
Secondary Sarcopenia and Spinal Cord Injury: Clinical Associations and Health Outcomes

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion/Exclusion Criteria
2.3. Study Tools
- -
- Group S-SCI, which included 66 patients with SCI and ALM above the cut-off values (sarcopenia group).
- -
- Group NS-SCI, which included 70 patients with SCI and ALM below the cut-off values (without sarcopenia).
2.4. Sample Size
2.5. Statistical Analysis
2.6. Study Hypotheses
3. Results
Sample Characteristics
4. Discussion
4.1. Strengths and Limitations of the Study
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moga, T.D.; Nistor-Cseppento, C.D.; Bungau, S.G.; Tit, D.M.; Sabau, A.M.; Behl, T.; Nechifor, A.C.; Bungau, A.F.; Negrut, N. The Effects of the Catabolic Crisis on Patients Prolonged Immobility after COVID-19 Infection. Medicina 2022, 58, 828. [Google Scholar] [CrossRef]
- Coletta, G.; Phillips, S.M. An elusive consensus definition of sarcopenia impedes research and clinical treatment: A narrative review. Ageing Res. Rev. 2023, 86, 101883. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, I.H. Sarcopenia: Origins and clinical relevance. Clin. Geriatr. Med. 2011, 27, 337–339. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Larsson, S.C. Epidemiology of sarcopenia: Prevalence, risk factors, and consequences. Metabolism 2023, 144, 155533. [Google Scholar] [CrossRef] [PubMed]
- Cevei, M.; Onofrei, R.R.; Gherle, A.; Gug, C.; Stoicanescu, D. Rehabilitation of Post-COVID-19 Musculoskeletal Sequelae in Geriatric Patients: A Case Series Study. Int. J. Environ. Res. Public Health 2022, 19, 15350. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Dionyssiotis, Y.; Skarantavos, G.; Petropoulou, K.; Galanos, A.; Rapidi, C.A.; Lyritis, G.P. Application of current sarcopenia definitions in spinal cord injury. J. Musculoskelet. Neuronal Interact. 2019, 19, 21–29. [Google Scholar] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Polito, A.; Barnaba, L.; Ciarapica, D.; Azzini, E. Osteosarcopenia: A Narrative Review on Clinical Studies. Int. J. Mol. Sci. 2022, 23, 5591. [Google Scholar] [CrossRef]
- Barbiellini Amidei, C.; Salmaso, L.; Bellio, S.; Saia, M. Epidemiology of traumatic spinal cord injury: A large population-based study. Spinal Cord. 2022, 60, 812–819. [Google Scholar] [CrossRef]
- Shackleton, C.; Evans, R.; Shamley, D.; West, S.; Albertus, Y. Effectiveness of over-ground robotic locomotor training in improving walking performance, cardiovascular demands, secondary complications and user-satisfaction in individuals with spinal cord injuries: A systematic review. J. Rehabil. Med. 2019, 51, 723–733. [Google Scholar] [CrossRef]
