
Haematological Trends and Transfusion during Adult Extracorporeal Membrane Oxygenation: A Single Centre Study

Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Demographics
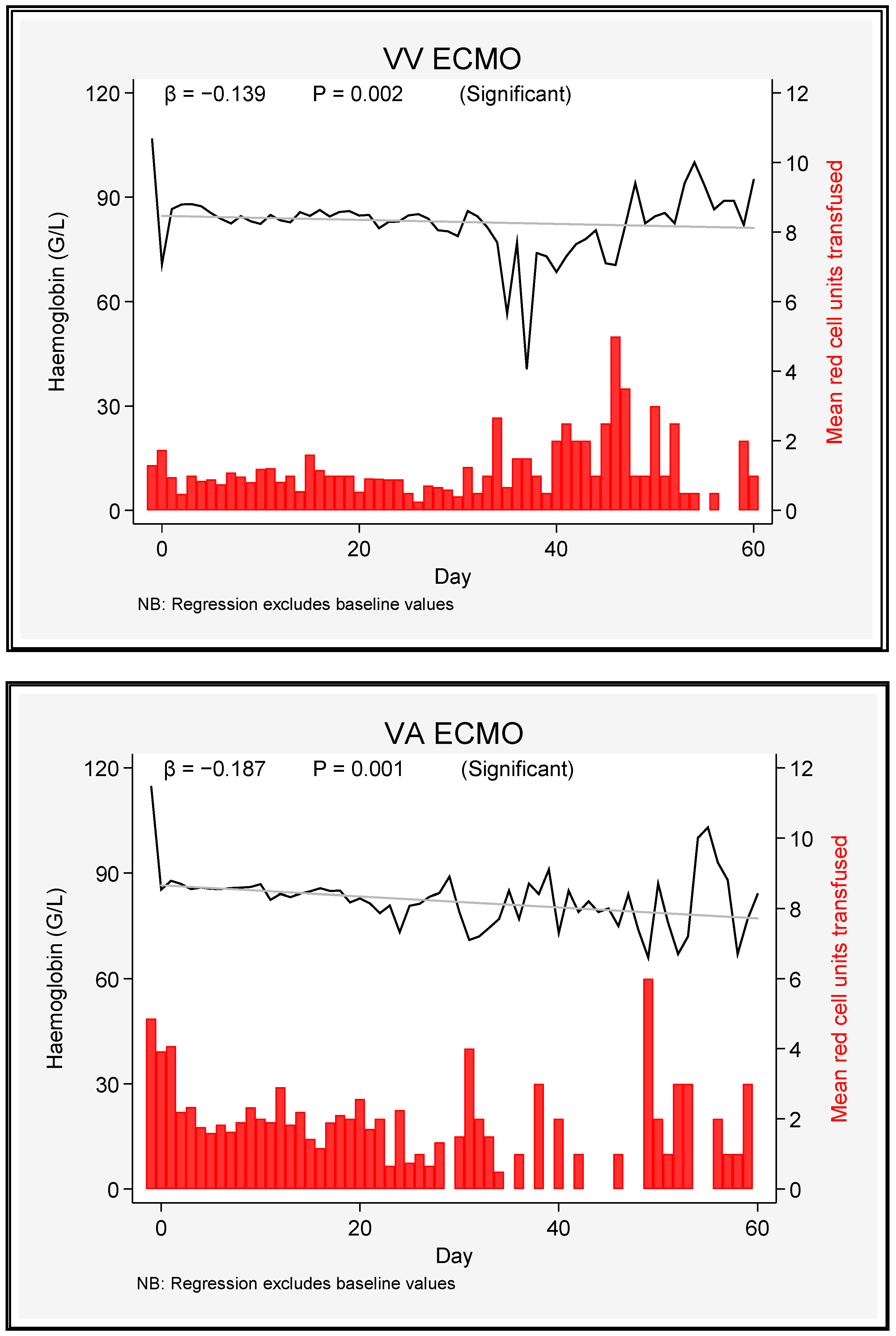
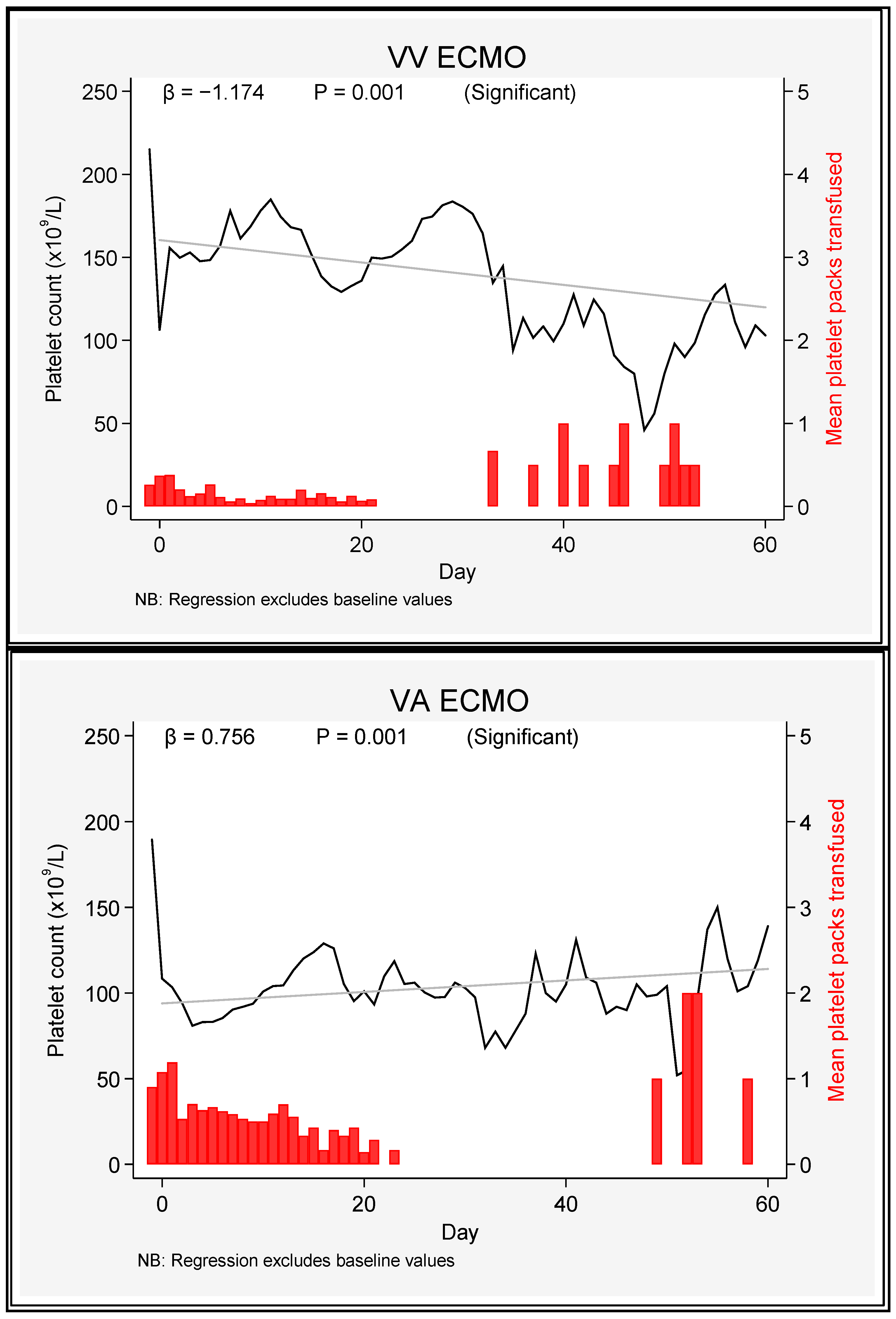
3.2. Haematological Parameters
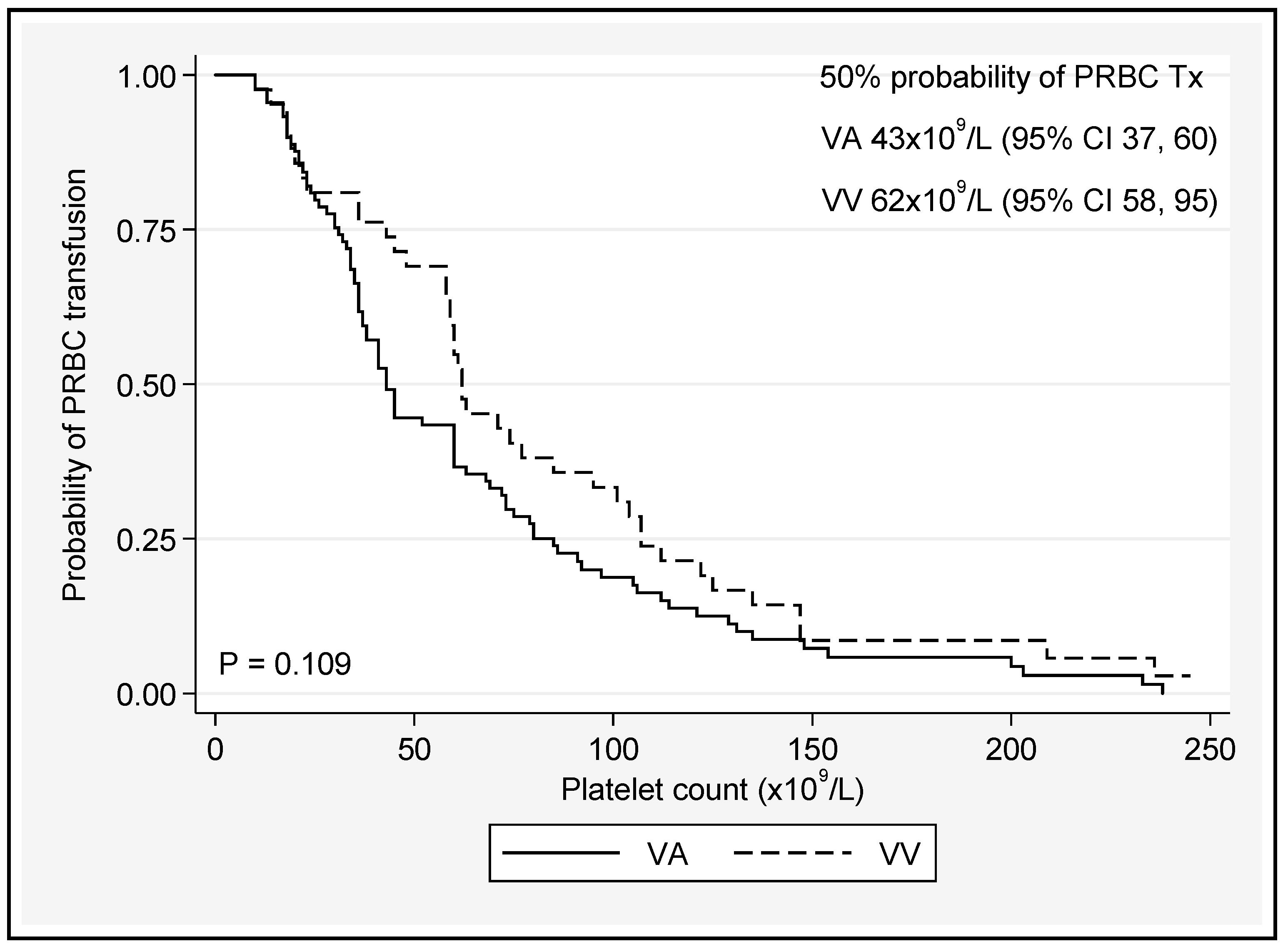
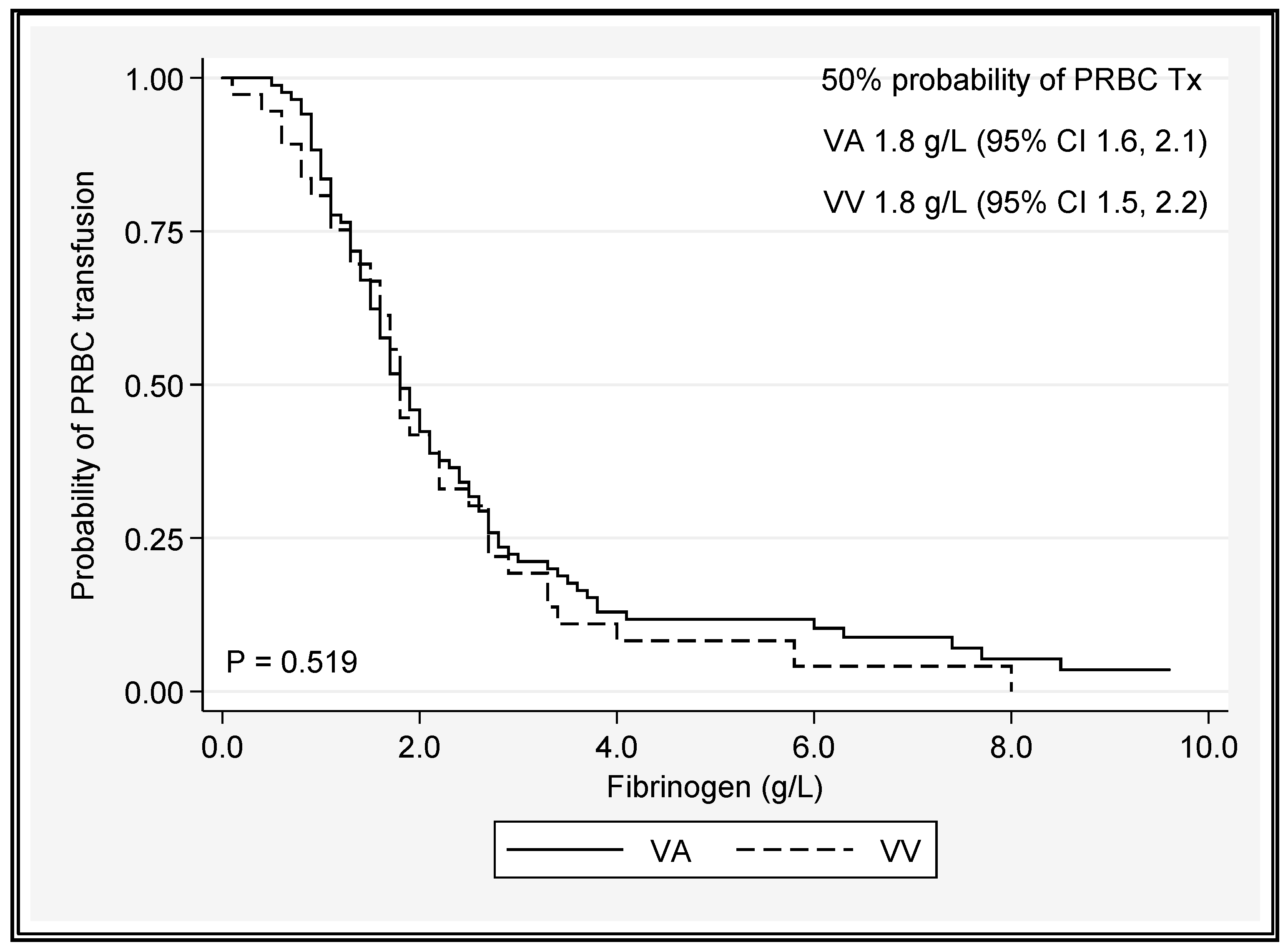
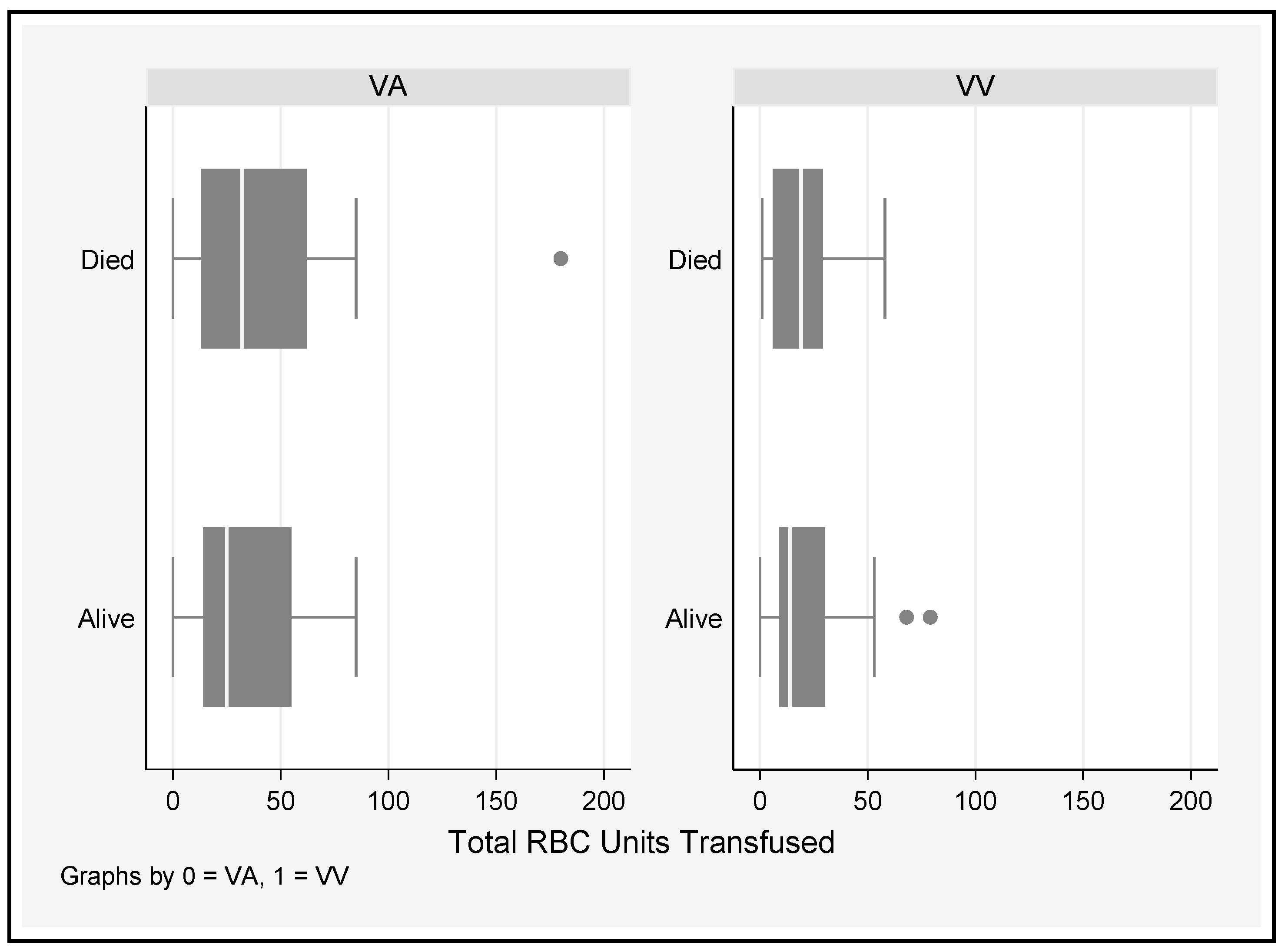
3.3. Transfusion Requirements
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bartlett, R.H.; Gattinoni, L. Current status of extracorporeal life support (ECMO) for cardiopulmonary failure. Minerva Anestesiol 2010, 76, 534–540. [Google Scholar] [PubMed]
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.; Holena, D.; McCunn, M.; Kohl, B.; Sarani, B. A review of the fundamental principles and evidence base in the use of extracorporeal membrane oxygenation (ECMO) in critically ill adult patients. J. Intensiv. Care Med. 2011, 26, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Ang, A.L.; Teo, D.; Lim, C.H.; Leou, K.K.; Tien, S.L.; Koh, M.B. Blood transfusion requirements and independent predictors of increased transfusion requirements among adult patients on extracorporeal membrane oxygenation—A single centre experience. Vox Sang. 2009, 96, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Hein, E.; Munthe-Fog, L.; Thiara, A.S.; Fiane, A.E.; Mollnes, T.E.; Garred, P. Heparin-coated cardiopulmonary bypass circuits selectively deplete the pattern recognition molecule ficolin-2 of the lectin complement pathway in vivo. Clin. Exp. Immunol. 2015, 179, 294–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ontaneda, A.; Annich, G.M. Novel Surfaces in Extracorporeal Membrane Oxygenation Circuits. Front. Med. 2018, 5, 321. [Google Scholar] [CrossRef] [PubMed]
- Lindholm, L.; Westerberg, M.; Bengtsson, A.; Ekroth, R.; Jensen, E.; Jeppsson, A. A closed perfusion system with heparin coating and centrifugal pump improves cardiopulmonary bypass biocompatibility in elderly patients. Ann. Thorac. Surg. 2004, 78, 2131–2138; discussion 8. [Google Scholar] [CrossRef]
- Morgan, I.S.; Codispoti, M.; Sanger, K.; Mankad, P.S. Superiority of centrifugal pump over roller pump in paediatric cardiac surgery: Prospective randomised trial. Eur. J. Cardiothorac. Surg. 1998, 13, 526–532. [Google Scholar] [CrossRef]
