
Unveiling Ocular Manifestations in Systemic Lupus Erythematosus
 ,
,  ,
,  and
and 
Abstract
:1. Introduction
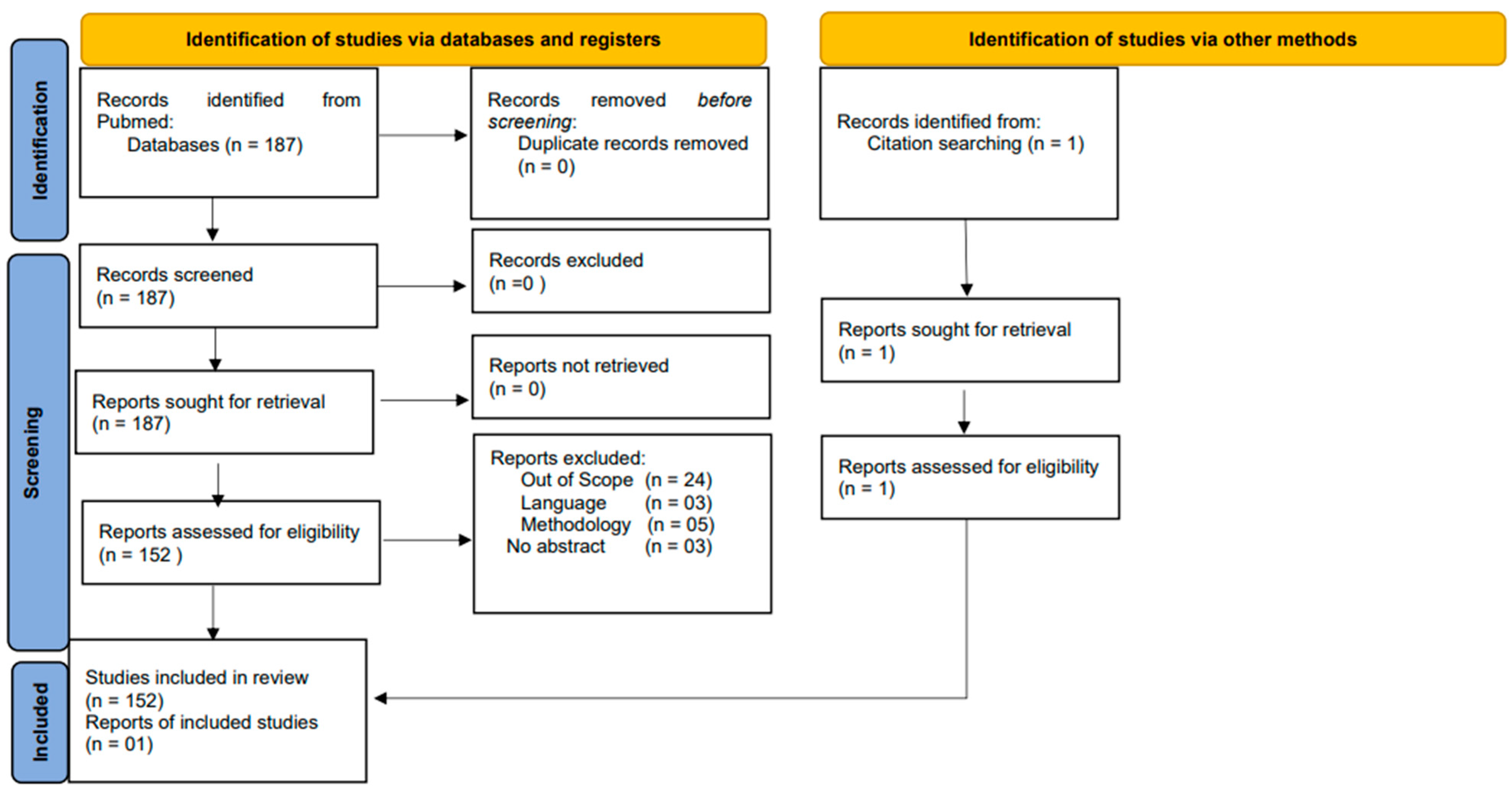
2. Methodology
3. Multidisciplinary Diagnosis
4. Diagnostic Criteria
5. Ocular Manifestations of SLE in the Oculovisual System
5.1. Anterior Segment
5.2. Cornea and Conjunctiva
5.3. Orbit, Extraocular Muscles and Refractive Shift
5.4. Uvea and Posterior Segment
6. Management and Treatment
7. Future Directions
8. Limitations
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lubon, W.; Lubon, M.; Kotyla, P.; Mrukwa-Kominek, E. Understanding Ocular Findings and Manifestations of Systemic Lupus Erythematosus: Update Review of the Literature. Int. J. Mol. Sci. 2022, 23, 12264. [Google Scholar] [CrossRef]
- Mohsenin, A.; Huang, J.J. Ocular manifestations of systemic inflammatory diseases. Conn. Med. 2012, 76, 533–544. [Google Scholar]
- Sonkodi, B.; Marsovszky, L.; Csorba, A.; Balog, A.; Kopper, B.; Nagy, Z.Z.; Resch, M.D. Neural Regeneration in Dry Eye Secondary to Systemic Lupus Erythematosus Is Also Disrupted like in Rheumatoid Arthritis, but in a Progressive Fashion. Int. J. Mol. Sci. 2023, 24, 10680. [Google Scholar] [CrossRef]
- Choudhary, M.M.; Hajj-Ali, R.A.; Lowder, C.Y. Gender and ocular manifestations of connective tissue diseases and systemic vasculitides. J. Ophthalmol. 2014, 2014, 403042. [Google Scholar] [CrossRef]
- Hayworth, J.L.; Turk, M.A.; Nevskaya, T.; Pope, J.E. The frequency of uveitis in patients with juvenile inflammatory rheumatic diseases. Jt. Bone Spine 2019, 86, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Androudi, S.; Dastiridou, A.; Symeonidis, C.; Kump, L.; Praidou, A.; Brazitikos, P.; Kurup, S.K. Retinal vasculitis in rheumatic diseases: An unseen burden. Clin. Rheumatol. 2013, 32, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Aldhefeery, N.; Alhadhood, N.; Alkadi, A. Bilateral Retinal Vasculitis as Initial Presentation of Systemic Lupus Erythematosus with Secondary Antiphospholipid Syndrome. Am. J. Case Rep. 2023, 24, e942085. [Google Scholar] [CrossRef] [PubMed]
- Bachtalia, K.; Frangia-Tsivou, K.; Patelis, A.; Palioura, S. A Rare Manifestation of Discoid Lupus Erythematosus Solely in the Lower Eyelid of a Young Man. Cureus 2023, 15, e47002. [Google Scholar] [CrossRef]
- Yang, W.; Lian, X.; Chen, H. The association of serum magnesium with infection in new-onset systemic lupus erythematosus patients. Lupus 2023, 32, 380–387. [Google Scholar] [CrossRef]
- El-Shereef, R.R.; Mohamed, A.S.; Hamdy, L. Ocular manifestation of systemic lupus erythematosus. Rheumatol. Int. 2013, 33, 1637–1642. [Google Scholar] [CrossRef]
- Shan, H.; Liu, W.; Li, Y.; Pang, K. The Autoimmune Rheumatic Disease Related Dry Eye and Its Association with Retinopathy. Biomolecules 2023, 13, 724. [Google Scholar] [CrossRef]
- Lee, B.W.; Kwon, E.J.; Park, Y.; Lee, J.J.; Ju, J.H.; Park, S.H.; Kwok, S.K. Predictors for future development of systemic lupus erythematosus in Korean Sjogren’s syndrome patients. Lupus 2023, 32, 1359–1368. [Google Scholar] [CrossRef]
- Itokawa, T.; Okajima, Y.; Iwashita, H.; Koji, K.; Suzuki, T.; Hori, Y. Association between mask-associated dry eye (MADE) and corneal sensations. Sci. Rep. 2023, 13, 1625. [Google Scholar] [CrossRef]
- Qin, G.; Chen, J.; Li, L.; Qi, Y.; Zhang, Q.; Wu, Y.; You, Y.; Yang, L.; Moore, J.; Xu, L.; et al. Relationship between ocular surface pain and corneal nerve loss in dry eye diabetics: A cross-sectional study in Shenyang, China. BMJ Open 2023, 13, e076932. [Google Scholar] [CrossRef]
- Wu, M.Y.; Wang, C.H.; Ng, C.Y.; Kuo, T.T.; Chang, Y.C.; Yang, C.H.; Lin, J.Y.; Ho, H.C.; Chung, W.H.; Chen, C.B. Periorbital erythema and swelling as a presenting sign of lupus erythematosus in tertiary referral centers and literature review. Lupus 2018, 27, 1828–1837. [Google Scholar] [CrossRef]
- Kopsachilis, N.; Tsaousis, K.T.; Tourtas, T.; Tsinopoulos, I.T. Severe chronic blepharitis and scarring ectropion associated with discoid lupus erythematosus. Clin. Exp. Optom. 2013, 96, 124–125. [Google Scholar] [CrossRef]
- Arrico, L.; Abbouda, A.; Abicca, I.; Malagola, R. Ocular Complications in Cutaneous Lupus Erythematosus: A Systematic Review with a Meta-Analysis of Reported Cases. J. Ophthalmol. 2015, 2015, 254260. [Google Scholar] [CrossRef]
- Kazemi, A.; McLaren, J.W.; Sit, A.J. Effect of Topical Phenylephrine 2.5% on Episcleral Venous Pressure in Normal Human Eyes. Invest. Ophthalmol. Vis. Sci. 2021, 62, 4. [Google Scholar] [CrossRef] [PubMed]
- Fustes, O.J.H. Orbital myositis in systemic lupus erythematosus. Eur. J. Rheumatol. 2021, 8, 180. [Google Scholar] [CrossRef] [PubMed]
- Vodopivec, I.; Lobo, A.M.; Prasad, S. Ocular inflammation in neurorheumatic disease. Semin. Neurol. 2014, 34, 444–457. [Google Scholar] [PubMed]
- Tseng, C.H.; Tai, Y.H.; Hong, C.T.; Dai, Y.X.; Chen, T.J.; Cherng, Y.G.; Lai, S.C. Systemic Lupus Erythematosus and Risk of Dry Eye Disease and Corneal Surface Damage: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2023, 20, 3776. [Google Scholar] [CrossRef]
- Bitirgen, G.; Kucuk, A.; Ergun, M.C.; Baloglu, R.; Gharib, M.H.; Al Emadi, S.; Ponirakis, G.; Malik, R.A. Subclinical Corneal Nerve Fiber Damage and Immune Cell Activation in Systemic Lupus Erythematosus: A Corneal Confocal Microscopy Study. Transl. Vis. Sci. Technol. 2021, 10, 10. [Google Scholar] [CrossRef]
- Kukan, M.; Driban, M.; Vupparaboina, K.K.; Schwarz, S.; Kitay, A.M.; Rasheed, M.A.; Busch, C.; Barthelmes, D.; Chhablani, J.; Al-Sheikh, M. Structural Features of Patients with Drusen-like Deposits and Systemic Lupus Erythematosus. J. Clin. Med. 2022, 11, 6012. [Google Scholar] [CrossRef]
- Fujieda, Y.; Ninagawa, K.; Matsui, Y.; Kono, M.; Kamishima, T.; Iwasaki, N.; Atsumi, T. Non-tuberculosis Mycobacterium Tenosynovitis with Rice Bodies in a Patient with Systemic Lupus Erythematosus. Intern. Med. 2020, 59, 2317–2320. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Uribe-Reina, P.; Munoz-Ortiz, J.; Cifuentes-Gonzalez, C.; Reyes-Guanes, J.; Terreros-Dorado, J.P.; Zambrano-Romero, W.; Lopez-Rojas, C.; Mantilla-Sylvain, F.; Mantilla-Hernandez, R.D.; de-la-Torre, A. Ocular Manifestations in Colombian Patients with Systemic Rheumatologic Diseases. Clin. Ophthalmol. 2021, 15, 2787–2802. [Google Scholar] [CrossRef] [PubMed]
- Dammacco, R.; Procaccio, P.; Racanelli, V.; Vacca, A.; Dammacco, F. Ocular Involvement in Systemic Lupus Erythematosus: The Experience of Two Tertiary Referral Centers. Ocul. Immunol. Inflamm. 2018, 26, 1154–1165. [Google Scholar] [CrossRef]
- Dammacco, R. Systemic lupus erythematosus and ocular involvement: An overview. Clin. Exp. Med. 2018, 18, 135–149. [Google Scholar] [CrossRef]
- Kotter, I.; Stubiger, N.; Deuter, C. Ocular involvement in rheumatoid arthritis, connective tissue diseases and vasculitis. Z. Rheumatol. 2017, 76, 673–681. [Google Scholar]
