Coronary Physiology in the Cardiac Catheterization Laboratory


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Historical Basis for Assessing Coronary Physiology in the Catheterization Laboratory
3. Coronary Physiology in the Evaluation of Coronary Artery Disease
4. Assessment of Microvascular Disease and Endothelial Dysfunction
5. Summary and Conclusions
Author Contributions
Conflicts of Interest
References
- Cheng, T.O. First selective coronary arteriogram. Circulation 2003, 107, E42-2, author reply E-2. [Google Scholar] [CrossRef]
- Ryan, T.J. The coronary angiogram and its seminal contributions to cardiovascular medicine over five decades. Circulation 2002, 106, 752–756. [Google Scholar] [CrossRef]
- Patel, M.R.; Peterson, E.D.; Dai, D.; Brennan, J.M.; Redberg, R.F.; Anderson, H.V.; Brindis, R.G.; Douglas, P.S. Low diagnostic yield of elective coronary angiography. N. Engl. J. Med. 2010, 362, 886–895. [Google Scholar] [CrossRef] [PubMed]
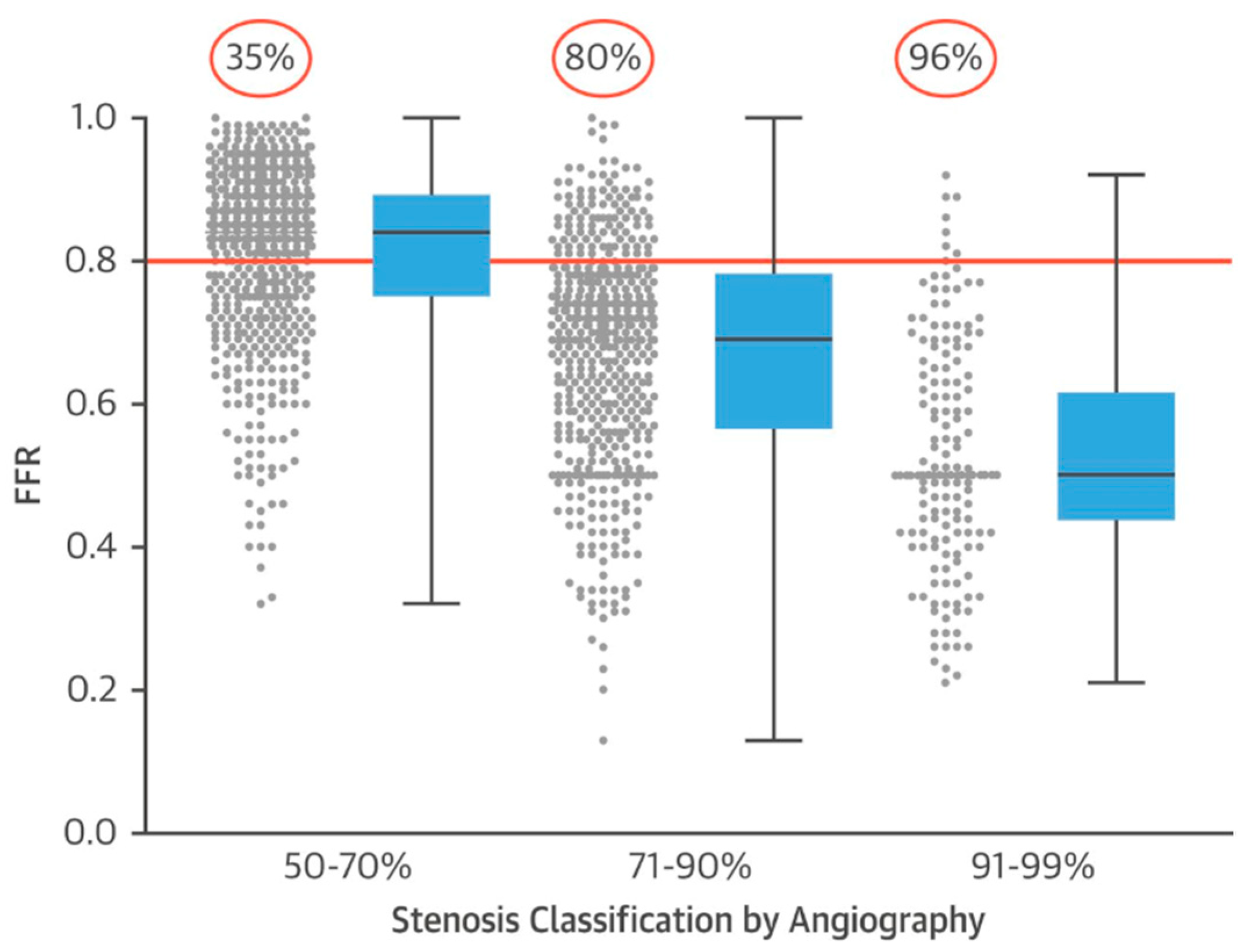
- Park, S.J.; Kang, S.J.; Ahn, J.M.; Shim, E.B.; Kim, Y.T.; Yun, S.C.; Song, H.; Lee, J.Y.; Kim, W.J.; Park, D.W.; et al. Visual-functional mismatch between coronary angiography and fractional flow reserve. JACC Cardiovasc. Interv. 2012, 5, 1029–1036. [Google Scholar] [CrossRef] [PubMed]
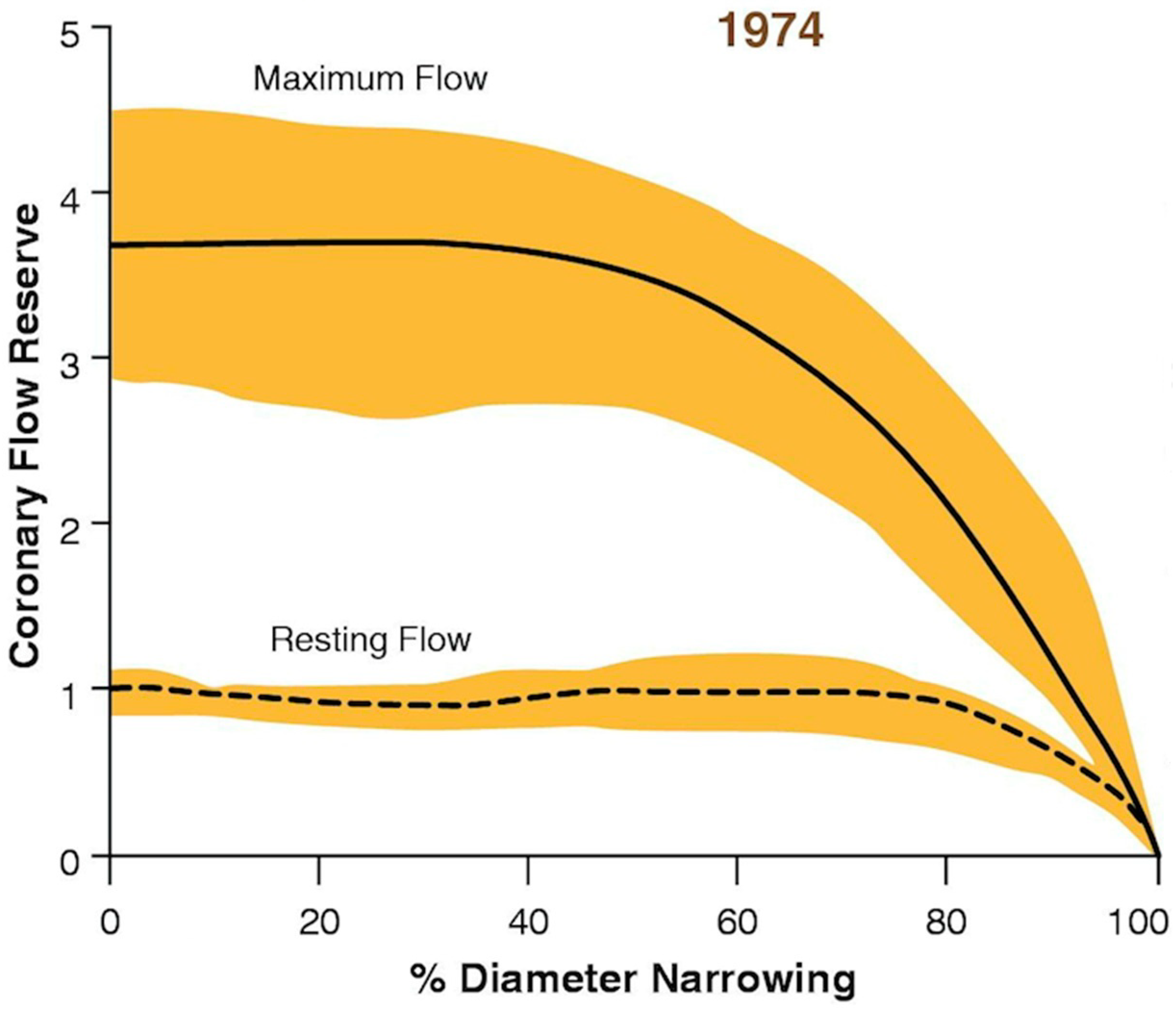
- Gould, K.L.; Lipscomb, K.; Hamilton, G.W. Physiologic basis for assessing critical coronary stenosis. Instantaneous flow response and regional distribution during coronary hyperemia as measures of coronary flow reserve. Am. J. Cardiol. 1974, 33, 87–94. [Google Scholar] [CrossRef]
- Stone, G.W.; Maehara, A.; Lansky, A.J.; de Bruyne, B.; Cristea, E.; Mintz, G.S.; Mehran, R.; McPherson, J.; Farhat, N.; Marso, S.P.; et al. A prospective natural-history study of coronary atherosclerosis. N. Engl. J. Med. 2011, 364, 226–235. [Google Scholar] [CrossRef]
- Klocke, F.J. Coronary blood flow in man. Prog. Cardiovasc. Dis. 1976, 19, 117–166. [Google Scholar] [CrossRef]
- Kitamura, K.; Jorgensen, C.R.; Gobel, F.L.; Taylor, H.L.; Wang, Y. Hemodynamic correlates of myocardial oxygen consumption during upright exercise. J. Appl. Physiol. 1972, 32, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Gould, K.L. Coronary flow reserve and pharmacologic stress perfusion imaging: Beginnings and evolution. JACC. Cardiovasc. Imaging 2009, 2, 664–669. [Google Scholar] [CrossRef] [PubMed]
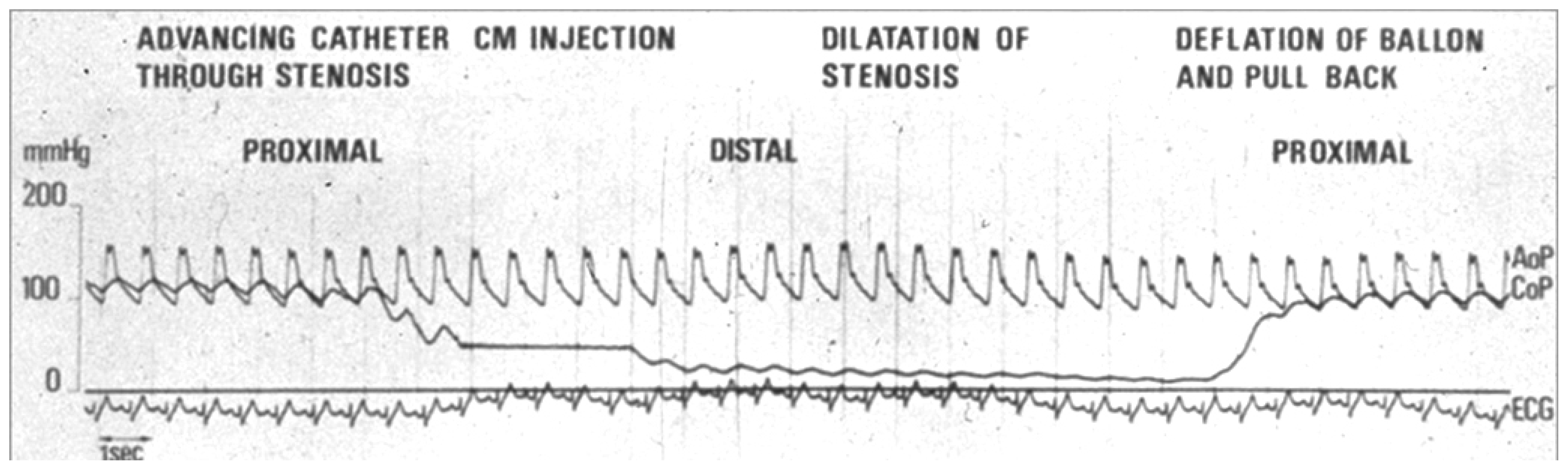
- Gruntzig, A.R.; Senning, A.; Siegenthaler, W.E. Nonoperative dilatation of coronary-artery stenosis: Percutaneous transluminal coronary angioplasty. N. Engl. J. Med. 1979, 301, 61–68. [Google Scholar] [CrossRef]
- Meier, B. The first patient to undergo coronary angioplasty--23-year follow-up. N. Engl. J. Med. 2001, 344, 144–145. [Google Scholar] [CrossRef] [PubMed]