- Aubron, C.; Cheng, A.C.; Pilcher, D.; Leong, T.; Magrin, G.; Cooper, D.J.; Scheinkestel, C.; Pellegrino, V. Factors associated with outcomes of patients on extracorporeal membrane oxygenation support: A 5-year cohort study. Crit. Care 2013, 17, R73. [Google Scholar] [CrossRef] [Green Version]
- Thiagarajan, R.R.; Barbaro, R.P.; Rycus, P.T.; Mcmullan, D.M.; Conrad, S.A.; Fortenberry, J.D.; Paden, M.L. Extracorporeal Life Support Organization Registry International Report 2016. ASAIO J. 2017, 63, 60–67. [Google Scholar] [CrossRef]
- Malfertheiner, M.V.; Philipp, A.; Lubnow, M.; Zeman, F.; Enger, T.B.; Bein, T.; Lunz, D.; Schmid, C.; Müller, T.; Lehle, K. Hemostatic Changes During Extracorporeal Membrane Oxygenation: A Prospective Randomized Clinical Trial Comparing Three Different Extracorporeal Membrane Oxygenation Systems. Crit. Care Med. 2016, 44, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Murphy, D.A.; Hockings, L.E.; Andrews, R.K.; Aubron, C.; Gardiner, E.E.; Pellegrino, V.A.; Davis, A.K. Extracorporeal membrane oxygenation-hemostatic complications. Transfus. Med. Rev. 2015, 29, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Figueroa Villalba, C.A.; Brogan, T.V.; McMullan, D.M.; Yalon, L.; Jordan, D.I.; Chandler, W.L. Conversion From Activated Clotting Time to Anti-Xa Heparin Activity Assay for Heparin Monitoring During Extracorporeal Membrane Oxygenation. Crit. Care Med. 2020, 48, e1179–e1184. [Google Scholar] [CrossRef] [PubMed]
- Millar, J.E.; Fanning, J.P.; McDonald, C.I.; McAuley, D.F.; Fraser, J.F. The inflammatory response to extracorporeal membrane oxygenation (ECMO): A review of the pathophysiology. Crit. Care 2016, 20, 387. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Krawiec, C.; Patel, S.; Kunselman, A.R.; Song, J.; Lei, F.; Baer, L.D.; Ündar, A. Laboratory Evaluation of Hemolysis and Systemic Inflammatory Response in Neonatal Nonpulsatile and Pulsatile Extracorporeal Life Support Systems. Artif. Organs 2015, 39, 774–781. [Google Scholar] [CrossRef]
- Hirthler, M.; Simoni, J.; Dickson, M. Elevated levels of endotoxin, oxygen-derived free radicals, and cytokines during extracorporeal membrane oxygenation. J. Pediatr. Surg. 1992, 27, 1199–1202. [Google Scholar] [CrossRef]
- Hoffman, M.; Monroe, D.M., 3rd. A cell-based model of hemostasis. Thromb. Haemost. 2001, 85, 958–965. [Google Scholar]