- Domngang Noche, C.; Kagmeni, G.; Dohvoma, V.; Bella, A.L.; Ebana Mvogo, C.; Singwe-Ngandeu, M. Ophthalmic Manifestations in Chronic Inflammatory Rheumatic Diseases at a Referral Hospital of Yaounde, Cameroon. Ocul. Immunol. Inflamm. 2018, 26, 259–264. [Google Scholar] [CrossRef]
- Sharma, S.K.; Sharma, A.L.; Mahajan, V.K. Ophthalmic manifestations in patients with collagen vascular disorders: A hospital-based retrospective observational study. Int. Ophthalmol. 2021, 41, 2765–2775. [Google Scholar] [CrossRef] [PubMed]
- Sitaula, R.; Shah, D.N.; Singh, D. The spectrum of ocular involvement in systemic lupus erythematosus in a tertiary eye care center in Nepal. Ocul. Immunol. Inflamm. 2011, 19, 422–425. [Google Scholar] [CrossRef] [PubMed]
- Kucukkomurcu, E.; Unal, A.U.; Esen, F.; Ozen, G.; Direskeneli, H.; Kazokoglu, H. Ocular Posterior Segment Involvement in Patients with Antiphospholipid Syndrome and Systemic Lupus Erythematosus. Ocul. Immunol. Inflamm. 2020, 28, 86–91. [Google Scholar] [CrossRef]
- Akhlaghi, M.; Abtahi-Naeini, B.; Pourazizi, M. Acute vision loss in systemic lupus erythematosus: Bilateral combined retinal artery and vein occlusion as a catastrophic form of clinical flare. Lupus 2018, 27, 1023–1026. [Google Scholar] [CrossRef] [PubMed]
- Hasanreisoglu, M.; Gulpinar Ikiz, G.D.; Kucuk, H.; Varan, O.; Ozdek, S. Acute lupus choroidopathy: Multimodal imaging and differential diagnosis from central serous chorioretinopathy. Int. Ophthalmol. 2018, 38, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Ru, L.; Xu, J.; Lin, Z.; Cao, L.; Zhang, L. Analysis of choroidal thickness in juvenile systemic lupus erythematosus and its correlation with laboratory tests. BMC Ophthalmol. 2023, 23, 148. [Google Scholar] [CrossRef]
- Conigliaro, P.; Cesareo, M.; Chimenti, M.S.; Triggianese, P.; Canofari, C.; Barbato, C.; Giannini, C.; Salandri, A.G.; Nucci, C.; Perricone, R. Take a look at the eyes in Systemic Lupus Erythematosus: A novel point of view. Autoimmun. Rev. 2019, 18, 247–254. [Google Scholar] [CrossRef]
- Fouad, S.A.; Esmat Mahmoud Ali, S.M.; Rezk Alnaggar, A.R.L.; Mahfouz, S.; Essam, M.; El-Gendy, H. Structural Retinal Assessment Using Optical Coherence Tomography and Fundus Fluorescein Angiography in Systemic Lupus Erythematosus Patients. J. Clin. Rheumatol. 2021, 27, 34–39. [Google Scholar] [CrossRef]
- Lee, K.R.; Peng, L.Y.; Iqbal, T.B.; Subrayan, V. Role of Angiography in Systemic Lupus Erythematosus-Induced Choroiditis. Ocul. Immunol. Inflamm. 2018, 26, 1146–1149. [Google Scholar] [CrossRef]
- Mahendradas, P.; Vala, R.; Kawali, A.; Akkali, M.C.; Shetty, R. Adaptive Optics Imaging in Retinal Vasculitis. Ocul. Immunol. Inflamm. 2018, 26, 760–766. [Google Scholar] [CrossRef]
- Pisetsky, D.S.; Lipsky, P.E. New insights into the role of antinuclear antibodies in systemic lupus erythematosus. Nat. Rev. Rheumatol. 2020, 16, 565–579. [Google Scholar] [CrossRef]
- Lee, I.; Zickuhr, L.; Hassman, L. Update on ophthalmic manifestations of systemic lupus erythematosus: Pathogenesis and precision medicine. Curr. Opin. Ophthalmol. 2021, 32, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Mimier-Janczak, M.; Kaczmarek, D.; Janczak, D.; Kaczmarek, R. Optical Coherence Tomography Angiography as a New Tool for Evaluation of the Subclinical Retinal Involvement in Patients with Systemic Lupus Erythematosus-A Review. J. Clin. Med. 2021, 10, 2887. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Jin, Y.; Zhou, M.; Lei, B.; Huang, L.; Chen, S.; Xue, K. Quantitative evaluation of retinal and choroidal vascularity in systemic lupus erythematosus by SS-OCT/OCTA. Graefes Arch. Clin. Exp. Ophthalmol. 2023, 261, 3385–3393. [Google Scholar] [CrossRef] [PubMed]
- Mimier-Janczak, M.; Kaczmarek, D.; Proc, K.; Misiuk-Hojlo, M.; Kaczmarek, R. Evaluation of Subclinical Retinal Disease in Patients Affected by Systemic Lupus Erythematosus with No Evidence of Ocular Involvement-An Optical Coherence Tomography Angiography Original Study. J. Clin. Med. 2022, 11, 7417. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, A.S.; Alqahtani, W.; Hazzazi, M.A.; Alqahtani, A.S. The Application of Optical Coherence Tomography Angiography in a Patient with Systemic Lupus Erythematosus. Cureus 2022, 14, e23843. [Google Scholar] [CrossRef] [PubMed]
- Pichi, F.; Woodstock, E.; Hay, S.; Neri, P. Optical coherence tomography angiography findings in systemic lupus erythematosus patients with no ocular disease. Int. Ophthalmol. 2020, 40, 2111–2118. [Google Scholar] [CrossRef]
- Ulviye, Y.; Betul, T.; Nur, T.H.; Selda, C. Spectral domain optical coherence tomography for early detection of retinal alterations in patients using hydroxychloroquine. Indian. J. Ophthalmol. 2013, 61, 168–171. [Google Scholar] [CrossRef]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019, 71, 1400–1412. [Google Scholar] [CrossRef]
- Emad, Y.; Gheita, T.; Darweesh, H.; Klooster, P.; Gamal, R.; Fathi, H.; El-Shaarawy, N.; Gamil, M.; Hawass, M.; El-Refai, R.M.; et al. Antibodies to extractable nuclear antigens (ENAS) in systemic lupus erythematosus patients: Correlations with clinical manifestations and disease activity. Reumatismo 2018, 70, 85–91. [Google Scholar] [CrossRef]
- Kumar, Y.; Bhatia, A.; Minz, R.W. Antinuclear antibodies and their detection methods in diagnosis of connective tissue diseases: A journey revisited. Diagn. Pathol. 2009, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Nashi, R.A.; Shmerling, R.H. Antinuclear Antibody Testing for the Diagnosis of Systemic Lupus Erythematosus. Med. Clin. N. Am. 2021, 105, 387–396. [Google Scholar] [CrossRef]
- Wichainun, R.; Kasitanon, N.; Wangkaew, S.; Hongsongkiat, S.; Sukitawut, W.; Louthrenoo, W. Sensitivity and specificity of ANA and anti-dsDNA in the diagnosis of systemic lupus erythematosus: A comparison using control sera obtained from healthy individuals and patients with multiple medical problems. Asian Pac. J. Allergy Immunol. 2013, 31, 292–298. [Google Scholar] [CrossRef]
- Ahn, S.S.; Jung, S.M.; Yoo, J.; Lee, S.W.; Song, J.J.; Park, Y.B. Anti-Smith antibody is associated with disease activity in patients with new-onset systemic lupus erythematosus. Rheumatol. Int. 2019, 39, 1937–1944. [Google Scholar] [CrossRef]
- Leuchten, N.; Hoyer, A.; Brinks, R.; Schoels, M.; Schneider, M.; Smolen, J.; Johnson, S.R.; Daikh, D.; Dorner, T.; Aringer, M.; et al. Systemic Lupus Erythematosus Classification Criteria Steering, C., Performance of Antinuclear Antibodies for Classifying Systemic Lupus Erythematosus: A Systematic Literature Review and Meta-Regression of Diagnostic Data. Arthritis Care Res. 2018, 70, 428–438. [Google Scholar] [CrossRef]
- Lin, M.; Boonsopon, S.; Manhapra, A.; Zhao, T.; Foster, C.S. Elevated serum BAFF in patients with ocular cicatricial pemphigoid. Can. J. Ophthalmol. 2022. [Google Scholar] [CrossRef]
- Kobak, L.; Abrahamovych, O.; Abrahamovych, U.; Maksymuk, A.; Ivanochko, R. Diagnostic Value of Laboratory Markers of Syntropic Lesions of the Circulatory System Organs in Patients with Systemic Lupus Erythematosus. Georgian Med. News 2023, 340–341, 159–164. [Google Scholar]
