

Analysis of Clinical Pattern of Musculoskeletal Disorders in the Cervical and Cervico—Thoracic Regions of the Spine
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
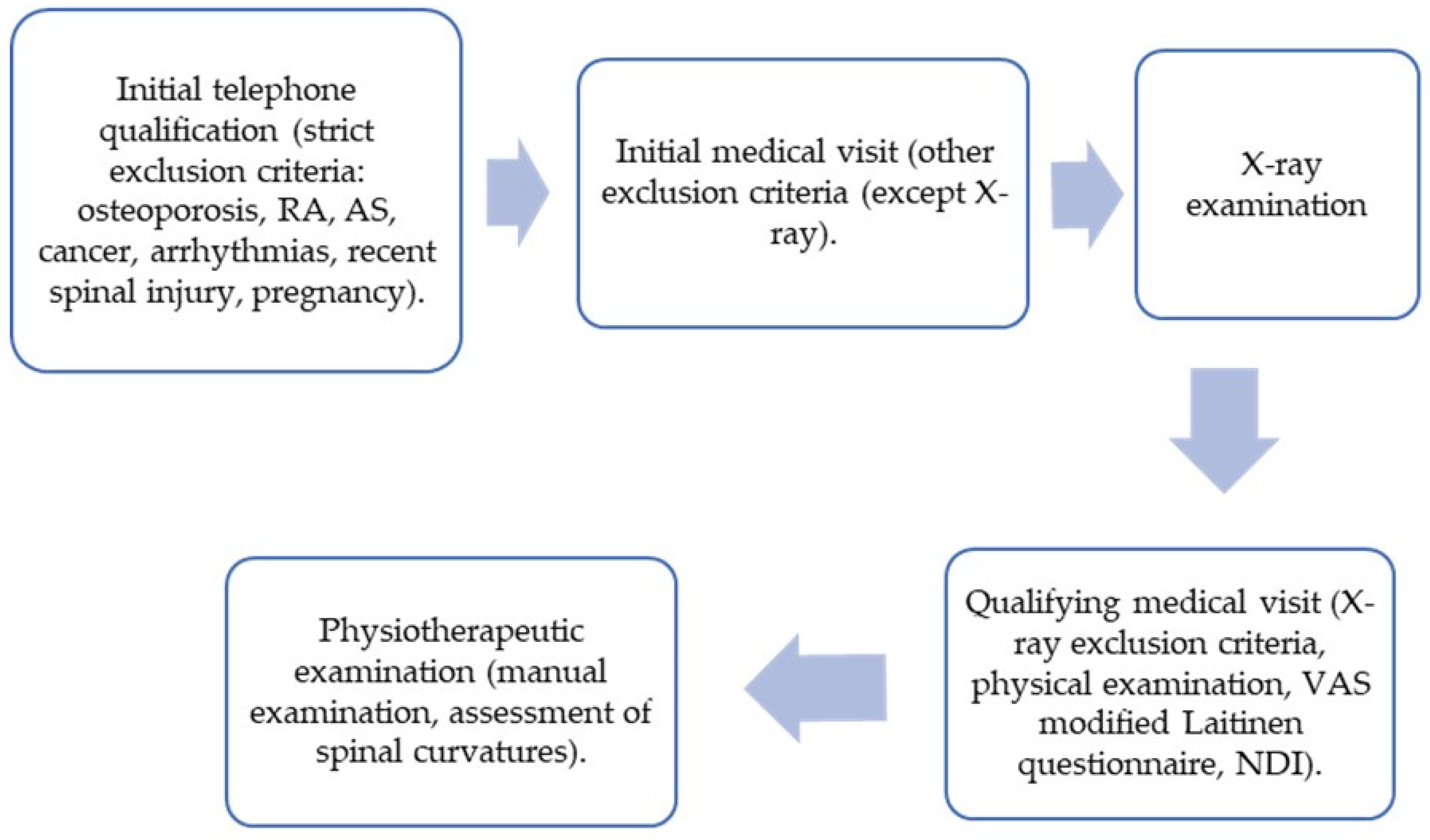
2.1. Participants
2.2. Protocol
2.2.1. Manual Examination
Patient Examination Methodology—General Principles
- −
- C0/C1—physiotherapist assesses movements taking place in this segment (flexion, extension, flexion to the left with rotation to the right, and flexion to the right with rotation to the left). The physiotherapist passively moves the head with one hand while the second hand palpates the space between the transverse process of C1 and mastoid process of the temporal bone. The examination is carried out on both sides.
- −
- C1/C2—physiotherapist assesses movements taking place in this segment (flexion, extension, rotation to the left, and rotation to the right). The physiotherapist passively moves the head and neck with one hand while the second hand palpates the space between the vertebral arc of C1 and the spinous process of C2.
- −
- C2/C3-Th3/Th4—physiotherapist assesses movements taking place in each segment (flexion, extension, lateral flexion to the left, lateral flexion to the right, rotation to the left, and rotation to the right). The physiotherapist passively moves the head and neck with one hand while the second hand palpates the space between the vertebral spinous processes of the tested segment.
