Elevated LV Mass and LV Mass Index Sign on the Athlete’s ECG: Athletes’ Hearts are Prone to Ventricular Arrhythmia


Abstract
:1. Introduction
2. Materials and Method
2.1. Echocardiography
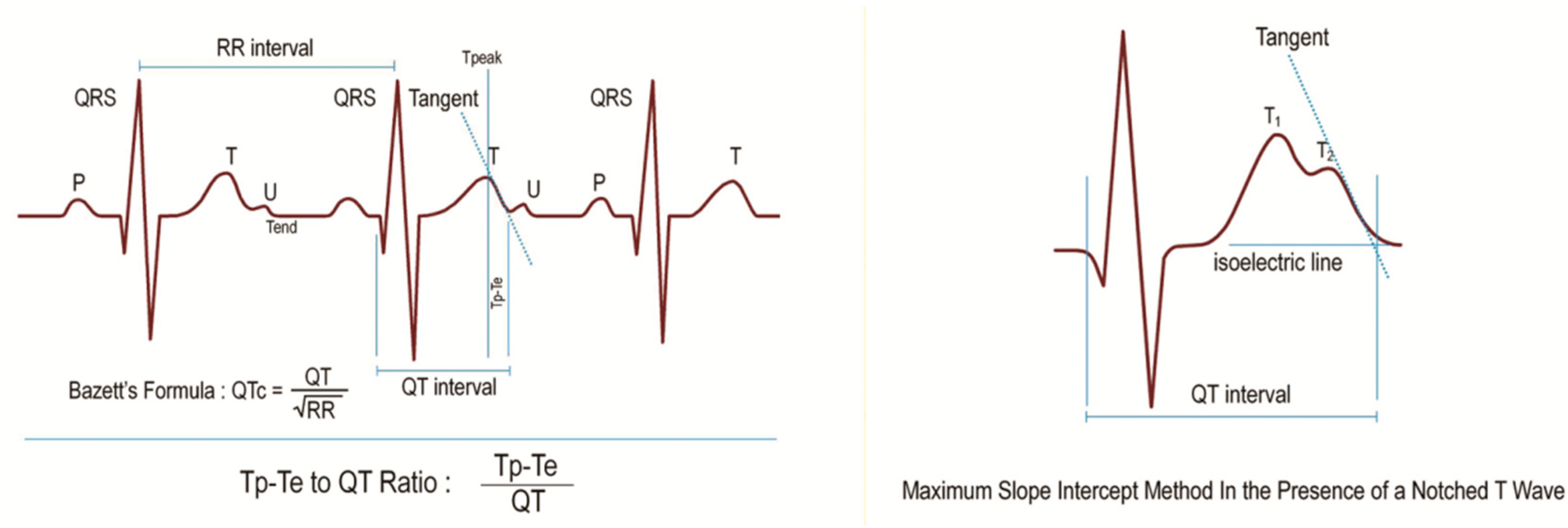
2.2. Electrocardiography
2.3. Exclusion Criteria of the Study
2.4. Statistical Evaluation
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mathew, T.P.; Menown, I.B.A.; Adgey, A.A.J. Death in the Course of Sports. In Forensic Medicine: Clinical and Pathological Aspects, 2nd ed.; Cambridge University Press: London, UK, 2003; pp. 275–288. [Google Scholar]
- Akalın, F.; Topcu, B.; Odabas, I.; Cotuk, B.; Mengutay, S. QT Dispersion in Young Athletes. 2007. Available online: Dergipark.gov.tr/download/article-file/141241 (accessed on 10 March 2018)(In Turkısh).
- Yilmaz, M.; Dagli, M.N. Athlete Health and Exercise-Related Deaths. 2016. Available online: tip.fusabil.org/pdf.php3?id=1149 (accessed on 10 March 2018). (In Turkısh).