- Nair, P.; Hoechter, D.J.; Buscher, H.; Venkatesh, K.; Whittam, S.; Joseph, J.; Jansz, P. Prospective observational study of hemostatic alterations during adult extracorporeal membrane oxygenation (ECMO) using point-of-care thromboelastometry and platelet aggregometry. J. Cardiothorac. Vasc. Anesth. 2015, 29, 288–296. [Google Scholar] [CrossRef] [Green Version]
- Passmore, M.R.; Ki, K.K.; Chan, C.H.; Lee, T.; Bouquet, M.; Wood, E.S.; Raman, S.; Rozencwajg, S.; Burrell, A.J.; McDonald, C.I.; et al. The effect of hyperoxia on inflammation and platelet responses in an ex vivo extracorporeal membrane oxygenation circuit. Artif. Organs 2020, 44, 1276–1285. [Google Scholar] [CrossRef]
- Orime, Y.; Shiono, M.; Hata, H.; Yagi, S.; Tsukamoto, S.; Okumura, H.; Nakata, K.I.; Kimura, S.I.; Hata, M.; Sezai, A.; et al. Cytokine and endothelial damage in pulsatile and nonpulsatile cardiopulmonary bypass. Artif. Organs 1999, 23, 508–512. [Google Scholar] [CrossRef]
- Koning, N.J.; Vonk, A.B.; Vink, H.; Boer, C. Side-by-Side Alterations in Glycocalyx Thickness and Perfused Microvascular Density During Acute Microcirculatory Alterations in Cardiac Surgery. Microcirculation 2016, 23, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, G.; Berg, N.; Broman, L.M.; Prahl Wittberg, L. Flow-induced platelet activation in components of the extracorporeal membrane oxygenation circuit. Sci. Rep. 2018, 8, 13985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross-Hardt, S.; Hesselmann, F.; Arens, J.; Steinseifer, U.; Vercaemst, L.; Windisch, W.; Brodie, D.; Karagiannidis, C. Low-flow assessment of current ECMO/ECCO2R rotary blood pumps and the potential effect on hemocompatibility. Crit. Care 2019, 23, 348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timothy, M.M.; Massicotte, M.P.; Peter, D.W. ECMO Biocompatibility: Surface Coatings, Anticoagulation, and Coagulation Monitoring. In Extracorporeal Membrane Oxygenation; Michael, S.F., Ed.; IntechOpen: Rijeka, Croatia, 2016; Chapter 3. [Google Scholar]
- Reynolds, M.M.; Annich, G.M. The artificial endothelium. Organogenesis 2011, 7, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Heilmann, C.; Trummer, G.; Beyersdorf, F.; Brehm, K.; Berchtold-Herz, M.; Schelling, J.; Geisen, U.; Zieger, B. Acquired Von Willebrand syndrome in patients on long-term support with HeartMate II. Eur. J. Cardiothorac. Surg. 2017, 51, 587–590. [Google Scholar] [CrossRef]