- Yu, C.; Gershwin, M.E.; Chang, C. Diagnostic criteria for systemic lupus erythematosus: A critical review. J. Autoimmun. 2014, 48–49, 10–13. [Google Scholar] [CrossRef]
- Hochberg, M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef]
- Tan, E.M.; Cohen, A.S.; Fries, J.F.; Masi, A.T.; McShane, D.J.; Rothfield, N.F.; Schaller, J.G.; Talal, N.; Winchester, R.J. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982, 25, 1271–1277. [Google Scholar] [CrossRef]
- Edworthy, S.M.; Zatarain, E.; McShane, D.J.; Bloch, D.A. Analysis of the 1982 ARA lupus criteria data set by recursive partitioning methodology: New insights into the relative merit of individual criteria. J. Rheumatol. 1988, 15, 1493–1498. [Google Scholar]
- Figueroa-Parra, G.; Meade-Aguilar, J.A.; Hulshizer, C.A.; Gunderson, T.M.; Chamberlain, A.M.; Thanarajasingam, U.; Greenlund, K.J.; Barbour, K.E.; Crowson, C.S.; Duarte-Garcia, A. Multimorbidity in systemic lupus erythematosus in a population-based cohort: The lupus Midwest network. Rheumatology 2023. [Google Scholar] [CrossRef]
- Aringer, M.; Dorner, T.; Leuchten, N.; Johnson, S.R. Toward new criteria for systemic lupus erythematosus-a standpoint. Lupus 2016, 25, 805–811. [Google Scholar] [CrossRef]
- Ines, L.; Silva, C.; Galindo, M.; Lopez-Longo, F.J.; Terroso, G.; Romao, V.C.; Rua-Figueroa, I.; Santos, M.J.; Pego-Reigosa, J.M.; Nero, P.; et al. Rheumatic Diseases Registry of the Portuguese Society of Rheumatology; Registry of Systemic Lupus Erythematosus Patients of the Spanish Society of, R. Classification of Systemic Lupus Erythematosus: Systemic Lupus International Collaborating Clinics Versus American College of Rheumatology Criteria. A Comparative Study of 2055 Patients From a Real-Life, International Systemic Lupus Erythematosus Cohort. Arthritis Care Res. 2015, 67, 1180–1185. [Google Scholar]
- Igoe, A.; Merjanah, S.; Harley, I.T.W.; Clark, D.H.; Sun, C.; Kaufman, K.M.; Harley, J.B.; Kaelber, D.C.; Scofield, R.H. Association between systemic lupus erythematosus and myasthenia gravis: A population-based National Study. Clin. Immunol. 2023, 109810. [Google Scholar] [CrossRef]
- Gamal, S.M.; Fouad, N.; Yosry, N.; Badr, W.; Sobhy, N. Disease characteristics in patients with juvenile- and adult-onset systemic lupus erythematosus: A multi-center comparative study. Arch. Rheumatol. 2022, 37, 280–287. [Google Scholar] [CrossRef]
- Turk, M.A.; Hayworth, J.L.; Nevskaya, T.; Pope, J.E. Ocular Manifestations in Rheumatoid Arthritis, Connective Tissue Disease, and Vasculitis: A Systematic Review and Metaanalysis. J. Rheumatol. 2021, 48, 25–34. [Google Scholar] [CrossRef]
- Zanussi, J.T.; Zhao, J.; Wei, W.Q.; Karakoc, G.; Chung, C.P.; Feng, Q.; Olsen, N.J.; Stein, C.M.; Kawai, V.K. Clinical diagnoses associated with a positive antinuclear antibody test in patients with and without autoimmune disease. BMC Rheumatol. 2023, 7, 24. [Google Scholar] [CrossRef]
- Tesija Kuna, A.; Derek, L.; Drvar, V.; Kozmar, A.; Gugo, K. Assessment of antinuclear antibodies (ANA): National recommendations on behalf of the Croatian society of medical biochemistry and laboratory medicine. Biochem. Med. 2021, 31, 020502. [Google Scholar] [CrossRef] [PubMed]
- Im, J.H.; Chung, M.H.; Park, Y.K.; Kwon, H.Y.; Baek, J.H.; Lee, S.Y.; Lee, J.S. Antinuclear antibodies in infectious diseases. Infect. Dis. 2020, 52, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Dorronsoro, M.; Bronfen, S.; Alconcher, L.; Lucarelli, L. Bilateral neuroretinitis and membranous lupus nephritis: 2 infrequent manifestations in juvenile lupus. Arch. Soc. Esp. Oftalmol. 2023, 98, 175–179. [Google Scholar] [CrossRef]
- Mehta, K.; Gujjar, A.P.; Babu, K. Peripheral Ulcerative Keratitis in a Young Lady with Systemic Lupus Erythematosus Post Rituximab Infusion-A Case Report. Ocul. Immunol. Inflamm. 2022, 30, 1312–1314. [Google Scholar] [CrossRef]
- Rao, Q.; Ku, M.; Wan, Q. A case report of systemic lupus erythematosus combined with central serous chorioretinopathy treated with glucocorticoids. J. Int. Med. Res. 2023, 51, 3000605231163716. [Google Scholar] [CrossRef]
- Yilmaz Tugan, B.; Sonmez, H.E.; Sahin, N.; Yuksel, N. Analysis of Meibomian Glands in Juvenile Systemic Lupus Erythematosus Patients without Dry Eye Symptoms and Signs. Jpn. J. Ophthalmol. 2023, 67, 32–37. [Google Scholar] [CrossRef]
- Yilmaz Tugan, B.; Sonmez, H.E.; Yuksel, N.; Karabas, L. Subclinical Retinal Capillary Abnormalities in Juvenile Systemic Lupus Erythematosus without Ocular Involvement. Ocul. Immunol. Inflamm. 2023, 31, 576–584. [Google Scholar] [CrossRef]
- Zeng, J.; Wu, M.; Zhou, Y.; Zhu, M.; Liu, X. Neutrophil Extracellular Traps (NETs) in Ocular Diseases: An Update. Biomolecules 2022, 12, 1440. [Google Scholar] [CrossRef]
- Chen, C.; Wang, S.; Li, X. Acute Syphilitic Posterior Placoid Chorioretinitis Misdiagnosed as Systemic Lupus Erythematosus Associated Uveitis. Ocul. Immunol. Inflamm. 2020, 28, 1116–1124. [Google Scholar] [CrossRef]
- Pareek, S.; Mohta, A.; Mehta, R.D.; Prasad, V. Ocular Discoid Lupus Erythematosus: More Than what Meets the Eye. Indian Dermatol. Online J. 2023, 14, 399–401. [Google Scholar]
- Tazin, F.; Kumar, H.; Israr, M.A.; Go, C.C. Ocular Migraine with Amaurosis Fugax of the Left Eye: A Case Report. Cureus 2022, 14, e28272. [Google Scholar] [CrossRef]
- Hsu, C.S.; Hsu, C.W.; Lu, M.C.; Koo, M. Risks of ophthalmic disorders in patients with systemic lupus erythematosus—A secondary cohort analysis of population-based claims data. BMC Ophthalmol. 2020, 20, 96. [Google Scholar] [CrossRef]
- Sanabria, M.R.; Toledo-Lucho, S.C. Evaluation of a follow-up protocol for patients on chloroquine and hydroxychloroquine treatment. Arch. Soc. Esp. Oftalmol. 2016, 91, 10–14. [Google Scholar] [CrossRef]
- Yazici, A.T.; Kara, N.; Yuksel, K.; Altinkaynak, H.; Baz, O.; Bozkurt, E.; Demirok, A. The biomechanical properties of the cornea in patients with systemic lupus erythematosus. Eye 2011, 25, 1005–1009. [Google Scholar] [CrossRef]
- Zhang, B.; Shweikh, Y.; Khawaja, A.P.; Gallacher, J.; Bauermeister, S.; Foster, P.J.; Eye, U.K.; Vision, C. Associations with Corneal Hysteresis in a Population Cohort: Results from 96 010 UK Biobank Participants. Ophthalmology 2019, 126, 1500–1510. [Google Scholar] [CrossRef]
- Franco, A.M.M.; Medina, F.M.C.; Balbi, G.G.M.; Levy, R.A.; Signorelli, F. Ophthalmologic manifestations in primary antiphospholipid syndrome patients: A cross-sectional analysis of a primary antiphospholipid syndrome cohort (APS-Rio) and systematic review of the literature. Lupus 2020, 29, 1528–1543. [Google Scholar] [CrossRef]
- Papagiannuli, E.; Rhodes, B.; Wallace, G.R.; Gordon, C.; Murray, P.I.; Denniston, A.K. Systemic lupus erythematosus: An update for ophthalmologists. Surv. Ophthalmol. 2016, 61, 65–82. [Google Scholar] [CrossRef]
- Modrzejewska, M.; Michalak, A.; Szmigiel, O.; Ostanek, L.; Ronin-Walknowska, E.; Lubinski, W. Ocular manifestations in a newborn from a pregnancy complicated by an antiphospholipid syndrome—A case report. Ginekol. Pol. 2013, 84, 888–891. [Google Scholar] [CrossRef] [PubMed]