- Hart, G. Exercise-induced cardiac hypertrophy: A substrate for sudden death in athletes? Exp. Physiol. 2003, 88, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Martínez, J.P.; Laguna, P.; Olmos, S.; Pahlm, O.; Pettersson, J.; Sörnmo, L. Assessment of QT-measurement accuracy using the 12-lead electrocardiogram derived from EASI leads. J. Electrocardiol. 2007, 40, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Kors, J.A.; Ritsema van Eck, H.J.; Van Herpen, G. The meaning of the Tp-Te interval and its diagnostic value. J. Electrocardiol. 2008, 41, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Antzelevitch, C.; Sicouri, S.; Di Diego, J.M.; Burashnikov, A.; Viskin, S.; Shimizu, W.; Yan, G.X.; Kowey, P.; Zhang, L. Does Tpeak-Tend provide an index of transmural dispersion of repolarization? Heart Rhythm. 2007, 4, 1114–1119. [Google Scholar] [CrossRef] [PubMed]
- Armaganijan, L.; Moreira, D.A.; Nolasco de Araújo, R.R.; Puzzi, M.A.; Munhoz, F.P.; Carvalho, M.J.; Gallo, L.N.; França, J.I.; Lopes, R.D. The usefulness of T-wave peak to T-wave end interval in identifying malignant arrhythmias in patients with Chagas disease. Hellenic J. Cardiol. 2013, 54, 429–434. [Google Scholar] [PubMed]
- Castro, H.J.; Antzelevitch, C.; Tornés, B.F.; Dorantes, S.M.; Dorticós, B.F.; Zayas, M.R.; Quiñones, P.M.A.; Fayad, R.Y. Tpeak-Tend and Tpeak-Tend dispersion as risk factors for ventricular tachycardia/ventricular fibrillation in patients with the Brugada syndrome. J. Am. Coll. Cardiol. 2006, 47, 1828–1834. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Patel, C.; Patel, H.; Narayanaswamy, S.; Malhotra, B.; Green, J.T.; Yan, G.X. T(p-e)/QT ratio as an index of arrhythmogenesis. J. Electrocardiol. 2008, 41, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Karaagac, K.; Tenekecıoglu, E.; Yontar, O.C.; Kuzeytemiz, M.; Vatansever, F.; Tutuncu, A.; Ozluk, O.A.; Yilmaz, M.; Demir, M. Effect of non-dipper and dipper blood pressure patterns on Tp-Te interval and Tp-Te/QT ratio in patients with metabolic syndrome. Int. J. Clin. Exp. Med. 2014, 7, 1397–1403. [Google Scholar] [PubMed]
- Sharashidze, N.; Pagava, Z.; Saatashvili, G.; Kishmarcia, T.; Agladze, R. Exercise induced QT dispersion changes in middle-aged veteran elite athletes. Georgian Med. New 2008, 157, 53–55. [Google Scholar]
- Omiya, K.; Sekizuka, H.; Kida, K.; Suzuki, K.; Akashi, Y.J.; Ohba, H.; Musha, H. Influence of gender and types of sports training on QT variables in young elite athletes. Eur. J. Sport Sci. 2014, 14, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Turkmen, M.; Barutcu, I.; Esen, A.M.; Ocak, Y.; Melek, M.; Kaya, D.; Karakaya, O.; Saglam, M.; Basaran, Y. Assessment of QT interval duration and dispersion in athlete’s heart. J. Int. Med. Res. 2004, 32, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Solomon, J.S.S.; et al. Recommendations for chamber quantification. Eur. J. Echocardiogr. 2006, 7, 79–108. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the American society of echocardiography’s guidelines and standards committee and the chamber quantification writing group, developed in conjunction with the European association of echocardiography, a branch of the European society of cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef] [PubMed]
- Teichholz, L.E.; Kreulen, T.; Herman, M.V.; Gorlin, R. Problems in echocardiographic volume determinations: Echocardiographic-angiographic correlations in the presence of absence of a synergy. Am. J. Cardiol. 1976, 37, 7–11. [Google Scholar] [CrossRef]
- Hudsmith, L.E.; Petersen, S.E.; Francis, J.M.; Robson, M.D.; Neubauer, S. Normal human left and right ventricular and left atrial dimensions using steady state free precession magnetic resonance imaging. J. Cardiovasc. Magn. Reson. 2005, 7, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Burns, E. ECG Basics. 2007. Available online: https://lifeinthefastlane.com/ecg-library/basics/ (accessed on 5 March 2018).