Interpretation
2.2.2. Assessment of Spinal Curvature
2.2.3. Assessment of Pain Intensity
2.2.4. Assessment of Neck Pain-Related Disability
2.2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group
3.2. Functional Disorders Observed in Segments C0/C1-Th3/Th4
3.3. Functional Disorders in Relation to the Upper, Middle, and Lower Cervical Spine
3.3.1. Upper Cervical Spine (C0/C1-C1/C2)—2 Segments
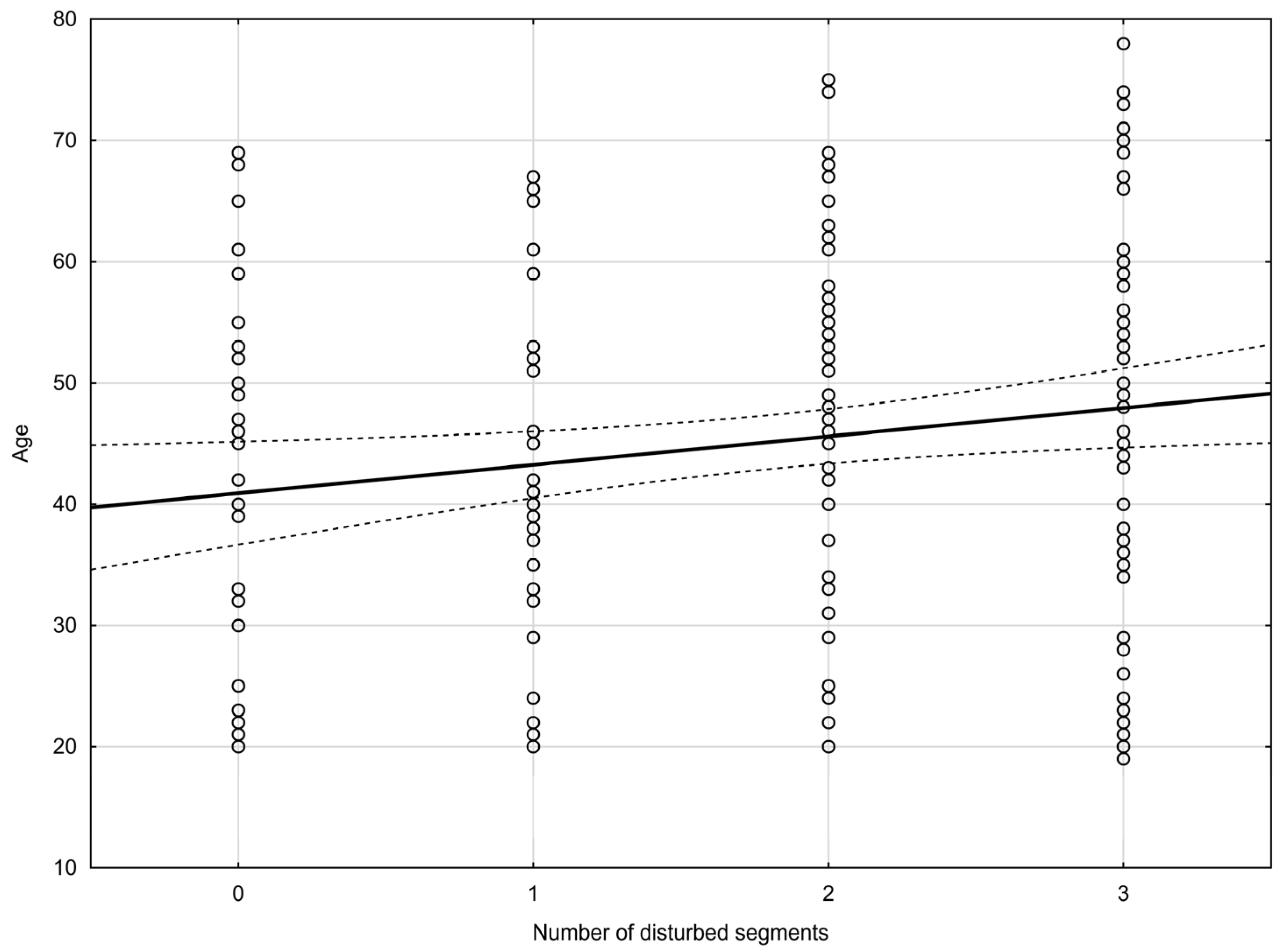
3.3.2. Middle Cervical Spine (C2/C3-C4/C5)—3 Segments
3.3.3. Lower Cervical Spine (C5/C6-Th3/Th4)—6 Segments
3.4. Functional Disorders in Relation to Sex and Age
3.4.1. Functional Disorders in Relation to Sex
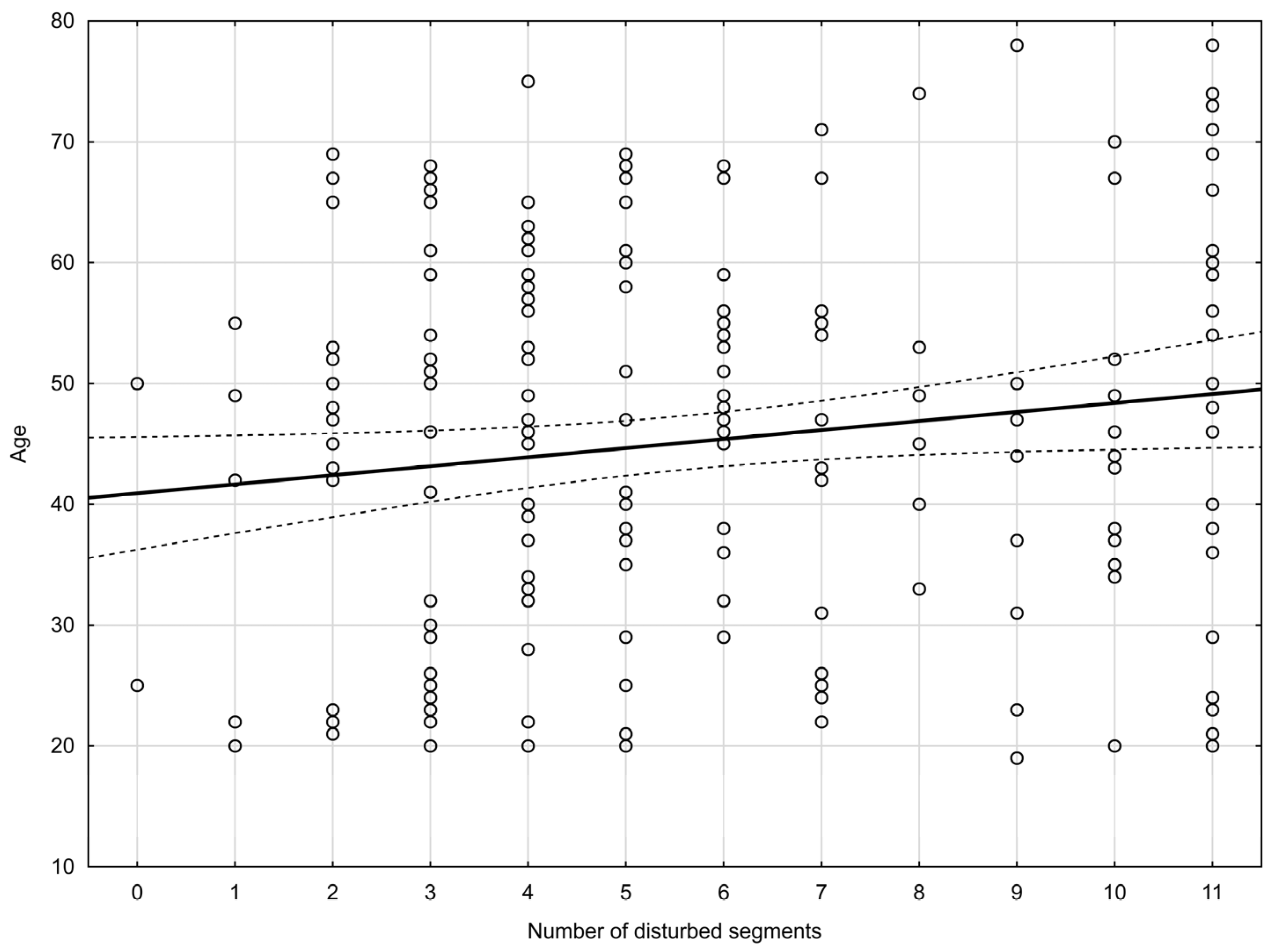
3.4.2. Functional Disorders in Relation to Age
3.5. Assessment of Spinal Curvatures
4. Discussion
Limitation of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- -
- unstable ischemic heart disease,
- -
- acute coronary syndrome in the last three months,
- -
- hemodynamically significant heart defects,
- -
- arrhythmias—atrial fibrillation (paroxysmal and persistent), uncontrolled heart rhythm disturbances,
- -
- heart failure above class II acc. NYHA,
- -
- uncontrolled hypertension (blood pressure at visit > 150/95 mmHg,
- -
- untreated hyperthyroidism and/or strumectomy performed within 3 months before visit 1 and/or the presence of a large thyroid goiter impairing the mobility of the neck,
- -
- uncontrolled diabetes and/or diabetic retinopathy and/or diabetic neuropathy,
- -
- diagnosed polyneuropathy or neuropathy,
- -
- obesity with a BMI > 35,
- -
- diagnosed osteoporosis and/or a history of low-energy fractures
- -
- condition after craniocerebral injuries with hospitalization for more than 7 days, up to 6 months,
- -
- status after neurosurgical operations in the field of the brain performed up to 12 months,
- -
- condition after documented spinal injuries up to 6 months,
- -
- status after spinal surgeries performed up to 12 months,
- -
- persistent ailments after spine surgeries and/or spinal implants,
- -
- instability of the cervical spine above 4 mm found in an X-ray examination,
- -