- Dossari, S.K.; Alkhars, A.Z.; Albaqshi, A.A.; AlHajri, H.M.; Alabdullah, Z.A.; Almuhnna, Z.A.; Almuhanna, B.A.; Aljanobi, M.A. Prevalence of Dry Eye Disease and Its Risk Factors Among the General Population of Saudi Arabia: A Cross-Sectional Survey. Cureus 2022, 14, e32552. [Google Scholar] [CrossRef] [PubMed]
- Palejwala, N.V.; Walia, H.S.; Yeh, S. Ocular manifestations of systemic lupus erythematosus: A review of the literature. Autoimmune Dis. 2012, 2012, 290898. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Gu, Z.; Liao, R.; Shuai, Z. Dry Eye Indexes Estimated by Keratograph 5M of Systemic Lupus Erythematosus Patients without Secondary Sjogren’s Syndrome Correlate with Lupus Activity. J. Ophthalmol. 2019, 2019, 8509089. [Google Scholar] [CrossRef] [PubMed]
- Resch, M.D.; Marsovszky, L.; Nemeth, J.; Bocskai, M.; Kovacs, L.; Balog, A. Dry eye and corneal langerhans cells in systemic lupus erythematosus. J. Ophthalmol. 2015, 2015, 543835. [Google Scholar] [CrossRef]
- Chan, T.C.Y.; Chow, S.S.W.; Wan, K.H.N.; Yuen, H.K.L. Update on the association between dry eye disease and meibomian gland dysfunction. Hong Kong Med. J. 2019, 25, 8–47. [Google Scholar] [CrossRef]
- Peng, X.; Lu, Y.; Wei, J.; Lin, T.; Lu, Q.; Liu, Q.; Ting, W.J. A cohort study of T helper 17 cell-related cytokine levels in tear samples of systemic lupus erythematosus and Sjogren’s syndrome patients with dry eye disease. Clin. Exp. Rheumatol. 2021, 39 (Suppl. S133), 159–165. [Google Scholar] [CrossRef] [PubMed]
- Shoughy, S.S.; Tabbara, K.F. Ocular findings in systemic lupus erythematosus. Saudi J. Ophthalmol. 2016, 30, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.H.; Kim, M.K.; Lee, H.J.; Lee, H.I.; Wee, W.R.; Lee, J.H. Interleukin-17 in various ocular surface inflammatory diseases. J. Korean Med. Sci. 2011, 26, 938–944. [Google Scholar] [CrossRef] [PubMed]
- Gu, Z.; Lu, Q.; Zhang, A.; Shuai, Z.W.; Liao, R. Analysis of Ocular Surface Characteristics and Incidence of Dry Eye Disease in Systemic Lupus Erythematosus Patients Without Secondary Sjogren’s Syndrome. Front. Med. 2022, 9, 833995. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ou, S.; Lin, S.; Qian, H.; Zhao, Z.; Zhang, M.; Li, S.; Liu, Y.; Shi, G. Meibomian gland alteration in patients with systemic lupus erythematosus. Lupus 2022, 31, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Zhang, H.; Wang, Z.; Gong, B.; Al-Ward, H.; Deng, Y.; Fan, O.; Wang, J.; Zhu, W.; Sun, Y.E. Exploring the shared molecular mechanisms between systemic lupus erythematosus and primary Sjogren’s syndrome based on integrated bioinformatics and single-cell RNA-seq analysis. Front. Immunol. 2023, 14, 1212330. [Google Scholar] [CrossRef] [PubMed]
- Nicolle, P.; Liang, H.; Reboussin, E.; Rabut, G.; Warcoin, E.; Brignole-Baudouin, F.; Melik-Parsadaniantz, S.; Baudouin, C.; Labbe, A.; Reaux-Le Goazigo, A. Proinflammatory Markers, Chemokines, and Enkephalin in Patients Suffering from Dry Eye Disease. Int. J. Mol. Sci. 2018, 19, 1221. [Google Scholar] [CrossRef] [PubMed]
- Zemba, M.; Ionescu, M.A.; Pirvulescu, R.A.; Dumitrescu, O.M.; Daniel-Constantin, B.; Radu, M.; Stamate, A.C.; Istrate, S. Biomarkers of ocular allergy and dry eye disease. Rom. J. Ophthalmol. 2023, 67, 250–259. [Google Scholar]
- De Paiva, C.S.; Chotikavanich, S.; Pangelinan, S.B.; Pitcher, J.D., 3rd; Fang, B.; Zheng, X.; Ma, P.; Farley, W.J.; Siemasko, K.F.; Niederkorn, J.Y.; et al. IL-17 disrupts corneal barrier following desiccating stress. Mucosal Immunol. 2009, 2, 243–253. [Google Scholar] [CrossRef]
- Chauhan, S.K.; El Annan, J.; Ecoiffier, T.; Goyal, S.; Zhang, Q.; Saban, D.R.; Dana, R. Autoimmunity in dry eye is due to resistance of Th17 to Treg suppression. J. Immunol. 2009, 182, 1247–1252. [Google Scholar] [CrossRef]
- Duru, N.; Altinkaynak, H.; Uysal, B.S.; Duru, Z.; Can, M.E.; Erten, S.; Yuksel, N.; Kalkan Akcay, E. Increased Tear Film Osmolarity in Systemic Lupus Erythematosus. Semin. Ophthalmol. 2017, 32, 582–587. [Google Scholar] [CrossRef]
- Guannan, H.; Long, S.; Xia, H.; Dong, W.; Shaozhen, Z. Clinical characterisation and cytological study of dry eye in patients with autoimmune disease. J. Pak. Med. Assoc. 2018, 68, 353–358. [Google Scholar]
- Halmay, O.; Ludwig, K. Bilateral Band-Shaped Deep Keratitis and Iridocyclitis in Systemic Lupus Erythematosus. Br. J. Ophthalmol. 1964, 48, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Ruusuvaara, P.; Setala, K. Keratoendotheliitis fugax hereditaria. A clinical and specular microscopic study of a family with dominant inflammatory corneal disease. Acta Ophthalmol. 1987, 65, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Messmer, E.M.; Foster, C.S. Vasculitic peripheral ulcerative keratitis. Surv. Ophthalmol. 1999, 43, 379–396. [Google Scholar] [CrossRef] [PubMed]
- Badakere, A.; Patil-Chhablani, P. Orbital Apex Syndrome: A Review. Eye Brain 2019, 11, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Mangan, M.S.; Sarici, A.M.; Yalcin, O.; Aydin, D.; Yegen, G.; Seyahi, E. Orbital Mass as the Only Presenting Sign with Overlapping Features of Lupus Erythematosus Panniculitis and Subcutaneous Panniculitis-Like T-Cell Lymphoma. Ocul. Immunol. Inflamm. 2023, 31, 717–720. [Google Scholar] [CrossRef] [PubMed]
- Stavrou, P.; Murray, P.I.; Batta, K.; Gordon, C. Acute ocular ischaemia and orbital inflammation associated with systemic lupus erythematosus. Br. J. Ophthalmol. 2002, 86, 474–475. [Google Scholar] [CrossRef]
- Alqahtani, E.; Albalawi, Y.; Altwaijri, N.A.; Alqahtani, L., Jr.; Alshail, S. An Orbital Pseudotumor Secondary to Systemic Lupus Erythematosus: A Case Report. Cureus 2023, 15, e44994. [Google Scholar] [CrossRef]
- Safari, S.; Weppelmann, T.A. Lupus-Induced Myopic Shift. Cureus 2022, 14, e22961. [Google Scholar] [CrossRef]
- Cruciani, F.; Anzidei, R.; Albanese, G. Acute Myopia: Could it be the presenting symptom of a rheumatic disease? A case report. Clin. Ter. 2011, 162, e63-6. [Google Scholar] [PubMed]
- Ohsie, L.H.; Murchison, A.P.; Wojno, T.H. Lupus erythematosus profundus masquerading as idiopathic orbital inflammatory syndrome. Orbit 2012, 31, 181–183. [Google Scholar] [CrossRef] [PubMed]
- Rangel, L.K.; Villa-Ruiz, C.; Lo, K.; Cobos, G.; Lo Sicco, K.; Vleugels, R.A.; Femia, A.N. Clinical Characteristics of Lupus Erythematosus Panniculitis/Profundus: A Retrospective Review of 61 Patients. JAMA Dermatol. 2020, 156, 1264–1266. [Google Scholar] [CrossRef] [PubMed]
- Barile-Fabris, L.; Hernandez-Cabrera, M.F.; Barragan-Garfias, J.A. Vasculitis in systemic lupus erythematosus. Curr. Rheumatol. Rep. 2014, 16, 440. [Google Scholar] [CrossRef] [PubMed]
- Paraskevi, V.V.; Aliki, V.I.; Antigone, P.; Zoi, T.; Anastasia, Z.K.; Alexandros, D.A. Orbital myositis in systemic lupus erythematosus: A case-based review. Rheumatol. Int. 2022, 42, 1453–1460. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, P.; Manno, R.L.; Miller, N.R. Bilateral sequential trochleitis as the presenting feature of systemic lupus erythematosus. J. Neuroophthalmol. 2013, 33, 74–76. [Google Scholar] [CrossRef]