- Gorgey, A.S.; Dudley, G.A. Skeletal muscle atrophy and increased intramuscular fat after incomplete spinal cord injury. Spinal Cord. 2007, 45, 304–309. [Google Scholar] [CrossRef]
- Nistor-Cseppento, C.D.; Gherle, A.; Negrut, N.; Bungau, S.G.; Sabau, A.M.; Radu, A.F.; Bungau, A.F.; Tit, D.M.; Uivaraseanu, B.; Ghitea, T.C.; et al. The Outcomes of Robotic Rehabilitation Assisted Devices Following Spinal Cord Injury and the Prevention of Secondary Associated Complications. Medicina 2022, 58, 1447. [Google Scholar] [CrossRef]
- Kim, T.N.; Choi, K.M. Sarcopenia: Definition, epidemiology, and pathophysiology. J. Bone Metab. 2013, 20, 1–10. [Google Scholar] [CrossRef]
- Roberts, T.T.; Leonard, G.R.; Cepela, D.J. Classifications In Brief: American Spinal Injury Association (ASIA) Impairment Scale. Clin. Orthop. Relat. Res. 2017, 475, 1499–1504. [Google Scholar] [CrossRef]
- Meseguer-Henarejos, A.B.; Sánchez-Meca, J.; López-Pina, J.A.; Carles-Hernández, R. Inter- and intra-rater reliability of the Modified Ashworth Scale: A systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2018, 54, 576–590. [Google Scholar] [CrossRef]
- Ashworth, B. Preliminary Trial of Carisoprodol in Multiple Sclerosis. Practitioner 1964, 192, 540–542. [Google Scholar] [PubMed]
- Ansari, N.N.; Naghdi, S.; Arab, T.K.; Jalaie, S. The interrater and intrarater reliability of the Modified Ashworth Scale in the assessment of muscle spasticity: Limb and muscle group effect. NeuroRehabilitation 2008, 23, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Harvey, N.C.; Orwoll, E.; Kwok, T.; Karlsson, M.K.; Rosengren, B.E.; Ribom, E.; Cauley, J.A.; Cawthon, P.M.; Ensrud, K.; Liu, E.; et al. Sarcopenia Definitions as Predictors of Fracture Risk Independent of FRAX. J. Bone Miner. Res. 2021, 36, 1235–1244. [Google Scholar] [CrossRef]
- Bagur, A.; Vega, E.; Mautalen, C. Discrimination of total body bone mineral density measured by dexa in vertebral osteoporosis. Calcif. Tissue Int. 1995, 56, 263–267. [Google Scholar] [CrossRef]
- Melton, L.J.; Khosla, S.; Crowson, C.S.; O’Connor, M.K.; O’Fallon, W.M.; Riggs, B.L. Epidemiology of sarcopenia. J. Am. Geriatr. Soc. 2000, 48, 625–630. [Google Scholar] [CrossRef]
