87 (<0.001) * | 0.11 (0.209) | 0.81 (<0.001) * | |||
| Pre | 0.16 ± 0.05 | 0.16 ± 0.04 | 0.16 ± 0.05 | |||
| Post (Immediate) | 0.21 ± 0.06 | 0.17 ± 0.04 | 0.16 ± 0.06 | |||
| Post (4 weeks) | 0.24 ± 0.06 | 0.19 ± 0.03 | 0.17 ± 0.06 | |||
| ROM | 0.96 (<0.001) * | 0.53 (<0.001) * | 0.92 (<0.001) * | |||
| Pre | 144.1 ± 4.57 | 146.73 ± 4.2 | 147.06 ± 4.72 | |||
| Post (Immediate) | 156.7 ± 3 | 154.23 ± 4.19 | 148.16 ± 4.77 | |||
| Post (4 weeks) | 166.53 ± 3.31 | 168.60 ± 3.31 | 148.40 ± 4.71 | |||
| CART | 0.96 (<0.001) * | 0.51 (<0.001) * | 0.88 (<0.001) * | |||
| Pre | 14.98 ± 1.94 | 14.66 ± 2.03 | 14.56 ± 1.72 | |||
| Post (Immediate) | 10.96 ± 1.98 | 11.98 ± 2.16 | 13.93 ± 1.79 | |||
| Post (4 weeks) | 5.35 ± 1.18 | 4.10 ± 1.22 | 12.81 ± 1.83 |
| Variables | Pre vs. Post (Immediate) | Pre vs. Post (4 Weeks) |
|---|---|---|
| MVIC | <0.001 * | <0.001 * |
| ROM | <0.001 * | <0.001 * |
| CART | <0.001 * | <0.001 * |
| Variables | PNF-CR vs. Control | Static Stretch vs. Control | PNF-CR vs. Static Stretch |
|---|---|---|---|
| MVIC | |||
| Pre | - | - | - |
| Post (Immediate) | 0.209 | 1 | 0.711 |
| Post (4 weeks) | 0.014 * | 1 | 0.107 |
| ROM | |||
| Pre | - | - | - |
| Post (Immediate) | <0.001 * | 0.007 * | 0.557 |
| Post (4 weeks) | <0.001 * | <0.001 * | 0.718 |
| CART | |||
| Pre | - | - | - |
| Post (Immediate) | 0.007 * | 0.112 | 0.79 |
| Post (4 weeks) | <0.001 * | <0.001 * | 0.193 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaidi, S.; Ahamad, A.; Fatima, A.; Ahmad, I.; Malhotra, D.; Al Muslem, W.H.; Abdulaziz, S.; Nuhmani, S. Immediate and Long-Term Effectiveness of Proprioceptive Neuromuscular Facilitation and Static Stretching on Joint Range of Motion, Flexibility, and Electromyographic Activity of Knee Muscles in Older Adults. J. Clin. Med. 2023, 12, 2610. https://doi.org/10.3390/jcm12072610
Zaidi S, Ahamad A, Fatima A, Ahmad I, Malhotra D, Al Muslem WH, Abdulaziz S, Nuhmani S. Immediate and Long-Term Effectiveness of Proprioceptive Neuromuscular Facilitation and Static Stretching on Joint Range of Motion, Flexibility, and Electromyographic Activity of Knee Muscles in Older Adults. Journal of Clinical Medicine. 2023; 12(7):2610. https://doi.org/10.3390/jcm12072610
Chicago/Turabian StyleZaidi, Sahar, Asfak Ahamad, Anam Fatima, Irshad Ahmad, Deepak Malhotra, Wafa Hashem Al Muslem, Sahar Abdulaziz, and Shibili Nuhmani. 2023. "Immediate and Long-Term Effectiveness of Proprioceptive Neuromuscular Facilitation and Static Stretching on Joint Range of Motion, Flexibility, and Electromyographic Activity of Knee Muscles in Older Adults" Journal of Clinical Medicine 12, no. 7: 2610. https://doi.org/10.3390/jcm12072610
APA StyleZaidi, S., Ahamad, A., Fatima, A., Ahmad, I., Malhotra, D., Al Muslem, W. H., Abdulaziz, S., & Nuhmani, S. (2023). Immediate and Long-Term Effectiveness of Proprioceptive Neuromuscular Facilitation and Static Stretching on Joint Range of Motion, Flexibility, and Electromyographic Activity of Knee Muscles in Older Adults. Journal of Clinical Medicine, 12(7), 2610. https://doi.org/10.3390/jcm12072610