- Pidro, A.; Dizdarevic, A.; Jovanovic, N.; Cerim, A.; Sacak, E.; Miokovic, A.P. Diagnostics and treatment of orbital myositis. Rom. J. Ophthalmol. 2022, 66, 173–177. [Google Scholar]
- Babu, K.; Nanda, S.; Hegde, P.; Rao, A.P.; Jois, R. Posterior segment involvement in systemic lupus erythematosus—A series from South India. Indian. J. Ophthalmol. 2023, 71, 1986–1993. [Google Scholar] [CrossRef]
- Joshi, U.; Afroz, S.; Ranka, S.; Mba, B. Bilateral central retinal artery occlusion from catastrophic antiphospholipid syndrome. BMJ Case Rep. 2018, 2018, bcr-2018-226463. [Google Scholar] [CrossRef]
- Dias-Santos, A.; Tavares Ferreira, J.; Pinheiro, S.; Cunha, J.P.; Alves, M.; Papoila, A.L.; Moraes-Fontes, M.F.; Proenca, R. Ocular involvement in systemic lupus erythematosus patients: A paradigm shift based on the experience of a tertiary referral center. Lupus 2020, 29, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Geamanu Panca, A.; Popa-Cherecheanu, A.; Marinescu, B.; Geamanu, C.D.; Voinea, L.M. Retinal toxicity associated with chronic exposure to hydroxychloroquine and its ocular screening. Review. J. Med. Life 2014, 7, 322–326. [Google Scholar] [PubMed]
- Kobak, S.; Deveci, H. Retinopathy due to antimalarial drugs in patients with connective tissue diseases: Are they so innocent? A single center retrospective study. Int. J. Rheum. Dis. 2010, 13, e11–e15. [Google Scholar] [CrossRef] [PubMed]
- Petris, C.K.; Almony, A. Ophthalmic manifestations of rheumatologic disease: Diagnosis and management. Mo. Med. 2012, 109, 53–58. [Google Scholar] [PubMed]
- Ostovan, V.R.; Ghorbani, A. Chorea and retinal vessel occlusion in a patient with systemic lupus erythematosus. Iran. J. Neurol. 2013, 12, 66–68. [Google Scholar] [PubMed]
- Chen, X.; Shi, X.; Li, J.; Wang, W.; Wang, C.; Cheng, Q.; Xie, Y.; Xue, J.; Du, Y. Bilateral central retinal artery occlusion as a presenting manifestation of systemic lupus erythematosus: A case-based review. Rheumatol. Int. 2023, 43, 1947–1956. [Google Scholar] [CrossRef] [PubMed]
- Wuthisiri, W.; Lai, Y.H.; Capasso, J.; Blidner, M.; Salz, D.; Kruger, E.; Levin, A.V. Autoimmune retinopathy associated with systemic lupus erythematosus: A diagnostic dilemma. Taiwan. J. Ophthalmol. 2017, 7, 172–176. [Google Scholar] [PubMed]
- Pelegrin, L.; Morato, M.; Araujo, O.; Figueras-Roca, M.; Zarranz-Ventura, J.; Adan, A.; Cervera, R.; Casaroli-Marano, R.P.; Budi, V.; Barrera-Lopez, L.; et al. Preclinical ocular changes in systemic lupus erythematosus patients by optical coherence tomography. Rheumatology 2023, 62, 2475–2482. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Aty, A.; Gupta, A.; Del Priore, L.; Kombo, N. Management of noninfectious scleritis. Ther. Adv. Ophthalmol. 2022, 14, 25158414211070879. [Google Scholar] [CrossRef]
- Leone, P.; Prete, M.; Malerba, E.; Bray, A.; Susca, N.; Ingravallo, G.; Racanelli, V. Lupus Vasculitis: An Overview. Biomedicines 2021, 9, 1626. [Google Scholar] [CrossRef]
- Foster, C.S. Ocular manifestations of the potentially lethal rheumatologic and vasculitic disorders. J. Fr. Ophtalmol. 2013, 36, 526–532. [Google Scholar] [CrossRef]
- Lin, M.; Anesi, S.D.; Chang, P.Y.; Eggenschwiler, L.; Manhapra, A.; Walsh, M.; Foster, C.S. Clinical features, visual outcome, and poor prognostic factors in occlusive retinal vasculitis. Can. J. Ophthalmol. 2022, 57, 207–213. [Google Scholar] [CrossRef]
- Manderson, A.P.; Botto, M.; Walport, M.J. The role of complement in the development of systemic lupus erythematosus. Annu. Rev. Immunol. 2004, 22, 431–456. [Google Scholar] [CrossRef]
- Khil, J.; Nguyen, T.M.; Troxell, M.L.; Zheng, S. Systemic Lupus Erythematosus and ANCA-Associated Vasculitis Overlap Syndrome: A Case Report. Kidney Med. 2022, 4, 100544. [Google Scholar] [CrossRef]
- Espinoza, G.M.; Desai, A.; Akduman, L. Ocular vasculitis. Curr. Rheumatol. Rep. 2013, 15, 355. [Google Scholar] [CrossRef]
- Manolova, I.; Dancheva, M.; Halacheva, K. Antineutrophil cytoplasmic antibodies in patients with systemic lupus erythematosus: Prevalence, antigen specificity, and clinical associations. Rheumatol. Int. 2001, 20, 197–204. [Google Scholar]
- Weiner, M.; Bjorneklett, R.; Hruskova, Z.; Mackinnon, B.; Poulton, C.J.; Sindelar, L.; Mohammad, A.J.; Eriksson, P.; Gesualdo, L.; Geetha, D.; et al. Proteinase-3 and myeloperoxidase serotype in relation to demographic factors and geographic distribution in anti-neutrophil cytoplasmic antibody-associated glomerulonephritis. Nephrol. Dial. Transplant. 2019, 34, 301–308. [Google Scholar] [CrossRef]
- Kronbichler, A.; Lee, K.H.; Denicolo, S.; Choi, D.; Lee, H.; Ahn, D.; Kim, K.H.; Lee, J.H.; Kim, H.; Hwang, M.; et al. Immunopathogenesis of ANCA-Associated Vasculitis. Int. J. Mol. Sci. 2020, 21, 7319. [Google Scholar] [CrossRef] [PubMed]
- Hilhorst, M.; van Paassen, P.; Tervaert, J.W.; Limburg Renal, R. Proteinase 3-ANCA Vasculitis versus Myeloperoxidase-ANCA Vasculitis. J. Am. Soc. Nephrol. 2015, 26, 2314–2327. [Google Scholar] [CrossRef] [PubMed]
- Belizna, C.; Duijvestijn, A.; Hamidou, M.; Tervaert, J.W. Antiendothelial cell antibodies in vasculitis and connective tissue disease. Ann. Rheum. Dis. 2006, 65, 1545–1550. [Google Scholar] [CrossRef] [PubMed]
- Cieslik, P.; Semik-Grabarczyk, E.; Hrycek, A.; Holecki, M. The impact of anti-endothelial cell antibodies (AECAs) on the development of blood vessel damage in patients with systemic lupus erythematosus: The preliminary study. Rheumatol. Int. 2022, 42, 791–801. [Google Scholar] [CrossRef]
- Gumede, N.; Khathi, A. The role of fibrinolysis in the development of prediabetes-associated coronary heart disease: A focus on the plasminogen activator inhibitor -1 and its potential use as a predictive marker in diet-induced prediabetes. Front. Nutr. 2023, 10, 1256427. [Google Scholar] [CrossRef]
- Menet, J.; Agrinier, N.; Dufrost, V.; Conart, J.B.; Wahl, D.; Duprez, K.A.; Zuily, S. Ophthalmologic manifestations in patients with antiphospholipid antibodies: Beware of iatrogenic complications. Lupus 2021, 30, 1799–1807. [Google Scholar] [CrossRef] [PubMed]
- Hysa, E.; Cutolo, C.A.; Gotelli, E.; Paolino, S.; Cimmino, M.A.; Pacini, G.; Pizzorni, C.; Sulli, A.; Smith, V.; Cutolo, M. Ocular microvascular damage in autoimmune rheumatic diseases: The pathophysiological role of the immune system. Autoimmun. Rev. 2021, 20, 102796. [Google Scholar] [CrossRef]
- Barth, T.; Helbig, H. Ischemic Choroidal Diseases. Klin. Monbl Augenheilkd. 2021, 238, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Kharel Sitaula, R.; Shah, D.N.; Singh, D. Role of lupus retinopathy in systemic lupus erythematosus. J. Ophthalmic Inflamm. Infect. 2016, 6, 15. [Google Scholar] [CrossRef]