- Clynes, M.A.; Gregson, C.L.; Bruyère, O.; Cooper, C.; Dennison, E.M. Osteosarcopenia: Where osteoporosis and sarcopenia collide. Rheumatology 2021, 60, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.D.; Craven, B.C.; Thabane, L.; Laing, A.C.; Frank-Wilson, A.W.; Kontulainen, S.A.; Papaioannou, A.; Adachi, J.D.; Giangregorio, L.M. Lower-extremity muscle atrophy and fat infiltration after chronic spinal cord injury. J. Musculoskelet. Neuronal Interact. 2015, 15, 32–41. [Google Scholar] [PubMed]
- Xu, X.; Talifu, Z.; Zhang, C.J.; Gao, F.; Ke, H.; Pan, Y.Z.; Gong, H.; Du, H.Y.; Yu, Y.; Jing, Y.L.; et al. Mechanism of skeletal muscle atrophy after spinal cord injury: A narrative review. Front. Nutr. 2023, 10, 1099143. [Google Scholar] [CrossRef] [PubMed]
- Carda, S.; Cisari, C.; Invernizzi, M. Sarcopenia or muscle modifications in neurologic diseases: A lexical or patophysiological difference? Eur. J. Phys. Rehabil. Med. 2013, 49, 119–130. [Google Scholar]
- Moga, T.D.; Moga, I.; Sabau, M.; Nistor-Cseppento, C.D.; Iovanovici, D.C.; Cavalu, S.; Dogaru, B.G. Sarcopenia, a major clinical problem in old age, potential causes, clinical consequences and therapeutic possibilities. Balneo PRM Res. J. 2022, 13, 492. [Google Scholar] [CrossRef]
- Sirbu, E.; Onofrei, R.R.; Szasz, S.; Susan, M. Predictors of disability in patients with chronic low back pain. Arch. Med. Sci. 2023, 19, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Leone, G.E.; Shields, D.C.; Haque, A.; Banik, N.L. Rehabilitation: Neurogenic Bone Loss after Spinal Cord Injury. Biomedicines 2023, 11, 2581. [Google Scholar] [CrossRef] [PubMed]
- Sadowsky, C.L. Targeting Sarcopenia as an Objective Clinical Outcome in the Care of Children with Spinal Cord-Related Paralysis: A Clinician’s View. Children 2023, 10, 837. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Alizadeh, A.; Dyck, S.M.; Karimi-Abdolrezaee, S. Traumatic Spinal Cord Injury: An Overview of Pathophysiology, Models and Acute Injury Mechanisms. Front. Neurol. 2019, 10, 282. [Google Scholar] [CrossRef]
- Drasites, K.P.; Shams, R.; Zaman, V.; Matzelle, D.; Shields, D.C.; Garner, D.P.; Sole, C.J.; Haque, A.; Banik, N.L. Pathophysiology, Biomarkers, and Therapeutic Modalities Associated with Skeletal Muscle Loss Following Spinal Cord Injury. Brain Sci. 2020, 10, 933. [Google Scholar] [CrossRef]
- Ishimoto, R.; Mutsuzaki, H.; Shimizu, Y.; Kishimoto, H.; Takeuchi, R.; Hada, Y. Prevalence of Sarcopenic Obesity and Factors Influencing Body Composition in Persons with Spinal Cord Injury in Japan. Nutrients 2023, 15, 437. [Google Scholar] [CrossRef]
- Gater, D.R.; Farkas, G.J.; Tiozzo, E. Pathophysiology of Neurogenic Obesity After Spinal Cord Injury. Top. Spinal Cord. Inj. Rehabil. 2021, 27, 1–10. [Google Scholar] [CrossRef]