- Heilmann, C.; Geisen, U.; Beyersdorf, F.; Nakamura, L.; Benk, C.; Trummer, G.; Berchtold-Herz, M.; Schlensak, C.; Zieger, B. Acquired von Willebrand syndrome in patients with extracorporeal life support (ECLS). Intensive Care Med. 2012, 38, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Vamvakas, E.C.; Blajchman, M.A. Transfusion-related immunomodulation (TRIM): An update. Blood Rev. 2007, 21, 327–348. [Google Scholar] [CrossRef]
- Cuschieri, J.; Freeman, B.; O’Keefe, G.; Harbrecht, B.G.; Bankey, P.; Johnson, J.L.; Minei, J.P.; Sperry, J.; West, M.A.; Nathens, A.; et al. Inflammation and the host response to injury a large-scale collaborative project: Patient-oriented research core standard operating procedure for clinical care X. Guidelines for venous thromboembolism prophylaxis in the trauma patient. J. Trauma 2008, 65, 944–950. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.; Hardison, D.; Bridges, B.; Pietsch, J. Red blood cell transfusion volume and mortality among patients receiving extracorporeal membrane oxygenation. Perfusion 2013, 28, 54–60. [Google Scholar] [CrossRef]
- Martucci, G.; Panarello, G.; Occhipinti, G.; Ferrazza, V.; Tuzzolino, F.; Bellavia, D.; Sanfilippo, F.; Santonocito, C.; Bertani, A.; Vitulo, P.; et al. Anticoagulation and Transfusions Management in Veno-Venous Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome: Assessment of Factors Associated With Transfusion Requirements and Mortality. J. Intensiv. Care Med. 2019, 34, 630–639. [Google Scholar] [CrossRef]
- Hodgson, C.L.F.B.; Salimi, F.; Anderson, S.; Bernard, S.; Board, J.V.; Brodie, D.; Buhr, H.; Burrell, A.J.C.; Cooper, D.J.; Fan, E.; et al. The EXCEL Registry Report 2019–2021; Monash University, Australian and New Zealand Intensive Care Research Centre: Melbourne, Australia, 2022. [Google Scholar]
- ELSO. ECLS Registry Report-International Summary October 2022 [Online Registry]. 2022. Available online: https://www.elso.org/portals/0/files/reports/2022_october/international%20report%20october.pdf (accessed on 1 October 2022).