- spine degenerative disease Kellgren-Lawrence-Grading-System 4 degrees found in an X-ray examination,
- -
- cervical lordosis disorders—kyphotization found in an X-ray examination,
- -
- fractures within the articular bodies and processes, spinous found in an X-ray examination,
- -
- congenital defects of the spine (bone blocks, semivertebrae, Kimerle’s syndrome, other congenital defects) found in an X-ray examination,
- -
- radiological features of osteoporosis (including fracture),
- -
- inflammation of the shaft and disc—discitis found in an X-ray examination,
- -
- condition after surgery with an implant or cement found in an X-ray examination,
- -
- neoplastic changes, metastases to the bones of the spine found in an X-ray examination,
- -
- symptomatic vertebral and basal artery insufficiency and/or a positive De Kleyn test,
- -
- diagnosed with RA (rheumatoid arthritis),
- -
- diagnosed AS (ankylosing spondylitis),
- -
- diagnosed exacerbation of PsA (psoriatic arthritis) within 12 months,
- -
- exacerbation of other systemic connective tissue diseases involving the cervical spine diagnosed within 12 months,
- -
- past or active inflammation of the spine,
- -
- significant mental disorders that may affect the safety or results of the experiment, taking psychoactive substances, addiction to drugs, legal highs, drugs, alcohol now and in the past,
- -
- hemophilia and other bleeding disorders,
- -
- patients treated with oral or parenteral anticoagulants,
- -
- active cancer,
- -
- condition after anti-cancer treatment including chemotherapy or radiotherapy,
- -
- infectious diseases untreated or under treatment,
- -
- abdominal surgeries up to 12 weeks after surgery,
- -
- chest surgeries up to 12 weeks after surgery,
- -
- pregnancy,
- -
- active gastric and/or duodenal ulcer,
- -
- expected unavailability of the patient during the experiment or up to 1 month after its completion,
- -
- current participation in another medical experiment,
- -
- current legal and/or insurance claims regarding the patient’s health,
- -
- inability to assume a sitting position on your own,
- -
- lack of cooperation on the part of the patient.