- Yeung, S.S.Y.; Reijnierse, E.M.; Pham, V.K.; Trappenburg, M.C.; Lim, W.K.; Meskers, C.G.M.; Maier, A.B. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 485–500. [Google Scholar] [CrossRef]
- Inglis, T.; Banaszek, D.; Rivers, C.S.; Kurban, D.; Evaniew, N.; Fallah, N.; Waheed, Z.; Christie, S.; Fox, R.; Thiong, J.M.; et al. In-Hospital Mortality for the Elderly with Acute Traumatic Spinal Cord Injury. J. Neurotrauma 2020, 37, 2332–2342. [Google Scholar] [CrossRef]
- Shafiee, G.; Keshtkar, A.; Soltani, A.; Ahadi, Z.; Larijani, B.; Heshmat, R. Prevalence of sarcopenia in the world: A systematic review and meta- analysis of general population studies. J. Diabetes Metab. Disord. 2017, 16, 21. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Park, S. Gender-Specific Risk Factors and Prevalence for Sarcopenia among Community-Dwelling Young-Old Adults. Int. J. Environ. Res. Public Health 2022, 19, 7232. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, J.; Ni, W.; Yuan, X.; Zhang, H.; Li, P.; Xu, J.; Zhao, Z. Sarcopenia in heart failure: A systematic review and meta-analysis. ESC Heart Fail. 2021, 8, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Park, Y.S.; Lee, K.; Youn, S.I.; Won, Y.; Min, S.H.; Ahn, S.H.; Park, D.J.; Kim, H.H. Prognostic significance of surgery-induced sarcopenia in the survival of gastric cancer patients: A sex-specific analysis. J. Cachexia Sarcopenia Muscle 2021, 12, 1897–1907. [Google Scholar] [CrossRef]
- Haizlip, K.M.; Harrison, B.C.; Leinwand, L.A. Sex-based differences in skeletal muscle kinetics and fiber-type composition. Physiology 2015, 30, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.J.; Liu, H.; Garcia, J.M. Sex Differences in Muscle Wasting. Adv. Exp. Med. Biol. 2017, 1043, 153–197. [Google Scholar] [CrossRef]
- Marzetti, E.; Calvani, R.; Tosato, M.; Cesari, M.; Di Bari, M.; Cherubini, A.; Collamati, A.; D’Angelo, E.; Pahor, M.; Bernabei, R.; et al. Sarcopenia: An overview. Aging Clin. Exp. Res. 2017, 29, 11–17. [Google Scholar] [CrossRef]
- Nishikawa, H.; Fukunishi, S.; Asai, A.; Yokohama, K.; Nishiguchi, S.; Higuchi, K. Pathophysiology and mechanisms of primary sarcopenia (Review). Int. J. Mol. Med. 2021, 48. [Google Scholar] [CrossRef]
- Wyndaele, M.; Wyndaele, J.J. Incidence, prevalence and epidemiology of spinal cord injury: What learns a worldwide literature survey? Spinal Cord 2006, 44, 523–529. [Google Scholar] [CrossRef]