- Vogel, R.A.; Bates, E.R.; O’Neill, W.W.; Aueron, F.M.; Meier, B.; Gruentzig, A.R. Coronary flow reserve measured during cardiac catheterization. Arch. Intern. Med. 1984, 144, 1773–1776. [Google Scholar] [CrossRef] [PubMed]
- Meier, B.; Gruentzig, A.R.; Goebel, N.; Pyle, R.; von Gosslar, W.; Schlumpf, M. Assessment of stenoses in coronary angioplasty. Inter- and intraobserver variability. Int. J. Cardiol. 1983, 3, 159–169. [Google Scholar] [CrossRef]
- Jeremias, A.; Kirtane, A.J.; Stone, G.W. A Test in Context: Fractional Flow Reserve: Accuracy, Prognostic Implications, and Limitations. J. Am. Coll. Cardiol. 2017, 69, 2748–2758. [Google Scholar] [CrossRef] [PubMed]
- Benchimol, A.; Stegall, H.F.; Gartlan, J.L. New method to measure phasic coronary blood velocity in man. Am. Heart J. 1971, 81, 93–101. [Google Scholar] [CrossRef]
- Wilson, R.F.; Laughlin, D.E.; Ackell, P.H.; Chilian, W.M.; Holida, M.D.; Hartley, C.J.; Armstrong, M.L.; Marcus, M.L.; White, C.W. Transluminal, subselective measurement of coronary artery blood flow velocity and vasodilator reserve in man. Circulation 1985, 72, 82–92. [Google Scholar] [CrossRef]
- White, C.W.; Wilson, R.F.; Marcus, M.L. Methods of measuring myocardial blood flow in humans. Prog. Cardiovasc. Dis. 1988, 31, 79–94. [Google Scholar] [CrossRef]
- Doucette, J.W.; Corl, P.D.; Payne, H.M.; Flynn, A.E.; Goto, M.; Nassi, M.; Segal, J. Validation of a Doppler guide wire for intravascular measurement of coronary artery flow velocity. Circulation 1992, 85, 1899–1911. [Google Scholar] [CrossRef] [PubMed]
- Serruys, P.W.; de Bruyne, B.; Carlier, S.; Sousa, J.E.; Piek, J.; Muramatsu, T.; Vrints, C.; Probst, P.; Seabra-Gomes, R.; Simpson, I.; et al. Randomized comparison of primary stenting and provisional balloon angioplasty guided by flow velocity measurement. Doppler Endpoints Balloon Angioplasty Trial Europe (DEBATE) II Study Group. Circulation 2000, 102, 2930–2937. [Google Scholar] [CrossRef]
- Meier, B. His master’s art, Andreas Gruntzig’s approach to performing and teaching coronary angioplasty. EuroIntervention 2017, 13, 15–27. [Google Scholar] [CrossRef]
- Pijls, N.H.; van Son, J.A.; Kirkeeide, R.L.; De Bruyne, B.; Gould, K.L. Experimental basis of determining maximum coronary, myocardial, and collateral blood flow by pressure measurements for assessing functional stenosis severity before and after percutaneous transluminal coronary angioplasty. Circulation 1993, 87, 1354–1367. [Google Scholar] [CrossRef] [PubMed]
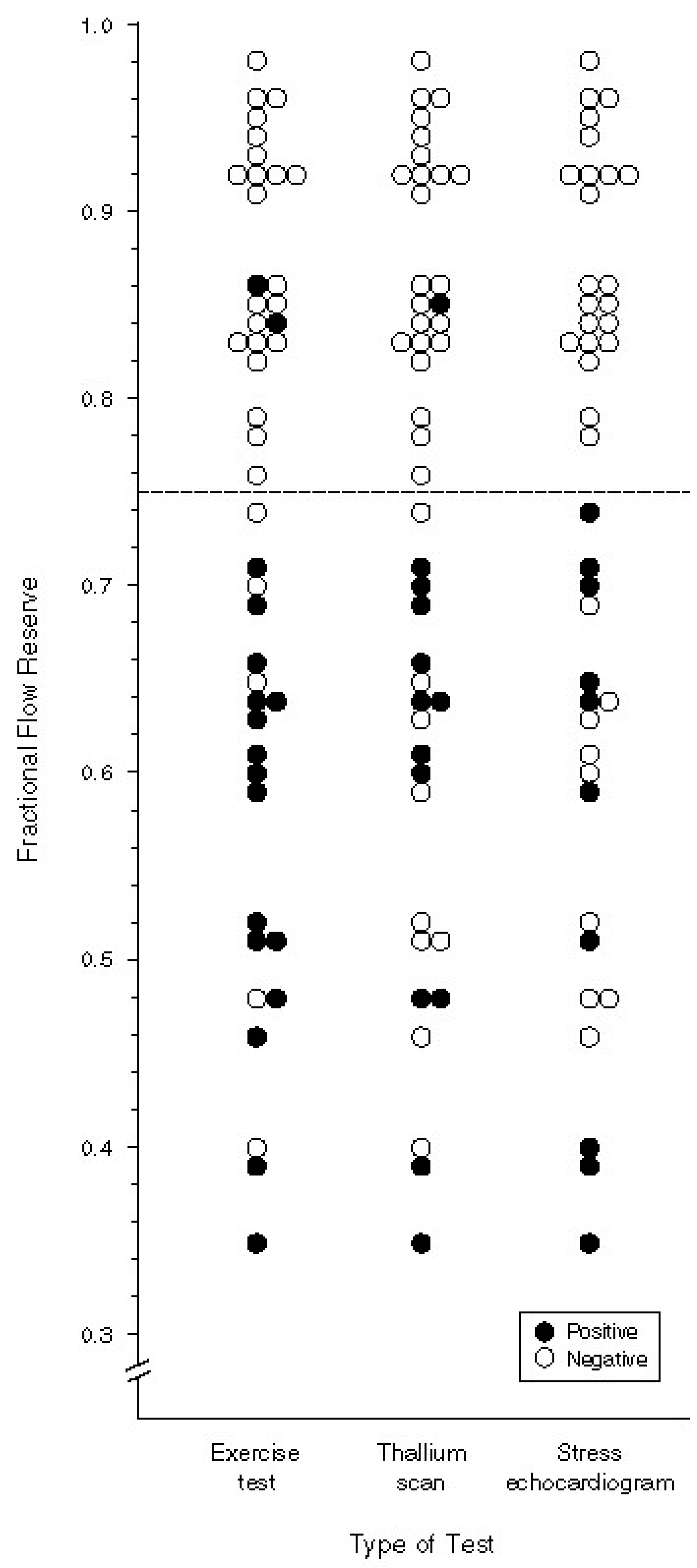
- Pijls, N.H.; De Bruyne, B.; Peels, K.; Van Der Voort, P.H.; Bonnier, H.J.; Bartunek, J.K.J.J.; Koolen, J.J. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N. Engl. J. Med. 1996, 334, 1703–1708. [Google Scholar] [CrossRef] [PubMed]
- Bech, G.J.; De Bruyne, B.; Pijls, N.H.; de Muinck, E.D.; Hoorntje, J.C.; Escaned, J.; Stella, P.R.; Boersma, E.; Bartunek, J.; Koolen, J.J.; et al. Fractional flow reserve to determine the appropriateness of angioplasty in moderate coronary stenosis: A randomized trial. Circulation 2001, 103, 2928–2934. [Google Scholar] [CrossRef] [PubMed]