- Indik, J.H.; Pearson, E.C.; Fried, K.; Woosley, R.L. Bazett and Fridericia QT correction formulas interfere with measurement of drug-induced changes in QT interval. Heart Rhythm. 2006, 3, 1003–1007. [Google Scholar] [CrossRef] [PubMed]
- Carbone, A.; D’Andrea, A.; Riegler, L.; Scarafile, R.; Pezzullo, E.; Martone, F.; America, R.; Liccardo, B.; Galderisi, M.; Bossone, E.; et al. Cardiac damage in athlete’s heart: When the “supernormal” heart fails! World J. Cardiol. 2017, 9, 470–480. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; La Gerche, A.; Golia, E.; Teske, A.J.; Bossone, E.; Russo, M.G.; Calabrò, R.; Baggish, A.L. Right heart structural and functional remodeling in athletes. Echocardiography 2015, 32, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Chivulescu, M.; Haugaa, K.; Lie, Ø.H.; Edvardsen, T.; Ginghină, C.; Popescu, B.A.; Jurcut, R. Right ventricular remodeling in athletes and in arrhythmogenic cardiomyopathy. Scand. Cardiovasc. J. 2018, 52, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, I.; Cafri, C.; Zeller, L.; Vodonos, A.; Perry, Z.H.; Kobal, S.L. Athlete’s heart in Israel: Fact or fiction. Isr. Med. Assoc. J. 2014, 16, 46–49. [Google Scholar] [PubMed]
- Bader, R.S.; Goldberg, L.; Sahn, D.J. Risk of sudden cardiac death in young athletes: Which screening strategies are appropriate? Pediatr. Clin. N. Am. 2004, 51, 1421–1441. [Google Scholar] [CrossRef] [PubMed]
- Corrado, D.; Basso, C.; Thiene, G. Sudden death in athletes. Lancet 2005, 366, 547–548. [Google Scholar] [CrossRef]
- Maron, B.J. Sudden death in young athletes. N. Engl. J. Med. 2003, 349, 1064–1075. [Google Scholar] [CrossRef] [PubMed]