- Tanaka, Y.; Miyagi, M.; Inoue, G.; Hori, Y.; Inage, K.; Murata, K.; Fujimaki, H.; Kuroda, A.; Yokozeki, Y.; Inoue, S.; et al. Muscle strength rather than appendicular skeletal muscle mass might affect spinal sagittal alignment, low back pain, and health-related quality of life. Sci. Rep. 2023, 13, 9894. [Google Scholar] [CrossRef] [PubMed]
- Supriya, R.; Singh, K.P.; Gao, Y.; Gu, Y.; Baker, J.S. Effect of Exercise on Secondary Sarcopenia: A Comprehensive Literature Review. Biology 2021, 11, 51. [Google Scholar] [CrossRef]
- Varacallo, M.; Davis, D.D.; Pizzutillo, P. Osteoporosis in Spinal Cord. In juries. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Verschueren, S.; Gielen, E.; O’Neill, T.W.; Pye, S.R.; Adams, J.E.; Ward, K.A.; Wu, F.C.; Szulc, P.; Laurent, M.; Claessens, F.; et al. Sarcopenia and its relationship with bone mineral density in middle-aged and elderly European men. Osteoporos. Int. 2013, 24, 87–98. [Google Scholar] [CrossRef]
- Yoshimura, N.; Muraki, S.; Oka, H.; Iidaka, T.; Kodama, R.; Kawaguchi, H.; Nakamura, K.; Tanaka, S.; Akune, T. Is osteoporosis a predictor for future sarcopenia or vice versa? Four-year observations between the second and third ROAD study surveys. Osteoporos. Int. 2017, 28, 189–199. [Google Scholar] [CrossRef]
- Mahitthiharn, K.; Kovindha, A.; Kaewchur, T.; Morse, L.R.; Pattanakuhar, S. Prevalence and influencing factors of spinal cord injury-related osteoporosis and fragility fractures in Thai people with chronic spinal cord injury: A cross-sectional, observational study. J. Spinal Cord. Med. 2023, 46, 458–465. [Google Scholar] [CrossRef]
- Li, S.; Gonzalez-Buonomo, J.; Ghuman, J.; Huang, X.; Malik, A.; Yozbatiran, N.; Magat, E.; Francisco, G.E.; Wu, H.; Frontera, W.R. Aging after stroke: How to define post-stroke sarcopenia and what are its risk factors? Eur. J. Phys. Rehabil. Med. 2022, 58, 683–692. [Google Scholar] [CrossRef] [PubMed]
- Pacifico, J.; Geerlings, M.A.J.; Reijnierse, E.M.; Phassouliotis, C.; Lim, W.K.; Maier, A.B. Prevalence of sarcopenia as a comorbid disease: A systematic review and meta-analysis. Exp. Gerontol. 2020, 131, 110801. [Google Scholar] [CrossRef] [PubMed]
- Burns, A.S.; Marino, R.J.; Kalsi-Ryan, S.; Middleton, J.W.; Tetreault, L.A.; Dettori, J.R.; Mihalovich, K.E.; Fehlings, M.G. Type and Timing of Rehabilitation Following Acute and Subacute Spinal Cord Injury: A Systematic Review. Glob. Spine J. 2017, 7, 175S–194S. [Google Scholar] [CrossRef] [PubMed]