- Pijls, N.H.; van Schaardenburgh, P.; Manoharan, G.; Boersma, E.; Bech, J.W.; van’t Veer, M.; Bär, F.; Hoorntje, J.; Koolen, J.; Wijns, W.; et al. Percutaneous coronary intervention of functionally nonsignificant stenosis: 5-year follow-up of the DEFER Study. J. Am. Coll. Cardiol. 2007, 49, 2105–2111. [Google Scholar] [CrossRef]
- Tonino, P.A.; De Bruyne, B.; Pijls, N.H.; Siebert, U.; Ikeno, F.; van’ t Veer, M.; Klauss, V.; Manoharan, G.; Engstrøm, T.; Oldroyd, K.G.; et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N. Engl. J. Med. 2009, 360, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Tonino, P.A.; Fearon, W.F.; De Bruyne, B.; Oldroyd, K.G.; Leesar, M.A.; Ver Lee, P.N.; Maccarthy, P.A.; Van’t Veer, M.; Pijls, N.H. Angiographic versus functional severity of coronary artery stenoses in the FAME study fractional flow reserve versus angiography in multivessel evaluation. J. Am. Coll. Cardiol. 2010, 55, 2816–2821. [Google Scholar] [CrossRef] [PubMed]
- De Bruyne, B.; Pijls, N.H.; Kalesan, B.; Barbato, E.; Tonino, P.A.; Piroth, Z.; Jagic, N.; Möbius-Winkler, S.; Rioufol, G.; Witt, N.; et al. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. N. Engl. J. Med. 2012, 367, 991–1001. [Google Scholar] [CrossRef]
- Fearon, W.F.; Nishi, T.; De Bruyne, B.; Boothroyd, D.B.; Barbato, E.; Tonino, P.; Jüni, P.; Pijls, N.H.J.; Hlatky, M.A. FAME 2 Trial Investigators. Clinical Outcomes and Cost-Effectiveness of Fractional Flow Reserve-Guided Percutaneous Coronary Intervention in Patients with Stable Coronary Artery Disease: Three-Year Follow-Up of the FAME 2 Trial (Fractional Flow Reserve Versus Angiography for Multivessel Evaluation). Circulation 2018, 137, 480–487. [Google Scholar]
- Ntalianis, A.; Sels, J.W.; Davidavicius, G.; Tanaka, N.; Muller, O.; Trana, C.; Barbato, E.; Hamilos, M.; Mangiacapra, F.; Heyndrickx, G.R.; et al. Fractional flow reserve for the assessment of nonculprit coronary artery stenoses in patients with acute myocardial infarction. JACC Cardiovasc. Interv. 2010, 3, 1274–1281. [Google Scholar] [CrossRef]
- Kern, M.J.; Samady, H. Current concepts of integrated coronary physiology in the catheterization laboratory. J. Am. Coll. Cardiol. 2010, 55, 173–185. [Google Scholar] [CrossRef]
- Hakeem, A.; Edupuganti, M.M.; Almomani, A.; Pothineni, N.V.; Payne, J.; Abualsuod, A.M.; Bhatti, S.; Ahmed, Z.; Uretsky, B.F. Long-Term Prognosis of Deferred Acute Coronary Syndrome Lesions Based on Nonischemic Fractional Flow Reserve. J. Am. Coll. Cardiol. 2016, 68, 1181–1191. [Google Scholar] [CrossRef] [PubMed]
- Al-Lamee, R.; Thompson, D.; Dehbi, H.M.; Sen, S.; Tang, K.; Davies, J.; Keeble, T.; Mielewczik, M.; Kaprielian, R.; Malik, I.S.; et al. Percutaneous coronary intervention in stable angina (ORBITA): A double-blind, randomised controlled trial. Lancet 2018, 391, 31–40. [Google Scholar] [CrossRef]