- de Andrade, F.A.; Guimaraes Moreira Balbi, G.; Bortoloti de Azevedo, L.G.; Provenzano Sa, G.; Vieira de Moraes Junior, H.; Mendes Klumb, E.; Abramino Levy, R. Neuro-ophthalmologic manifestations in systemic lupus erythematosus. Lupus 2017, 26, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Konen, F.F.; Mohn, N.; Witte, T.; Schefzyk, M.; Wiestler, M.; Lovric, S.; Hufendiek, K.; Schwenkenbecher, P.; Suhs, K.W.; Friese, M.A.; et al. Treatment of autoimmunity: The impact of disease-modifying therapies in multiple sclerosis and comorbid autoimmune disorders. Autoimmun. Rev. 2023, 22, 103312. [Google Scholar] [CrossRef] [PubMed]
- Garal-Pantaler, E.; Schultze, M.; Georgiou, M.E.; Pignot, M.; Gairy, K.; Hunnicutt, J.N. Real-World Burden of Immunosuppressant-Treated Lupus Nephritis: A German Claims Database Analysis. Rheumatol. Ther. 2023, 11, 113–127. [Google Scholar] [CrossRef]
- Duxbury, B.; Combescure, C.; Chizzolini, C. Rituximab in systemic lupus erythematosus: An updated systematic review and meta-analysis. Lupus 2013, 22, 1489–1503. [Google Scholar] [CrossRef]
- Deaner, J.D.; Zeft, A.S.; Emami-Naeini, P.; Lowder, C.Y. Visual recovery and vascular reperfusion after vaso-occlusive retinopathy from anti-phospholipid syndrome associated with systemic lupus erythematosus. Am. J. Ophthalmol. Case Rep. 2020, 19, 100763. [Google Scholar] [CrossRef]
- Li, X.; Fei, J.; Lei, Z.; Liu, K.; Wu, J.; Meng, T.; Yu, J.; Li, J. Chloroquine impairs visual transduction via modulation of acid sensing ion channel 1a. Toxicol. Lett. 2014, 228, 200–206. [Google Scholar] [CrossRef]
- Abd Hamid, A.; Zakaria, N.; Masnon, N.A.; Muhammed, J.; Wan Hitam, W.H. Functional Visual Loss in a Young Patient with Systemic Lupus Erythematosus. Cureus 2021, 13, e20513. [Google Scholar] [CrossRef]
- Barbagallo, M.; Straumann, D.; Binaghi, E.; Schmick, A. A rare case of a wall-eyed bilateral internuclear ophthalmoplegia (WEBINO) syndrome in a patient with cutaneous lupus erythematosus after COVID-19 infection. J. Neurol. 2023, 270, 1224–1228. [Google Scholar] [CrossRef]
- Youssef, M.M.; El-Fayoumi, D.; Sidky, M.K.; Hegazy, A.I.; Marzouk, H.; Eltanamly, R.M. Value of Microperimetry in Detecting Early Retinal Toxicity of Hydroxychloroquine in Children with Juvenile Systemic Lupus Erythematosus. Ophthalmologica 2017, 237, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, K.; Kiri, H.; Tyagi, M. Frosted branch angiitis in systemic lupus erythematosus. Ann. Rheum. Dis. 2023. [Google Scholar] [CrossRef] [PubMed]
- Budoff, G.; Tsui, E. Systemic Lupus Erythematosus Presenting as Unilateral Frosted Branch Angiitis. Ophthalmology 2023, 130, 836. [Google Scholar] [CrossRef]
- Li, M.; Jin, Y.; He, J. Purtscher-like retinopathy associated with systemic lupus erythematosus treated with rituximab plus low-dose interleukin-2: A case report. Int. J. Rheum. Dis. 2023, 26, 1373–1376. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Soler, E.; Martinez-Rubio, C.; De Smet, M.D.; Udaondo, P.; Salom-Alonso, D. Systemic lupus erythematosus purtscher like retinopathy: Optical coherence tomography angiography assessment implications. Eur. J. Ophthalmol. 2023, 11206721231171705. [Google Scholar] [CrossRef]
- Prakash, S.; Gunderia, A.M.; Khadar, S.M.A. A rare simultaneous presentation of combined occlusion and optic neuritis in a lupus erythematosus patient with anti-phospholipid antibody syndrome. Lupus 2023, 32, 804–809. [Google Scholar] [CrossRef]
- Subasi, S.; Kucuk, K.D.; San, S.; Cefle, A.; Tokuc, E.O.; Balci, S.; Yazici, A. Macular and peripapillary vessel density alterations in a large series of patients with systemic lupus erythematosus without ocular involvement. Graefes Arch. Clin. Exp. Ophthalmol. 2022, 260, 3543–3552. [Google Scholar] [CrossRef] [PubMed]
- David, S.; Davidson, S.O.; Grigorian, R. Bilateral Lupus Chorioretinopathy in a Patient with Active Systemic Lupus Erythematosus. Cureus 2022, 14, e30081. [Google Scholar] [CrossRef]
- Alhassan, E.; Gendelman, H.K.; Sabha, M.M.; Hawkins-Holt, M.; Siaton, B.C. Bilateral Retinal Vasculitis as the First Presentation of Systemic Lupus Erythematosus. Am. J. Case Rep. 2021, 22, e930650. [Google Scholar] [CrossRef] [PubMed]
- Kuthyar, S.; Barnes, A.C.; Bhawal, J.; Christiansen, J.; Shantha, J.G.; Yeh, S. Systemic Lupus Erythematosus-associated Retinal Vasculitis Treated with Adalimumab. Ocul. Immunol. Inflamm. 2022, 30, 981–985. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Dong, F.T.; Chen, Y.X.; Wang, Q.; Dai, R.P.; Zhang, H. Systemic lupus erythematosus and antiphospholipid syndrome related retinal vasculitis mimicking ocular cysticercosis: A case report. Chin. Med. Sci. J. 2015, 30, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Guan, C.; Ye, Z.; Lu, Y. Unilateral branch retinal artery occlusion in a patient with systemic lupus erythematosus: A case report. Medicine 2022, 101, e29005. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Wang, Y.; Xia, Q.; Xu, T.; Han, T.; Cai, S.; Luo, S.L.; Wu, R.; Shao, Y. Retinal thickness and microvascular alterations in the diagnosis of systemic lupus erythematosus: A new approach. Quant. Imaging Med. Surg. 2022, 12, 823–837. [Google Scholar] [CrossRef]
- Shi, W.Q.; Han, T.; Liu, R.; Xia, Q.; Xu, T.; Wang, Y.; Cai, S.; Luo, S.L.; Shao, Y.; Wu, R. Retinal Microvasculature and Conjunctival Vessel Alterations in Patients with Systemic Lupus Erythematosus-An Optical Coherence Tomography Angiography Study. Front. Med. 2021, 8, 724283. [Google Scholar] [CrossRef]
- Lin, W.V.; Saumur, M.; Al-Mohtaseb, Z. Scleritis, keratitis, and orbital cellulitis: Isolated ocular manifestation of systemic lupus erythematosus. Lupus 2018, 27, 1985–1988. [Google Scholar] [CrossRef]
- Wang, L.; Yang, Y.; Jia, Y.; Miao, H.; Zhou, Y.S.; Zhang, X.Y. Clinical characteristics of 4 cases of scleritis associated with systemic lupus erythematosus. Beijing Da Xue Xue Bao Yi Xue Ban 2016, 48, 1081–1085. [Google Scholar]
- Braga, J.; Rothwell, R.; Oliveira, M.; Rodrigues, D.; Fonseca, S.; Varandas, R.; Ribeiro, L. Choroid thickness profile in patients with lupus nephritis. Lupus 2019, 28, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Agin, A.; Kadayifcilar, S.; Sonmez, H.E.; Baytaroglu, A.; Demir, S.; Sag, E.; Ozen, S.; Eldem, B. Evaluation of Choroidal Thickness, Choroidal Vascularity Index and Peripapillary Retinal Nerve Fiber Layer in Patients with Juvenile Systemic Lupus Erythematosus. Lupus 2019, 28, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Fischer, W.G.G.; Kae, T.O.; de Almeida, R.; de Oliveira Filho, U.L.; Vilela, M.A.P.; Araujo, D.B. Bilateral chorioretinopathy in child-onset systemic lupus erythematosus. Lupus 2017, 26, 1112–1114. [Google Scholar] [CrossRef] [PubMed]
- Invernizzi, A.; dell’Arti, L.; Leone, G.; Galimberti, D.; Garoli, E.; Moroni, G.; Santaniello, A.; Agarwal, A.; Viola, F. Drusen-like Deposits in Young Adults Diagnosed with Systemic Lupus Erythematosus. Am. J. Ophthalmol. 2017, 175, 68–76. [Google Scholar] [CrossRef]
- Kumar, J.; Chandrappa, D.; Sen, S.; Sivakumar, R. Retinopathy secondary to flare-up of systemic lupus erythematosus. Natl. Med. J. India 2023, 36, 26–28. [Google Scholar] [CrossRef]