- De Spiegeleer, A.; Beckwée, D.; Bautmans, I.; Petrovic, M.; Sarcopenia Guidelines Development Group of the Belgian Society of Geriatrics. Pharmacological Interventions to Improve Muscle Mass, Muscle Strength and Physical Performance in Older People: An Umbrella Review of Systematic Reviews and Meta-analyses. Drugs Aging 2018, 35, 719–734. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Jun, H.S. Role of Myokines in Regulating Skeletal Muscle Mass and Function. Front. Physiol. 2019, 10, 42. [Google Scholar] [CrossRef]
- McClung, J.M.; Davis, J.M.; Wilson, M.A.; Goldsmith, E.C.; Carson, J.A. Estrogen status and skeletal muscle recovery from disuse atrophy. J. Appl. Physiol. 2006, 100, 2012–2023. [Google Scholar] [CrossRef]
- Kaur, J.; Ghosh, S.; Singh, P.; Dwivedi, A.K.; Sahani, A.K.; Sinha, J.K. Cervical Spinal Lesion, Completeness of Injury, Stress, and Depression Reduce the Efficiency of Mental Imagery in People With Spinal Cord Injury. Am. J. Phys. Med. Rehabil. 2022, 101, 513–519. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Group S-SCI | Group NS-SCI | p-Value | SS/NS |
|---|---|---|---|---|
| ALM-value, M, SD | 0.49 ± 0.042 | 0.65 ± 0.099 | - | - |
| Patients N (%) | 66 (48.529) | 70 (51.471) | - | - |
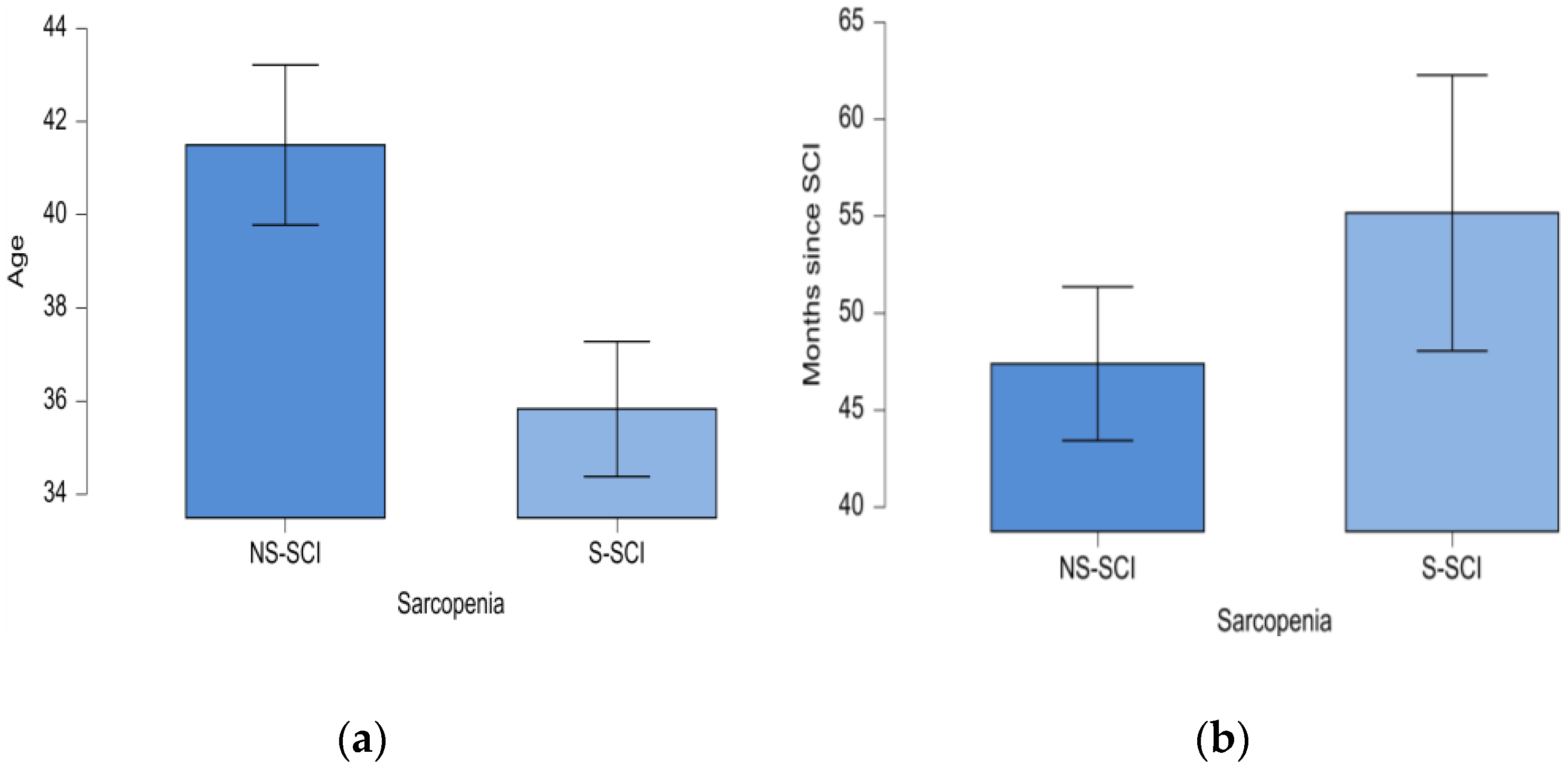
| Age, M, SD (years) | 35.83 ± 11.75 | 41.50 ± 14.36 | 0.013 * | SS |
| Female, N (%) | 18 (75.00) | 6 (25.00) | 0.014 ** | SS |
| Male, N (%) | 48 (42.86) | 64 (57.14) | 0.131 ** | NS |
| Number of months since SCI (M, SD) | 55.17 ± 57.77 | 47.40 ± 33.17 | 0.620 *** | NS |
| Neurological level of injury | ||||
| Level Cervical, N (%) | 27 (52.94) | 24 (47.06) | 0.674 ** | NS |
| Level Thoracal, N (%) | 33 (47.14) | 37 (52.85) | 0.633 ** | NS |
| Level Lumbar, N (%) | 6 (40) | 9 (60) | 0.439 ** | NS |
| AIS Scale | ||||
| Grade A, N (%) | 29 (55.77) | 23 (44.23) | 0.405 ** | NS |
| Grade B, N (%) | 23 (58.97) | 16 (41.02) | 0.262 ** | NS |
| Grade C, N (%) | 8 (28.57) | 20 (71.43) | 0.023 ** | NS |
| Grade D, N (%) | 6 (35.29) | 11 (64.70) | 0.225 ** | NS |
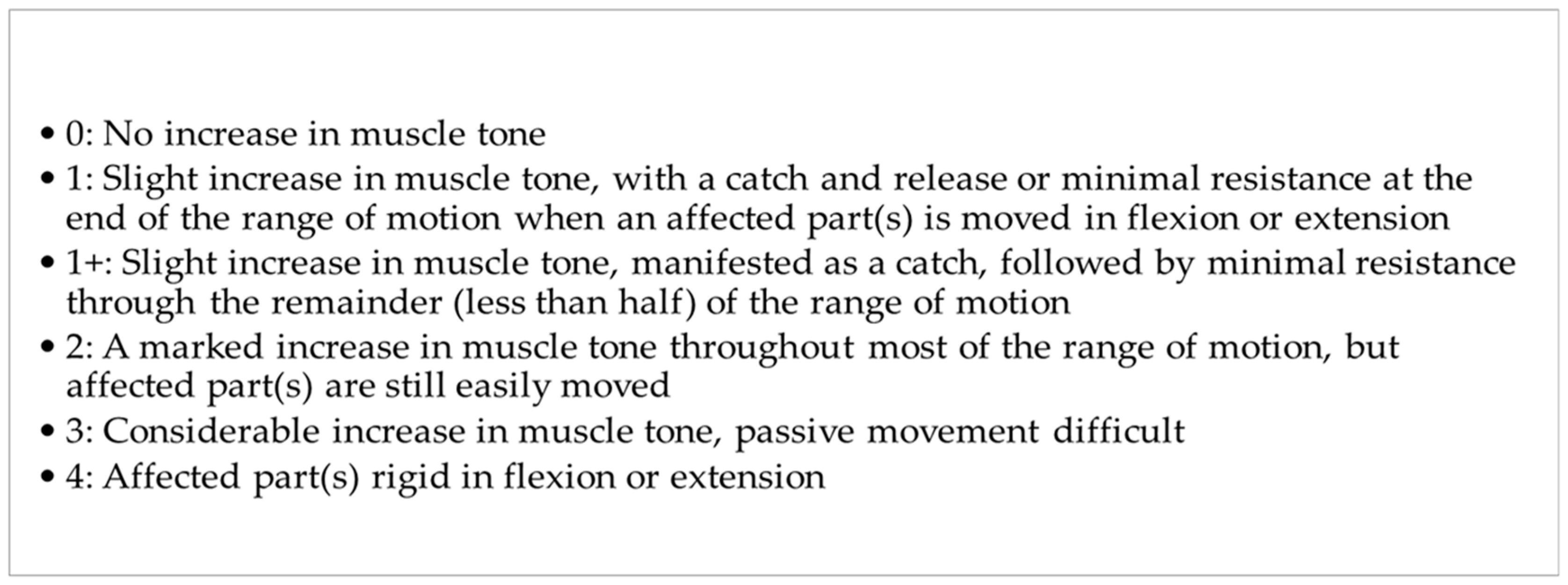
| Modified Ashworth Scale | ||||
| Score 0, N (%) | 23 (69.69) | 10 (30.30) | 0.024 ** | NS |
| Score 1, N (%) | 9 (42.85) | 12 (57.14) | 0.513 ** | NS |
| Score 2, N (%) | 17 (41.46) | 24 (58.53) | 0.274 ** | NS |
| Score 3, N (%) | 11 (40.74) | 16 (59.25) | 0.336 ** | NS |
| Score 4, N (%) | 6 (42.85) | 8(57.14) | 0.583 ** | NS |
| Comorbidities (M, SD) | 2.667 ± 1.522 | 2.086 ± 1.164 | 0.028 ** | SS |
| Immobilization Osteoporosis, Z-score | ||||
| Lumbar M, SD | −1.318 ± 1.182 | −1.280 ± 0.976 | - | |
| Right hip M, SD | −1.948 ± 0.945 | −1.444 ± 1.454 | - | |
| Left hip M, SD | −1.802 ± 1.330 | −1.467 ± 1.233 | - |
| Region Z-Score | Group | M ± SD | MIN | MAX |
|---|---|---|---|---|
| Lumbar Z-score | Group NS-SCI | −1.280 ± 0.976 | −3.500 | 1.400 |
| Group S-SCI | −1.318 ± 1.182 | −4.600 | 1.900 | |
| Right hip Z-score | Group NS-SCI | −1.444 ± 1.454 | −3.700 | 4.400 |
| Group S-SCI | −1.948 ± 0.945 | −3.900 | −0.100 | |
| Left hip Z-score | Group NS-SCI | −1.467 ± 1.233 | −3.700 | 2.800 |
| Group S-SCI | −1.802 ± 1.330 | −3.900 | 5.200 |
| Immobilization Osteoporosis | Group NS-SCI | Group S-SCI | p-Value ** |
|---|---|---|---|
| Yes, N (%) | 47 (48.45) | 50 (51.55) | 0.761 ** NS |
| No, N (%) | 23 (58.97) | 16(41.03) | 0.262 ** NS |
| Model | Deviance | AIC | BIC | df | Χ2 | p-Value ** |
|---|---|---|---|---|---|---|
| H₀ | 112.701 | 465.175 | 468.088 | 135 | ||
| H₁ | 107.858 | 462.332 | 468.157 | 134 | 4.843 | 0.028 |
| Coefficients | 95% Confidence Interval for B | ||||||
|---|---|---|---|---|---|---|---|
| B | Std. Error | Exp(B) | Z-Score | p-Value ** | Lower Bound | Upper Bound | |
| Intercept | 0.735 | 0.083 | 2.086 | 8.882 | <0.001 | 0.568 | 0.893 |
| Sarcopenia (Yes) | 0.246 | 0.112 | 1.279 | 2.195 | 0.028 | 0.027 | 0.466 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gherle, A.; Nistor-Cseppento, C.D.; Iovanovici, D.-C.; Cevei, I.R.; Cevei, M.L.; Vasileva, D.; Deac, S.; Stoicanescu, D. Secondary Sarcopenia and Spinal Cord Injury: Clinical Associations and Health Outcomes. J. Clin. Med. 2024, 13, 885. https://doi.org/10.3390/jcm13030885
Gherle A, Nistor-Cseppento CD, Iovanovici D-C, Cevei IR, Cevei ML, Vasileva D, Deac S, Stoicanescu D. Secondary Sarcopenia and Spinal Cord Injury: Clinical Associations and Health Outcomes. Journal of Clinical Medicine. 2024; 13(3):885. https://doi.org/10.3390/jcm13030885
Chicago/Turabian StyleGherle, Anamaria, Carmen Delia Nistor-Cseppento, Diana-Carina Iovanovici, Iulia Ruxandra Cevei, Mariana Lidia Cevei, Danche Vasileva, Stefania Deac, and Dorina Stoicanescu. 2024. "Secondary Sarcopenia and Spinal Cord Injury: Clinical Associations and Health Outcomes" Journal of Clinical Medicine 13, no. 3: 885. https://doi.org/10.3390/jcm13030885
APA StyleGherle, A., Nistor-Cseppento, C. D., Iovanovici, D. -C., Cevei, I. R., Cevei, M. L., Vasileva, D., Deac, S., & Stoicanescu, D. (2024). Secondary Sarcopenia and Spinal Cord Injury: Clinical Associations and Health Outcomes. Journal of Clinical Medicine, 13(3), 885. https://doi.org/10.3390/jcm13030885