References
- Childress, M.A.; Stuek, S.J. Neck Pain: Initial Evaluation and Management. Am. Fam. Physician 2020, 102, 150–156. [Google Scholar]
- Popescu, A.; Lee, H. Neck Pain and Lower Back Pain. Med. Clin. N. Am. 2020, 104, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Fandim, J.V.; Nitzsche, R.; Michaleff, Z.A.; Pena Costa, L.O.; Saragiotto, B. The contemporary management of neck pain in adults. Pain Manag. 2021, 11, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Barreto, T.W.; Svec, J.H. Chronic Neck Pain: Nonpharmacologic Treatment. Am. Fam. Physician 2019, 100, 180–182. [Google Scholar] [PubMed]
- Kazeminasab, S.; Nejadghaderi, S.A.; Amiri, P.; Pourfathi, H.; Araj-Khodaei, M.; Sullman MJ, M.; Kolahi, A.A.; Safiri, S. Neck pain: Global epidemiology, trends and risk factors. BMC Musculoskelet. Disord. 2022, 23, 26. [Google Scholar] [CrossRef] [PubMed]
- May, S.; Gardiner, E.; Young, S.; Klaber-Moffett, J. Predictor Variables for a Positive Long-Term Functional Outcome in Patients with Acute and Chronic Neck and Back Pain Treated with a McKenzie Approach: A Secondary Analysis. J. Man. Manip. Ther. 2008, 16, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Peterson, C.; Bolton, J.; Humphreys, B.K. Predictors of outcome in neck pain patients undergoing chiropractic care: Comparison of acute and chronic patients. Chiropr. Man. Ther. 2012, 20, 27. [Google Scholar] [CrossRef]
- Mahmoud, N.F.; Hassan, K.A.; Abdelmajeed, S.F.; Moustafa, I.M.; Silva, A.G. The Relationship Between Forward Head Posture and Neck Pain: A Systematic Review and Meta-Analysis. Curr. Rev. Musculoskelet. Med. 2019, 12, 562–577. [Google Scholar] [CrossRef]
- Derakhshanrad, N.; Yekaninejad, M.S.; Mehrdad, R.; Saberi, H. Neck pain associated with smartphone overuse: Cross-sectional report of a cohort study among office workers. Eur. Spine J. 2021, 30, 461–467. [Google Scholar] [CrossRef]
- Minoonejad, H.; Feiz Khademi, A.; Akochakian, M.; Moghadas Tabrizi, Y. Investigating the Effect of Simultaneous Dual Task Execution on the Balance Position of People with Forward Head Posture. Int. J. Mot. Control Learn. 2023, 5, 43–50. [Google Scholar]
- Deodato, M.; Granato, A.; Borgino, C.; Galmonte, A.; Manganotti, P. Instrumental assessment of physiotherapy and onabolulinumtoxin-A on cervical and headache parameters in chronic migraine. Neurol Sci. 2022, 43, 2021–2029. [Google Scholar] [CrossRef]
- Kaltenborn, F.M.; Evjenth, O. Manual Mobilization of the Extremity Joints; Orthopedic Physical Therapy Products: Minneapolis, MN, USA, 1989. [Google Scholar]
- Maitland, G.D. The Maitland Concept: Assessment, examination and treatment of movement impairments by passive movement. Maitland’s Vertebr. Manip. Manag. Neuromusculoskel. Disord. 2013, 1, 1. [Google Scholar]
- Blanpied, P.R.; Gross, A.R.; Elliott, J.M.; Devaney, L.L.; Clewley, D.; Walton, D.M.; Sparks, C.; Robertson, E.K. Neck Pain: Revision 2017. J. Orthop. Sports Phys. Ther. 2017, 47, A1–A83. [Google Scholar] [CrossRef]
- Banks, K.; Hengeveld, E. Terapia Manualna Według Maitlanda, 1st ed.; Elsevier: Wrocław, Poland, 2013; p. 176. [Google Scholar]
- Van Minnen, J.H. Biomechanics of the spine. In Clinical Patterns in Manual Therapy, 2nd ed.; Westerhuis, P., Wiesner, R., Eds.; Georg Thieme Publishing Company: Stuttgart, Germany, 2015; p. 103. [Google Scholar]
- Corp, N.; Mansell, G.; Stynes, S.; Wynne-Jones, G.; Morsø, L.; Hill, J.C.; van der Windt, D.A. Evidence-based treatment recommendations for neck and low back pain across Europe: A systematic review of guidelines. Eur. J. Pain 2021, 25, 275–295. [Google Scholar] [CrossRef]
- Guzman, J.; Haldeman, S.; Carroll, L.J.; Carragee, E.J.; Hurwitz, E.L.; Peloso, P.; Nordin, M.; Cassidy, J.D.; Holm, L.W.; Côté, P.; et al. Clinical practice implications of the Bone and Joint Decade 2000𠈓2010 Task Force on Neck Pain and Its Associated Disorders: From concepts and findings to recommendations. Spine 2008, 33 (Suppl. S4), 199–213. [Google Scholar] [CrossRef]