- Haider, A.W.; Larson, M.G.; Benjamin, E.J.; Levy, D. Increased left ventricular mass and hypertrophy are associated with increased risk for sudden death. J. Am. Coll. Cardiol. 1998, 32, 1454–1459. [Google Scholar] [CrossRef]
- Pelliccia, A. Athlete’s heart and hypertrophic cardiomyopathy. Curr. Cardiol. Rep. 2000, 2, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Yan, G.X.; Lankipalli, R.S.; Burke, J.F.; Musco, S.; Kowey, P.R. Ventricular repolarization components on the electrocardiogram: Cellular basis and clinical significance. J. Am. Coll. Cardiol. 2003, 42, 401–409. [Google Scholar] [CrossRef]
- Tokatli, A.; Kiliçaslan, F.; Alis, M.; Yiginer, O.; Uzun, M. Prolonged Tp-e interval, Tp-e/QT Ratio and Tp-e/QTc Ratio in patients with Type 2 diabetes mellitus. Endocrinol. Metab. 2016, 31, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Whyte, G.P.; Sheppard, M.; George, K.P.; Shave, R.E.; Wilson, M.; Stephens, N.; Senior, R.; Sharma, S. Arrhythmias and the athlete: Mechanisms and clinical significance. Eur. Heart J. 2007, 28, 1399–1401. [Google Scholar] [CrossRef] [PubMed]
- Aleong, R.G.; Mulvahill, M.J.; Halder, I.; Carlson, N.E.; Singh, M.; Bloom, H.L.; Dudley, S.C.; Ellinor, P.T.; Shalaby, A.; Weiss, R.; et al. Left ventricular dilatation increases the risk of ventricular arrhythmias in patients with reduced systolic function. J. Am. Heart. Assoc. 2015, 4, e001566. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, K.; Reinier, K.; Teodorescu, C.; Uy-Evanado, A.; Aleong, R.; Chugh, H.; Nichols, G.A.; Gunson, K.; London, B.; Jui, J.; et al. Left ventricular diameter and risk stratification for sudden cardiac death. J. Am. Heart Assoc. 2014, 3, e001193. [Google Scholar] [CrossRef] [PubMed]