- Elsharkawy, H.A.; Li, L.; Esa, W.A.; Sessler, D.I.; Bashour, C.A. Outcome in patients who require venoarterial extracorporeal membrane oxygenation support after cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2010, 24, 946–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rastan, A.J.; Dege, A.; Mohr, M.; Doll, N.; Falk, V.; Walther, T.; Mohr, F.W. Early and late outcomes of 517 consecutive adult patients treated with extracorporeal membrane oxygenation for refractory postcardiotomy cardiogenic shock. J. Thorac. Cardiovasc. Surg. 2010, 139, 302–311.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loungani, R.S.; Fudim, M.; Ranney, D.; Kochar, A.; Samsky, M.D.; Bonadonna, D.; Itoh, A.; Takayama, H.; Takeda, K.; Wojdyla, D.; et al. Contemporary Use of Venoarterial Extracorporeal Membrane Oxygenation: Insights from the Multicenter RESCUE Registry. J. Card. Fail. 2021, 27, 327–337. [Google Scholar] [CrossRef]
- Hughes, T.; Zhang, D.; Nair, P.; Buscher, H. A Systematic Literature Review of Packed Red Cell Transfusion Usage in Adult Extracorporeal Membrane Oxygenation. Membranes 2021, 11, 251. [Google Scholar] [CrossRef]
- Lotz, C.; Streiber, N.; Roewer, N.; Lepper, P.M.; Muellenbach, R.M.; Kredel, M. Therapeutic Interventions and Risk Factors of Bleeding During Extracorporeal Membrane Oxygenation. ASAIO J. 2017, 63, 624–630. [Google Scholar] [CrossRef]
- Mazzeffi, M.; Greenwood, J.; Tanaka, K.; Menaker, J.; Rector, R.; Herr, D.; Kon, Z.; Lee, J.; Griffith, B.; Rajagopal, K.; et al. Bleeding, Transfusion, and Mortality on Extracorporeal Life Support: ECLS Working Group on Thrombosis and Hemostasis. Ann. Thorac. Surg. 2016, 101, 682–689. [Google Scholar] [CrossRef] [Green Version]
- Agerstrand, C.L.; Burkart, K.M.; Abrams, D.C.; Bacchetta, M.D.; Brodie, D. Blood conservation in extracorporeal membrane oxygenation for acute respiratory distress syndrome. Ann. Thorac. Surg. 2015, 99, 590–595. [Google Scholar] [CrossRef]
- Ferraris, V.A.; Davenport, D.L.; Saha, S.P.; Bernard, A.; Austin, P.C.; Zwischenberger, J.B. Intraoperative transfusion of small amounts of blood heralds worse postoperative outcome in patients having noncardiac thoracic operations. Ann. Thorac. Surg. 2011, 91, 1674–1680; discussion 80. [Google Scholar] [CrossRef] [PubMed]
- ELSO. Extracorporeal Life Support Organization Guidelines for Adult Respiratory Failure. 2017. Available online: https://www.elso.org/Portals/0/ELSO%20Guidelines%20For%20Adult%20Respiratory%20Failure%201_4.pdf (accessed on 26 November 2020).