- Norlander, S.; Gustavsson, B.A.; Lindell, J.; Nordgren, B. Reduced mobility in the cervico-thoracic motion segment--a risk factor for musculoskeletal neck-shoulder pain: A two-year prospective follow-up study. Scand. J. Rehabil. Med. 1997, 29, 167–174. [Google Scholar]
- Kaltenborn, F.M. Kręgosłup—Badanie Manualne i Mobilizacja, 1st ed.; Rolewski Nowa Wieś: Lubicz, Poland, 1998; pp. 253–267, 302–311. [Google Scholar]
- Chiarotto, A.; Maxwell, L.J.; Ostelo, R.W.; Boers, M.; Tugwell, P.; Terwee, C.B. Measurement Properties of Visual Analogue Scale, Numeric Rating Scale, and Pain Severity Subscale of the Brief Pain Inventory in Patients with Low Back Pain: A Systematic Review. J. Pain 2019, 20, 245–263. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63 (Suppl. S11), 240–252. [Google Scholar] [CrossRef]
- Kamper, S.J. Pain intensity ratings. J. Physiother. 2012, 58, 61. [Google Scholar] [CrossRef]
- Zwolińska, J.; Weres, A.; Wyszyńska, J. One-Year Follow-Up of Spa Treatment in Older Patients with Osteoarthritis: A Prospective, Single Group Study. BioMed. Res. Int. 2018, 2018, 7492106. [Google Scholar] [CrossRef]
- Rottermund, J.; Knapik, A.; Saulicz, E.; Myśliwiec, A.; Saulicz, M.; Rygiel, K.A.; Linek, P. Back and neck pain among school teachers in Poland and its correlations with physical activity. Med. Pr. 2015, 66, 771–778. [Google Scholar] [CrossRef]
- Moses, M.J.; Tishelman, J.C.; Stekas, N.; Jevotovsky, D.S.; Vasquez-Montes, D.; Karia, R.; Errico, T.; Buckland, A.; Protopsaltis, T.S. Comparison of Patient Reported Outcome Measurement Information System with Neck Disability Index and Visual Analog Scale in Patients with Neck Pain. Spine 2019, 44, 162–167. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Langhorst, J.; Dobos, G.J.; Michalsen, A. Validation of the German version of the Neck Disability Index (NDI). BMC Musculoskelet. Disord. 2014, 15, 91. [Google Scholar] [CrossRef]
- Safiri, S.; Kolahi, A.A.; Hoy, D.; Buchbinder, R.; Mansournia, M.A.; Bettampadi, D.; Ashrafi-Asgarabad, A.; Almasi-Hashiani, A.; Smith, E.; Sepidarkish, M.; et al. Global, regional, and national burden of neck pain in the general population, 1990-2017: Systematic analysis of the Global Burden of Disease Study 2017. BMJ 2020, 368, m791. [Google Scholar] [CrossRef]
- Cunha, A.C.; Burke, T.N.; França, F.J.; Marques, A.P. Effect of global posture reeducation and of static stretching on pain, range of motion, and quality of life in women with chronic neck pain: A randomized clinical trial. Clinics 2008, 63, 763–770. [Google Scholar] [CrossRef]
- Fjellner, A.; Bexander, C.; Faleij, R.; Strender, L.E. Interexaminer reliability in physical examination of the cervical spine. J. Manip. Physiol. Ther. 1999, 22, 511–516. [Google Scholar] [CrossRef]
- Axelsson, P.; Karlsson, B.S. Intervertebral mobility in the progressive degenerative process. A radiostereometric analysis. Eur. Spine J. 2004, 13, 567–572. [Google Scholar] [CrossRef]
- Peng, B.; Yang, L.; Li, Y.; Liu, T.; Liu, Y. Cervical Proprioception Impairment in Neck Pain-Pathophysiology, Clinical Evaluation, and Management: A Narrative Review. Pain Ther. 2021, 10, 143–164. [Google Scholar] [CrossRef]
- Ylinen, J.; Takala, E.P.; Kautiainen, H.; Nykänen, M.; Häkkinen, A.; Pohjolainen, T.; Karppi, S.L.; Airaksinen, O. Association of neck pain, disability and neck pain during maximal effort with neck muscle strength and range of movement in women with chronic non-specific neck pain. Eur. J. Pain 2004, 8, 473–478. [Google Scholar] [CrossRef]
- Suvarnnato, T.; Puntumetakul, R.; Kaber, D.; Boucaut, R.; Boonphakob, Y.; Arayawichanon, P.; Chatchawan, U. The effects of thoracic manipulation versus mobilization for chronic neck pain: A randomized controlled trial pilot study. J. Phys. Ther. Sci. 2013, 25, 865–871. [Google Scholar] [CrossRef]