- Al-Lamee, R.; Howard, J.P.; Shun-Shin, M.J.; Thompson, D.; Dehbi, H.M.; Sen, S.; Nijjer, S.; Petraco, R.; Davies, J.; Keeble, T.; et al. Fractional Flow Reserve and Instantaneous Wave-Free Ratio as Predictors of the Placebo-Controlled Response to Percutaneous Coronary Intervention in Stable Single-Vessel Coronary Artery Disease: Physiology-Stratified Analysis of ORBITA. Circulation 2018, 138, 1780–1792. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J. Am. Coll. Cardiol. 2011, 58, e44–e122. [Google Scholar] [CrossRef] [PubMed]
- Pothineni, N.V.; Shah, N.N.; Rochlani, Y.; Nairooz, R.; Raina, S.; Leesar, M.A.; Uretsky, B.F.; Hakeem, A. U.S. Trends in Inpatient Utilization of Fractional Flow Reserve and Percutaneous Coronary Intervention. J. Am. Coll. Cardiol. 2016, 67, 732–733. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, R.; Charron, T.; Puley, G.; Dick, A.; Strauss, B.H. Microvascular obstruction and the no-reflow phenomenon after percutaneous coronary intervention. Circulation 2008, 117, 3152–3156. [Google Scholar] [CrossRef] [PubMed]
- Polimeni, A.; De Rosa, S.; Sabatino, J.; Sorrentino, S.; Indolfi, C. Impact of intracoronary adenosine administration during primary PCI: A meta-analysis. Int. J. Cardiol. 2016, 203, 1032–1041. [Google Scholar] [CrossRef]
- Sen, S.; Escaned, J.; Malik, I.S.; Mikhail, G.W.; Foale, R.A.; Mila, R.; Tarkin, J.; Petraco, R.; Broyd, C.; Jabbour, R.; et al. Development and validation of a new adenosine-independent index of stenosis severity from coronary wave-intensity analysis: Results of the ADVISE (ADenosine Vasodilator Independent Stenosis Evaluation) study. J. Am. Coll. Cardiol. 2012, 59, 1392–1402. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.E.; Sen, S.; Escaned, J. Instantaneous Wave-free Ratio versus Fractional Flow Reserve. N. Engl. J. Med. 2017, 377, 1597–1598. [Google Scholar] [PubMed]
- Jeremias, A.; Maehara, A.; Genereux, P.; Asrress, K.N.; Berry, C.; De Bruyne, B.; Davies, J.E.; Escaned, J.; Fearon, W.F.; Gould, K.L.; et al. Multicenter core laboratory comparison of the instantaneous wave-free ratio and resting Pd/Pa with fractional flow reserve: The RESOLVE study. J. Am. Coll. Cardiol. 2014, 63, 1253–1261. [Google Scholar] [CrossRef]
- Johnson, N.P.; Kirkeeide, R.L.; Asrress, K.N.; Fearon, W.F.; Lockie, T.; Marques, K.M.; Pyxaras, S.A.; Rolandi, M.C.; van ’t Veer, M.; De Bruyne, B.; et al. Does the instantaneous wave-free ratio approximate the fractional flow reserve? J. Am. Coll. Cardiol. 2013, 61, 1428–1435. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.E.; Sen, S.; Dehbi, H.M.; Al-Lamee, R.; Petraco, R.; Nijjer, S.S.; Bhindi, R.; Lehman, S.J.; Walters, D.; Sapontis, J.; et al. Use of the Instantaneous Wave-free Ratio or Fractional Flow Reserve in PCI. N. Engl. J. Med. 2017, 376, 1824–1834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gotberg, M.; Christiansen, E.H.; Gudmundsdottir, I.J.; Sandhall, L.; Danielewicz, M.; Jakobsen, L.; Olsson, S.E.; Öhagen, P.; Olsson, H.; Omerovic, E.; et al. Instantaneous Wave-free Ratio versus Fractional Flow Reserve to Guide PCI. N. Engl. J. Med. 2017, 376, 1813–1823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, C.; McClure, J.D.; Oldroyd, K.G. Meta-Analysis of Death and Myocardial Infarction in the DEFINE-FLAIR and iFR-SWEDEHEART Trials. Circulation 2017, 136, 2389–2391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Rosa, S.; Polimeni, A.; Petraco, R.; Davies, J.E.; Indolfi, C. Diagnostic Performance of the Instantaneous Wave-Free Ratio: Comparison With Fractional Flow Reserve. Circ. Cardiovasc. Interv. 2018, 11, e004613. [Google Scholar] [CrossRef] [PubMed]
- Indolfi, C.; Mongiardo, A.; Spaccarotella, C.; Torella, D.; Caiazzo, G.; Polimeni, A.; Sorrentino, S.; Micieli, M.; Sabatino, J.; Curcio, A.; et al. The instantaneous wave-free ratio (iFR) for evaluation of non-culprit lesions in patients with acute coronary syndrome and multivessel disease. Int. J. Cardiol. 2015, 178, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Ruigomez, A.; Rodriguez, L.A.; Wallander, M.A.; Johansson, S.; Jones, R. Chest pain in general practice: Incidence, comorbidity and mortality. Fam. Pract. 2006, 23, 167–174. [Google Scholar] [CrossRef]
- Safdar, B.; Dziura, J.; Bathulapalli, H.; Leslie, D.L.; Skanderson, M.; Brandt, C.; Haskell, S.G. Chest pain syndromes are associated with high rates of recidivism and costs in young United States Veterans. BMC Fam. Pract. 2015, 16, 88. [Google Scholar] [CrossRef]
- Lee, B.K.; Lim, H.S.; Fearon, W.F.; Yong, A.S.; Yamada, R.; Tanaka, S.; Lee, D.P.; Yeung, A.C.; Tremmel, J.A. Invasive evaluation of patients with angina in the absence of obstructive coronary artery disease. Circulation 2015, 131, 1054–1060. [Google Scholar] [CrossRef]
- DeMaria, A.N.; Lee, G.; Amsterdam, E.A.; Low, R.; Mason, D.T. The anginal syndrome with normal coronary arteries. Etiologic and prognostic considerations. JAMA 1980, 244, 826–828. [Google Scholar] [CrossRef]
- Gould, K.L.; Johnson, N.P. Coronary Physiology Beyond Coronary Flow Reserve in Microvascular Angina: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 2642–2662. [Google Scholar] [CrossRef] [PubMed]
- Ford, T.J.; Stanley, B.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; Robertson, K.; et al. Stratified Medical Therapy Using Invasive Coronary Function Testing in Angina: The CorMicA Trial. J. Am. Coll. Cardiol. 2018, 72, 2841–2855. [Google Scholar] [CrossRef] [PubMed]
- Mann, D.L.; Zipes, D.P.; Libby, P.; Bonow, R.O.; Braunwald, E. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine, 10th ed.; Elsevier/Saunders: Philadelphia, PA, USA, 2015. [Google Scholar]