- Sawyer, A.A.; Wise, L.; Ghosh, S.; Bhatia, J.; Stansfield, B.K. Comparison of transfusion thresholds during neonatal extracorporeal membrane oxygenation. Transfusion 2017, 57, 2115–2120. [Google Scholar] [CrossRef]
- Singh, G.; Nahirniak, S.; Arora, R.; Légaré, J.F.; Kanji, H.D.; Nagpal, D.; Lamarche, Y.; Fan, E.; Parhar, K.K.S. Transfusion Thresholds for Adult Respiratory Extracorporeal Life Support: An Expert Consensus Document. Can. J. Cardiol. 2020, 36, 1550–1553. [Google Scholar] [CrossRef]
- Martucci, G.; Grasselli, G.; Tanaka, K.; Tuzzolino, F.; Panarello, G.; Schmidt, M.; Bellani, G.; Arcadipane, A. Hemoglobin trigger and approach to red blood cell transfusions during veno-venous extracorporeal membrane oxygenation: The international TRAIN-ECMO survey. Perfusion 2019, 34 (Suppl. S1), 39–48. [Google Scholar] [CrossRef] [PubMed]
- Ducrocq, G.; Gonzalez-Juanatey, J.R.; Puymirat, E.; Lemesle, G.; Cachanado, M.; Durand-Zaleski, I.; Arnaiz, J.A.; Martínez-Sellés, M.; Silvain, J.; Ariza-Solé, A.; et al. Effect of a Restrictive vs Liberal Blood Transfusion Strategy on Major Cardiovascular Events Among Patients With Acute Myocardial Infarction and Anemia: The REALITY Randomized Clinical Trial. JAMA 2021, 325, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Carson, J.L.; Stanworth, S.J.; Dennis, J.A.; Trivella, M.; Roubinian, N.; Fergusson, D.A.; Triulzi, D.; Dorée, C.; Hébert, P.C. Transfusion thresholds for guiding red blood cell transfusion. Cochrane Database Syst. Rev. 2021, 12, CD002042. [Google Scholar] [CrossRef] [PubMed]
- Holst, L.B.; Haase, N.; Wetterslev, J.; Wernerman, J.; Guttormsen, A.B.; Karlsson, S.; Johansson, P.I.; Åneman, A.; Vang, M.L.; Winding, R.; et al. Lower versus higher hemoglobin threshold for transfusion in septic shock. N. Engl. J. Med. 2014, 371, 1381–1391. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Park, S. Blood Transfusion Strategies in Patients Undergoing Extracorporeal Membrane Oxygenation. Korean J. Crit. Care Med. 2017, 32, 22–28. [Google Scholar] [CrossRef]
- Hébert, P.C.; Wells, G.; Blajchman, M.A.; Marshall, J.; Martin, C.; Pagliarello, G.; Tweeddale, M.; Schweitzer, I.; Yetisir, E.; Transfusion Requirements in Critical Care Investigators for the Canadian Critical Care Trials Group. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N. Engl. J. Med. 1999, 340, 409–417. [Google Scholar] [CrossRef]
- Fiser, R.T.; Irby, K.; Ward, R.M.; Tang, X.; McKamie, W.; Prodhan, P.; Corwin, H.L. RBC Transfusion in Pediatric Patients Supported with Extracorporeal Membrane Oxygenation: Is There an Impact on Tissue Oxygenation? Pediatr. Crit. Care Med. 2014, 15, 806–813. [Google Scholar] [CrossRef]
- Abbasciano, R.G.; Yusuff, H.; Vlaar, A.P.J.; Lai, F.; Murphy, G.J. Blood Transfusion Threshold in Patients Receiving Extracorporeal Membrane Oxygenation Support for Cardiac and Respiratory Failure-A Systematic Review and Meta-Analysis. J. Cardiothorac. Vasc. Anesth. 2021, 35, 1192–1202. [Google Scholar] [CrossRef]
- Ramanathan, K.; MacLaren, G.; Combes, A.; Brodie, D.; Shekar, K. Blood transfusion strategies and ECMO during the COVID-19 pandemic-Authors’ reply. Lancet Respir. Med. 2020, 8, e41. [Google Scholar] [CrossRef]
- Bembea, M.M.; Annich, G.; Rycus, P.; Oldenburg, G.; Berkowitz, I.; Pronovost, P. Variability in anticoagulation management of patients on extracorporeal membrane oxygenation: An international survey. Pediatr. Crit. Care Med. 2013, 14, e77–e84. [Google Scholar] [CrossRef]
- Doyle, A.J.; Richardson, C.; Sanderson, B.; Wong, K.; Wyncoll, D.; Camporota, L.; Barrett, N.A.; Hunt, B.J.; Retter, A. Restrictive Transfusion Practice in Adults Receiving Venovenous Extracorporeal Membrane Oxygenation: A Single-Center Experience. Crit. Care Explor. 2020, 2, e0077. [Google Scholar] [CrossRef] [PubMed]
- Martucci, G.; Schmidt, M.; Agerstrand, C.; Tabatabai, A.; Tuzzolino, F.; Giani, M.; Ramanan, R.; Grasselli, G.; Schellongowski, P.; Riera, J.; et al. Transfusion practice in patients receiving VV ECMO (PROTECMO): A prospective, multicentre, observational study. Lancet Respir. Med. 2022, 11, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Swol, J.; Marschall, C.; Strauch, J.T.; Schildhauer, T.A. Hematocrit and impact of transfusion in patients receiving extracorporeal life support. Perfusion 2018, 33, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Cahill, C.M.; Blumberg, N.; Schmidt, A.E.; Knight, P.A.; Melvin, A.L.; Massey, H.T.; Delehanty, J.M.; Zebrak, S.B.; Refaai, M.A. Implementation of a Standardized Transfusion Protocol for Cardiac Patients Treated With Venoarterial Extracorporeal Membrane Oxygenation Is Associated With Decreased Blood Component Utilization and May Improve Clinical Outcome. Anesth. Analg. 2018, 126, 1262–1267. [Google Scholar] [CrossRef] [PubMed]
- Tolksdorf, B.; Schmeck, J.; Osika, A.; Bender, H.J.; Quintel, M. Autotransfusion during extracorporeal membrane oxygenation. Int. J. Artif. Organs 2000, 23, 840–844. [Google Scholar] [CrossRef]
- Mueller, M.M.; Van Remoortel, H.; Meybohm, P.; Aranko, K.; Aubron, C.; Burger, R.; Carson, J.L.; Cichutek, K.; De Buck, E.; Devine, D.; et al. Patient Blood Management: Recommendations From the 2018 Frankfurt Consensus Conference. JAMA 2019, 321, 983–997. [Google Scholar] [CrossRef]