- Buchheıt, M.; Gındre, C. Cardiac parasympathetic regulation: Respective associations with cardiorespiratory fitness and training load. Am. J. Physiol. Heart Circ. Physiol. 2006, 291, 451–458. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Athlete Group n= 226 | Control Group n= 339 | p | |
|---|---|---|---|
| Age (Year) | 25 (21–30) | 25 (20–33) | 0.63 |
| Gender (Male/Female) | 198/28 | 294/45 | 0.76 |
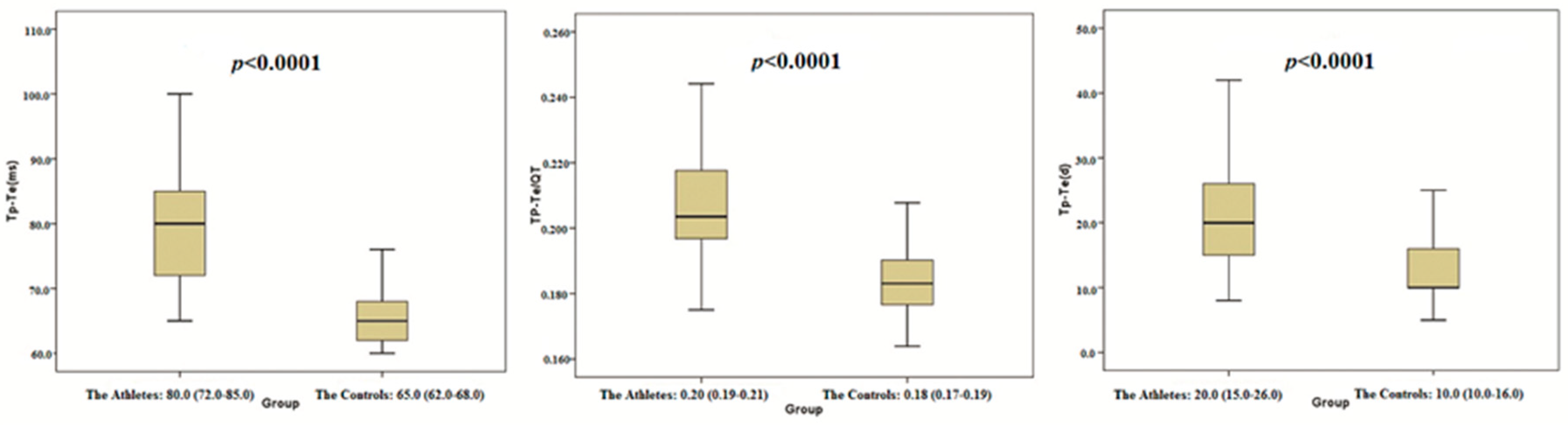
| Tp-Te (ms) | 80.0 (72.0–85.0) | 65.0 (62.0–68.0) | <0.0001 |
| QTmax (ms) | 381.0 (369.0–402.0) | 356.0 (347.0–365.0) | <0.0001 |
| QTc (ms) | 401.29 ± 17.47 | 393.34 ± 23.23 | <0.0001 # |
| Tp-Te/QT ratio | 0.20 (0.19–0.21) | 0.18 (0.17–0.19) | <0.0001 |
| Tp-Te/QTc ratio | 0.20 (0.18–0.21) | 0.16 (0.15–0.17) | <0.0001 |
| Tp-Te(d) (ms) | 20 (15–26) | 10 (10–16) | <0.0001 |
| HR | 65 (57.75–72) | 74 (70–80) | <0.0001 |
| PW (mm) | 10.0 (9.0–11.0) | 8.0 (7.0–8.0) | <0.0001 |
| IVS (mm) | 11.0 (10.0–12.0) | 8.0 (7.0–8.0) | <0.0001 |
| LVEDD (mm) | 54.0 (48.0–58.0) | 42.0 (40.0–44.0) | <0.0001 |
| LVESD (mm) | 39.0 (34.75–43.0) | 27.0 (25.0–29.0) | <0.0001 |
| EF% | 54.0 (50.0–58.0) | 66.13 (63.26–69.41) | <0.0001 |
| FS% | 28.0 (26.0–30.0) | 36.1 (34.1–38.6) | <0.0001 |
| RWT% | 37.5 (34.5–40.0) | 37.0 (34–40) | 0.83 |
| LVEDV (mL) | 141.31 (107.52–166.56) | 78.58 (70.0–87.69) | <0.0001 |
| LVEDVI (mL/m2) | 75.43 (62.78–87.81) | 42 (37.68–46.72) | <0.0001 |
| Length (m) | 1.78 (1.75–1.82) | 1.74 (1.70–1.76) | <0.0001 |
| Weight (kg) | 70.78 ± 9.02 | 75.65 ± 9.78 | <0.0001 # |
| BMI (kg/m2) | 21.97 (21.22–22.87) | 25.42 (23.18–27.11) | <0.0001 |
| BSA (m2) | 1.87 ± 0.16 | 1.90 ± 0.14 | 0.02 # |
| LV mass (g) | 220.59 (158.82–280.42) | 100.60 (89.37–113.63) | <0.0001 |
| LV mass index (g/m2) | 118.74 (87.94–148.26) | 53.22 (47.54–58.88) | <0.0001 |