- Camici, P.G.; Crea, F. Coronary microvascular dysfunction. N. Engl. J. Med. 2007, 356, 830–840. [Google Scholar] [CrossRef] [PubMed]
- Camici, P.G.; d’Amati, G.; Rimoldi, O. Coronary microvascular dysfunction: Mechanisms and functional assessment. Nat. Rev. Cardiol. 2015, 12, 48–62. [Google Scholar] [CrossRef] [PubMed]
- Fihn, S.D.; Gardin, J.M.; Abrams, J.; Berra, K.; Blankenship, J.C.; Dallas, A.P.; Douglas, P.S.; Foody, J.M.; Gerber, T.C.; Hinderliter, A.L.; et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J. Am. Coll. Cardiol. 2012, 60, e44–e164. [Google Scholar] [PubMed]
- Lotfi, A.; Jeremias, A.; Fearon, W.F.; Feldman, M.D.; Mehran, R.; Messenger, J.C.; Grines, C.L.; Dean, L.S.; Kern, M.J.; Klein, L.W.; et al. Expert consensus statement on the use of fractional flow reserve, intravascular ultrasound, and optical coherence tomography: A consensus statement of the Society of Cardiovascular Angiography and Interventions. Catheter. Cardiovasc. Interv. 2014, 83, 509–518. [Google Scholar] [CrossRef]
- Hannawi, B.; Lam, W.W.; Wang, S.; Younis, G.A. Current use of fractional flow reserve: A nationwide survey. Tex. Heart Inst. J. 2014, 41, 579–584. [Google Scholar] [CrossRef]
- Reis, S.E.; Holubkov, R.; Lee, J.S.; Sharaf, B.; Reichek, N.; Rogers, W.J.; Walsh, E.G.; Fuisz, A.R.; Kerensky, R.; Detre, K.M.; et al. Coronary flow velocity response to adenosine characterizes coronary microvascular function in women with chest pain and no obstructive coronary disease. Results from the pilot phase of the Women’s Ischemia Syndrome Evaluation (WISE) study. J. Am. Coll. Cardiol. 1999, 33, 1469–1475. [Google Scholar] [CrossRef]
- Geltman, E.M.; Henes, C.G.; Senneff, M.J.; Sobel, B.E.; Bergmann, S.R. Increased myocardial perfusion at rest and diminished perfusion reserve in patients with angina and angiographically normal coronary arteries. J. Am. Coll. Cardiol. 1990, 16, 586–595. [Google Scholar] [CrossRef] [Green Version]
- Britten, M.B.; Zeiher, A.M.; Schachinger, V. Microvascular dysfunction in angiographically normal or mildly diseased coronary arteries predicts adverse cardiovascular long-term outcome. Coron. Artery. Dis. 2004, 15, 259–264. [Google Scholar] [CrossRef]
- Bugiardini, R.; Bairey Merz, C.N. Angina with “normal” coronary arteries: A changing philosophy. JAMA 2005, 293, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Crea, F.; Camici, P.G.; Bairey Merz, C.N. Coronary microvascular dysfunction: An update. Eur. Heart J. 2014, 35, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- Pijls, N.H.; De Bruyne, B.; Smith, L.; Aarnoudse, W.; Barbato, E.; Bartunek, J.; Bech, G.J.; Van De Vosse, F. Coronary thermodilution to assess flow reserve: Validation in humans. Circulation 2002, 105, 2482–2486. [Google Scholar] [CrossRef] [PubMed]
