New Generation Cardiac Contractility Modulation Device—Filling the Gap in Heart Failure Treatment

Abstract
:1. Introduction
2. Experimental Section
3. Results
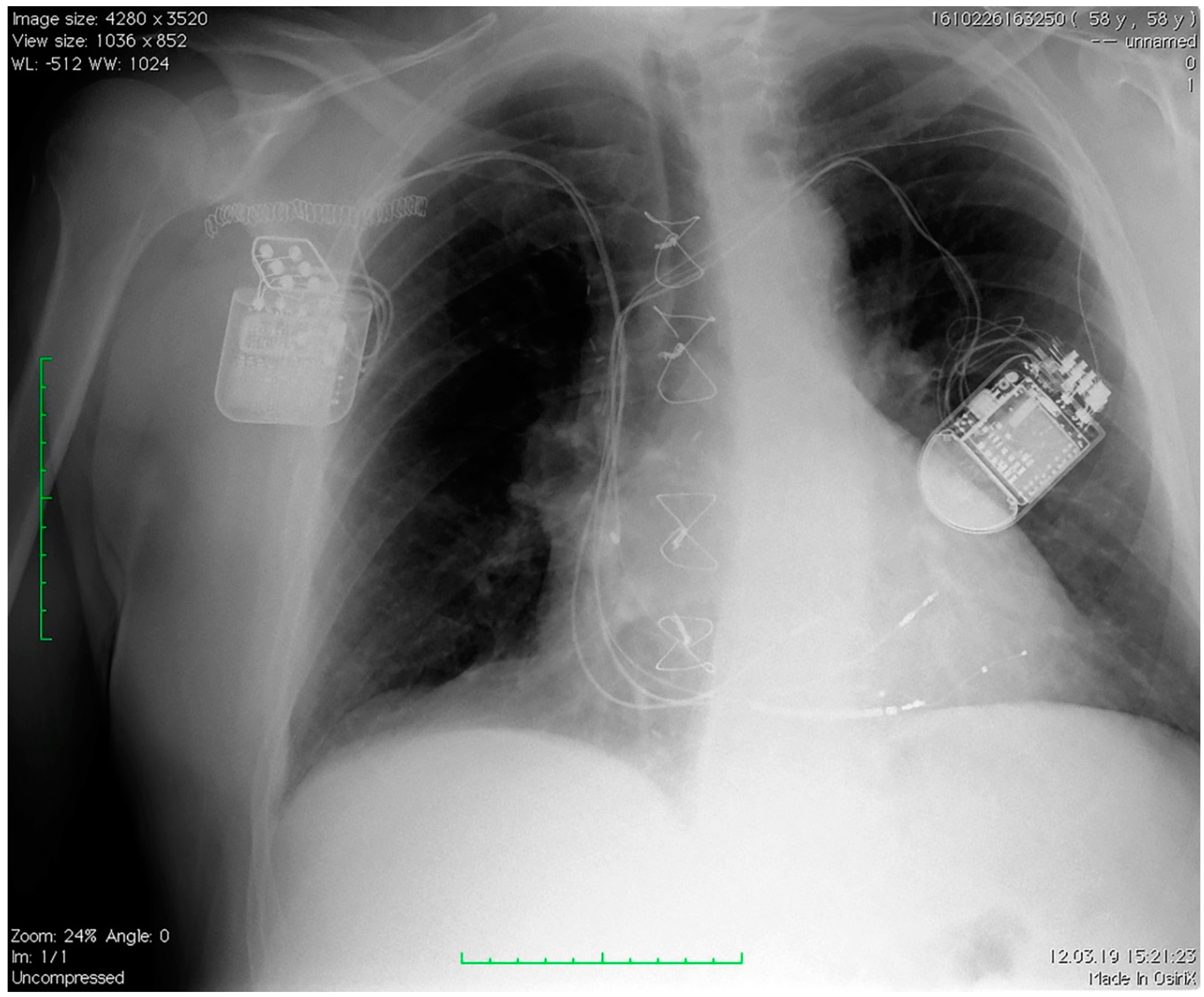
3.1. CCM and Interaction with Other Devices
3.2. Outcome
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Conflicts of Interest
References
- Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Moss, A.J.; Zareba, W.; Hall, W.J.; Klein, H.; Wilber, D.J.; Cannom, D.S.; Daubert, J.P.; Higgins, S.L.; Brown, M.W.; Andrews, M.L. Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. New Engl. J. Med. 2002, 346, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Bardy, G.H.; Lee, K.L.; Mark, D.B.; Poole, J.E.; Packer, D.L.; Boineau, R.; Domanski, M.; Troutman, C.; Anderson, J.; Johnson, G.; et al. Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators. Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. New Engl. J. Med. 2005, 352, 225–237. [Google Scholar] [CrossRef]
- Bristow, M.R.; Saxon, L.A.; Boehmer, J.; Krueger, S.; Kass, D.A.; De Marco, T.; Carson, P.; DiCarlo, L.; DeMets, D.; White, B.G.; et al. Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure (COMPANION) Investigators. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. New Engl. J. Med. 2004, 350, 2140–2150. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.G.; Daubert, J.-C.; Erdmann, E.; Freemantle, N.; Gras, D.; Kappenberger, L.; Tavazzi, L. The Effect of Cardiac Resynchronization on Morbidity and Mortality in Heart Failure. New Engl. J. Med. 2005, 352, 1539–1549. [Google Scholar] [CrossRef] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef]
- Lund, L.H.; Jurga, J.; Edner, M.; Benson, L.; Dahlström, U.; Linde, C.; Alehagen, U. Prevalence, correlates, and prognostic significance of QRS prolongation in heart failure with reduced and preserved ejection fraction. Eur. Heart J. Fail. 2013, 34, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Linde, C.; Ellenbogen, K.; McAlister, F.A. Cardiac resynchronization therapy (CRT): Clinical trials, guidelines, and target populations. Hear. Rhythm. 2012, 9, S3–S13. [Google Scholar] [CrossRef]
- Hawkins, N.M.; Petrie, M.C.; Macdonald, M.R.; Hogg, K.J.; McMurray, J.J. Selecting patients for cardiac resynchronization therapy: electrical or mechanical dyssynchrony? Eur. Hear. J. 2006, 27, 1270–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birnie, D.H.; Tang, A.S. The problem of non-response to cardiac resynchronization therapy. Curr. Opin. Cardiol. 2006, 21, 20–26. [Google Scholar] [CrossRef]
- Lyon, A.R.; Samara, M.A.; Feldman, D.S. Cardiac contractility modulation therapy in advanced systolic heart failure. Nat. Rev. Cardiol. 2013, 10, 584–598. [Google Scholar] [CrossRef]
- Butter, C.; Rastogi, S.; Minden, H.-H.; Meyhöfer, J.; Burkhoff, D.; Sabbah, H.N. Cardiac Contractility Modulation Electrical Signals Improve Myocardial Gene Expression in Patients With Heart Failure. J. Am. Cardiol. 2008, 51, 1784–1789. [Google Scholar] [CrossRef] [Green Version]