| SBP (mmHg) | 110.0 (100.0–120.0) | 115.0 (110.0–120.0) | <0.0001 |
| DBP (mmHg) | 70.0 (65.0–70.0) | 70.0 (70.0–80.0) | <0.0001 |
| Tp-Te (ms) | QTmax (ms) | QTc (ms) | TP-Te/QT Ratio | TP-Te/QTc Ratio | Tp-Te(d) (ms) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | r | p | r | p | |
| PW (mm) | 0.874 | <0.0001 | 0.799 | <0.0001 | 0.152 | <0.0001 | 0.741 | <0.0001 | 0.808 | <0.0001 | 0.809 | <0.0001 |
| IVS (mm) | 0.883 | <0.0001 | 0.803 | <0.0001 | 0.173 | <0.0001 | 0.755 | <0.0001 | 0.808 | <0.0001 | 0.792 | <0.0001 |
| LVEDD (mm) | 0.883 | <0.0001 | 0.771 | <0.0001 | 0.106 | 0.050 | 0.776 | <0.0001 | 0.835 | <0.0001 | 0.779 | <0.0001 |
| LVESD (mm) | 0.872 | <0.0001 | 0.762 | <0.0001 | 0.119 | 0.020 | 0.768 | <0.0001 | 0.820 | <0.0001 | 0.758 | <0.0001 |
| LVEDV (mL) | 0.880 | <0.0001 | 0.768 | <0.0001 | 0.095 | 0.023 | 0.771 | <0.0001 | 0.836 | <0.0001 | 0.786 | <0.0001 |
| LVEDVI (mL/m2) | 0.872 | <0.0001 | 0.765 | <0.0001 | 0.114 | 0.007 | 0.760 | <0.0001 | 0.820 | <0.0001 | 0.769 | <0.0001 |
| RWT% | 0.237 | <0.0001 | 0.268 | <0.0001 | 0.122 | 0.004 | 0.164 | <0.0001 | 0.186 | <0.0001 | 0.271 | <0.0001 |
| LV mass (g) | 0.926 | <0.0001 | 0.821 | <0.0001 | 0.117 | 0.010 | 0.798 | <0.0001 | 0.872 | <0.0001 | 0.844 | <0.0001 |
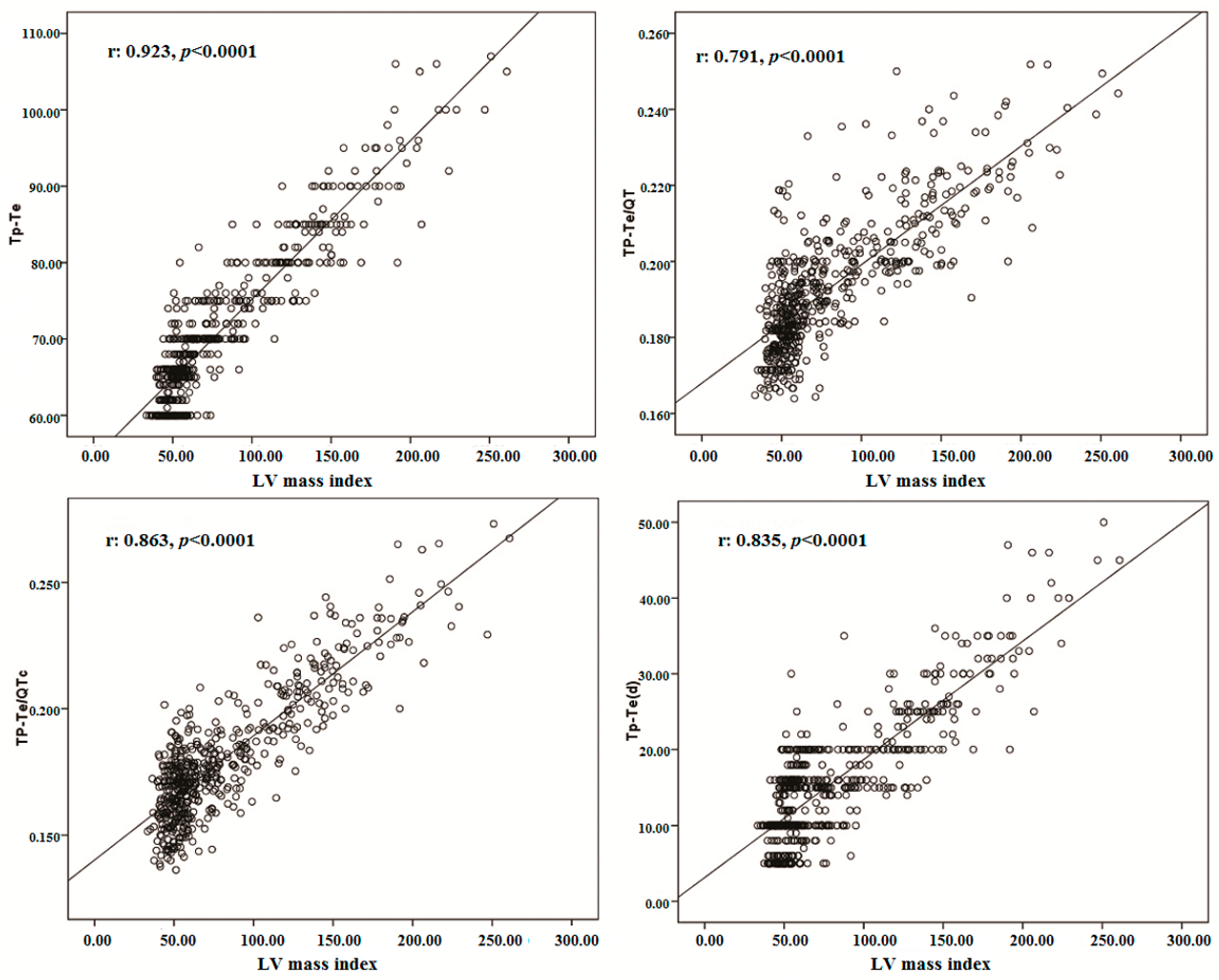
| LV mass index (g/m2) | 0.923 | <0.0001 | 0.823 | <0.0001 | 0.132 | 0.004 | 0.791 | <0.0001 | 0.863 | <0.0001 | 0.835 | <0.0001 |
| Weekly Training Durations | Training Durations–As Years | |||
|---|---|---|---|---|
| r | p | r | p | |
| PW (mm) | 0.147 | 0.02 | 0.652 | <0.0001 |
| IVS (mm) | 0.211 | 0.001 | 0.625 | <0.0001 |
| LVEDD (mm) | 0.036 | 0.06 | 0.710 | <0.0001 |
| LV mass (g) | 0.132 | 0.04 | 0.732 | <0.0001 |
| LV mass index (g/m2) | 0.144 | 0.03 | 0.723 | <0.0001 |