- Danial, P.; Hajage, D.; Nguyen, L.S.; Mastroianni, C.; Demondion, P.; Schmidt, M.; Bouglé, A.; Amour, J.; Leprince, P.; Combes, A.; et al. Percutaneous versus surgical femoro-femoral veno-arterial ECMO: A propensity score matched study. Intensiv. Care Med. 2018, 44, 2153–2161. [Google Scholar] [CrossRef]
- Maggio, P.; Hemmila, M.; Haft, J.; Bartlett, R. Extracorporeal life support for massive pulmonary embolism. J. Trauma 2007, 62, 570–576. [Google Scholar] [CrossRef]
- Subramaniam, A.V.; Barsness, G.W.; Vallabhajosyula, S.; Vallabhajosyula, S. Complications of Temporary Percutaneous Mechanical Circulatory Support for Cardiogenic Shock: An Appraisal of Contemporary Literature. Cardiol. Ther. 2019, 8, 211–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostermann, M.; Lumlertgul, N. Acute kidney injury in ECMO patients. Crit. Care 2021, 25, 313. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Lertjitbanjong, P.; Aeddula, N.R.; Bathini, T.; Watthanasuntorn, K.; Srivali, N.; Mao, M.A.; Kashani, K. Incidence and Impact of Acute Kidney Injury in Patients Receiving Extracorporeal Membrane Oxygenation: A Meta-Analysis. J. Clin. Med. 2019, 8, 981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostermann, M.; Connor, M., Jr.; Kashani, K. Continuous renal replacement therapy during extracorporeal membrane oxygenation: Why, when and how? Curr. Opin. Crit. Care 2018, 24, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Grandin, E.W.; Nunez, J.I.; Willar, B.; Kennedy, K.; Rycus, P.; Tonna, J.E.; Kapur, N.K.; Shaefi, S.; Garan, A.R. Mechanical Left Ventricular Unloading in Patients Undergoing Venoarterial Extracorporeal Membrane Oxygenation. J. Am. Coll. Cardiol. 2022, 79, 1239–1250. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, R.; Meani, P.; Raffa, G.M.; Kowalewski, M. Extracorporeal membrane oxygenation and left ventricular unloading: What is the evidence? JTCVS Tech. 2022, 13, 101–114. [Google Scholar] [CrossRef] [PubMed]
- Kaseer, H.; Soto-Arenall, M.; Sanghavi, D.; Moss, J.; Ratzlaff, R.; Pham, S.; Guru, P. Heparin vs bivalirudin anticoagulation for extracorporeal membrane oxygenation. J. Card. Surg. 2020, 35, 779–786. [Google Scholar] [CrossRef]
- Lind, S.E.; Boyle, M.E.; Fisher, S.; Ishimoto, J.; Trujillo, T.C.; Kiser, T.H. Comparison of the aPTT with alternative tests for monitoring direct thrombin inhibitors in patient samples. Am. J. Clin. Pathol. 2014, 141, 665–674. [Google Scholar] [CrossRef] [Green Version]
- Mazzeffi, M.A.; Tanaka, K.; Roberts, A.; Rector, R.; Menaker, J.; Kon, Z.; Deatrick, K.B.; Kaczorowski, D.; Griffith, B.; Herr, D. Bleeding, Thrombosis, and Transfusion With Two Heparin Anticoagulation Protocols in Venoarterial ECMO Patients. J. Cardiothorac. Vasc. Anesth. 2019, 33, 1216–1220. [Google Scholar] [CrossRef]
- Rhoades, R.; Leong, R.; Kopenitz, J.; Thoma, B.; McDermott, L.; Dovidio, J.; Barletti, S.; Gong, J.Z.; Massey, H.T.; McKenzie, S.E.; et al. Coagulopathy monitoring and anticoagulation management in COVID-19 patients on ECMO: Advantages of a heparin anti-Xa-based titration strategy. Thromb. Res. 2021, 203, 1–4. [Google Scholar] [CrossRef]
- Irby, K.; Swearingen, C.; Byrnes, J.; Bryant, J.; Prodhan, P.; Fiser, R. Unfractionated heparin activity measured by anti-factor Xa levels is associated with the need for extracorporeal membrane oxygenation circuit/membrane oxygenator change: A retrospective pediatric study. Pediatr. Crit. Care Med. 2014, 15, e175–e182. [Google Scholar] [CrossRef] [Green Version]
- Chlebowski, M.M.; Baltagi, S.; Carlson, M.; Levy, J.H.; Spinella, P.C. Clinical controversies in anticoagulation monitoring and antithrombin supplementation for ECMO. Crit. Care 2020, 24, 19. [Google Scholar] [CrossRef] [Green Version]
- Niimi, K.S.; Fanning, J.J. Initial experience with recombinant antithrombin to treat antithrombin deficiency in patients on extracorporeal membrane oxygenation. J. Extra Corpor. Technol. 2014, 46, 84–90. [Google Scholar] [PubMed]
- Byrnes, J.W.; Swearingen, C.J.; Prodhan, P.; Fiser, R.; Dyamenahalli, U. Antithrombin III supplementation on extracorporeal membrane oxygenation: Impact on heparin dose and circuit life. ASAIO J. 2014, 60, 57–62. [Google Scholar] [CrossRef]
- Gorbet, M.B.; Sefton, M.V. Biomaterial-associated thrombosis: Roles of coagulation factors, complement, platelets and leukocytes. Biomaterials 2004, 25, 5681–5703. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, B.; Bruce, H.M.; Kershaw, G.; Cai, N.; Othman, J.; Gattas, D.; Robson, J.L.; Hayes, S.; Alicajic, H.; Hines, A.; et al. Hemostasis, coagulation and thrombin in venoarterial and venovenous extracorporeal membrane oxygenation: The HECTIC study. Sci. Rep. 2021, 11, 7975. [Google Scholar] [CrossRef] [PubMed]
- Loscalzo, J. From clinical observation to mechanism--Heyde’s syndrome. N. Engl. J. Med. 2012, 367, 1954–1956. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y. Contact pathway of coagulation and inflammation. Thromb. J. 2015, 13, 17. [Google Scholar] [CrossRef] [Green Version]
- Schneider, S.W.; Nuschele, S.; Wixforth, A.; Gorzelanny, C.; Alexander-Katz, A.; Netz, R.R.; Schneider, M.F. Shear-induced unfolding triggers adhesion of von Willebrand factor fibers. Proc. Natl. Acad. Sci. USA 2007, 104, 7899–7903. [Google Scholar] [CrossRef] [Green Version]
- Heilmann, C.; Geisen, U.; Beyersdorf, F.; Nakamura, L.; Benk, C.; Berchtold-Herz, M.; Trummer, G.; Schlensak, C.; Zieger, B. Acquired von Willebrand syndrome in patients with ventricular assist device or total artificial heart. Thromb. Haemost. 2010, 103, 962–967. [Google Scholar] [CrossRef]