- Fearon, W.F.; Balsam, L.B.; Farouque, H.M.; Caffarelli, A.D.; Robbins, R.C.; Fitzgerald, P.J.; Yock, P.G.; Yeung, A.C. Novel index for invasively assessing the coronary microcirculation. Circulation 2003, 107, 3129–3132. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.K.; Yeung, A.C.; Fearon, W.F. Invasive assessment of the coronary microcirculation: Superior reproducibility and less hemodynamic dependence of index of microcirculatory resistance compared with coronary flow reserve. Circulation 2006, 113, 2054–2061. [Google Scholar] [CrossRef] [PubMed]
- Martinez, G.J.; Yong, A.S.; Fearon, W.F.; Ng, M.K. The index of microcirculatory resistance in the physiologic assessment of the coronary microcirculation. Coron. Artery. Dis. 2015, 26, e15–e26. [Google Scholar] [CrossRef] [PubMed]
- Aarnoudse, W.; Fearon, W.F.; Manoharan, G.; Geven, M.; van de Vosse, F.; Rutten, M.; De Bruyne, B.; Pijls, N.H. Epicardial stenosis severity does not affect minimal microcirculatory resistance. Circulation 2004, 110, 2137–2142. [Google Scholar] [CrossRef] [PubMed]
- Yong, A.S.; Layland, J.; Fearon, W.F.; Ho, M.; Shah, M.G.; Daniels, D.; Whitbourn, R.; Macisaac, A.; Kritharides, L.; Wilson, A.; et al. Calculation of the index of microcirculatory resistance without coronary wedge pressure measurement in the presence of epicardial stenosis. JACC Cardiovasc. Interv. 2013, 6, 53–58. [Google Scholar] [CrossRef]
- Yong, A.S.; Ho, M.; Shah, M.G.; Ng, M.K.; Fearon, W.F. Coronary microcirculatory resistance is independent of epicardial stenosis. Circ. Cardiovasc. Interv. 2012, 5, 103–108. [Google Scholar] [CrossRef]
- Carrick, D.; Haig, C.; Carberry, J.; May, V.T.; McCartney, P.; Welsh, P.; Ahmed, N.; McEntegart, M.; Petrie, M.C.; Eteiba, H.; et al. Microvascular resistance of the culprit coronary artery in acute ST-elevation myocardial infarction. JCI Insight 2016, 1, e85768. [Google Scholar] [CrossRef]
- Cuculi, F.; De Maria, G.L.; Meier, P.; Dall’Armellina, E.; de Caterina, A.R.; Channon, K.M.; Prendergast, B.D.; Choudhury, R.P.; Forfar, J.C.; Kharbanda, R.K.; et al. Impact of microvascular obstruction on the assessment of coronary flow reserve, index of microcirculatory resistance, and fractional flow reserve after ST-segment elevation myocardial infarction. J. Am. Coll. Cardiol. 2014, 64, 1894–1904. [Google Scholar] [CrossRef] [PubMed]
- Samady, H.; Hung, O.Y. Coronary microvasculature: Small vessels with large impact. Circ. Cardiovasc. Interv. 2013, 6, 323–325. [Google Scholar] [CrossRef] [PubMed]
- Fearon, W.F.; Farouque, H.M.; Balsam, L.B.; Caffarelli, A.D.; Cooke, D.T.; Robbins, R.C.; Fitzgerald, P.J.; Yeung, A.C.; Yock, P.G. Comparison of coronary thermodilution and Doppler velocity for assessing coronary flow reserve. Circulation 2003, 108, 2198–2200. [Google Scholar] [CrossRef] [PubMed]