| RWT% | 0.190 | 0.004 | 0.225 | 0.001 |
| LVEDV (mL) | 0.050 | 0.46 | 0.702 | <0.0001 |
| LVEDVI (mL/m2) | 0.051 | 0.44 | 0.700 | <0.0001 |
| Tp-Te (ms) | 0.214 | 0.001 | 0.712 | <0.0001 |
| TP-Te/QT ratio | 0.219 | 0.001 | 0.555 | <0.0001 |
| TP-Te/QTc ratio | 0.159 | 0.017 | 0.651 | <0.0001 |
| Tp-Te (d) (ms) | 0.202 | 0.002 | 0.668 | <0.0001 |
| The Athletes | The Controls | |||
|---|---|---|---|---|
| r | p | r | p | |
| Tp-Te (ms) | −0.659 | <0.0001 | −0.166 | 0.002 |
| QTmax (ms) | −0.776 | <0.0001 | −0.366 | <0.0001 |
| QTc (ms) | 0.652 | <0.0001 | 0.735 | <0.0001 |
| Tp-Te/QT ratio | −0.407 | <0.0001 | 0.076 | 0.16 |
| Tp-Te/QTc ratio | −0.817 | <0.0001 | −0.667 | <0.0001 |
| Tp-Te(d) (ms) | −0.620 | <0.0001 | −0.147 | <0.0001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yılmaz, M.; Kayançiçek, H. Elevated LV Mass and LV Mass Index Sign on the Athlete’s ECG: Athletes’ Hearts are Prone to Ventricular Arrhythmia. J. Clin. Med. 2018, 7, 122. https://doi.org/10.3390/jcm7060122
Yılmaz M, Kayançiçek H. Elevated LV Mass and LV Mass Index Sign on the Athlete’s ECG: Athletes’ Hearts are Prone to Ventricular Arrhythmia. Journal of Clinical Medicine. 2018; 7(6):122. https://doi.org/10.3390/jcm7060122
Chicago/Turabian StyleYılmaz, Mücahid, and Hidayet Kayançiçek. 2018. "Elevated LV Mass and LV Mass Index Sign on the Athlete’s ECG: Athletes’ Hearts are Prone to Ventricular Arrhythmia" Journal of Clinical Medicine 7, no. 6: 122. https://doi.org/10.3390/jcm7060122
APA StyleYılmaz, M., & Kayançiçek, H. (2018). Elevated LV Mass and LV Mass Index Sign on the Athlete’s ECG: Athletes’ Hearts are Prone to Ventricular Arrhythmia. Journal of Clinical Medicine, 7(6), 122. https://doi.org/10.3390/jcm7060122