- Ki, K.K.; Passmore, M.R.; Chan, C.H.; Malfertheiner, M.V.; Fanning, J.P.; Bouquet, M.; Millar, J.E.; Fraser, J.F.; Suen, J.Y. Low flow rate alters haemostatic parameters in an ex-vivo extracorporeal membrane oxygenation circuit. Intensiv. Care Med. Exp. 2019, 7, 51. [Google Scholar] [CrossRef]
- Wu, J.; Paden, B.E.; Borovetz, H.S.; Antaki, J.F. Computational fluid dynamics analysis of blade tip clearances on hemodynamic performance and blood damage in a centrifugal ventricular assist device. Artif. Organs 2010, 34, 402–411. [Google Scholar] [CrossRef] [Green Version]
- The Australia and New Zealand Extracorporeal Membrane Oxygenation (ANZ ECMO) Influenza Investigators. Extracorporeal Membrane Oxygenation for 2009 Influenza A(H1N1) Acute Respiratory Distress Syndrome. JAMA 2009, 302, 1888–1895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aubron, C.; McQuilten, Z.; Bailey, M.; Board, J.; Buhr, H.; Cartwright, B.; Dennis, M.; Hodgson, C.; Forrest, P.; McIlroy, D.; et al. Low-Dose Versus Therapeutic Anticoagulation in Patients on Extracorporeal Membrane Oxygenation: A Pilot Randomized Trial. Crit. Care Med. 2019, 47, e563–e571. [Google Scholar] [CrossRef] [PubMed]
- Alkazemi, A.; Eche, I.M.; Adra, M.; Cabezas, F.; Patel, P.; Rick, K.; Grandin, E.W. Conventional versus restricted anti-Xa-guided heparin protocol in adult patients undergoing extracorporeal membrane oxygenation. Artif. Organs 2022, 46, 128–137. [Google Scholar] [CrossRef]
- Muellenbach, R.M.; Kredel, M.; Kunze, E.; Kranke, P.; Kuestermann, J.; Brack, A.; Gorski, A.; Wunder, C.; Roewer, N.; Wurmb, T. Prolonged heparin-free extracorporeal membrane oxygenation in multiple injured acute respiratory distress syndrome patients with traumatic brain injury. J. Trauma Acute Care Surg. 2012, 72, 1444–1447. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | VA ECMO (N = 92) | VV ECMO (N = 46) | p-Value |
|---|---|---|---|
| Age | 47.2 (16.5) | 38.7 (14.7) | p = 0.0037 |
| Male sex (%) | 65 (70.7%) | 24 (52.2%) | p = 0.03 |
| Weight (kg) | 81.9 (21.5) | 78.1 (17.5) | p = 0.31 |
| APACHE II | 23 [17, 29] | 22 [18, 27] | p = 0.88 |
| APACHE III | 80 [58, 114] | 76 [61, 93] | p = 0.44 |
| ICU LOS (hours) | 427 [143, 661] | 673 [319, 983] | p = 0.006 |
| Hospital LOS (hours) Mortality (%) | 664 [199, 1162] 45 (48.9%) | 940 [532, 1167] 8 (17.4%) | p = 0.10 p < 0.001 |
| Indication | VA ECMO (N = 92) | VV ECMO (N = 46) | p-Value |
|---|---|---|---|
| Pulmonary–ARDS | 2 (2.2%) | 28 (60.9%) | |
| Pulmonary–Other | 9 (9.8%) | 10 (21.7%) | |
| Pulmonary–Total | 11 (11.9%) | 38 (82.6%) | p < 0.001 |
| Cardiomyopathy–MI | 4 (4.3%) | 0 (0.0%) | |
| Cardiomyopathy–Other | 49 (53.3%) | 0 (0.0%) | |
| Cardiomyopathy–Postop | 23 (25.0%) | 1 (2.2%) | |
| Cardiomyopathy–Total | 76 (82.6%) | 1 (2.2%) | p < 0.001 |
| Sepsis | 5 (5.4%) | 7 (15.2%) | p = 0.594 |
| VA ECMO | Pre-ECMO | Day 1 | p-Value |
|---|---|---|---|
| Haemoglobin (g/L) | 114 (26) | 85 (24) | p < 0.001 |
| Platelet count (×109/L) | 190 (99) | 108 (61) | p < 0.001 |
| Fibrinogen (g/L) | 3.96 (2.12) | 2.71 (1.83) | p < 0.001 |
| VV ECMO | |||
| Haemoglobin (g/L) | 107 (26) | 71 (34) | p < 0.001 |
| Platelet count (×109/L) | 215 (138) | 106 (124) | p < 0.001 |
| Fibrinogen (g/L) | 5.41 (2.61) | 2.98 (1.92) | p < 0.001 |
| Variable | Median [IQR] | β (95% CI) | p-Value |
|---|---|---|---|
| VV ECMO Survivor | |||
| INR | 1.1 [1.1, 1.2] | −0.015 (−0.027, −0.003) | 0.015 |
| APTT | 49 [39, 63] | −1.180 (−1.553, −0.806) | <0.001 |
| VA ECMO Survivor | |||
| INR | 1.2 [1.1, 1.5] | −0.051 (−0.081, −0.022) | 0.001 |
| APTT | 49 [38, 68] | −1.752 (−2.516, −0.987) | <0.001 |
| VV ECMO Nonsurvivor | |||
| INR | 1.1 [1.0, 1.2] | 0.000 (−0.014, +0.014) | 0.969 |
| APTT | 44 [36, 62] | −0.229 (−1.010, +0.552) | 0.566 |
| VA ECMO Nonsurvivor | |||
| INR | 1.3 [1.2, 1.7] | −0.051 (−0.081, −0.022) | 0.001 |
| APTT | 50 [41, 74] | −2.51 (−3.43, −1.59) | <0.001 |
| Product Units | VA ECMO | VV ECMO |
|---|---|---|
| PRBC | 2455 (3.8/ECMO day) | 807 (1.0/ECMO day) |
| Platelets | 636 (0.9/ECMO day) | 125 (0.2/ECMO day) |
| Cryoprecipitate | 1189 (1.8/ECMO day) | 464 (0.6/ECMO day) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Worku, E.T.; Win, A.M.; Parmar, D.; Anstey, C.; Shekar, K. Haematological Trends and Transfusion during Adult Extracorporeal Membrane Oxygenation: A Single Centre Study. J. Clin. Med. 2023, 12, 2629. https://doi.org/10.3390/jcm12072629
Worku ET, Win AM, Parmar D, Anstey C, Shekar K. Haematological Trends and Transfusion during Adult Extracorporeal Membrane Oxygenation: A Single Centre Study. Journal of Clinical Medicine. 2023; 12(7):2629. https://doi.org/10.3390/jcm12072629
Chicago/Turabian StyleWorku, Elliott T., April M. Win, Dinesh Parmar, Chris Anstey, and Kiran Shekar. 2023. "Haematological Trends and Transfusion during Adult Extracorporeal Membrane Oxygenation: A Single Centre Study" Journal of Clinical Medicine 12, no. 7: 2629. https://doi.org/10.3390/jcm12072629
APA StyleWorku, E. T., Win, A. M., Parmar, D., Anstey, C., & Shekar, K. (2023). Haematological Trends and Transfusion during Adult Extracorporeal Membrane Oxygenation: A Single Centre Study. Journal of Clinical Medicine, 12(7), 2629. https://doi.org/10.3390/jcm12072629