- de Waard, G.A.; Fahrni, G.; de Wit, D.; Kitabata, H.; Williams, R.; Patel, N.; Teunissen, P.F.; van de Ven, P.M.; Umman, S.; Knaapen, P.; et al. Hyperaemic microvascular resistance predicts clinical outcome and microvascular injury after myocardial infarction. Heart 2018, 104, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Yamanaga, K.; Tsujita, K.; Komura, N.; Kaikita, K.; Sakamoto, K.; Miyazaki, T.; Saito, M.; Ishii, M.; Tabata, N.; Akasaka, T.; et al. Single-wire pressure and flow velocity measurement for quantifying microvascular dysfunction in patients with coronary vasospastic angina. Am. J. Physiol. Heart Circ. Physiol. 2015, 308, H478–H484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, R.P.; de Waard, G.A.; De Silva, K.; Lumley, M.; Asrress, K.; Arri, S.; Ellis, H.; Mir, A.; Clapp, B.; Chiribiri, A.; et al. Doppler Versus Thermodilution-Derived Coronary Microvascular Resistance to Predict Coronary Microvascular Dysfunction in Patients With Acute Myocardial Infarction or Stable Angina Pectoris. Am. J. Cardiol. 2018, 121, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Everaars, H.; de Waard, G.A.; Driessen, R.S.; Danad, I.; van de Ven, P.M.; Raijmakers, P.G.; Lammertsma, A.A.; van Rossum, A.C.; Knaapen, P.; van Royen, N. Doppler Flow Velocity and Thermodilution to Assess Coronary Flow Reserve: A Head-to-Head Comparison With [(15)O]H2O PET. JACC Cardiovasc. Interv. 2018, 11, 2044–2054. [Google Scholar] [CrossRef]
- Engstrom, T.; Kelbaek, H.; Helqvist, S.; Hofsten, D.E.; Klovgaard, L.; Holmvang, L.; Jørgensen, E.; Pedersen, F.; Saunamäki, K.; Clemmensen, P.; et al. Complete revascularisation versus treatment of the culprit lesion only in patients with ST-segment elevation myocardial infarction and multivessel disease (DANAMI-3-PRIMULTI): An open-label, randomised controlled trial. Lancet 2015, 386, 665–671. [Google Scholar] [CrossRef]
- Tu, S.; Westra, J.; Yang, J.; von Birgelen, C.; Ferrara, A.; Pellicano, M.; Nef, H.; Tebaldi, M.; Murasato, Y.; Lansky, A.; et al. Diagnostic Accuracy of Fast Computational Approaches to Derive Fractional Flow Reserve From Diagnostic Coronary Angiography: The International Multicenter FAVOR Pilot Study. JACC Cardiovasc. Interv. 2016, 9, 2024–2035. [Google Scholar] [CrossRef]




© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shah, S.M.; Pfau, S.E. Coronary Physiology in the Cardiac Catheterization Laboratory. J. Clin. Med. 2019, 8, 255. https://doi.org/10.3390/jcm8020255
Shah SM, Pfau SE. Coronary Physiology in the Cardiac Catheterization Laboratory. Journal of Clinical Medicine. 2019; 8(2):255. https://doi.org/10.3390/jcm8020255
Chicago/Turabian StyleShah, Samit M., and Steven E. Pfau. 2019. "Coronary Physiology in the Cardiac Catheterization Laboratory" Journal of Clinical Medicine 8, no. 2: 255. https://doi.org/10.3390/jcm8020255
APA StyleShah, S. M., & Pfau, S. E. (2019). Coronary Physiology in the Cardiac Catheterization Laboratory. Journal of Clinical Medicine, 8(2), 255. https://doi.org/10.3390/jcm8020255