- Ghorbani, F.; Kamyab, M.; Azadinia, F. Smartphone Applications as a Suitable Alternative to CROM Device and Inclinometers in Assessing the Cervical Range of Motion in Patients with Nonspecific Neck Pain. J. Chiropr. Med. 2020, 19, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Grip strength: A summary of studies comparing dominant and nondominant limb measurements. Percept. Mot. Ski. 2003, 96 Pt 1, 728–730. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Balthillaya, G.; Neelapala YV, R. Immediate effects of cervicothoracic junction mobilization versus thoracic manipulation on the range of motion and pain in mechanical neck pain with cervicothoracic junction dysfunction: A pilot randomized controlled trial. Chiropr. Man. Ther. 2020, 28, 38. [Google Scholar] [CrossRef]
- McLean, S.M.; May, S.; Klaber-Moffett, J.; Sharp, D.M.; Gardiner, E. Risk factors for the onset of non-specific neck pain: A systematic review. J. Epidemiol. Community Health 2010, 64, 565–572. [Google Scholar] [CrossRef]
- Palacios-Ceña, D.; Albaladejo-Vicente, R.; Hernández-Barrera, V.; Lima-Florencio, L.; Fernández-de-Las-Peñas, C.; Jimenez-Garcia, R.; López-de-Andrés, A.; de Miguel-Diez, J.; Perez-Farinos, N. Female Gender Is Associated with a Higher Prevalence of Chronic Neck Pain, Chronic Low Back Pain, and Migraine: Results of the Spanish National Health Survey, 2017. Pain Med. 2021, 22, 382–395. [Google Scholar] [CrossRef]
- Mills SE, E.; Nicolson, K.P.; Smith, B.H. Chronic pain: A review of its epidemiology and associated factors in population-based studies. Br. J. Anaesth. 2019, 123, e273–e283. [Google Scholar] [CrossRef]
- Vink, D.; Aartsen, M.J.; Schoevers, R.A. Risk factors for anxiety and depression in the elderly: A review. J. Affect. Disord. 2008, 106, 29–44. [Google Scholar] [CrossRef]
- Xu, Y.; Wang, Y.; Chen, J.; He, Y.; Zeng, Q.; Huang, Y.; Xu, X.; Lu, J.; Wang, Z.; Sun, X.; et al. The comorbidity of mental and physical disorders with self-reported chronic back or neck pain: Results from the China Mental Health Survey. J. Affect. Disord. 2020, 260, 334–341. [Google Scholar] [CrossRef]
- Frontera, W.R. Physiologic Changes of the Musculoskeletal System with Aging: A Brief Review. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 705–711. [Google Scholar] [CrossRef]
- Kocur, P.; Tomczak, M.; Wiernicka, M.; Goliwąs, M.; Lewandowski, J.; Łochyński, D. Relationship between age, BMI, head posture and superficial neck muscle stiffness and elasticity in adult women. Sci. Rep. 2019, 9, 8515. [Google Scholar] [CrossRef]
- Lenoir, T.; Hoffmann, E.; Thevenin-Lemoine, C.; Lavelle, G.; Rillardon, L.; Guigui, P. Neurological and functional outcome after unstable cervicothoracic junction injury treated by posterior reduction and synthesis. Spine J. 2006, 6, 507–513. [Google Scholar] [CrossRef]
- Hardacker, J.W.; Shuford, R.F.; Capicotto, P.N.; Pryor, P.W. Radiographic standing cervical segmental alignment in adult volunteers without neck symptoms. Spine 1997, 22, 1472–1480. [Google Scholar] [CrossRef]
- Grob, D.; Frauenfelder, H.; Mannion, A.F. The association between cervical spine curvature and neck pain. Eur. Spine J. 2007, 16, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Hariharan, K.V.; Timko, M.G.; Bise, C.G.; Sundaram, M.; Schneider, M.J. Inter-examinerreliability study of physical examination procedures to assess the cervical spine. Chiropr. Man. Ther. 2021, 29, 20. [Google Scholar] [CrossRef] [PubMed]
- Billis, E.V.; Foster, N.E.; Wright, C.C. Reproducibility and repeatability: Errors of three groups of physiotherapists in locating spinal levels by palpation. Man. Ther. 2003, 8, 223–232. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Mean ± SD |
|---|---|
| Age (years) | 45.1 ± 16.1 |
| BMI (kg/m2) | 25.69 ± 4.09 |
| VAS (points) | 3.1 ± 2.3 |
| modified Laitinen questionnaire (points) | 3.5 ± 2.4 |
| NDI (points) | 7.6 ± 6.1 |
| Average number of segments with movement restrictions | 5.63 ± 3.07 |
| C0/C1 | ||||||
