Clinical Stratification of High-Grade Ovarian Serous Carcinoma Using a Panel of Six Biomarkers

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection and Preparation
2.2. Animal Studies
2.3. Immunohistochemical (IHC) and Histochemical Staining (HC)
2.4. Statistical Analysis
3. Results
3.1. Selection of Class-Specific Biomarkers, Development of SOPs for Detection, a Reference Human Tissue Library and Guidelines for Scoring
- (i)
- Score for Marker Frequency (SFreq)-percentage expression in total tumor cells of tissue section on a scale of 0–3 (0: absent, 1: 1–10%, 2: 11–50%, and 3: ≥51% marker-positive),
- TCF21: cardiac myocytes, ovarian stromal cells, and germinal cells of testis represented SFreq 0, 1, and 3 respectively; SFreq = 2 could not be identified in healthy tissues.
- E-cadherin: cardiac myocytes, liver hepatocytes, and prostate epithelial cells represented SFreq 0, 2, and 3 respectively; healthy tissues representing SFreq = 1 could not be identified.
- PARP1: mucosa of the small intestine, cardiac myocytes, germinal basal cells of testis represented SFreq as 0, 1, and 3 respectively; healthy tissues representing SFreq = 2 could not be identified.
- Slug: cardiac myocytes, smooth muscles of the appendix, lymphocytes of the small intestine represented SFreq 0, 1, and 2 respectively; healthy tissues representing SFreq = 3 could not be identified.
- HA: cartilage and sub-mucosa of the small intestine represented SFreq as 2 and 3 respectively; healthy tissues representing SFreq = 0 or 1 could not be identified.
- ANXA2: cardiac myocytes, the somatic muscle of the small intestine, epithelial cells of the gall bladder represented SFreq 0, 1, and 3 respectively; healthy tissues representing SFreq = 2 could not be identified.
- (ii)
- Score for marker intensity (SInt)-intensity of brown stain for IHC and blue for HC in positively stained tissue sections. A scale of 0–3 was established, 0: absent, 1: weak, 2: moderate, and 3: strong intensity of marker-positive cells,
- TCF21: cardiac myocytes, ovarian stromal cells, germinal basal cells of testis represented SInt 0, 1, and 2 respectively; SInt = 3 could not be identified in healthy tissues.
- E-cadherin: cardiac myocytes, epithelial cells of the small intestine, epithelial cells of prostate represented SInt 0, 2, and 3 respectively; healthy tissues representing SInt = 1 could not be identified.
- PARP1: mucosa of the small intestine, cardiac myocytes, and germinal basal cells of testis represented SInt 0, 1, and 2 respectively; healthy tissues representing SFreq = 3 could not be identified.
- Slug: cardiac myocytes, smooth muscle of the appendix, and lymphocytes of the small intestine represented SInt 0, 1, and 2 respectively; healthy tissues representing SInt = 3 could not be identified.
- HA: Intensity for hyaluronan was measured as blue color intensity developed by Alcian blue in comparison to hyaluronidase digested tissue section. Sub-mucosa of the small intestine and cartilage tissues represented SInt 1 and 2 respectively; healthy tissues representing SInt = 0 or 3 could not be identified.
- ANXA2: cardiac myocytes and epithelial cells of gall bladder represented SInt 0 and 2 respectively; healthy tissues representing SInt = 1 or 3 could not be identified.
- (iii)
- Score for Marker Localization (SLoc)-representing sub-cellular location of marker in the tissue section on a scale of 0–2, 0: Absent, 1: mislocalized (cellular localization does not correspond to known functionality, for example, cytoplasmic location for TCF21, PARP1, Slug, E-cadherin, ANXA2 or HA), 2: normal localization (for example, nuclear expression of TCF21, PARP1 or Slug, membrane for E-cadherin, membrane or cytoplasmic for ANXA2 and extracellular expression of HA.
- TCF21: cardiac myocytes, liver hepatocytes, germinal basal cells of testis represented SLoc 0, 1, and 2 respectively.
- E-cadherin: cardiac myocytes, prostate epithelial cells represented SLoc 0 and 2 respectively; healthy tissues representing SLoc = 1 could not be identified.
- PARP1: mucosa of the small intestine, germinal basal cells of testis represented SLoc 0 and 2 respectively; healthy tissues representing SLoc = 1 could not be identified.
- Slug: cardiac myocytes, the somatic muscle of the appendix, lymphocytes of the small intestine, represented SLoc 0, 1, and 2 respectively.
- HA: cartilage represented SLoc of score 2; healthy tissues representing SLoc = 1 could not be identified. A further consensus was reached in the pathology review to consider extracellular staining in tumor nests that is eliminated following hyaluronidase treatment as a proper localization, while distant stroma-associated HA was considered as mislocalization.
- ANXA2: cardiac myocytes, stromal cells of the gall bladder, epithelial cells of the gall bladder represented SLoc as 0, 1, and 2 respectively.
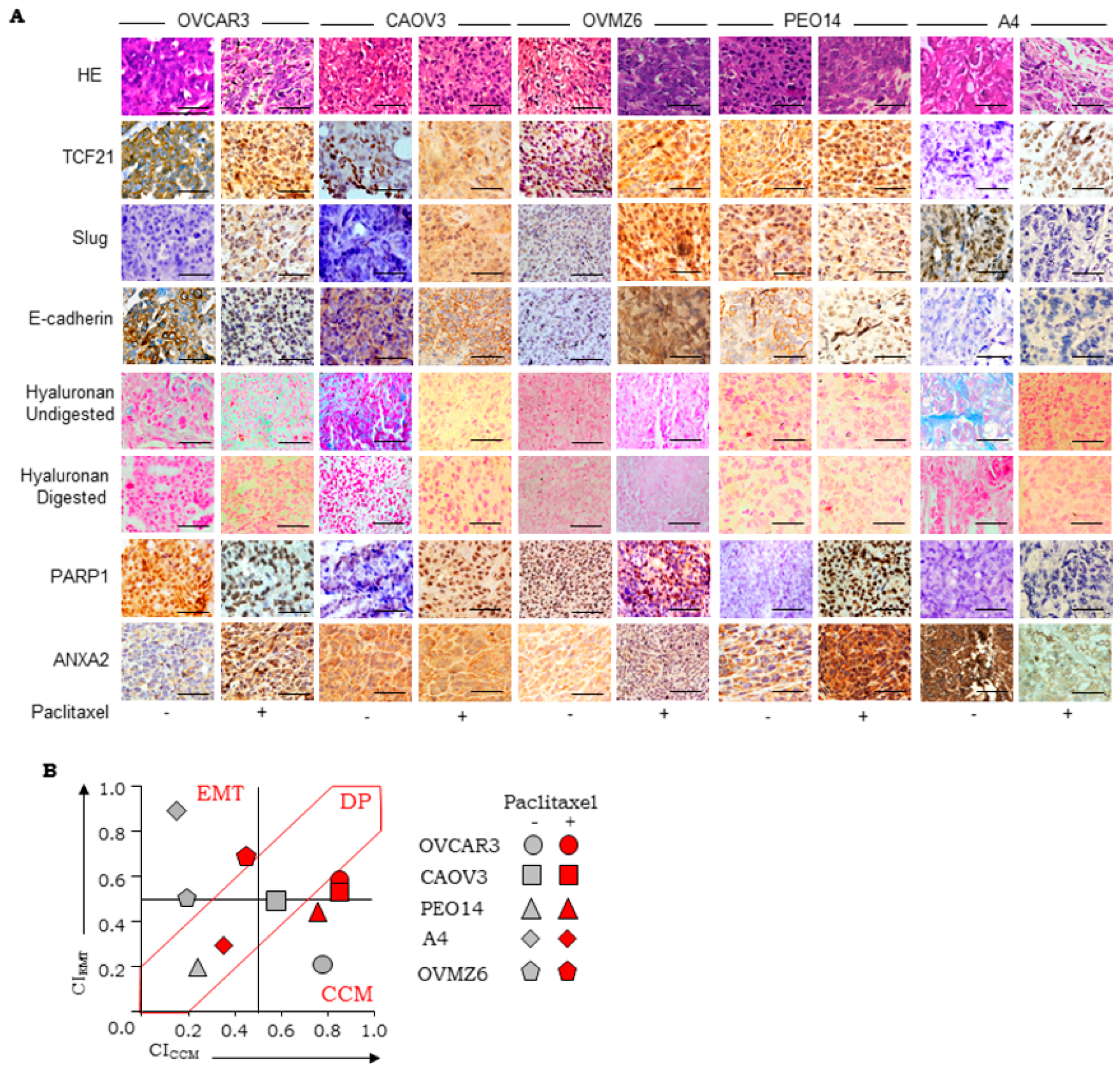
3.2. Establishment of Scoring Guidelines for Stratification Using a Panel of Xenograft
3.3. Evaluation of Stratification Guidelines in TMAs
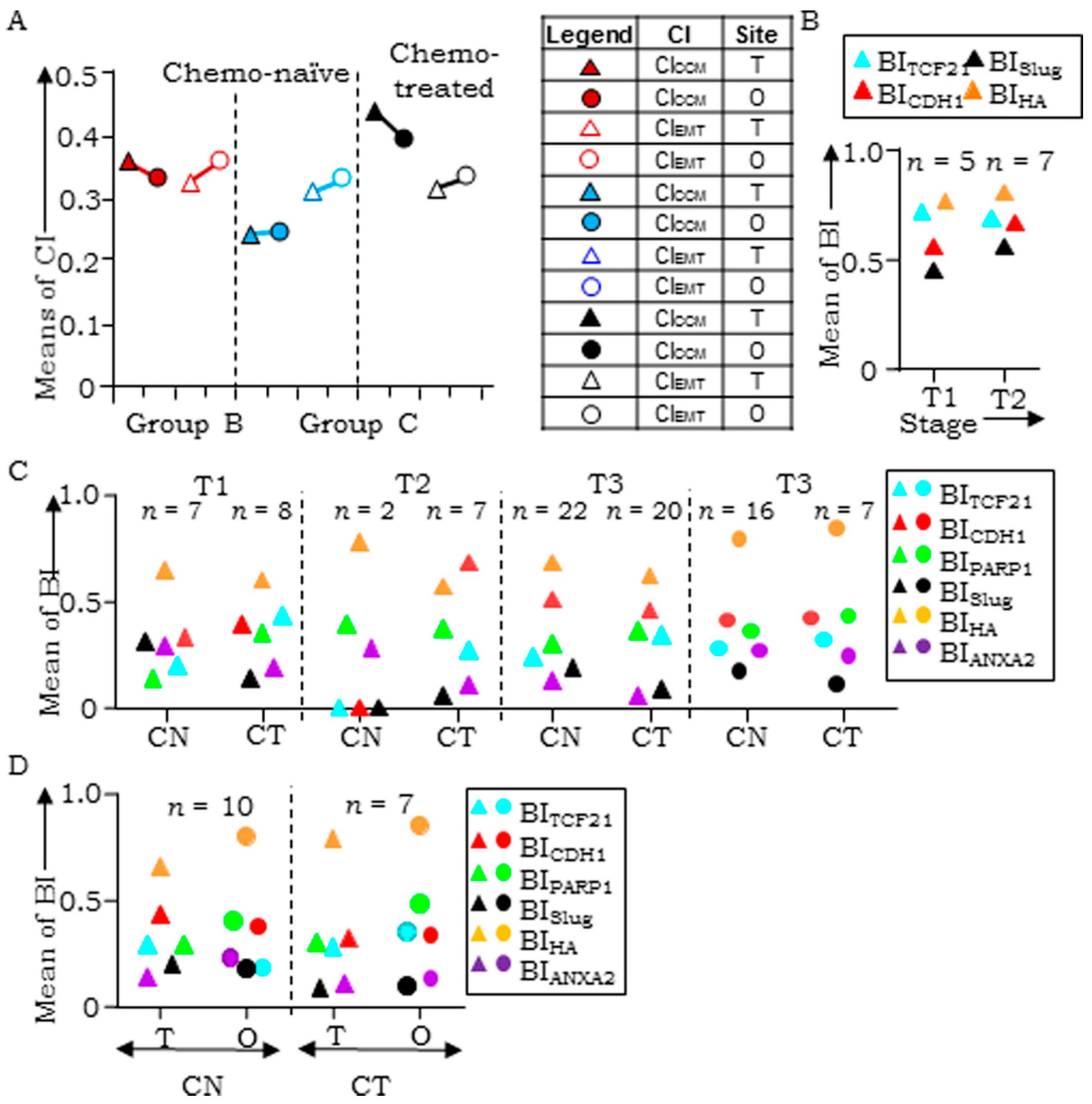
3.4. Evaluation of Clinical Samples Associates CCM-Markers with Metastases and Chemotherapy
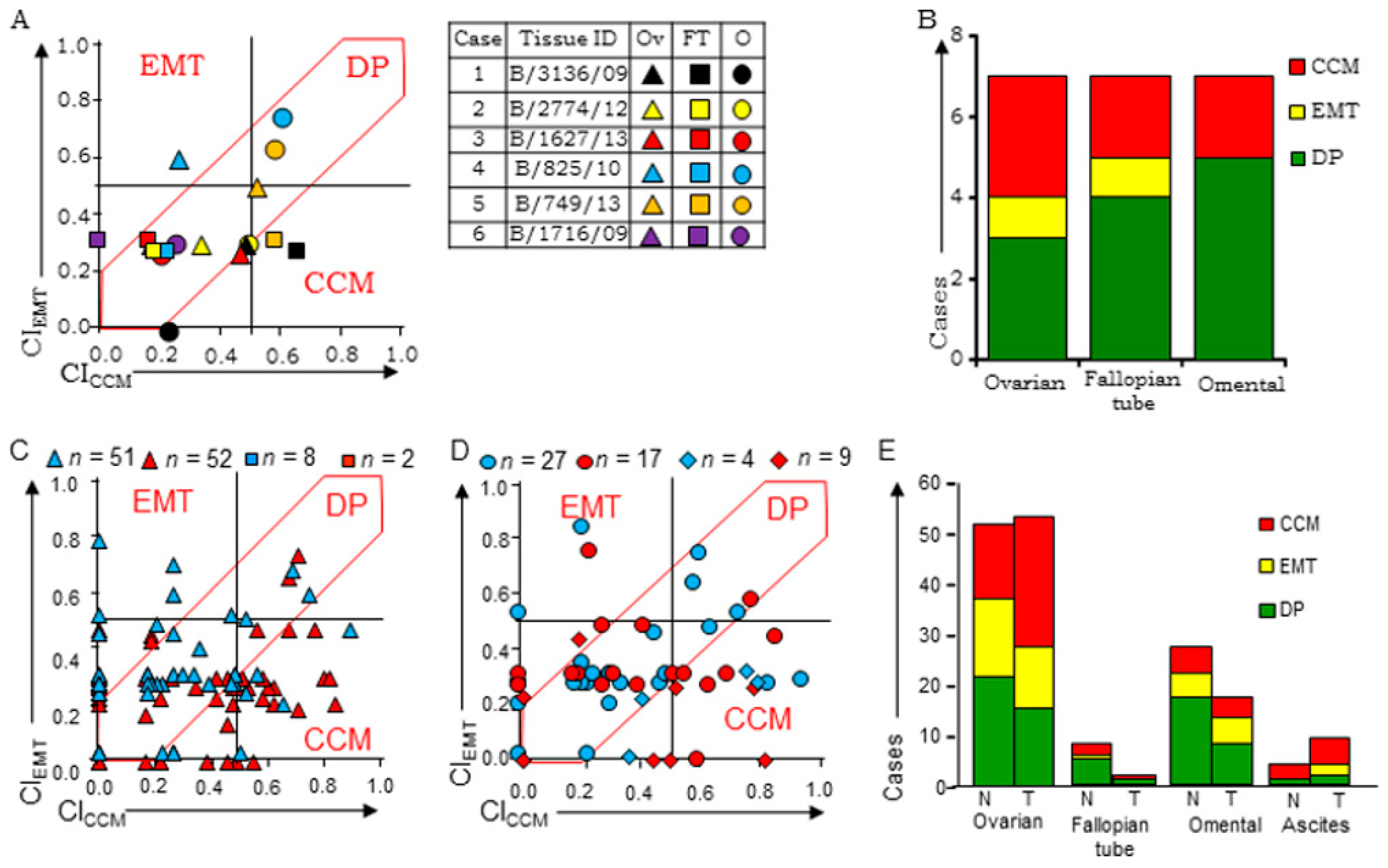
3.5. HGSC Tumors at Different Sites Exhibit Molecular Heterogeneity and Class-Switching
3.6. Disease Progression is Inclined Towards Enrichment of CCM-Markers
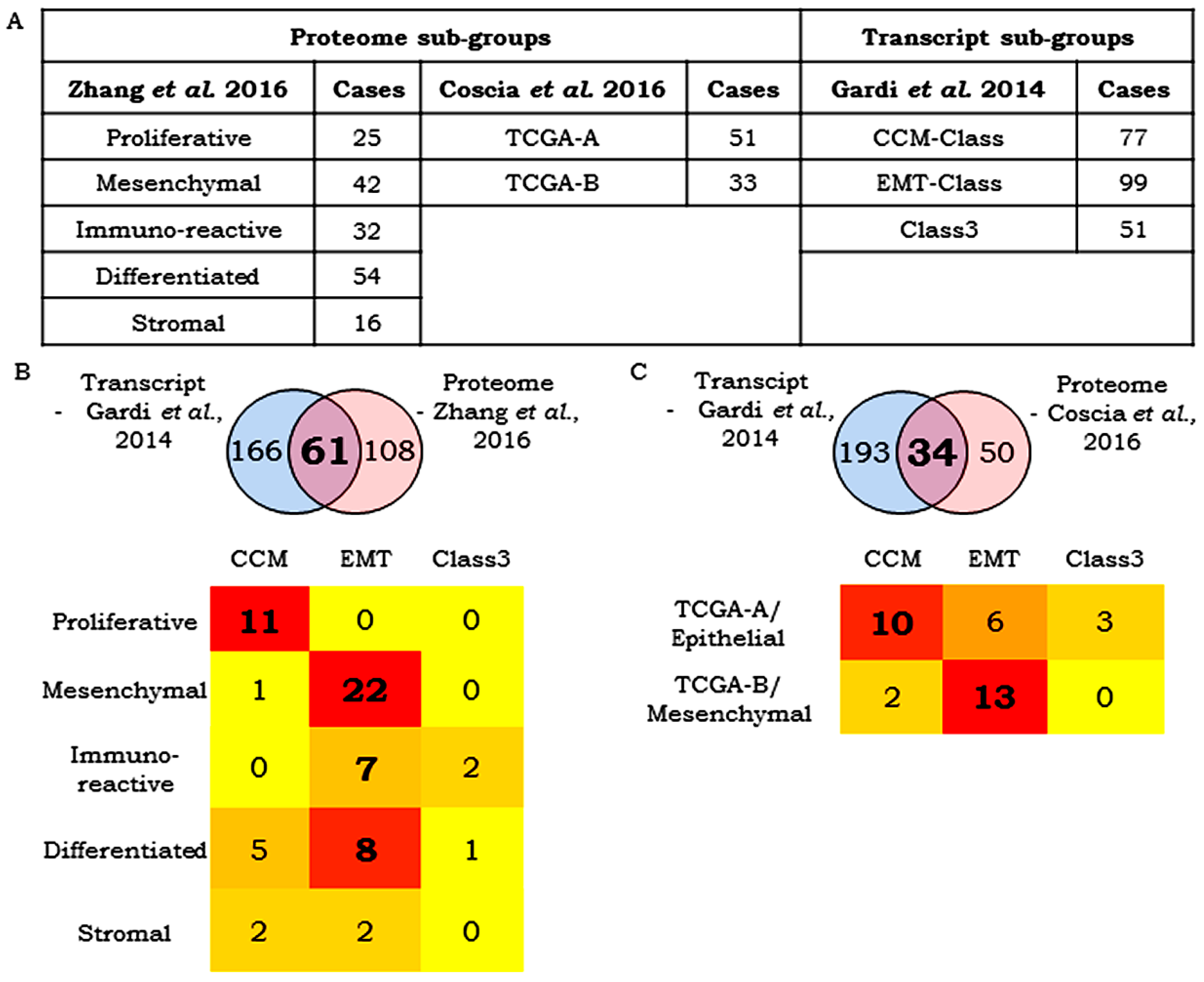
3.7. Correlation Between Transcript- and Protein-Based Stratification
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Weigelt, B.; Reis-Filho, J.S.; Swanton, C. Genomic analyses to select patients for adjuvant chemotherapy: Trials and tribulations. Ann. Oncol. 2012, 23, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Bass, A.J.; Thorsson, V.; Shmulevich, I.; Reynolds, S.M.; Miller, M.; Bernard, B.; Hinoue, T.; Laird, P.W.; Curtis, C.; Shen, H.; et al. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorgun, G.; Calabrese, E.; Hideshima, T.; Ecsedy, J.; Perrone, G.; Mani, M.; Ikeda, H.; Bianchi, G.; Hu, Y.; Cirstea, D.; et al. A novel aurora-A kinase inhibitor MLN8237 induces cytotoxicity and cell cycle arrest in multiple experimental multiple myeloma model. Blood 2010, 115, 5202–5213. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, M.G.; Ecsedy, J.A.; Chakravarty, A.; Silverman, L.; Zhang, M.; Hoar, K.M.; Stroud, S.G.; Chen, W.; Shinde, V.; Huck, J.J.; et al. Characterization of alisertib (MLN8237), an investigational small-molecule inhibitor of Aurora A kinase using novel in vivo pharmacodynamic assays. Clin. Cancer Res. 2011, 17, 7614–7624. [Google Scholar] [CrossRef] [PubMed]
- Cidon, E.U.; Ellis, S.G.; Inam, Y.; Adeleke, S.; Zarif, S.; Geldart, T. Molecular targeted agents for gastric cancer: A step forward towards personalized therapy. Cancers 2013, 5, 64–91. [Google Scholar] [CrossRef] [PubMed]
- Muro, K.; Chung, H.C.; Shankaran, V.; Geva, R.; Catenacci, D.; Gupta, S.; Eder, J.P.; Golan, T.; Le, D.T.; Burtness, B.; et al. Pembrolizumab for patients with PD-L1-positive advanced gastric cancer (KEYNOTE-012): A multicentre, open-label, phase 1b trial. Lancet Oncol. 2016, 17, 717–726. [Google Scholar] [CrossRef]
- Magaki, S.; Hojat, S.A.; Wei, B.; So, A.; Yong, W.H. An Introduction to the Performance of Immunohistochemistry. In Biobanking. Methods in Molecular Biology; Humana Press: New York, NY, USA, 2019; pp. 289–298. [Google Scholar]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.-M.; Ting, J.C.; Wong, S.S.; Liu, J.; Yue, Y.G.; Wang, J.; Yu, K.; et al. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef]
- Díaz del Arco, C.; Estrada Muñoz, L.; Molina Roldán, E.; Cerón Nieto, M.Á.; Ortega Medina, L.; García Gómez de las Heras, S.; Fernández Aceñero, M.J. Immunohistochemical classification of gastric cancer based on new molecular biomarkers: A potential predictor of survival. Virchows Arch. 2018, 473, 687–695. [Google Scholar] [CrossRef]
- Kim, J.; Kong, J.K.; Yang, W.; Cho, H.; Chay, D.B.; Lee, B.H.; Cho, S.J.; Hong, S.; Kim, J.-H. DNA Mismatch Repair Protein Immunohistochemistry and MLH1 Promotor Methylation Testing for Practical Molecular Classification and the Prediction of Prognosis in Endometrial Cancer. Cancers 2018, 10, 279. [Google Scholar] [CrossRef]
- Karnezis, A.N.; Leung, S.; Magrill, J.; McConechy, M.K.; Yang, W.; Chow, C.; Kobel, M.; Lee, C.-H.; Huntsman, D.G.; Talhouk, A.; et al. Evaluation of endometrial carcinoma prognostic immunohistochemistry markers in the context of molecular classification. J. Pathol. Clin. Res. 2017, 3, 279–293. [Google Scholar] [CrossRef] [Green Version]
- Ten Hoorn, S.; Trinh, A.; de Jong, J.; Koens, L.; Vermeulen, L. Classification of Colorectal Cancer in Molecular Subtypes by Immunohistochemistry. In Methods in molecular biology (Clifton, N.J.); Beaulieu, J.-F., Ed.; Humana Press: New York, NY, USA, 2018. [Google Scholar]
- Kim, S.; Moon, B.-I.; Lim, W.; Park, S.; Cho, M.S.; Sung, S.H. Feasibility of Classification of Triple Negative Breast Cancer by Immunohistochemical Surrogate Markers. Clin. Breast Cancer 2018, 18, e1123–e1132. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wu, Y.; Ma, K.; Fan, Y.; Dong, D.; Geng, N.; Li, E. Molecular classification of esophagogastric junction carcinoma correlated with prognosis. Onco. Targets. Ther. 2017, 10, 4765–4772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilie, M.; Beaulande, M.; Hamila, M.; Erb, G.; Hofman, V.; Hofman, P. Automated chromogenic multiplexed immunohistochemistry assay for diagnosis and predictive biomarker testing in non-small cell lung cancer. Lung Cancer 2018, 124, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA. Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Bast, R.C.; Hennessy, B.; Mills, G.B. The biology of ovarian cancer: New opportunities for translation. Nat. Rev. Cancer 2009, 9, 415–428. [Google Scholar] [CrossRef] [PubMed]
- Yap, T.A.; Carden, C.P.; Kaye, S.B. Beyond chemotherapy: Targeted therapies in ovarian cancer. Nat. Rev. Cancer 2009, 9, 167–181. [Google Scholar] [CrossRef] [PubMed]
- Tothill, R.W.; Tinker, A.V.; George, J.; Brown, R.; Fox, S.B.; Lade, S.; Johnson, D.S.; Trivett, M.K.; Etemadmoghadam, D.; Locandro, B.; et al. Novel Molecular Subtypes of Serous and Endometrioid Ovarian Cancer Linked to Clinical Outcome. Clin. Cancer Res. 2008, 14, 5198–5208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- TCGA Network; Bell, D.; Berchuck, A.; Birrer, M.; Chien, J.; Cramer, D.W.; Dao, F.; Dhir, R.; DiSaia, P.; Gabra, H.; et al. Integrated genomic analyses of ovarian carcinoma. Nature 2011, 474, 609–615. [Google Scholar] [CrossRef] [Green Version]
- Yang, D.; Sun, Y.; Hu, L.; Zheng, H.; Ji, P.; Pecot, C.V.; Zhao, Y.; Reynolds, S.; Cheng, H.; Rupaimoole, R.; et al. Integrated Analyses Identify a Master MicroRNA Regulatory Network for the Mesenchymal Subtype in Serous Ovarian Cancer. Cancer Cell 2013, 23, 186–199. [Google Scholar] [CrossRef] [Green Version]
- Hoadley, K.A.; Yau, C.; Wolf, D.M.; Cherniack, A.D.; Tamborero, D.; Ng, S.; Leiserson, M.D.M.; Niu, B.; McLellan, M.D.; Uzunangelov, V.; et al. Multiplatform Analysis of 12 Cancer Types Reveals Molecular Classification within and across Tissues of Origin. Cell 2014, 158, 929–944. [Google Scholar] [CrossRef] [Green Version]
- Kanchi, K.L.; Johnson, K.J.; Lu, C.; McLellan, M.D.; Leiserson, M.D.M.; Wendl, M.C.; Zhang, Q.; Koboldt, D.C.; Xie, M.; Kandoth, C.; et al. Integrated analysis of germline and somatic variants in ovarian cancer. Nat. Commun. 2014, 5, 3156. [Google Scholar] [CrossRef] [PubMed]
- Gardi, N.L.; Deshpande, T.U.; Kamble, S.C.; Budhe, S.R.; Bapat, S.A. Discrete molecular classes of ovarian cancer suggestive of unique mechanisms of transformation and metastases. Clin. Cancer Res. 2014, 20, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Uhlen, M.; Fagerberg, L.; Hallstrom, B.M.; Lindskog, C.; Oksvold, P.; Mardinoglu, A.; Sivertsson, A.; Kampf, C.; Sjostedt, E.; Asplund, A.; et al. Tissue-based map of the human proteome. Science 2015, 347, 1260419. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Liu, T.; Zhang, Z.; Chan, D.W.; Rodland, K.D.; Zhang, H.; Liu, T.; Zhang, Z.; Payne, S.H.; Zhang, B.; et al. Integrated Proteogenomic Characterization of Human High-Grade Serous Ovarian Cancer. Cell 2016, 166, 755–765. [Google Scholar] [CrossRef] [PubMed]
- Coscia, F.; Watters, K.M.; Curtis, M.; Eckert, M.A.; Chiang, C.Y.; Tyanova, S.; Montag, A.; Lastra, R.R.; Lengyel, E.; Mann, M. Integrative proteomic profiling of ovarian cancer cell lines reveals precursor cell associated proteins and functional status. Nat. Commun. 2016, 7, 12645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winget, M.D.; Baron, J.A.; Spitz, M.R.; Brenner, D.E.; Warzel, D.; Kincaid, H.; Thornquist, M.; Feng, Z. Development of common data elements: The experience of and recommendations from the early detection research network. Int. J. Med. Inform. 2003, 70, 41–48. [Google Scholar] [CrossRef]
- Shariat, S.; Lotan, Y.; Vickers, A.; Karakiewicz, P.; Schmitz-Dräger, B.; Goebell, P.; Malats, N. Statistical consideration for clinical biomarker research in bladder cancer. Urol. Oncol. 2010, 28, 389–400. [Google Scholar] [CrossRef] [Green Version]
- Kothe, S.; Muller, J.; Bohmer, S.-A.; Tschongov, T.; Fricke, M.; Koch, S.; Thiede, C.; Requardt, R.P.; Rubio, I.; Bohmer, F.D. Features of Ras activation by a mislocalized oncogenic tyrosine kinase: FLT3 ITD signals through K-Ras at the plasma membrane of acute myeloid leukemia cells. J. Cell Sci. 2013, 126, 4746–4755. [Google Scholar] [CrossRef] [Green Version]
- Barham, W.; Chen, L.; Tikhomirov, O.; Onishko, H.; Gleaves, L.; Stricker, T.P.; Blackwell, T.S.; Yull, F.E. Aberrant activation of NF-κB signaling in mammary epithelium leads to abnormal growth and ductal carcinoma in situ. BMC Cancer 2015, 1–17. [Google Scholar] [CrossRef]
- Guttilla, I.K.; Phoenix, K.N.; Hong, X.; Tirnauer, J.S.; Claffey, K.P.; White, B.A. Prolonged mammosphere culture of MCF-7 cells induces an EMT and repression of the estrogen receptor by microRNAs. Breast Cancer Res. Treat. 2012, 132, 75–85. [Google Scholar] [CrossRef]
- Sidney, L.E.; McIntosh, O.D.; Hopkinson, A. Phenotypic change and induction of cytokeratin expression during in vitro culture of corneal stromal cells. Investig. Ophthalmol. Vis. Sci. 2015, 56, 7225–7235. [Google Scholar] [CrossRef] [PubMed]
- Jolly, M.K.; Tripathi, S.C.; Jia, D.; Mooney, S.M.; Celiktas, M.; Hanash, S.M.; Mani, S.A.; Pienta, K.J.; Ben-Jacob, E.; Levine, H. Stability of the hybrid epithelial/mesenchymal phenotype. Oncotarget 2016, 7, 27067–27084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, R.Y.; Antony, J.; Tan, T.Z.; Tan, D.S. Targeting the AXL signaling pathway in ovarian cancer. Mol. Cell Oncol. 2016, 4, e1263716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smigiel, J.M.; Parameswaran, N.; Jackson, M.W. Targeting Pancreatic Cancer Cell Plasticity: The Latest in Therapeutics. Cancers 2018, 10, 14. [Google Scholar] [CrossRef] [PubMed]
- Banyard, J.; Chung, I.; Wilson, A.M.; Vetter, G.; Le Béchec, A.; Bielenberg, D.R.; Zetter, B.R. Regulation of epithelial plasticity by miR-424 and miR-200 in a new prostate cancer metastasis model. Sci. Rep. 2013, 3, 3151. [Google Scholar] [CrossRef] [PubMed]
- Quagliata, L.; Schlageter, M.; Quintavalle, C.; Tornillo, L.; Terracciano, L. Identification of New Players in Hepatocarcinogenesis: Limits and Opportunities of Using Tissue Microarray (TMA). Microarrays 2014, 3, 91–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ku, M.; Kang, M.; Suh, J.; Yang, J. Effects for Sequential Treatment of siAkt and Paclitaxel on Gastric Cancer Cell Lines. Int. J. Med. Sci. 2016, 13, 708–716. [Google Scholar] [CrossRef] [Green Version]
- Su, H.; Lin, F.; Deng, X.; Shen, L.; Fang, Y.; Fei, Z.; Zhao, L.; Zhang, X.; Pan, H.; Xie, D.; et al. Profiling and bioinformatics analyses reveal differential circular RNA expression in radioresistant esophageal cancer cells. J. Transl. Med. 2016, 14, 225. [Google Scholar] [CrossRef]
- Litviakov, N.V.; Cherdyntseva, N.V.; Tsyganov, M.M.; Slonimskaya, E.M.; Ibragimova, M.K.; Kazantseva, P.V.; Kzhyshkowska, J.; Choinzonov, E.L. Deletions of multidrug resistance gene loci in breast cancer leads to the down-regulation of its expression and predict tumor response to neoadjuvant chemotherapy. Oncotarget 2016, 5, 7829–7841. [Google Scholar] [CrossRef]
- Negrei, C.; Hudita, A.; Ginghina, O.; Galateanu, B.; Voicu, S.N.; Stan, M.; Costache, M.; Fenga, C.; Drakoulis, N.; Tsatsakis, A.M. Colon Cancer Cells Gene Expression Signature As Response to 5-Fluorouracil, Oxaliplatin, and Folinic Acid Treatment. Front. Pharmacol. 2016, 7, 172. [Google Scholar] [CrossRef]
- Bjarnadottir, O.; Kimbung, S.; Johansson, I.; Veerla, S.; Jönsson, M.; Bendahl, P.-O.; Grabau, D.; Hedenfalk, I.; Borgquist, S. Global Transcriptional Changes Following Statin Treatment in Breast Cancer. Clin. Cancer Res. 2015, 21, 3402–3411. [Google Scholar] [CrossRef] [PubMed]
- Chiu, J.W.; Hotte, S.J.; Kollmannsberger, C.K.; Renouf, D.J.; Cescon, D.W.; Hedley, D.; Chow, S.; Moscow, J.; Chen, Z.; Perry, M.; et al. A phase I trial of ANG1/2-Tie2 inhibitor trebaninib (AMG386) and temsirolimus in advanced solid tumors (PJC008/NCI#9041). Invest. New Drugs 2016, 34, 104–111. [Google Scholar] [PubMed]
- Kim, G.; Ison, G.; McKee, A.E.; Zhang, H.; Tang, S.; Gwise, T.; Sridhara, R.; Lee, E.; Tzou, A.; Philip, R.; et al. FDA Approval Summary: Olaparib Monotherapy in Patients with Deleterious Germline BRCA-Mutated Advanced Ovarian Cancer Treated with Three or More Lines of Chemotherapy. Clin. Cancer Res. 2015, 21, 4257–4261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlHilli, M.M.; Becker, M.A.; Weroha, S.J.; Flatten, K.S.; Hurley, R.M.; Harrell, M.I.; Oberg, A.L.; Maurer, M.J.; Hawthorne, K.M.; Hou, X.; et al. In vivo anti-tumor activity of the PARP inhibitor niraparib in homologous recombination deficient and proficient ovarian carcinoma. Gynecol. Oncol. 2016, 143, 379–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ke, Z.; Caiping, S.; Qing, Z.; Xiaojing, W. Sonic hedgehog-Gli1 signals promote epithelial-mesenchymal transition in ovarian cancer by mediating PI3K/AKT pathway. Med. Oncol. 2015, 32, 368. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, Y.H.; García-García, C.; Serra, V.; He, L.; Torres-Lockhart, K.; Prat, A.; Anton, P.; Cozar, P.; Guzmán, M.; Grueso, J.; et al. PI3K inhibition impairs BRCA1/2 expression and sensitizes BRCA-proficient triple-negative breast cancer to PARP inhibition. Cancer Discov. 2012, 2, 1036–1047. [Google Scholar] [CrossRef] [PubMed]
- Juvekar, A.; Burga, L.N.; Hu, H.; Lunsford, E.P.; Ibrahim, Y.H.; Balmañà, J.; Rajendran, A.; Papa, A.; Spencer, K.; Lyssiotis, C.A.; et al. Combining a PI3K inhibitor with a PARP inhibitor provides an effective therapy for BRCA1-related breast cancer. Cancer Discov. 2012, 2, 1048–1063. [Google Scholar] [CrossRef] [PubMed]
- González-Billalabeitia, E.; Seitzer, N.; Song, S.J.; Song, M.S.; Patnaik, A.; Liu, X.-S.; Epping, M.T.; Papa, A.; Hobbs, R.M.; Chen, M.; et al. Vulnerabilities of PTEN-TP53-deficient prostate cancers to compound PARP-PI3K inhibition. Cancer Discov. 2014, 4, 896–904. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Li, C.; Zhang, Y.; Wang, M.; Jiang, N.; Xiang, L.; Li, T.; Roberts, T.M.; Zhao, J.J.; Cheng, H.; et al. Combined inhibition of PI3K and PARP is effective in the treatment of ovarian cancer cells with wild-type PIK3CA genes. Gynecol. Oncol. 2016, 142, 548–556. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CCM Markers | |||||||||||||
| Cell Line Derived Xenograft | TCF21 | E-cadherin | PARP1 | CICCM | |||||||||
| SFreq | SInt | SLoc | BITCF21 | SFreq | SInt | SLoc | BICDH1 | SFreq | SInt | SLoc | BIPARP1 | ||
| CAOV3 | 2 | 2 | 2 | 0.78 | 3 | 2 | 2 | 0.89 | 0 | 0 | 0 | 0 | 0.56 |
| OVMZ6 | 2 | 1 | 1 | 0.5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0.17 |
| CP70 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| OV90 | 2 | 1 | 1 | 0.5 | 1 | 2 | 1 | 0.5 | 0 | 0 | 0 | 0 | 0.17 |
| A4 | 1 | 1 | 1 | 0.39 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0.13 |
| OVCAR3 | 2 | 3 | 1 | 0.72 | 2 | 2 | 2 | 0.78 | 2 | 2 | 2 | 0.78 | 0.76 |
| PEO14 | 1 | 2 | 2 | 0.67 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0.22 |
| EMT Markers | |||||||||||||
| Cell Line Derived Xenograft | Slug | HA | ANXA2 | CIEMT | |||||||||
| SFreq | SInt | SLoc | BISlug | SFreq | SInt | SLoc | BIHA | SFreq | SInt | SLoc | BIAnxA2 | ||
| CAOV3 | 3 | 1 | 1 | 0.61 | 3 | 2 | 2 | 0.89 | 0 | 0 | 0 | 0 | 0.5 |
| OVMZ6 | 2 | 1 | 2 | 0.67 | 0 | 0 | 0 | 0 | 3 | 2 | 2 | 0.89 | 0.52 |
| CP70 | 1 | 1 | 1 | 0.39 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0.13 |
| OV90 | 1 | 1 | 2 | 0.56 | 3 | 3 | 2 | 1 | 0 | 0 | 0 | 0 | 0.52 |
| A4 | 3 | 3 | 2 | 1 | 3 | 2 | 2 | 0.89 | 3 | 1 | 2 | 0.78 | 0.89 |
| OVCAR3 | 0 | 0 | 0 | 0 | 2 | 1 | 2 | 0.67 | 0 | 0 | 0 | 0 | 0.22 |
| PEO14 | 0 | 0 | 0 | 0 | 2 | 1 | 2 | 0.67 | 0 | 0 | 0 | 0 | 0.22 |
| Group | Analyses | Samples (n) |
|---|---|---|
| A | Between-group analyses of tumors in chemo-naïve tumors (T vs. FT vs. O) | 6 |
| B | Within the group of single tumors derived from either ovarian or FT sites, omental deposits or cell blocks from tumor ascites in chemo-naïve (CN) cases and chemo-treated (CT) cases | CN–51 (T), 8 (FT), 27 (O), 4 (A); CT–52 (T), 2 (FT), 17 (O), 2 (A) |
| C | Within groups of primary tumor & omental tumors pairs from either chemo-naïve (CN) or chemo-treated (CT) cases | CN–17; CT–16 |
| D | Between-group analyses of tumor samples of the same case before and after chemotherapy | 6 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamble, S.C.; Sen, A.; Dhake, R.D.; Joshi, A.N.; Midha, D.; Bapat, S.A. Clinical Stratification of High-Grade Ovarian Serous Carcinoma Using a Panel of Six Biomarkers. J. Clin. Med. 2019, 8, 330. https://doi.org/10.3390/jcm8030330
Kamble SC, Sen A, Dhake RD, Joshi AN, Midha D, Bapat SA. Clinical Stratification of High-Grade Ovarian Serous Carcinoma Using a Panel of Six Biomarkers. Journal of Clinical Medicine. 2019; 8(3):330. https://doi.org/10.3390/jcm8030330
Chicago/Turabian StyleKamble, Swapnil C., Arijit Sen, Rahul D. Dhake, Aparna N. Joshi, Divya Midha, and Sharmila A. Bapat. 2019. "Clinical Stratification of High-Grade Ovarian Serous Carcinoma Using a Panel of Six Biomarkers" Journal of Clinical Medicine 8, no. 3: 330. https://doi.org/10.3390/jcm8030330
APA StyleKamble, S. C., Sen, A., Dhake, R. D., Joshi, A. N., Midha, D., & Bapat, S. A. (2019). Clinical Stratification of High-Grade Ovarian Serous Carcinoma Using a Panel of Six Biomarkers. Journal of Clinical Medicine, 8(3), 330. https://doi.org/10.3390/jcm8030330