- Gupta, R.C.; Mishra, S.; Rastogi, S.; Wang, M.; Rousso, B.; Mika, Y.; Remppis, A.; Sabbah, H.N. Ca(2+)-binding proteins in dogs with heart failure: effects of cardiac contractility modulation electrical signals. Clin. Transl. Sci. 2009, 2, 211–215. [Google Scholar] [CrossRef]
- Remppis, A.; Greten, T.; Schafer, B.W.; Hunziker, P.; Erne, P.; Katus, H.A.; Heizmann, C.W. Altered expression of the Ca(2+)-binding protein S100A1 in human cardiomyopathy. Biochim. Biophys. Acta. 1996, 1313, 253–257. [Google Scholar] [CrossRef]
- Stix, G.; Borggrefe, M.; Wolpert, C.; Hindricks, G.; Kottkamp, H.; Böcker, D.; Wichter, T.; Mika, Y.; Ben-Haim, S.; Burkhoff, D.; et al. Chronic electrical stimulation during the absolute refractory period of the myocardium improves severe heart failure. Eur. Hear. J. 2004, 25, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Borggrefe, M.M.; Lawo, T.; Butter, C.; Schmidinger, H.; Lunati, M.; Pieske, B.; Misier, A.R.; Curnis, A.; Böcker, D.; Remppis, A.; et al. Randomized, double blind study of non-excitatory, cardiac contractility modulation electrical impulses for symptomatic heart failure. Eur. Hear. J. 2008, 29, 1019–1028. [Google Scholar] [CrossRef] [Green Version]
- Kadish, A.; Nademanee, K.; Volosin, K.; Krueger, S.; Neelagaru, S.; Raval, N.; Obel, O.; Weiner, S.; Wish, M.; Carson, P.; et al. A randomized controlled trial evaluating the safety and efficacy of cardiac contractility modulation in advanced heart failure. Am. Hear. J. 2011, 161, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T.; Lindenfeld, J.; Reddy, V.Y.; Hasenfuss, G.; Kuck, K.H.; Boscardin, J.; Gibbons, R.; Burkhoff, D.; FIX-HF-5C Investigators and Coordinators. A randomized controlled trial to evaluate the efficacy and safety of cardiac contractility modulation in patients with moderately reduced left ventricular ejection fraction and a narrow QRs duration: study rationale and design. J. Card. Fail. 2015, 21, 16–23. [Google Scholar] [CrossRef]
- Abraham, W.T.; Kuck, K.-H.; Goldsmith, R.L.; Lindenfeld, J.; Reddy, V.Y.; Carson, P.E.; Mann, D.L.; Saville, B.; Parise, H.; Chan, R.; et al. A Randomized Controlled Trial to Evaluate the Safety and Efficacy of Cardiac Contractility Modulation. JACC: Hear. Fail. 2018, 6, 874–883. [Google Scholar] [CrossRef] [PubMed]
- Nägele, H.; Behrens, S.; Eisermann, C. Cardiac contractility modulation in non-responders to cardiac resynchronization therapy. Europace 2008, 10, 1375–1380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuschyk, J.; Nägele, H.; Heinz-Kuck, K.; Butter, C.; Lawo, T.; Wietholt, D.; Roeger, S.; Gutterman, D.; Burkhoff, D.; Rousso, B.; et al. Cardiac contractility modulation treatment in patients with symptomatic heart failure despite optimal medical therapy and cardiac resynchronization therapy (CRT). Int. J. Cardiol. 2019, 277, 173–177. [Google Scholar] [CrossRef]
- Röger, S.; Schneider, R.; Rudic, B.; Liebe, V.; Stach, K.; Schimpf, R.; Borggrefe, M.; Kuschyk, J. Cardiac contractility modulation: first experience in heart failure patients with reduced ejection fraction and permanent atrial fibrillation. Europace 2014, 16, 1205–1209. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | |
|---|---|---|---|---|---|
| