
The Relationship between Cancer Stage, Selected Immunological Parameters, Epstein–Barr Virus Infection, and Total Serum Content of Iron, Zinc, and Copper in Patients with Laryngeal Cancer
 , , , ,
, , , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
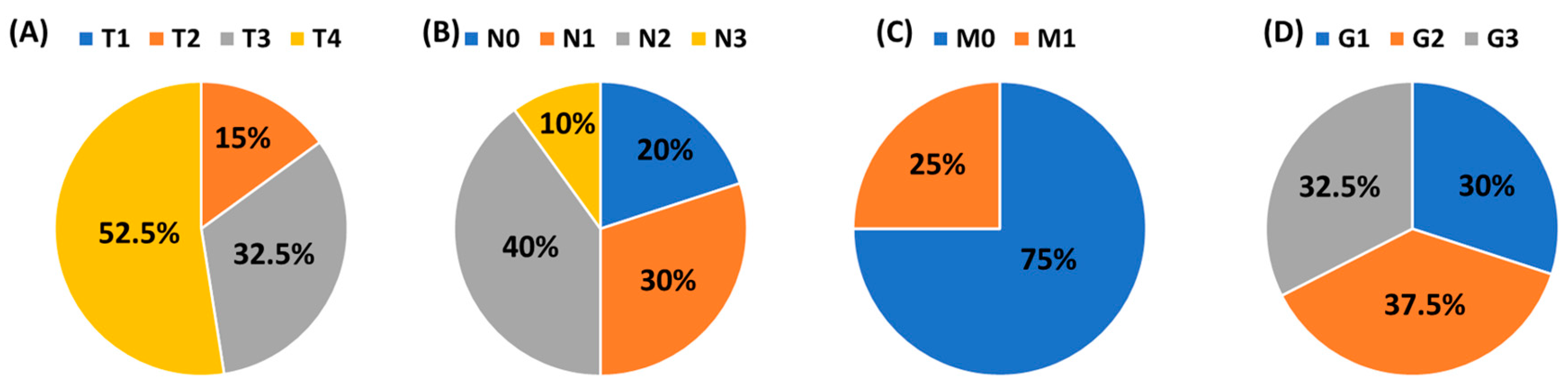
2.1. Patient Characteristics
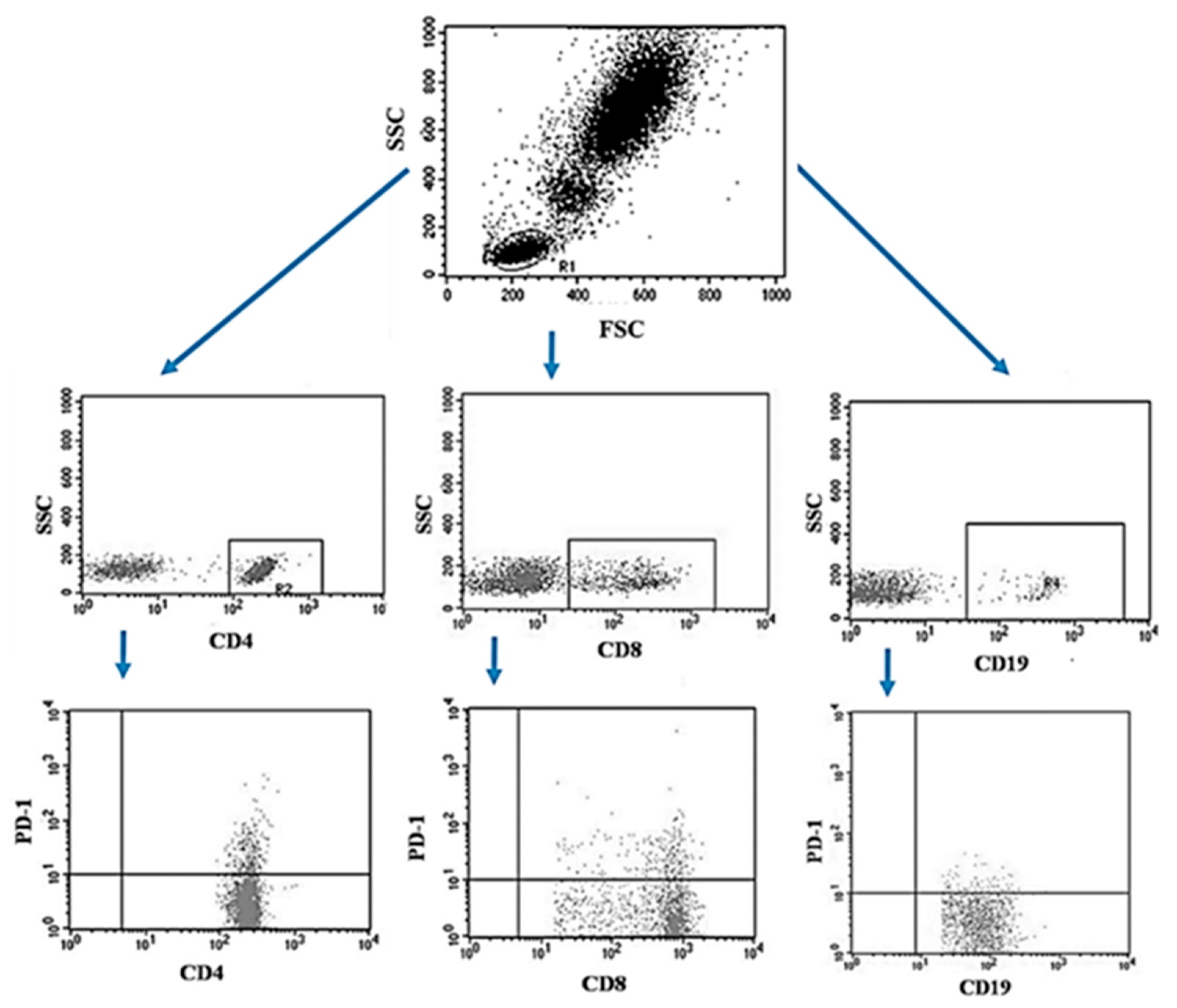
2.2. Flow Cytometric Analysis of Cells in Peripheral Blood
2.3. Flow Cytometric of Cells in Tumor Tissue and Lymph Nodes
2.4. Analysis of the Total (Organic and Inorganic) Content of Fe Zn, Cu, and Cu/Zn in Serum
2.5. Assessment of the Presence of Specific Antibodies EBV IgM VCA, EBV IgG VCA
2.6. Assessment of the Amount of Viral DNA in the Studied Patients
2.7. Statistical Analysis
3. Results
3.1. Characteristics of Selected Parameters of Peripheral Blood Count, Serum Iron, Zinc and Copper Concentration and Immunophenotype in Patients with Laryngeal Cancer and in the Control Group
3.2. Assessment of the Concentration of Selected Elements in Relation to the Grade (G) and TNM Scale
3.3. Effect of EBV Reactivation on Laryngeal Cancer Development
3.4. The Importance of Serum Iron, Zinc and Copper Concentration in the Context of Survival in Patients with Laryngeal Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znar, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020; Available online: https://gco.iarc.fr/today (accessed on 1 May 2022).
- Steuer, C.E.; El-Deiry, M.; Parks, J.R.; Higgins, K.A.; Saba, N.F. An update on larynx cancer. CA Cancer J. Clin. 2017, 67, 31–50. [Google Scholar] [CrossRef] [PubMed]
- Wierzbicka, M.; Winiarski, P.; Osuch-Wójcikiewicz, E. The incidence of laryngeal cancer in Europe with special regard to Poland in last 2 decades. Otolaryngol. Pol. 2016, 70, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Xia, P.; Zheng, H.C.; Takahashi, H.; Masuda, S.; Takano, Y. The screening of viral risk factors in tongue and pharyngolaryngeal squamous carcinoma. Anticancer Res. 2010, 30, 1233–1238. [Google Scholar] [PubMed]
- Klatka, J.; Szkatuła-Łupina, A.; Hymos, A.; Klatka, M.; Mertowska, P.; Mertowski, S.; Grywalska, E.; Charytanowicz, M.; Błażewicz, A.; Poniewierska-Baran, A.; et al. The Clinical, Pathological, and Prognostic Value of High PD-1 Expression and the Presence of Epstein–Barr Virus Reactivation in Patients with Laryngeal Cancer. Cancers 2022, 14, 480. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Zhang, W.; Ye, Q.; Zhou, Y.; Xiong, W.; He, W.; Deng, M.; Zhou, M.; Guo, X.; Chen, P.; et al. Inhibition of Epstein-Barr Virus Infection by Lactoferrin. J. Innate Immun. 2012, 4, 387–398. [Google Scholar] [CrossRef] [PubMed]
- Bandeira, C.M.; de Almeida, A.Á.; Carta, C.F.L.; Almeida, A.A.; de Figueiredo, F.A.T.; Sandrim, V.C.; Gonçalves, A.J.; Almeida, J.D. Tobacco influence in heavy metals levels in head and neck cancer cases. Environ. Sci. Pollut. Res. Int. 2018, 25, 27650–27656. [Google Scholar] [CrossRef] [PubMed]
- Golasik, M.; Jawień, W.; Przybyłowicz, A.; Szyfter, W.; Herman, M.; Golusiński, W.; Florek, E.; Piekoszewski, W. Classification models based on the level of metals in hair and nails of laryngeal cancer patients: Diagnosis support or rather speculation? Metallomics 2015, 7, 455–465. [Google Scholar] [CrossRef]
- Genchi, G.; Sinicropi, M.S.; Lauria, G.; Carocci, A.; Catalano, A. The Effects of Cadmium Toxicity. Int. J. Environ. Res. Public Health 2020, 17, 3782. [Google Scholar] [CrossRef]
- Järup, L.; Bellander, T.; Hogstedt, C.; Spång, G. Mortality and cancer incidence in Swedish battery workers exposed to cadmium and nickel. Occup. Environ. Med. 1998, 55, 755–759. [Google Scholar] [CrossRef]
- Błażewicz, A.; Wiśniewska, P.; Skórzyńska-Dziduszko, K. Selected Essential and Toxic Chemical Elements in Hypothyroidism—A Literature Review (2001–2021). Int. J. Mol. Sci. 2021, 22, 10147. [Google Scholar] [CrossRef]
- Naoum, F.A. Iron deficiency in cancer patients. Rev. Bras. Hematol. Hemoter. 2016, 38, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Lelièvre, P.; Sancey, L.; Coll, J.L.; Deniaud, A.; Busser, B. The Multifaceted Roles of Copper in Cancer: A Trace Metal Element with Dysregulated Metabolism, but Also a Target or a Bullet for Therapy. Cancers 2020, 12, 3594. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, R.; Tanaka, Y.; Senju, T.; Morita, Y.; Lee, L.; Hijioka, M.; Hisano, T.; Furukawa, M. Serum zinc levels in cancer patients are low and difficult to elevate when complicated by liver cirrhosis: A retrospective study. Medicine 2023, 102, e32703. [Google Scholar] [CrossRef] [PubMed]
- Maggini, S.; Pierre, A.; Calder, P.C. Immune Function and Micronutrient Requirements Change over the Life Course. Nutrients 2018, 10, 1531. [Google Scholar] [CrossRef] [PubMed]
- Jomova, K.; Makova, M.; Alomar, S.Y.; Alwasel, S.H.; Nepovimova, E.; Kuca, K.; Rhodes, C.J.; Valko, M. Essential metals in health and disease. Chem. Biol. Interact. 2022, 367, 110173. [Google Scholar] [CrossRef]
- Liem, D.A.; Honda, H.M.; Zhang, J.; Ping, P. Past and present course of cardioprotection against ischemia-reperfusion injury. J. Appl. Physiol. 2007, 103, 2129–2136. [Google Scholar] [CrossRef] [PubMed]
- Lukasewycz, O.A.; Prohaska, J.R.; Meyer, S.G.; Schmidtke, J.R.; Hatfield, S.M.; Marder, P. Alterations in lymphocyte subpopulations in copper-deficient mice. Infect. Immun. 1985, 48, 644–647. [Google Scholar] [CrossRef] [PubMed]
- Paulazo, M.A.; Klecha, A.J.; Sterle, H.A.; Valli, E.; Torti, H.; Cayrol, F.; Barreiro Arcos, M.L.; Cremaschi, G.A. Hypothyroidism-related zinc deficiency leads to suppression of T lymphocyte activity. Endocrine 2019, 66, 266–277. [Google Scholar] [CrossRef]
- Wessels, I.; Maywald, M.; Rink, L. Zinc as a Gatekeeper of Immune Function. Nutrients 2017, 9, 1286. [Google Scholar] [CrossRef]
- Bonaventura, P.; Benedetti, G.; Albarède, F.; Miossec, P. Zinc and its role in immunity and inflammation. Autoimmun. Rev. 2015, 14, 277–285. [Google Scholar] [CrossRef]
- Souffriau, J.; Libert, C. Mechanistic insights into the protective impact of zinc on sepsis. Cytokine Growth Factor Rev. 2018, 39, 92–101. [Google Scholar] [CrossRef]
- Mazzatti, D.J.; Uciechowski, P.; Hebel, S.; Engelhardt, G.; White, A.J.; Powell, J.R.; Rink, L.; Haase, H. Effects of long-term zinc supplementation and deprivation on gene expression in human THP-1 mononuclear cells. J. Trace Elem. Med. Biol. 2008, 22, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Hellman, N.E.; Gitlin, J.D. Ceruloplasmin metabolism and function. Annu. Rev. Nutr. 2002, 22, 439–458. [Google Scholar] [CrossRef] [PubMed]
- Jończy, A.; Mazgaj, R.; Smuda, E.; Żelazowska, B.; Kopeć, Z.; Starzyński, R.R.; Lipiński, P. The Role of Copper in the Regulation of Ferroportin Expression in Macrophages. Cells 2021, 10, 2259. [Google Scholar] [CrossRef] [PubMed]
- Kulprachakarn, K.; Chen, Y.L.; Kong, X.; Arno, M.C.; Hider, R.C.; Srichairatanakool, S.; Bansal, S.S. Copper(II) binding properties of hepcidin. J. Biol. Inorg. Chem. 2016, 21, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Seco-Cervera, M.; González-Cabo, P.; Pallardó, F.V.; Romá-Mateo, C.; García-Giménez, J.L. Thioredoxin and Glutaredoxin Systems as Potential Targets for the Development of New Treatments in Friedreich’s Ataxia. Antioxidants 2020, 9, 1257. [Google Scholar] [CrossRef] [PubMed]
- Tifoun, N.; De las Heras, J.M.; Guillaume, A.; Bouleau, S.; Mignotte, B.; Le Floch, N. Insights into the Roles of the Sideroflexins/SLC56 Family in Iron Homeostasis and Iron-Sulfur Biogenesis. Biomedicines 2021, 9, 103. [Google Scholar] [CrossRef] [PubMed]
- Torti, S.V.; Torti, F.M. Iron and Cancer: More Ore to Be Mined. Nat. Rev. Cancer 2013, 13, 342–355. [Google Scholar] [CrossRef]
- Jung, M.; Mertens, C.; Tomat, E.; Brüne, B. Iron as a Central Player and Promising Target in Cancer Progression. Int. J. Mol. Sci. 2019, 20, 273. [Google Scholar] [CrossRef]
- Jomova, K.; Valko, M. Advances in Metal-Induced Oxidative Stress and Human Disease. Toxicology 2011, 283, 65–87. [Google Scholar] [CrossRef]
- Koppenol, W.H.; Hider, R.H. Iron and Redox Cycling. Do’s and Don’ts. Free Radic. Biol. Med. 2019, 133, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Torti, S.V.; Manz, D.H.; Paul, B.T.; Blanchette-Farra, N.; Torti, F.M. Iron and Cancer. Annu. Rev. Nutr. 2018, 38, 97–125. [Google Scholar] [CrossRef]
- Lipinski, B. Hydroxyl Radical and Its Scavengers in Health and Disease. Oxid. Med. Cell. Longev. 2011, 2011, 809696. [Google Scholar] [CrossRef] [PubMed]
- Haschka, D.; Hoffmann, A.; Weiss, G. Iron in immune cell function and host defense. Semin. Cell Dev. Biol. 2021, 115, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Bassiouni, W.; Ali, M.A.M.; Schulz, R. Multifunctional intracellular matrix metalloproteinases: Implications in disease. FEBS J. 2021, 288, 7162–7182. [Google Scholar] [CrossRef] [PubMed]
- Kabata-Pendias, A.; Szteke, B. Trace Elements in Abiotic and Biotic Environments; CRC Press: Boca Raton, FL, USA, 2015; ISBN 978-0-429-16151-3. [Google Scholar]
- Brown, R.A.M.; Richardson, K.L.; Kabir, T.D.; Trinder, D.; Ganss, R.; Leedman, P.J. Altered Iron Metabolism and Impact in Cancer Biology, Metastasis, and Immunology. Front. Oncol. 2020, 10, 476. [Google Scholar] [CrossRef]
- Kakhlon, O.; Cabantchik, Z.I. The Labile Iron Pool: Characterization, Measurement, and Participation in Cellular Processes. Free Radic. Biol. Med. 2002, 33, 1037–1046. [Google Scholar] [CrossRef]
- Gaur, A.; Collins, H.; Wulaningsih, W.; Holmberg, L.; Garmo, H.; Hammar, N.; Walldius, G.; Jungner, I.; Van Hemelrijck, M. Iron Metabolism and Risk of Cancer in the Swedish AMORIS Study. Cancer Causes Control 2013, 24, 1393–1402. [Google Scholar] [CrossRef]
- Cross, A.J.; Sinha, R.; Wood, R.J.; Xue, X.; Huang, W.Y.; Yeager, M.; Hayes, R.B.; Gunter, M.J. Iron Homeostasis and Distal Colorectal Adenoma Risk in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. Cancer Prev. Res. 2011, 4, 1465–1475. [Google Scholar] [CrossRef]
- Wells, B.J.; Mainous, A.G.; Everett, C.J.; Gill, J.M. Iron, Cholesterol, and the Risk of Cancer in an 18-Year Cohort. Asian Pac. J. Cancer Prev. 2005, 6, 505–509. [Google Scholar]
- Ali, M.A.; Akhmedkhanov, A.; Zeleniuch-Jaquotte, A.; Toniolo, P.; Frenkel, K.; Huang, X. Reliability of Serum Iron, Ferritin, Nitrite, and Association with Risk of Renal Cancer in Women. Cancer Detect. Prev. 2003, 27, 116–121. [Google Scholar] [CrossRef]
- Knekt, P.; Reunanen, A.; Takkunen, H.; Aromaa, A.; Heliövaara, M.; Hakulinen, T. Body Iron Stores and Risk of Cancer. Int. J. Cancer 1994, 56, 379–382. [Google Scholar] [CrossRef]
- Mainous, A.G.; Wells, B.J.; Koopman, R.J.; Everett, C.J.; Gill, J.M. Iron, Lipids, and Risk of Cancer in the Framingham Offspring Cohort. Am. J. Epidemiol. 2005, 161, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Sempos, C.T.; Freudenheim, J.L.; Muti, P.; Smit, E. Serum Iron, Copper and Zinc Concentrations and Risk of Cancer Mortality in US Adults. Ann. Epidemiol. 2004, 14, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Wurzelmann, J.I.; Silver, A.; Schreinemachers, D.M.; Sandler, R.S.; Everson, R.B. Iron Intake and the Risk of Colorectal Cancer. Cancer Epidemiol. Biomark. Prev. 1996, 5, 503–507. [Google Scholar]
- Akatsuka, S.; Yamashita, Y.; Ohara, H.; Liu, Y.-T.; Izumiya, M.; Abe, K.; Ochiai, M.; Jiang, L.; Nagai, H.; Okazaki, Y.; et al. Fenton Reaction Induced Cancer in Wild Type Rats Recapitulates Genomic Alterations Observed in Human Cancer. PLoS ONE 2012, 7, e43403. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, U.; Wingen, L.U.; Brakensiek, K.; Wedemeyer, H.; Becker, T.; Heim, A.; Metzig, K.; Hasemeier, B.; Kreipe, H.; Flemming, P. Epigenetic Defects of Hepatocellular Carcinoma Are Already Found in Non-Neoplastic Liver Cells from Patients with Hereditary Haemochromatosis. Hum. Mol. Genet. 2007, 16, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Błażewicz, A.; Orlicz-Szczęsna, G.; Prystupa, A.; Szczęsny, P. Use of Ion Chromatography for the Determination of Selected Metals in Blood Serum of Patients with Type 2 Diabetes. J. Trace Elem. Med. Biol. 2010, 24, 14–19. [Google Scholar] [CrossRef]
- Prystupa, A.; Błażewicz, A.; Kiciński, P.; Sak, J.J.; Niedziałek, J.; Załuska, W. Serum Concentrations of Select-ed Heavy Metals in Patients with Alcoholic Liver Cirrhosis from the Lublin Region in Eastern Poland. Int. J. Environ. Res. Public Health 2016, 13, 582. [Google Scholar] [CrossRef]
- Devkota, B.P. Iron. Available online: https://emedicine.medscape.com/article/2085704-overview?form=fpf (accessed on 1 May 2022).
- Cancer survival rates from the experts at Courage Health © 2024. Available online: https://cancersurvivalrates.com (accessed on 1 May 2022).
- Lubiński, J.; Jaworowska, E.; Derkacz, R.; Marciniak, W.; Białkowska, K.; Baszuk, P.; Scott, R.J.; Lubiński, J.A. Survival of Laryngeal Cancer Patients Depending on Zinc Serum Level and Oxidative Stress Genotypes. Biomolecules 2021, 11, 865. [Google Scholar] [CrossRef]
- Doguer, C.; Ha, J.H.; Collins, J.F. Intersection of Iron and Copper Metabolism in the Mammalian Intestine and Liver. Compr. Physiol. 2018, 8, 1433–1461. [Google Scholar] [CrossRef]
- Nishito, Y.; Kambe, T. Absorption Mechanisms of Iron, Copper, and Zinc: An Overview. J. Nutr. Sci. Vitaminol. 2018, 64, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Abnet, C.C.; Lai, B.; Qiao, Y.L.; Vogt, S.; Luo, X.M.; Taylor, P.R.; Dong, Z.W.; Mark, S.D.; Dawsey, S.M. Zinc concentration in esophageal biopsy specimens measured by x-ray fluorescence and esophageal cancer risk. J. Natl. Cancer Inst. 2005, 97, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Yang, H. Ovarian cancer risk according to circulating zinc and copper concentrations: A meta-analysis and Mendelian randomization study. Clin. Nutr. 2021, 40, 2464–2468. [Google Scholar] [CrossRef]
- Vogel-González, M.; Musa-Afaneh, D.; Rivera Gil, P.; Vicente, R. Zinc Favors Triple-Negative Breast Cancer’s Microenvironment Modulation and Cell Plasticity. Int. J. Mol. Sci. 2021, 22, 9188. [Google Scholar] [CrossRef] [PubMed]
- Riesop, D.; Hirner, A.V.; Rusch, P.; Bankfalvi, A. Zinc distribution within breast cancer tissue: A possible marker for histological grading? J. Cancer Res. Clin. Oncol. 2015, 141, 1321–1331. [Google Scholar] [CrossRef]
- Xie, Y.; Wang, J.; Zhao, X.; Zhou, X.; Nie, X.; Li, C.; Huang, F.; Yuan, H. Higher serum zinc levels may reduce the risk of cervical cancer in Asian women: A meta-analysis. J. Int. Med. Res. 2018, 46, 4898–4906. [Google Scholar] [CrossRef] [PubMed]
- Costello, L.C.; Franklin, R.B. Decreased zinc in the development and progression of malignancy: An important common relationship and potential for prevention and treatment of carcinomas. Expert. Opin. Ther. Targets 2017, 21, 51–66. [Google Scholar] [CrossRef]
- Abdulla, M.; Biorklund, A.; Mathur, A.; Wallenius, K. Zinc and copper levels in whole blood and plasma from patients with squamous cell carcinomas of head and neck. J. Surg. Oncol. 1979, 12, 107–113. [Google Scholar] [CrossRef]
- Woźniak, A.; Kujawa, A.; Seńczuk-Przybyłowska, M.; Kulza, M.; Gawecki, W.; Szybiak, B.; Herman, M.; Czarnywojtek, A.; Kurhańska-Flisykowska, A.; Chesy, P.; et al. Physiological metals in the serum, hair and nails of patients with head and neck cancer. Prz. Lek. 2012, 69, 785–797. (In Polish) [Google Scholar]
- Dobrowolski, R.; Klatka, J.; Brodnjak-Voncina, D.; Trojanowska, A.; Myśliwiec, D.; Ostrowski, J.; Remer, M. Chemometric methods for studying the relationships between trace elements in laryngeal cancer and healthy tissues. Biol. Trace Elem. Res. 2014, 159, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Pavithra, V.; Sathisha, T.G.; Kasturi, K.; Mallika, D.S.; Amos, S.J.; Ragunatha, S. Serum levels of metal ions in female patients with breast cancer. J. Clin. Diagn. Res. 2015, 9, BC25–BC27. [Google Scholar] [CrossRef] [PubMed]
- Yaman, M.; Kaya, G.; Simsek, M. Comparison of trace element concentrations in cancerous and noncancerous human endometrial and ovary tissues. Int. J. Gynecol. Cancer 2007, 17, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Yang, Q. Association between serum copper levels and lung cancer risk: A meta-analysis. J. Int. Med. Res. 2018, 46, 4863–4873. [Google Scholar] [CrossRef] [PubMed]
- Baharvand, M.; Manifar, S.; Akkafan, R.; Mortazavi, H.; Sabour, S. Serum levels of ferritin, copper, and zinc in patients with oral cancer. Biomed. J. 2014, 37, 331–336. [Google Scholar] [PubMed]
- Lener, M.R.; Scott, R.J.; Wiechowska-Kozlowska, A.; Serrano-Fernandez, P.; Baszuk, P.; Jaworska-Bieniek, K.; Sukiennicki, G.; Marciniak, W.; Muszyńska, M.; Kładny, J.; et al. Serum concentrations of selenium and copper in patients diagnosed with pancreatic cancer. Cancer Res. Treat. 2016, 48, 1056–1064. [Google Scholar] [CrossRef] [PubMed]
- Ressnerova, A.; Raudenska, M.; Holubova, M.; Svobodova, M.; Polanska, H.; Babula, P.; Masarik, M.; Gumulec, J. Zinc and copper homeostasis in head and neck cancer: Review and meta-analysis. Curr. Med. Chem. 2016, 23, 1304–1330. [Google Scholar] [CrossRef] [PubMed]
- Golasik, M.; Przybyłowicz, A.; Woźniak, A.; Herman, M.; Gawęcki, W.; Golusiński, W.; Walas, S.; Krejpcio, Z.; Szyfter, K.; Florek, E.; et al. Essential metals profile of the hair and nails of patients with laryngeal cancer. J. Trace Elem. Med. Biol. 2015, 31, 67–73. [Google Scholar] [CrossRef]
- Rostkowska-Nadolska, B.; Pośpiech, L.; Bochnia, M. Content of trace elements in serum of patients with carcinoma of the larynx. Arch. Immunol. Ther. Exp. 1999, 47, 321–325. [Google Scholar]
- Borst, J.; Busselaar, J.; Bosma, D.M.T.; Ossendorp, F. Mechanism of action of PD-1 receptor/ligand targeted cancer immunotherapy. Eur. J. Immunol. 2021, 51, 1911–1920. [Google Scholar] [CrossRef]
- Seifert, A.M.; Eymer, A.; Heiduk, M.; Wehner, R.; Tunger, A.; von Renesse, J.; Decker, R.; Aust, D.E.; Welsch, T.; Reissfelder, C.; et al. PD-1 Expression by Lymph Node and Intratumoral Regulatory T Cells Is Associated with Lymph Node Metastasis in Pancreatic Cancer. Cancers 2020, 12, 2756. [Google Scholar] [CrossRef] [PubMed]
- Gianchecchi, E.; Fierabracci, A. Inhibitory Receptors and Pathways of Lymphocytes: The Role of PD-1 in Treg Development and Their Involvement in Autoimmunity Onset and Cancer Progression. Front. Immunol. 2018, 9, 2374. [Google Scholar] [CrossRef] [PubMed]
- Piersiala, K.; da Silva, P.F.N.; Lagebro, V.; Kolev, A.; Starkhammar, M.; Elliot, A.; Marklund, L.; Munck-Wikland, E.; Margolin, G.; Georén, S.K.; et al. Tumour-draining lymph nodes in head and neck cancer are characterized by accumulation of CTLA-4 and PD-1 expressing Treg cells. Transl. Oncol. 2022, 23, 101469. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Wang, D.; Zhang, G.; Guo, X. The Role of PD-1/PD-L1 Axis In Treg Development And Function: Implications For Cancer Immunotherapy. OncoTargets Ther. 2019, 12, 8437–8445. [Google Scholar] [CrossRef] [PubMed]
- Núñez, N.G.; Tosello Boari, J.; Ramos, R.N.; Richer, W.; Cagnard, N.; Anderfuhren, C.D.; Niborski, L.L.; Bigot, J.; Meseure, D.; De La Rochere, P.; et al. Tumor invasion in draining lymph nodes is associated with Treg accumulation in breast cancer patients. Nat. Commun. 2020, 11, 3272. [Google Scholar] [CrossRef] [PubMed]
- Fransen, M.F.; Schoonderwoerd, M.; Knopf, P.; Camps, M.G.; Hawinkels, L.J.; Kneilling, M.; van Hall, T.; Ossendorp, F. Tumor-draining lymph nodes are pivotal in PD-1/PD-L1 checkpoint therapy. JCI Insight 2018, 3, e124507. [Google Scholar] [CrossRef]
- Dammeijer, F.; van Gulijk, M.; Mulder, E.E.; Lukkes, M.; Klaase, L.; van den Bosch, T.; van Nimwegen, M.; Lau, S.P.; Latupeirissa, K.; Schetters, S.; et al. The PD-1/PD-L1-Checkpoint Restrains T cell Immunity in Tumor-Draining Lymph Nodes. Cancer Cell 2020, 38, 685–700.e8. [Google Scholar] [CrossRef]
- Jiang, Y.; Chen, M.; Nie, H.; Yuan, Y. PD-1 and PD-L1 in cancer immunotherapy: Clinical implications and future considerations. Hum. Vaccines Immunother. 2019, 15, 1111–1122. [Google Scholar] [CrossRef]
- Cheng, F.; Peng, G.; Lu, Y.; Wang, K.; Ju, Q.; Ju, Y.; Ouyang, M. Relationship between copper and immunity: The potential role of copper in tumor immunity. Front. Oncol. 2022, 12, 1019153. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Study Group (n = 40) | Control Group (n = 20) | p-Value | |||
|---|---|---|---|---|---|---|
| Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | |||
| Selected parameters of peripheral blood counts | WBC [103/mm3] Reference range: 4.0–10.0 | 9.64 ± 2.74 | 9.65 (2.55–15.78) | 7.19 ± 1.64 | 7.08 (4.12–10.50) | 0.0000 1 * |
| NEU [103/mm3] Reference range: 1.8–7.5 | 6.89 ± 2.68 | 6.82 (0.00–13.89) | 7.12 ± 2.68 | 7.05 (0.23–14.12) | 0.5539 1 | |
| LYM [103/mm3] Reference range: 0.6–3.4 | 1.92 ± 0.63 | 1.93 (0.69–3.22) | 1.78 ± 0.63 | 1.79 (0.55–3.08) | 0.8699 1 | |
| MON [103/mm3] Reference range: 0.0–0.9 | 0.56 ± 0.19 | 0.52 (0.00–1.06) | 0.60 ± 0.17 | 0.58 (0.28–0.91) | 0.3969 1 | |
| EOS [103/mm3] Reference range: 0.0–0.7 | 0.17 ± 0.13 | 0.14 (0.00–0.50) | 0.21 ± 0.13 | 0.18 (0.04–0.54) | 0.0733 2 | |
| BAS [103/mm3] Reference range: 0.0–0.2 | 0.04 ± 0.02 | 0.03 (0.01–0.06) | 0.03 ± 0.02 | 0.03 (0.01–0.06) | 0.6790 2 | |
| RBC [106/mm3] Reference range: 4.5–6.5 | 4.59 ± 0.52 | 4.67 (3.09–5.80) | 4.80 ± 0.52 | 4.88 (3.30–6.01) | 0.0422 2 * | |
| HGB [g/dL] Reference range: 13.0–17.5 | 14.27 ± 1.51 | 14.35 (9.50–17.70) | 15.01 ± 1.19 | 14.46 (12.36–16.66) | 0.0172 2 * | |
| HCT [%] Reference range: 40–54 | 42.08 ± 4.74 | 42.75 (28.00–49.80) | 45.90 ± 3.42 | 45.30 (10.20–56.00) | 0.0057 2 * | |
| MCV [fL] Reference range: 77–93 | 92.04 ± 5.07 | 91.53 (80.33–104.53) | 94.66 ± 5.02 | 94.30 (85.50–104.90) | 0.9769 1 | |
| MCH [pg] Reference range: 27–32 | 31.15 ± 1.68 | 31.68 (26.19–34.37) | 31.54 ± 3.78 | 31.20 (24.39–41.70) | 0.5999 1 | |
| MCHC [g/dL] Reference range: 32–38 | 34.11 ± 3.65 | 33.25 (30.77–51.01) | 32.86 ± 3.63 | 33.28 (26.36–41.96) | 0.9961 1 | |
| RDW [%] Reference range: 10.0–15.0 | 13.87 ± 1.24 | 13.60 (11.80–17.70) | 12.94 ± 0.96 | 12.89 (11.39–16.29) | 0.0010 2 * | |
| PLT [103/mm3] Reference range: 150–400 | 260.45 ± 61.73 | 259.00 (150.00–453.00) | 265.45 ± 61.81 | 265.00 (137.00–440.00) | 0.8814 1 | |
| Serum Fe (mcg/dL) | 79.87 ± 17.28 | 83.90 (43.93–125.30) | 100.86 ± 27.53 | 96.45 (54.10–186.23) | 0.00001 2 * | |
| Serum Zn (mcg/dL) | 66.36 ± 14.24 | 64.40 (43.1–93.3) | 83.89 ± 10.16 | 86.45 (63.8–107.5) | 0.00000 1 * | |
| Serum Cu (mcg/dL) | 78.24 ± 11.06 | 75.35 (69.8–125.55) | 81.96 ± 12.13 | 79.22 (61.79–117.2) | 0.04760 2 * | |
| Cu/Zn in serum | 1.23 ± 0.29 | 1.18 (0.76–1.84) | 0.98 ± 0.13 | 0.97 (0.71–1.28) | 0.00001 1 * | |
| Frequency of Occurrence [%] | Study Group (n = 40) | Control Group (n = 20) | p-Value | |||
|---|---|---|---|---|---|---|
| Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | |||
| Blood Sample | NK cells | 14.15 ± 5.58 | 14.74 (4.16–24.93) | 12.69 ± 5.59 | 13.48 (5.48–23.14) | 0.3597 1 |
| Lymphocytes T CD3+ | 69.98 ± 7.26 | 70.66 (57.27–84.20) | 76.25 ± 6.66 | 76.33 (63.34–87.66) | 0.0097 1 * | |
| Lymphocytes B CD19+ | 14.07 ± 4.18 | 14.28 (7.11–22.66 | 9.46 ± 4.38 | 8.47 (4.35–22.12) | 0.0005 1 * | |
| Lymphocytes T CD4+ CD3+ | 43.55 ± 6.61 | 42.89 (29.91–63.96) | 48.96 ± 5.89 | 47.04 (38.97–61.22) | 0.0031 2 * | |
| Lymphocytes T CD8+ CD3+ | 26.46 ± 6.32 | 25.44 (16.66–41.76) | 27.01 ± 4.51 | 26.86 (21.31–36.71) | 0.4681 1 | |
| Ratio of lymphocytes T CD4+ CD3+ to CD8+ CD3+ | 1.77 ± 0.61 | 1.69 (0.72–3.84) | 1.87 ± 0.39 | 1.80 (1.13–2.69) | 0.2607 2 | |
| Lymphocytes T CD3+ CD69+ | 5.50 ± 3.08 | 4.87 (1.40–12.32) | 3.07 ± 1.21 | 2.38 (1.77–5.74) | 0.0061 2 * | |
| Lymphocytes B CD19+ CD69+ | 6.07 ± 3.19 | 5.42 (1.32–15.42) | 6.74 ± 2.71 | 6.53 (2.17–15.40) | 0.3554 2 | |
| Lymphocytes T CD3+ CD25+ | 45.05 ± 13.86 | 45.44 (12.97–89.93) | 31.34 ± 6.01 | 30.13 (23.46–50.20) | 0.001 2 * | |
| Lymphocytes B CD19+ CD25+ | 31.20 ± 11.57 | 28.53 (10–74.64 | 30.22 ± 10.71 | 29.10 (12.04–45.48) | 0.9205 2 | |
| Lymphocytes T CD4+ CD69+ | 5.34 ± 2.85 | 4.70 (1.23–13.84) | 3.27 ± 1.99 | 2.19 (1.17–7.58) | 0.0058 2 * | |
| Lymphocytes T CD8+ CD69+ | 4.49 ± 2.36 | 3.69 (1.06–10.99 | 1.41 ± 1.05 | 1.19 (0.29–4.19) | 0.0000 2 * | |
| Lymphocytes T CD4+ CD25+ | 56.32 ± 16.01 | 53.32 (29.61–96.69) | 46.90 ± 8.41 | 45.60 (29.98–67.74) | 0.0262 2 * | |
| Lymphocytes T CD8+ CD25+ | 8.77 ± 8.46 | 5.97 (1.45–41.06) | 1.97 ± 0.88 | 1.91 (0.55–4.22) | 0.0000 2 * | |
| Lymphocytes B CD19+ PD-1+ | 4.29 ± 1.90 | 4.20 (1.14–10.87) | 6.42 ± 3.19 | 7.11 (1.73–11.34) | 0.0330 2 * | |
| Lymphocytes T CD4+ PD-1+ | 21.39 ± 5.28 | 21.44 (12.21–32.16) | 7.57 ± 1.63 | 7.49 (5.09–10.24) | 0.0000 1 * | |
| Lymphocytes T CD8+ PD-1+ | 18.15 ± 5.83 | 17.19 (10.12–32.45) | 4.33 ± 2.08 | 4.02 (1.32–8.36) | 0.0000 2 * | |
| Tumor Sample | Lymphocytes T CD3+ CD69+ | 40.08 ± 14.83 | 39.59 (5.63–74.51) | N/A | N/A | N/A |
| Lymphocytes B CD19+ CD69+ | 26.76 ± 12.69 | 24.01 (10.87–56.67) | N/A | N/A | N/A | |
| Lymphocytes T CD3+ CD25+ | 30.92 ± 15.04 | 28.87 (9.25–67.18) | N/A | N/A | N/A | |
| Lymphocytes B CD19+ CD25+ | 27.75 ± 20.56 | 19.95 (4.67–81.11) | N/A | N/A | N/A | |
| Lymphocytes T CD4+ CD69+ | 46.24 ± 18.01 | 45.50 (15.67 –81.51) | N/A | N/A | N/A | |
| Lymphocytes T CD8+ CD69+ | 42.59 ± 21.54 | 39.07 (11.25–89.92) | N/A | N/A | N/A | |
| Lymphocytes T CD4+ CD25+ | 28.87 ± 15.81 | 26.82 (6.57–64.14) | N/A | N/A | N/A | |
| Lymphocytes T CD8+ CD25+ | 9.55 ± 4.82 | 8.34 (2.12–21.12) | N/A | N/A | N/A | |
| Lymphocytes B CD19+ PD-1 | 26.41 ± 9.90 | 22.86 (12.25–50.25) | N/A | N/A | N/A | |
| Lymphocytes T CD4+ PD-1+ | 41.64 ± 16.88 | 36.97 (15.89–75.45) | N/A | N/A | N/A | |
| Lymphocytes T CD8+ PD-1+ | 42.82 ± 17.73 | 38.02 (10.45–79.45) | N/A | N/A | N/A | |
| Lymph Node Sample | Lymphocytes T CD3+ CD69+ | 26.31 ± 16.03 | 25.39 (2.74–76.58) | N/A | N/A | N/A |
| Lymphocytes B CD19+ CD69+ | 25.25 ± 11.07 | 23.61 (10.23–65.15) | N/A | N/A | N/A | |
| Lymphocytes T CD3+ CD25+ | 28.74 ± 10.04 | 28.88 (7.36–51.72) | N/A | N/A | N/A | |
| Lymphocytes B CD19+ CD25+ | 24.12 ± 8.35 | 22.20 (12.21–39.92) | N/A | N/A | N/A | |
| Lymphocytes T CD4+ CD69+ | 16.21 ± 9.89 | 13.57 (2.85–38.59) | N/A | N/A | N/A | |
| Lymphocytes T CD8+ CD69+ | 15.93 ± 10.38 | 15.43 (2.39–47.97) | N/A | N/A | N/A | |
| Lymphocytes T CD4+ CD25+ | 33.97 ± 11.42 | 31.91 (10.23–60.47) | N/A | N/A | N/A | |
| Lymphocytes T CD8+ CD25+ | 7.43 ± 5.74 | 6.06 (1.96–34.16) | N/A | N/A | N/A | |
| Lymphocytes B CD19+ PD-1 | 10.37 ± 5.49 | 8.71 (3.47–22.14) | N/A | N/A | N/A | |
| Lymphocytes T CD4+ PD-1+ | 21.63 ± 9.46 | 18.70 (9.18–42.87) | N/A | N/A | N/A | |
| Lymphocytes T CD8+ PD-1+ | 19.43 ± 6.94 | 20.07 (7.12–32.46) | N/A | N/A | N/A | |
| Grade | G1 | G2 | G3 | ANOVA p-Value | G1 vs. G2 | G1 vs. G3 | G2 vs. G3 | ||||
| Parameters | Men ± SD | Median (Range) | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | |||||
| Serum Fe | 90.48 ± 13.51 | 89.4 (73.8–125.3) | 76.34 ± 19.26 | 83.9 (43.93–102) | 74.17 ± 15.25 | 78.1 (45.87–91.6) | 0.0364 1 * | 0.0807 | 0.046 * | 0.9356 | |
| Serum Zn | 62.12 ± 11.2 | 60.4 (45.3–85.56) | 67.61 ± 13.4 | 68 (43.2–90.7) | 68.82 ± 17.56 | 64.59 (43.1–93.3) | 0.4677 1 | NS | NS | NS | |
| Serum Cu | 85.33 ± 15.59 | 79.3 (74.2–125.55) | 77 ± 8.05 | 76.4 (69.9–102.2) | 73.12 ± 4.29 | 70.7 (69.8–83.9) | 0.0064 2 * | 0.2317 | 0.0045 * | 0.3625 | |
| Cu/Zn | 1.4 ± 0.27 | 1.4 (0.95–1.84) | 1.17 ± 0.23 | 1.15 (0.79–1.67) | 1.13 ± 0.31 | 1.13 (0.75–1.84) | 0.027 2 * | 0.0879 | 0.0374 * | 1.0 | |
| Statistically significant results, p < 0.05; Statistically significant differences were analyzed with the use of 1 ANOVA test, 2 ANOVA Kruskal–Wallis test with post hoc tests to confirm where the differences occurred. | |||||||||||
| Tumor—the Size of the Primary Tumor | T2 | T3 | T4 | ANOVA p-Value | |||||||
| Parameters | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | |||||
| Serum Fe | 76.41 ± 25.25 | 81.67 (45.7–102) | 77.14 ± 16.31 | 82.5 (43.93–96) | 82.56 ± 16.2 | 84.9 (45.87–125.3) | 0.7862 2 | ||||
| Serum Zn | 69.1 ± 8.44 | 67.81 (60.4–79.45) | 67.14 ± 18 | 62.3 (43.1–90.7) | 65.09 ± 13.38 | 64.2 (43.2–93.3) | 0.8152 1 | ||||
| Serum Cu | 80.17 ± 10.26 | 78.8 (70.4–98.9) | 82.04 ± 15.34 | 76.45 (70.5–125.55) | 75.33 ± 7.19 | 73.7 (69.8–101.6) | 0.1264 2 | ||||
| Cu/Zn | 1.17 ± 0.2 | 1.11 (0.98–1.49) | 1.29 ± 0.35 | 1.23 (0.78–1.84) | 1.2 ± 0.26 | 1.16 (0.75–1.84) | 0.6009 1 | ||||
| Statistically significant results, p < 0.05; Statistically significant differences were analyzed with the use of 1 ANOVA test, 2 ANOVA Kruskal–Wallis test with post hoc tests to confirm where the differences occurred. | |||||||||||
| Nodules—Metastases in the Lymph Nodes | N0 | N1 | N2 | N3 | ANOVA p-Value | ||||||
| Parameters | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | |||
| Serum Fe | 78.83 ± 21.24 | 85.25 (43.93–102) | 84.17 ± 17.27 | 83.7 (54.78–125.3) | 79.52 ± 15.2 | 84.3 (45.87–94.6) | 70.51 ± 22.07 | 69.67 (45.7–97) | 0.8511 2 | ||
| Serum Zn | 61.94 ± 14.39 | 60.43 (45.3–90.7) | 65.61 ± 10.55 | 62.05 (52–85.56) | 65.15 ± 15.47 | 64.4 (43.1–92.45) | 82.27 ± 12.27 | 84.63 (66.51–93.3) | 0.1119 1 | ||
| Serum Cu | 78.69 ± 9.99 | 75.9 (70.4–102.2) | 79.79 ± 14.98 | 75.88 (69.9–125.55) | 76.6 ± 8.08 | 74.05 (69.8–101.6) | 79.23 ± 13.49 | 73.8 (70.4–98.9) | 0.9067 2 | ||
| Cu/Zn | 1.31 ± 0.24 | 1.26 (1.02–1.67) | 1.23 ± 0.21 | 1.22 (0.95–1.74) | 1.24 ± 0.34 | 1.15 (0.76–1.84) | 1 ± 0.34 | 0.88 (0.75–1.49) | 0.3673 1 | ||
| * Statistically significant results, p < 0.05; Statistically significant differences were analyzed with the use of 1 ANOVA test, 2 ANOVA Kruskal–Wallis test with post hoc tests to confirm where the differences occurred. | |||||||||||
| Metastases—Distant (Organ) Metastases | M0 | M1 | p-Value | ||||||||
| Parameters | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | |||||||
| Serum Fe | 84.81 ± 14.6 | 85.45 (45.7–125.3) | 65.05 ± 17.74 | 58.52 (43.93–91.6) | 0.0076 2 * | ||||||
| Serum Zn | 65.73 ± 13.15 | 64.1 (43.1–90.7) | 68.25 ± 17.8 | 64.4 (46.3–93.3) | 0.6345 1 | ||||||
| Serum Cu | 80.15 ± 12.11 | 76.75 (69.9–125.55) | 72.5 ± 2.88 | 70.8 (69.8–77.3) | 0.0125 2 * | ||||||
| Cu/Zn | 1.26 ± 0.28 | 1.2 (0.79–1.84) | 1.13 ± 0.3 | 1.13 (0.75–1.67) | 0.2235 1 | ||||||
| * Statistically significant results, p < 0.05; Statistically significant differences were analyzed with the use of 1 Student’s t-test (d.f. = 38). 2 Mann–Whitney U test. | |||||||||||
| Parameters | Study Group (n = 40) | Control Group (n = 20) | p-Value | ||
|---|---|---|---|---|---|
| Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | ||
| EBV DNA copy number/µg DNA in the tumor tissue | 266.82 ± 361.23 | 37.88 (0.00–1212.28) | 0.00 ± 0.00 | 0.00 (0.00–0.00) | 0.0000 * |
| EBV DNA copy number/µg DNA in the lymph node | 203.69 ± 286.92 | 29.95 (0.00–863.08) | 0.00 ± 0.00 | 0.00 (0.00–0.00) | 0.0000 * |
| EBV DNA copy number/µg DNA in the blood | 117.96 ± 176.25 | 16.24 (0.00–675.30) | 0.00 ± 0.00 | 0.00 (0.00–0.00) | 0.0000 * |
| IgM VCA EBV | 24.19 ± 8.98 | 21.49 (15.31–49.74) | 0.00 ± 0.00 | 0.00 (0.00–0.00) | 0.0000 * |
| IgG VCA EBV | 91.52 ± 51.17 | 77.32 (26.22–242.62) | 56.39 ± 22.19 | 53.87 (25.58–89.74) | 0.0100 * |
| Lymphocyte subpopulations | Parameters | Study Group | Control Group | ANOVA | p-Value | ||||||
| EBV+ (n = 20) | EBV− (n = 20) | EBV− (n = 20) | p-Value | Study Group EBV+ vs. EBV− | Study Group EBV+ vs. Control Group EBV− | Study Group EBV− vs. Control Group EBV− | |||||
| Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | ||||||
| T CD3+ | 69.55 ± 7.11 | 70.89 (59.02–81.68) | 70.41 ± 7.74 | 70,44 (57.27–84.20) | 76.10 ± 6.46 | 76.11 (63.34–87.66) | 0.00995 1 * | 0.71523 | 0.00415 * | 0.01598 * | |
| B CD19+ | 13.34 ± 4.18 | 13.46 (7.11–22.15) | 14.81 ± 4.26 | 14.48 (8.11–22.66) | 10.26 ± 4.54 | 9.94 (4.35–22.12) | 0.00529 1 * | 0.27644 | 0.03177 * | 0.00229 * | |
| T CD4+CD3+ | 42.26 ± 5.89 | 41.94 (29.91–57.94) | 44.83 ± 7.34 | 45.40 (33.17–63.96) | 49.29 ± 5.81 | 48.29 (38.97–61.22) | 0.00174 2 * | 0.20358 | 0.00056 * | 0.02072 * | |
| T CD3+CD69+ blood | 4.46 ± 2.68 | 3.39 (1.40–10.85) | 6.54 ± 3.25 | 6.64 (1.72–12.32) | 3.08 ± 1.16 | 2.61 (1.77–5.74) | 0.00296 2 * | 0.06787 | 0.04375 * | 0.00016 * | |
| B CD19+CD69+ blood | 5.04 ± 2.40 | 5.17 (1.32–9.12) | 7.10 ± 3.66 | 6.23 (1.77–15.42) | 6.82 ± 2.75 | 6.76 (2.17–15.40) | 0.04961 2 * | 0.04323 * | 0.04987 * | 0.88172 | |
| T CD3+CD25+ blood | 42.26 ± 11.34 | 45.44 (12.97–56.16) | 47.85 ± 16.11 | 45.39 (26.15–89.93) | 31.85 ± 7.25 | 30.02 (23.46–51.12) | 0.00041 2 * | 0.21346 | 0.00112 * | 0.00051 * | |
| CD4+CD69+ blood | 5.27 ± 2.99 | 4.44 (2.00–13.84) | 5.41 ± 2.86 | 4.84 (1.23–10.11) | 3.08 ± 1.90 | 2.14 (1.17–7.58) | 0.00392 2 * | 0.87964 | 0.00333 * | 0.00579 * | |
| CD8+CD69+ blood | 4.71 ± 2.38 | 4.35 (1.06–8.85) | 4.28 ± 2.45 | 3.66 (1.09–10.99) | 1.29 ± 1.00 | 1.10 (0.29–4.19) | 0.00001 2 * | 0.57918 | 0.00000 * | 0.00002 * | |
| CD4+CD25+ blood | 53.48 ± 14.22 | 49.49 (29.61–76.88) | 59.17 ± 17.91 | 56.58 (31.14–96.69) | 46.82 ± 8.60 | 45.10 (29.98–67.74) | 0.03072 2 * | 0.27337 | 0.07643 | 0.01436 * | |
| CD8+CD25+ blood | 9.50 ± 9.28 | 7.25 (1.45–41.06) | 8.04 ± 7.97 | 5.88 (1.76–35.94) | 2.02 ± 1.03 | 1.76 (0.55–4.59) | 0.00003 2 * | 0.57920 | 0.00000 * | 0.00001 * | |
| B CD19+PD-1 | 4.11 ± 1.70 | 3.78 (1.89–7.18) | 4.48 ± 2.15 | 4.20 (1.14–10.87) | 6.58 ± 3.08 | 7.11 (1.73–11.34) | 0.02350 2 * | 0.66512 | 0.00979 * | 0.04112 * | |
| CD4+PD-1 blood | 23.26 ± 4.47 | 22.13 (15.67–32.16) | 19.53 ± 5.60 | 17.93 (12.21–30.27) | 7.74 ± 1.66 | 7.80 (5.09–10.24) | 0.00000 1 * | 0.02530* | 0.00000 * | 0.00000 * | |
| CD8+PD-1 blood | 19.54 ± 7.36 | 17.45 (10.12–32.45) | 16.77 ± 3.65 | 16.50 (11.45–25.26) | 4.22 ± 2.07 | 4.02 (1.32–8.36) | 0.00000 2 * | 0.42482 | 0.00000 * | 0.00000 * | |
| IgG VCA EBV quantitative | 83.04 ± 35.91 | 77.04 (31.56–148.30) | 99.99 ± 63.81 | 77.77 (26.22–242.62) | 58.71 ± 21.44 | 60.33 (20.58–89.74) | 0.04617 2 * | 0.30895 | 0.03851 * | 0.05652 | |
| Parameters | Study Group | Control Group | ANOVA | Post-hoc p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| EBV+ (n = 20) | EBV− (n = 20) | EBV− | p-Value | Study Group EBV+ vs. EBV− | Study Group EBV+ vs. Control Group EBV− | Study Group EBV− vs. Control Group EBV− | ||||
| Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | |||||
| Serum Fe (mcg/dL) | 69.16 ± 16.81 | 73.75 (43.93–96.40) | 90.59 ± 10.23 | 89.50 (75.30–125.30) | 100.86 ± 27.86 | 96.45 (54.10–186.23) | 0.00001 2 * | 0.00007 * | 0.00002 * | 0.16045 |
| Serum Zn (mcg/dL) | 66.50 ± 13.75 | 63.25 (46.30–93.30) | 66.22 ± 15.07 | 66.46 (43.10–90.70) | 83.89 ± 10.16 | 86.45 (63.80–107.50) | 0.00101 1 * | 0.95238 | 0.00002 * | 0.00006 * |
| Serum Cu (mcg/dL) | 75.71 ± 7.28 | 73.95 (69.80–101.60) | 80.76 ± 13.59 | 75.90 (69.90–125.55) | 81.96 ± 12.13 | 79.22 (61.79–117.20) | 0.04998 2 * | 0.15167 | 0.01826 * | 0.39271 |
| Cu/Zn in serum | 1.19 ± 0.28 | 1.18 (0.76–1.84) | 1.27 ± 0.30 | 1.18 (0.79–1.84) | 0.98 ± 0.13 | 0.97 (0.71–1.28) | 0.00577 1 * | 0.36958 | 0.00481 * | 0.00043 * |
| Characteristics of the Basic Parameters of the Immune System | ||||||||
|---|---|---|---|---|---|---|---|---|
| Age | NK | Lymphocytes T CD3+ | Lymphocytes B CD19+ | Lymphocytes T CD4+CD3+ | Lymphocytes T CD8+CD3+ | Ratio CD4/CD8 | ||
| Serum Fe | r | −0.1600 | −0.2334 | 0.1832 | −0.0108 | 0.3674 | −0.1699 | 0.3847 |
| p | 0.324 | 0.147 | 0.258 | 0.947 | 0.020 * | 0.295 | 0.014 * | |
| Serum Zn | r | 0.236 | 0.036 | 0.065 | −0.048 | −0.009 | 0.133 | −0.109 |
| p | 0.14227 | 0.82444 | 0.69022 | 0.76893 | 0.95624 | 0.41352 | 0.50312 | |
| Serum Cu | r | −0.036 | -0.176 | 0.121 | 0.039 | 0.195 | 0.041 | 0.052 |
| p | 0.82522 | 0.27721 | 0.45754 | 0.81320 | 0.22674 | 0.79985 | 0.74786 | |
| Cu/ Zn in serum | r | −0.151 | −0.112 | −0.046 | 0.132 | 0.082 | −0.168 | 0.178 |
| p | 0.35169 | 0.49066 | 0.77998 | 0.41750 | 0.61661 | 0.29979 | 0.27220 | |
| Lymphocyte Subpopulations | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CD3+CD69+ | CD19+CD69+ | CD3+CD25+ | CD19+CD25+ | CD4+CD69+ | CD8+CD69+ | CD4+CD25+ | CD8+CD25+ | CD19+PD-1+ | CD4+PD-1+ | CD8+PD-1+ | ||||||||||||
| Serum Fe | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p |
| Blood samples | 0.257 | 0.109 | 0.165 | 0.310 | 0.101 | 0.534 | −0.171 | 0.290 | 0.187 | 0.248 | 0.092 | 0.571 | 0.064 | 0.697 | −0.187 | 0.249 | 0.213 | 0.186 | −0.180 | 0.267 | −0.042 | 0.799 |
| Tumor samples | 0.316 | 0.04708 * | −0.056 | 0.733 | 0.273 | 0.088 | 0.143 | 0.378 | 0.386 | 0.014 * | 0.210 | 0.194 | 0.360 | 0.023 * | 0.105 | 0.520 | 0.039 | 0.814 | −0.263 | 0.101 | −0.359 | 0.023 * |
| Node samples | −0.042 | 0.795 | 0.225 | 0.163 | 0.371 | 0.018 * | −0.047 | 0.772 | −0.109 | 0.503 | −0.005 | 0.978 | 0.306 | 0.055 | −0.210 | 0.193 | 0.127 | 0.434 | −0.529 | 0.000 * | −0.036 | 0.827 |
| Lymphocyte Subpopulations | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CD3+CD69+ | CD19+CD69+ | CD3+CD25+ | CD19+CD25+ | CD4+CD69+ | CD8+CD69+ | CD4+CD25+ | CD8+CD25+ | CD19+PD-1+ | CD4+PD-1+ | CD8+PD-1+ | ||||||||||||
| Serum Zn | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p |
| Blood samples | −0.020 | 0.90396 | −0.056 | 0.73095 | 0.020 | 0.90305 | 0.027 | 0.86946 | 0.060 | 0.71420 | −0.059 | 0.71756 | −0.061 | 0.70771 | 0.022 | 0.89486 | −0.054 | 0.73875 | 0.110 | 0.50120 | −0.027 | 0.86809 |
| Tumor samples | −0.147 | 0.36441 | −0.340 | 0.03190 * | −0.003 | 0.98579 | 0.058 | 0.72275 | −0.032 | 0.84464 | 0.006 | 0.97296 | 0.121 | 0.45789 | 0.144 | 0.37382 | −0.062 | 0.70358 | 0.131 | 0.42154 | −0.100 | 0.53803 |
| Node samples | −0.042 | 0.79634 | −0.103 | 0.52683 | −0.244 | 0.12914 | 0.029 | 0.85836 | 0.067 | 0.68301 | −0.098 | 0.54880 | 0.327 | 0.03918 * | −0.079 | 0.62679 | 0.074 | 0.64983 | −0.173 | 0.28602 | −0.042 | 0.79833 |
| Lymphocyte Subpopulations | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CD3+CD69+ | CD19+CD69+ | CD3+CD25+ | CD19+CD25+ | CD4+CD69+ | CD8+CD69+ | CD4+CD25+ | CD8+CD25+ | CD19+PD-1+ | CD4+PD-1+ | CD8+PD-1+ | ||||||||||||
| Serum Cu | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p |
| Blood samples | −0.088 | 0.58834 | 0.026 | 0.87123 | 0.031 | 0.84910 | −0.263 | 0.10102 | −0.280 | 0.08061 | −0.218 | 0.17695 | 0.125 | 0.44254 | −0.233 | 0.14765 | −0.215 | 0.18263 | −0.160 | 0.32366 | −0.233 | 0.14744 |
| Tumor samples | 0.364 | 0.02090 * | 0.203 | 0.20979 | 0.104 | 0.52164 | 0.137 | 0.39839 | 0.306 | 0.05492 | 0.103 | 0.52808 | 0.134 | 0.41076 | 0.302 | 0.05832 | −0.204 | 0.20649 | −0.491 | 0.00131 * | −0.339 | 0.03224 * |
| Node samples | −0.061 | 0.70890 | −0.143 | 0.37721 | 0.182 | 0.26184 | −0.014 | 0.93357 | 0.039 | 0.81277 | −0.047 | 0.77129 | 0.026 | 0.87531 | 0.272 | 0.08980 | −0.076 | 0.64021 | −0.399 | 0.01074 * | −0.459 | 0.00288 * |
| Lymphocyte Subpopulations | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CD3+CD69+ | CD19+CD69+ | CD3+CD25+ | CD19+CD25+ | CD4+CD69+ | CD8+CD69+ | CD4+CD25+ | CD8+CD25+ | CD19+PD-1+ | CD4+PD-1+ | CD8+PD-1+ | ||||||||||||
| Cu/Zn in serum | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p |
| Blood samples | −0.008 | 0.96243 | 0.064 | 0.69488 | 0.068 | 0.67457 | −0.075 | 0.64450 | −0.139 | 0.39066 | −0.045 | 0.78173 | 0.223 | 0.16684 | −0.074 | 0.64865 | −0.010 | 0.95006 | −0.090 | 0.57965 | −0.077 | 0.63745 |
| Tumor samples | 0.269 | 0.09331 | 0.395 | 0.01164 * | 0.055 | 0.73792 | −0.071 | 0.66281 | 0.126 | 0.43888 | 0.024 | 0.88488 | −0.044 | 0.78699 | 0.024 | 0.88213 | −0.025 | 0.87669 | −0.310 | 0.05147 | −0.039 | 0.80968 |
| Node samples | 0.066 | 0.68725 | 0.105 | 0.51800 | 0.226 | 0.16101 | −0.067 | 0.68169 | 0.057 | 0.72580 | 0.042 | 0.79768 | −0.250 | 0.12047 | 0.033 | 0.83880 | −0.096 | 0.55730 | −0.006 | 0.96975 | −0.122 | 0.45413 |
| Characteristics of Parameters Related to the Presence of EBV | ||||||
|---|---|---|---|---|---|---|
| EBV DNA Copy Number/µg DNA in the Tumor Tissue | EBV DNA Copy Number/µg DNA in the Lymph Node | EBV DNA Copy Number/µg DNA in the Blood | IgM VCA EBV Quantitatively | IgG VCA EBV Quantitatively | ||
| Serum Fe | r | 0.3319 | 0.3518 | 0.1723 | 0.2457 | 0.1085 |
| p | 0.153 | 0.128 | 0.468 | 0.296 | 0.505 | |
| Serum Zn | r | −0.105 | −0.096 | −0.140 | −0.183 | −0.026 |
| p | 0.658 | 0.68649 | 0.55649 | 0.43879 | 0.91480 | |
| Serum Cu | r | −0.243 | −0.236 | −0.234 | −0.522 | 0.150 |
| p | 0.30183 | 0.31592 | 0.32070 | 0.01818 * | 0.52654 | |
| Cu/ Zn in serum | r | 0.054 | 0.048 | 0.078 | 0.048 | −0.035 |
| p | 0.82067 | 0.84034 | 0.74315 | 0.84034 | 0.88490 | |
| Parameters | Study Group (n = 40) | Nonsurvivng vs. Surviving Patients p-Value | |||
|---|---|---|---|---|---|
| Nonsurivivng Patients (n = 10) | Surviving Patients (n = 30) | ||||
| Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | ||
| WBC [103/mm3] | 9.52 ± 3.26 | 9.18 (5.83–15.78) | 9.67 ± 2.66 | 9.69 (2.55–15.78) | 0.89510 1 |
| NEU [103/mm3] | 6.78 ± 3.45 | 5.81 (3.16–13.89) | 6.93 ± 2.49 | 6.91 (0–13.89) | 0.88470 1 |
| LYM [103/mm3] | 1.83 ± 0.52 | 1.84 (1.12–3.08) | 1.76 ± 0.68 | 1.63 (0.55–2.98) | 0.78365 1 |
| MON [103/mm3] | 0.59 ± 0.20 | 0.52 (0.42–1.06) | 0.55 ± 0.19 | 0.52 (0–0.89) | 0.55694 1 |
| EOS [103/mm3] | 0.18 ± 0.15 | 0.14 (0.03–0.50) | 0.16 ± 0.13 | 0.14 (0–0.5) | 0.88804 2 |
| BAS [103/mm3] | 0.03 ± 0.01 | 0.03 (0.01–0.06) | 0.04 ± 0.02 | 0.04 (0.01–0.07) | 0.31570 2 |
| NEU [%] | 67.73 ± 12.68 | 67.45 (53.50–88.00) | 69.18 ± 15.73 | 73.70 (0–90.60) | 0.44961 2 |
| LYM [%] | 21.83 ± 9.49 | 22.15 (7.10–32.50) | 21.16 ± 16.10 | 17.80 (4.90–98.40) | 0.44963 2 |
| MON [%] | 6.51 ± 2.11 | 6.00 (4.00–10.90) | 5.79 ± 2.01 | 5.50 (0–10.40) | 0.44947 2 |
| EOS [%] | 1.91 ± 1.48 | 1.55 (0.2–4.00) | 1.75 ± 1.54 | 1.30 (0–6.80) | 0.77186 2 |
| BAS [%] | 0.35 ± 0.15 | 0.30 (0.10–0.60) | 0.45 ± 0.31 | 0.40 (0.1–1.6) | 0.49357 2 |
| RBC [106/mm3] | 4.70 ± 0.26 | 4.71 (4.36–5.06) | 4.56 ± 0.59 | 4.59 (3.09–5.8) | 0.46256 2 |
| HGB [g/dl] | 14.12 ± 0.81 | 14.40 (12.60–15.00) | 14.32 ± 1.72 | 14.25 (9.5–17.7) | 0.87575 2 |
| HCT [%] | 42.98 ± 2.49 | 44.15 (38.70–45.30) | 43.37 ± 5.25 | 44.2 (28–54.7) | 0.67312 2 |
| MCV [fL] | 92.91 ± 4.42 | 93.70 (87.30–101.60) | 95.25 ± 5.22 | 95.4 (85.5–104.9) | 0.18393 1 |
| MCH [Pg] | 30.50 ± 1.69 | 30.55 (28.30–32.60) | 31.51 ± 1.39 | 31.8 (28.4–34.2) | 0.10945 1 |
| MCHC [g/dL] | 32.80 ± 0.74 | 32.55 (32.00–34.20) | 33.15 ± 1.00 | 33.2 (30.9–35.5) | 0.25492 1 |
| RDW [%] | 13.80 ± 1.14 | 13.55 (12.90–16.60) | 13.80 ± 1.35 | 13.55 (11.8–17.7) | 0.93766 2 |
| PLT [103/mm3] | 255.60 ± 50.59 | 260.00 (150.00–334.00) | 262.07 ± 66.72 | 259 (150–453) | 0.91289 1 |
| MPV [fL] | 7.39 ± 1.20 | 6.85 (6.30–9.40) | 7.67 ± 1.12 | 7.45 (6.2–10.6) | 0.38111 2 |
| Creatinine [mg/dl] | 0.65 ± 0.15 | 0.60 (0.5–1.00) | 0.73 ± 0.23 | 0.7 (0.5–1.6) | 0.25299 2 |
| Serum Fe [mcg/dL] | 66.89 ± 16.05 | 66.93 (43.93–91.60) | 87.66 ± 13.38 | 87.4 (45.7–125.3) | 0.00039 2 * |
| Serum Zn [mcg/dL] | 66.44 ± 16.02 | 64.2 (45.3–93.3) | 66.31 ± 13.42 | 66.4 (43.1–90.7) | 0.97725 1 |
| Serum Cu [mcg/dL] | 72.88 ± 3.66 | 70.7 (69.8–82.1) | 81.45 ± 12.74 | 78.1 (70.5–125.55) | 0.001192 * |
| Cu/Zn in serum | 1.16 ± 0.29 | 1.13 (0.76–1.67) | 1.27 ± 0.28 | 1.21 (0.79–1.84) | 0.23425 1 |
| Parameters | Study Group (n = 40) | Nonsurviving vs. Surviving Patients p-Value | |||
|---|---|---|---|---|---|
| Nonsurviving Patients (n = 15) | Surviving Patients (n = 25) | ||||
| Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | ||
| EBV DNA copy numer/µg DNA in the tumor tissue | 509.80 ± 433.43 | 367.46 (0–1212.28) | 121.04 ± 221.03 | 0 (0–635.66) | 0.00043 * |
| EBV DNA copy numer/ µg DNA in the lymph node | 401.11 ± 355.42 | 232.52 (0–863.08) | 85.21 ± 156.64 | 0 (0–456.35) | 0.00038 * |
| EBV DNA copy numer/µg DNA in the blood | 248.20 ± 223.95 | 126.59 (0–675.30) | 39.82 ± 74.53 | 0 (0–272.82) | 0.00027 * |
| IgM VCA EBV | 26.12 ± 10.10 | 23.3 (15.31–49.74) | 20.61 ± 6.46 | 17.59 (15.4–30) | 0.23458 |
| IgG VCA EBV | 76.82 ± 39.24 | 72.65 (31.56–148.3) | 100.33 ± 57.01 | 90.08 (26.22–242.62) | 0.15422 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wojnicka, J.; Grywalska, E.; Hymos, A.; Mertowska, P.; Mertowski, S.; Charytanowicz, M.; Klatka, M.; Klatka, J.; Dolliver, W.R.; Błażewicz, A. The Relationship between Cancer Stage, Selected Immunological Parameters, Epstein–Barr Virus Infection, and Total Serum Content of Iron, Zinc, and Copper in Patients with Laryngeal Cancer. J. Clin. Med. 2024, 13, 511. https://doi.org/10.3390/jcm13020511
Wojnicka J, Grywalska E, Hymos A, Mertowska P, Mertowski S, Charytanowicz M, Klatka M, Klatka J, Dolliver WR, Błażewicz A. The Relationship between Cancer Stage, Selected Immunological Parameters, Epstein–Barr Virus Infection, and Total Serum Content of Iron, Zinc, and Copper in Patients with Laryngeal Cancer. Journal of Clinical Medicine. 2024; 13(2):511. https://doi.org/10.3390/jcm13020511
Chicago/Turabian StyleWojnicka, Julia, Ewelina Grywalska, Anna Hymos, Paulina Mertowska, Sebastian Mertowski, Małgorzata Charytanowicz, Maria Klatka, Janusz Klatka, Wojciech Remington Dolliver, and Anna Błażewicz. 2024. "The Relationship between Cancer Stage, Selected Immunological Parameters, Epstein–Barr Virus Infection, and Total Serum Content of Iron, Zinc, and Copper in Patients with Laryngeal Cancer" Journal of Clinical Medicine 13, no. 2: 511. https://doi.org/10.3390/jcm13020511
APA StyleWojnicka, J., Grywalska, E., Hymos, A., Mertowska, P., Mertowski, S., Charytanowicz, M., Klatka, M., Klatka, J., Dolliver, W. R., & Błażewicz, A. (2024). The Relationship between Cancer Stage, Selected Immunological Parameters, Epstein–Barr Virus Infection, and Total Serum Content of Iron, Zinc, and Copper in Patients with Laryngeal Cancer. Journal of Clinical Medicine, 13(2), 511. https://doi.org/10.3390/jcm13020511