- Monov, S.; Hristova, R.; Dacheva, R.; Toncheva, R.; Shumnalieva, R.; Shoumnalieva-Ivanova, V.; Monova, D. Acute necrotizing retinal vasculitis as onset of systemic lupus erythematosus: A case report. Medicine 2017, 96, e5754. [Google Scholar] [CrossRef]
- Park, K.R.; Seo, M.R.; Ryu, H.J.; Chi, M.J.; Baek, H.J.; Choi, H.J. Acquired enophthalmos with systemic lupus erythematosus. Lupus 2016, 25, 88–92. [Google Scholar] [CrossRef]
- Jeyachandran, D.; Natarajan, G.; Balasubramaniyan, T.; Thanigachalam, D. Rare Ocular Manifestations of Systemic Lupus Erythematosus--Two Case Reports. J. Assoc. Physicians India 2014, 62, 52–54. [Google Scholar]
- Hu, C.L.; Peng, K.L. Bilateral macular infarction as an ocular manifestation of systemic lupus erythematosus (SLE). Clin. Ophthalmol. 2014, 8, 1845–1848. [Google Scholar]
- Chin, Y.C.; Bhargava, M.; Khor, C.C.; Cheung, C.M.; Wong, T.Y. Polypoidal choroidal vasculopathy and systemic lupus erythematosus. Lupus 2014, 23, 319–322. [Google Scholar] [CrossRef]
- Baglio, V.; Gharbiya, M.; Balacco-Gabrieli, C.; Mascaro, T.; Gangemi, C.; Di Franco, M.; Pistolesi, V.; Morabito, S.; Pecci, G.; Pierucci, A. Choroidopathy in patients with systemic lupus erythematosus with or without nephropathy. J. Nephrol. 2011, 24, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Salazar, H.; Sadaka, A.; Berry, S.; Torres, P.; Lee, A.G. Nine syndrome in a patient with systemic lupus erythematosus. Can. J. Ophthalmol. 2018, 53, e52–e55. [Google Scholar] [CrossRef]
- Fraga, M.M.; Len, C.A.; dos Santos Finamor, L.P.; Matos, K.T.; Muccioli, C.; Hilario, M.O.; Terreri, M.T. Ocular changes due to the treatment of juvenile systemic lupus erythematosus. Rev. Bras. Reumatol. 2011, 51, 554–557. [Google Scholar] [CrossRef]
- Pan, Q.; Chen, J.; Guo, L.; Lu, X.; Liao, S.; Zhao, C.; Wang, S.; Liu, H. Mechanistic insights into environmental and genetic risk factors for systemic lupus erythematosus. Am. J. Transl. Res. 2019, 11, 1241–1254. [Google Scholar]
- Al-ghamdi, A.A. Eye and Rheumatology. In Skills in Rheumatology; Almoallim, H., Cheikh, M., Eds.; Springer: Singapore, 2021; pp. 419–428. [Google Scholar]
- Ameer, M.A.; Chaudhry, H.; Mushtaq, J.; Khan, O.S.; Babar, M.; Hashim, T.; Zeb, S.; Tariq, M.A.; Patlolla, S.R.; Ali, J.; et al. An Overview of Systemic Lupus Erythematosus (SLE) Pathogenesis, Classification, and Management. Cureus 2022, 14, e30330. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef]
- Smolen, J.S.; Landewe, R.; Breedveld, F.C.; Dougados, M.; Emery, P.; Gaujoux-Viala, C.; Gorter, S.; Knevel, R.; Nam, J.; Schoels, M.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs. Ann. Rheum. Dis. 2010, 69, 964–975. [Google Scholar] [CrossRef]
- Schallhorn, J.M.; Schallhorn, S.C.; Hettinger, K.A.; Venter, J.A.; Pelouskova, M.; Teenan, D.; Hannan, S.J. Outcomes and complications of excimer laser surgery in patients with collagen vascular and other immune-mediated inflammatory diseases. J. Cataract. Refract. Surg. 2016, 42, 1742–1752. [Google Scholar] [CrossRef]
- Jawahar, N.; Walker, J.K.; Murray, P.I.; Gordon, C.; Reynolds, J.A. Epidemiology of disease-activity related ophthalmological manifestations in Systemic Lupus Erythematosus: A systematic review. Lupus 2021, 30, 2191–2203. [Google Scholar] [CrossRef]
- Gladman, D.D.; Ibanez, D.; Urowitz, M.B. Systemic lupus erythematosus disease activity index 2000. J. Rheumatol. 2002, 29, 288–291. [Google Scholar]
- Arora, S.; Isenberg, D.A.; Castrejon, I. Measures of Adult Systemic Lupus Erythematosus: Disease Activity and Damage. Arthritis Care Res. 2020, 72 (Suppl. S10), 27–46. [Google Scholar] [CrossRef] [PubMed]
- Almaghlouth, I.; Almalag, H.M.; Alzuhair, H.; Alsaigh, R.; Bedaiwi, A.; Hassen, L.M.; Alzomia, S.; Alanazi, B.; Alabdulkareem, A.M.; Alahmari, S.; et al. Impact of telemedicine on disease activity assessment: A case-crossover study nested within a cohort of patients with systemic lupus erythematosus. Lupus 2023, 32, 1610–1618. [Google Scholar] [CrossRef]
- Aldarwesh, A.; Almustanyir, A.; Alhayan, D.; Alharthi, M.; Alblowi, M. Self-Efficacy of Saudi Patients with Autoimmune Diseases in Managing Hydroxychloroquine-Induced Ocular Complications: A Cross-Sectional Survey. Healthcare 2022, 10, 565. [Google Scholar] [CrossRef]
- Rabin, J.C.; Ramirez, K. Hydroxychloroquine Ocular Toxicity: Lessons Learned. J. Rheumatol. 2019, 46, 1640–1641. [Google Scholar] [CrossRef]
- Martin-Iglesias, D.; Artaraz, J.; Fonollosa, A.; Ugarte, A.; Arteagabeitia, A.; Ruiz-Irastorza, G. Evolution of retinal changes measured by optical coherence tomography in the assessment of hydroxychloroquine ocular safety in patients with systemic lupus erythematosus. Lupus 2019, 28, 555–559. [Google Scholar] [CrossRef]
- Salu, P.; Uvijls, A.; van den Brande, P.; Leroy, B.P. Normalization of generalized retinal function and progression of maculopathy after cessation of therapy in a case of severe hydroxychloroquine retinopathy with 19 years follow-up. Doc. Ophthalmol. 2010, 120, 251–264. [Google Scholar] [CrossRef] [PubMed]
- Pena-Vizcarra, O.R.; Zavala-Miranda, M.F.; Juarez-Cuevas, B.; Marquez-Macedo, S.E.; Hernandez-Andrade, A.; Nordmann-Gomes, A.; Perez-Arias, A.A.; Morales-Buenrostro, L.E.; Mejia-Vilet, J.M. Effect of antimalarials on clinical outcomes in lupus nephritis. Rheumatology 2023. [Google Scholar] [CrossRef]
- Moschos, M.M.; Nitoda, E.; Chatziralli, I.P.; Gatzioufas, Z.; Koutsandrea, C.; Kitsos, G. Assessment of hydroxychloroquine maculopathy after cessation of treatment: An optical coherence tomography and multifocal electroretinography study. Drug Des. Devel Ther. 2015, 9, 2993–2999. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimiadib, N.; Riazi-Esfahani, H.; Heidari, M.; Mahmoudi, A. Ocular flare-up in patients with systemic lupus erythematosus following discontinuation of hydroxychloroquine. Lupus 2020, 29, 987–992. [Google Scholar] [CrossRef]
- Porta, S.; Danza, A.; Arias Saavedra, M.; Carlomagno, A.; Goizueta, M.C.; Vivero, F.; Ruiz-Irastorza, G. Glucocorticoids in Systemic Lupus Erythematosus. Ten Questions and Some Issues. J. Clin. Med. 2020, 9, 2709. [Google Scholar] [CrossRef]
- Ponticelli, C.; Moroni, G. Hydroxychloroquine in systemic lupus erythematosus (SLE). Expert. Opin. Drug Saf. 2017, 16, 411–419. [Google Scholar] [CrossRef]
- Pego-Reigosa, J.M.; Cobo-Ibanez, T.; Calvo-Alen, J.; Loza-Santamaria, E.; Rahman, A.; Munoz-Fernandez, S.; Rua-Figueroa, I. Efficacy and safety of nonbiologic immunosuppressants in the treatment of nonrenal systemic lupus erythematosus: A systematic review. Arthritis Care Res. 2013, 65, 1775–1785. [Google Scholar] [CrossRef]
- Luijten, R.K.; Fritsch-Stork, R.D.; Bijlsma, J.W.; Derksen, R.H. The use of glucocorticoids in systemic lupus erythematosus. After 60 years still more an art than science. Autoimmun. Rev. 2013, 12, 617–628. [Google Scholar] [CrossRef]
- Shields, C.L.; Ramasubramanian, A.; Mellen, P.L.; Shields, J.A. Conjunctival squamous cell carcinoma arising in immunosuppressed patients (organ transplant, human immunodeficiency virus infection). Ophthalmology 2011, 118, 2133–2137.e1. [Google Scholar] [CrossRef]