| Mobility Restrictions | Flexion n [%] | Extension n [%] | Lateral Flexion to the Left with Rotation to the Right n [%] | Lateral Flexion to the Right with Rotation to the Left n [%] | ||
| Unrestricted movement | 163 [81.5] | 168 [84.0] | 147 [73.5] | 151 [75.5] | ||
| Restricted movement | 33 [16.5] | 29 [14.5] | 46 [23.0] | 44 [22.0] | ||
| No movement | 1 [0.5] | 2 [1.0] | 6 [3.0] | 4 [2.0] | ||
| No observation | 3 [1.5] | 1 [0.5] | 1 [0.5] | 1 [0.5] | ||
| C1/C2 | ||||||
| Mobility Restrictions | Flexion n [%] | Extension n [%] | Rotation to the Left n [%] | Rotation to the Right n [%] | ||
| Unrestricted movement | 176 [88.0] | 175 [87.5] | 147 [73.5] | 147 [73.5] | ||
| Restricted movement | 21 [10.5] | 19 [9.5] | 48 [24] | 47 [23.5] | ||
| No movement | - | 1 [0.5] | - | 2 [1.0] | ||
| No observation | 3 [1.5] | 5 [2.5] | 5 [2.5] | 4 [2.0] | ||
| C2/C3 | ||||||
| Mobility Restrictions | Flexion n [%] | Extension n [%] | Lateral Flexion to the Left n [%] | Lateral Flexion to the Right n [%] | Rotation to the Left n [%] | Rotation to the Right n [%] |
| Unrestricted movement | 174 [87.0] | 178 [89.0] | 122 [61.0] | 140 [70.0] | 149 [74.5] | 156 [78.0] |
| Restricted movement | 21 [10.5] | 17 [8.5] | 70 [35.0] | 55 [27.5] | 44 [22.0] | 36 [18.0] |
| No movement | 1 [0.5] | 1 [0.5] | 3 [1.5] | 2 [1.0] | 2 [1.0] | 2 [1.0] |
| No observation | 4 [2.0] | 4 [2.0] | 5 [2.5] | 3 [1.5] | 5 [2.5] | 6 [3.0] |
| C3/C4 | ||||||
| Mobility Restrictions | Flexion n [%] | Extension n [%] | Lateral Flexion to the Left n [%] | Lateral Flexion to the Right n [%] | Rotation to the Left n [%] | Rotation to the Right n [%] |
| Unrestricted movement | 178 [89.0] | 184 [92.0] | 118 [59.0] | 139 [69.5] | 146 [73.0] | 154 [77.0] |
| Restricted movement | 18 [9.0] | 12 [6.0] | 72 [36.0] | 51 [25.5] | 48 [24.0] | 35 [17.5] |
| No movement | 1 [0.5] | 1 [0.5] | 4 [2.0] | 5 [2.5] | - | 3 [1.5] |
| No observation | 3 [1.5] | 3 [1.5] | 6 [3.0] | 5 [2.5] | 6 [3.0] | 8 [4.0] |
| C4/C5 | ||||||
| Mobility Restrictions | Flexion n [%] | Extension n [%] | Lateral Flexion to the Left n [%] | Lateral Flexion to the Right n [%] | Rotation to the Left n [%] | Rotation to the Right n [%] |
| Unrestricted movement | 180 [90.0] | 183 [91.5] | 135 [67.5] | 140 [70.0] | 158 [79.0] | 163 [81.5] |
| Restricted movement | 18 [9.0] | 11 [5.5] | 55 [27.5] | 50 [25] | 37 [18.5] | 30 [15.0] |
| No movement | 1 [0.5] | - | 5 [2.5] | 4 [2.0] | 2 [1.0] | 1 [0.5] |
| No observation | 1 [0.5] | 6 [3.0] | 5 [2.5] | 6 [3.0] | 3 [1.5] | 6 [3.0] |
| C5/C6 | ||||||
| Mobility Restrictions | Flexion n [%] | Extension n [%] | Lateral Flexion to the Left n [%] | Lateral Flexion to the Right n [%] | Rotation to the Left n [%] | Rotation to the Right n [%] |
| Unrestricted movement | 172 [86.0] | 178 [89.0] | 146 [73.0] | 140 [70.0] | 158 [79.0] | 161 [80.5] |
| Restricted movement | 21 [10.5] | 13 [6.5] | 43 [21.5] | 50 [25.0] | 36 [18.0] | 31 [15.5] |
| No movement | 3 [1.5] | 1 [0.5] | 3 [1.5] | 3 [1.5] | 3 [1.5] | 1 [0.5] |
| No observation | 4 [2.0] | 8 [4.0] | 8 [4.0] | 7 [3.5] | 3 [1.5] | 7 [3.5] |
| C6/C7 | ||||||
| Mobility Restrictions | Flexion n [%] | Extension n [%] | Lateral Flexion to the Left n [%] | Lateral Flexion to the Right n [%] | Rotation to the Left n [%] | Rotation to the Right n [%] |
| Unrestricted movement | 172 [86.0] | 153 [76.5] | 134 [67.0] | 140 [70.0] | 160 [80.0] | 160 [80.0] |
| Restricted movement | 26 [13.0] | 37 [18.5] | 56 [28.0] | 46 [23.0] | 32 [16.0] | 33 [16.5] |
| No movement | - | 6 [3.0] | 4 [2.0] | 6 [3.0] | 5 [2.5] | 2 [1.0] |
| No observation | 2 [1.0] | 4 [2.0] | 6 [3.0] | 8 [4.0] | 3 [1.5] | 5 [2.5] |
| C7/Th1 | ||||||
| Mobility Restrictions | Flexion n [%] | Extension n [%] | Lateral Flexion to the Left n [%] | Lateral Flexion to the Right n [%] | Rotation to the Left n [%] | Rotation to the Right n [%] |
| Unrestricted movement | 151 [75.5] | 108 [54.0] | 118 [59.0] | 128 [64.0] | 143 [71.5] | 142 [71.0] |