- Arrico, L.; Abbouda, A.; Bianchi, S.; Malagola, R. Acute monolateral proptosis and orbital myositis in a patient with discoid lupus erythematosus: A case report. J. Med. Case Rep. 2014, 8, 375. [Google Scholar] [CrossRef]
- Chan, A.J.; Rai, A.S.; Lake, S. Orbital myositis in systemic lupus erythematosus: A case report and literature review. Eur. J. Rheumatol. 2020, 7, 135–137. [Google Scholar] [CrossRef]
- Tabbara, K.F.; Vera-Cristo, C.L. Sjogren syndrome. Curr. Opin. Ophthalmol. 2000, 11, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.T.W.; Lam, S.C.; Kwok, T.Y.T.; Yuen, H.K.L. Atypical mycobacterium infection following upper eyelid Muller’s muscle-conjunctival resection—Case report. Orbit 2023, 42, 437–440. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.L.; Bergem, H.O.; Gilboe, I.M.; Husby, G.; Axell, T. Oral and ocular sicca symptoms and findings are prevalent in systemic lupus erythematosus. J. Oral. Pathol. Med. 1999, 28, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Moscovici, B.K.; Holzchuh, R.; Chiacchio, B.B.; Santo, R.M.; Shimazaki, J.; Hida, R.Y. Clinical treatment of dry eye using 0.03% tacrolimus eye drops. Cornea 2012, 31, 945–949. [Google Scholar] [CrossRef] [PubMed]
- Bai, W.; Li, M.; Zhou, S.; Peng, L.; Zhao, J.; Tian, X.; Wang, Q.; Leng, X.; Zhang, S.; Wang, Y.; et al. Clinical efficacy of tacrolimus in systemic lupus erythematosus with various manifestations: A real-world study. China Med. J. 2022, 135, 2245–2247. [Google Scholar] [CrossRef]
- Cao, Y.; Zhang, W.; Wu, J.; Zhang, H.; Zhou, H. Peripheral Ulcerative Keratitis Associated with Autoimmune Disease: Pathogenesis and Treatment. J. Ophthalmol. 2017, 2017, 7298026. [Google Scholar] [CrossRef]
- Roldan, P.C.; Ratliff, M.; Snider, R.; Macias, L.; Rodriguez, R.; Sibbitt, W.; Roldan, C.A. Aortic Atherosclerosis in Systemic Lupus Erythematosus. Rheumatology 2014, (Suppl. S5), S5-006. [Google Scholar] [CrossRef]
- Sivaraj, R.R.; Durrani, O.M.; Denniston, A.K.; Murray, P.I.; Gordon, C. Ocular manifestations of systemic lupus erythematosus. Rheumatology 2007, 46, 1757–1762. [Google Scholar] [CrossRef] [PubMed]
- Nemet, A.Y.; Vinker, S.; Bahar, I.; Kaiserman, I. The association of keratoconus with immune disorders. Cornea 2010, 29, 1261–1264. [Google Scholar] [CrossRef]
- Simpson, R.G.; Moshirfar, M.; Edmonds, J.N.; Christiansen, S.M.; Behunin, N. Laser in situ keratomileusis in patients with collagen vascular disease: A review of the literature. Clin. Ophthalmol. 2012, 6, 1827–1837. [Google Scholar]
- Silpa-archa, S.; Lee, J.J.; Foster, C.S. Ocular manifestations in systemic lupus erythematosus. Br. J. Ophthalmol. 2016, 100, 135–141. [Google Scholar] [CrossRef]
- Davies, J.B.; Rao, P.K. Ocular manifestations of systemic lupus erythematosus. Curr. Opin. Ophthalmol. 2008, 19, 512–518. [Google Scholar] [CrossRef]
- Sainz de la Maza, M.; Jabbur, N.S.; Foster, C.S. Severity of scleritis and episcleritis. Ophthalmology 1994, 101, 389–396. [Google Scholar] [CrossRef]
- Gallagher, K.; Viswanathan, A.; Okhravi, N. Association of systemic lupus erythematosus with uveitis. JAMA Ophthalmol. 2015, 133, 1190–1193. [Google Scholar] [CrossRef] [PubMed]
- Zink, J.M.; Singh-Parikshak, R.; Johnson, C.S.; Zacks, D.N. Hypopyon uveitis associated with systemic lupus erythematosus and antiphospholipid antibody syndrome. Graefes Arch. Clin. Exp. Ophthalmol. 2005, 243, 386–388. [Google Scholar] [CrossRef]
- Ushiyama, O.; Ushiyama, K.; Koarada, S.; Tada, Y.; Suzuki, N.; Ohta, A.; Oono, S.; Nagasawa, K. Retinal disease in patients with systemic lupus erythematosus. Ann. Rheum. Dis. 2000, 59, 705–708. [Google Scholar] [CrossRef]
- Lacava, A.C. Ocular complications of chloroquine and derivatives therapy. Arq. Bras. Oftalmol. 2010, 73, 384–389. [Google Scholar] [CrossRef]
- Pedrosa, T.; Kupa, L.V.K.; Pasoto, S.G.; Aikawa, N.E.; Borba, E.F.; Duarte, N.J.; Leon, E.P.; Silva, C.A.; Bonfa, E. The influence of obesity on hydroxychloroquine blood levels in lupus nephritis patients. Lupus 2021, 30, 554–559. [Google Scholar] [CrossRef]
- Killian, M.; Colaone, F.; Haumont, P.; Nicco, C.; Cerles, O.; Chouzenoux, S.; Cathebras, P.; Rochereau, N.; Chanut, B.; Thomas, M.; et al. Therapeutic Potential of Anti-Interferon alpha Vaccination on SjS-Related Features in the MRL/lpr Autoimmune Mouse Model. Front. Immunol. 2021, 12, 666134. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors | Signs and Symptoms |
|---|---|
| Chauhan et al. [156], Budoff and Tsui [157] | Fronsted branch angiitis. |
| Li et al. [158], Garcia-Soler et al. [159] | Purtscher-like retinopathy |
| Prakash et al. [160] | Simultaneous occlusion of the central retinal artery and vein, and optic neuritis |
| Subasi et al. [161] | Changes in macular and peripapillary microvascular density |
| David et al. [162] | Chorioretinopathy |
| Alhassan et al. [163], Kuthyar et al. [164], Wu et al. [165] | Retinal vasculitis |
| Zhang et al. [166] | Unilateral branched retinal occlusion |
| Liu et al. [167], Shi et al. [168] | Retinal thickness and microvascular alterations |
| Lin et al. [169], Wang et al. [170] | Scleritis, keratitis, and orbital cellulitis |
| Braga et al. [171], Agin et al. [172] | Choroidal thickness alterations |
| Fischer et al. [173] | Child-onset chorioretinopathy |
| Invernizzi et al. [174] | Drusenoid retinopathy in young adult |
| Kumar et al. [175] | SLE flare up resulting in retinopathy |
| Monov et al. [176] | Acute necrotizing scleritis |
| Park et al. [177] | Acquired enophthalmos. |
| Jeyachandran et al. [178] | Optic neuropathy |
| Hu and Peng [179] | Macular infarction |
| Chin et al. [180] | Polypoidal choroidal vasculopathy |
| Baglio et al. [181] | Choroidopathy |
| Salazar et al. [182] | Nine syndromes |
| Fraga et al. [183] | A cohort of pediatric SLE patients were reported to have significant chloroquine-induced retinopathies and other ocular morbidities |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Musa, M.; Chukwuyem, E.; Ojo, O.M.; Topah, E.K.; Spadea, L.; Salati, C.; Gagliano, C.; Zeppieri, M. Unveiling Ocular Manifestations in Systemic Lupus Erythematosus. J. Clin. Med. 2024, 13, 1047. https://doi.org/10.3390/jcm13041047
Musa M, Chukwuyem E, Ojo OM, Topah EK, Spadea L, Salati C, Gagliano C, Zeppieri M. Unveiling Ocular Manifestations in Systemic Lupus Erythematosus. Journal of Clinical Medicine. 2024; 13(4):1047. https://doi.org/10.3390/jcm13041047
Chicago/Turabian StyleMusa, Mutali, Ekele Chukwuyem, Oluwasola Michael Ojo, Efioshiomoshi Kings Topah, Leopoldo Spadea, Carlo Salati, Caterina Gagliano, and Marco Zeppieri. 2024. "Unveiling Ocular Manifestations in Systemic Lupus Erythematosus" Journal of Clinical Medicine 13, no. 4: 1047. https://doi.org/10.3390/jcm13041047
APA StyleMusa, M., Chukwuyem, E., Ojo, O. M., Topah, E. K., Spadea, L., Salati, C., Gagliano, C., & Zeppieri, M. (2024). Unveiling Ocular Manifestations in Systemic Lupus Erythematosus. Journal of Clinical Medicine, 13(4), 1047. https://doi.org/10.3390/jcm13041047