| Restricted movement | 40 [20.0] | 72 [36.0] | 62 [31.0] | 49 [24.5] | 45 [22.5] | 48 [24.0] |
| No movement | 3 [1.5] | 18 [9.0] | 11 [5.5] | 15 [7.5] | 9 [4.5] | 7 [3.5] |
| No observation | 6 [3.0] | 2 [1.0] | 9 [4.5] | 8 [4.0] | 3 [1.5] | 3 [1.5] |
| Th1/Th2 | ||||||
| Mobility Restrictions | Flexion n [%] | Extension n [%] | Lateral Flexion to the Left n [%] | Lateral Flexion to the Right n [%] | Rotation to the Left n [%] | Rotation to the Right n [%] |
| Unrestricted movement | 151 [75.5] | 128 [64.0] | 119 [59.5] | 130 [65.0] | 138 [69.0] | 143 [71.5] |
| Restricted movement | 39 [19.5] | 52 [26.0] | 54 [27.0] | 44 [22.0] | 43 [21.5] | 45 [22.5] |
| No movement | 5 [2.5] | 17 [8.5] | 14 [7.0] | 16 [8.0] | 15 [7.5] | 10 [5.0] |
| No observation | 5 [2.5] | 3 [1.5] | 13 [6.5] | 10 [5.0] | 4 [2.0] | 2 [1.0] |
| Th2/Th3 | ||||||
| Mobility Restrictions | Flexion n [%] | Extension n [%] | Lateral Flexion to the Left n [%] | Lateral Flexion to the Right n [%] | Rotation to the Left n [%] | Rotation to the Right n [%] |
| Unrestricted movement | 164 [82.0] | 138 [69.0] | 137 [68.5] | 135 [67.5] | 139 [69.5] | 146 [73.0] |
| Restricted movement | 24 [12.0] | 38 [19.0] | 32 [16.0] | 32 [16.0] | 40 [20.0] | 39 [19.5] |
| No movement | 6 [3.0] | 18 [9.0] | 24 [12.0] | 23 [11.5] | 16 [8.0] | 10 [5.0] |
| No observation | 6 [3.0] | 6 [3.0] | 7 [3.5] | 10 [5.0] | 5 [2.5] | 5 [2.5] |
| Th3/Th4 | ||||||
| Mobility Restrictions | Flexion n [%] | Extension n [%] | Lateral Flexion to the Left n [%] | Lateral Flexion to the Right n [%] | Rotation to the Left n [%] | Rotation to the Right n [%] |
| Unrestricted movement | 163 [81.5] | 147 [73.5] | 143 [71.5] | 146 [73.0] | 142 [71.0] | 146 [73.0] |
| Restricted movement | 18 [9.0] | 23 [11.5] | 15 [7.5] | 18 [9.0] | 25 [12.5] | 28 [14.0] |
| No movement | 11 [5.5] | 24 [12.0] | 30 [15.0] | 26 [13.0] | 28 [14.0] | 18 [9.0] |
| No observation | 8 [4.0] | 6 [3.0] | 12 [6.0] | 10 [5.0] | 5 [2.5] | 8 [4.0] |
| Segments | Mobility Disorders n [%] | No Mobility Disorders n [%] |
|---|---|---|
| C0/C1 | 77 [38.5] | 123 [61.5] |
| C1/C2 | 79 [39.5] | 121 [60.5] |
| C2/C3 | 124 [62.0] | 76 [38.0] |
| C3/C4 | 127 [63.5] | 73 [36.5] |
| C4/C5 | 108 [54.0] | 92 [46.0] |
| C5/C6 | 102 [51.0] | 98 [49.0] |
| C6/C7 | 101 [50.5] | 99 [49.5] |
| C7/Th1 | 143 [71.5] | 57 [28.5] |
| Th1/Th2 | 120 [60.0] | 80 [40.0] |
| Th2/Th3 | 83 [41.5] | 117 [58.5] |
| Th3/Th4 | 61 [30.5] | 139 [69.5] |
| Pair of Variables | n | r | R2 (%) | p |
|---|---|---|---|---|
| Disturbed segments & age | 200 | 0.14 | 2.02 | 0.04 |
| Upper part—disturbed segments & age | 200 | 0.06 | 0.34 | 0.41 |
| Middle part—disturbed segments & age | 200 | 0.160 | 2.58 | 0.02 |
| Lower part—disturbed segments & age | 200 | 0.11 | 1.15 | 0.13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Figas, G.; Kostka, J.; Pikala, M.; Kujawa, J.E.; Adamczewski, T. Analysis of Clinical Pattern of Musculoskeletal Disorders in the Cervical and Cervico—Thoracic Regions of the Spine. J. Clin. Med. 2024, 13, 840. https://doi.org/10.3390/jcm13030840
Figas G, Kostka J, Pikala M, Kujawa JE, Adamczewski T. Analysis of Clinical Pattern of Musculoskeletal Disorders in the Cervical and Cervico—Thoracic Regions of the Spine. Journal of Clinical Medicine. 2024; 13(3):840. https://doi.org/10.3390/jcm13030840
Chicago/Turabian StyleFigas, Gabriela, Joanna Kostka, Małgorzata Pikala, Jolanta Ewa Kujawa, and Tomasz Adamczewski. 2024. "Analysis of Clinical Pattern of Musculoskeletal Disorders in the Cervical and Cervico—Thoracic Regions of the Spine" Journal of Clinical Medicine 13, no. 3: 840. https://doi.org/10.3390/jcm13030840
APA StyleFigas, G., Kostka, J., Pikala, M., Kujawa, J. E., & Adamczewski, T. (2024). Analysis of Clinical Pattern of Musculoskeletal Disorders in the Cervical and Cervico—Thoracic Regions of the Spine. Journal of Clinical Medicine, 13(3), 840. https://doi.org/10.3390/jcm13030840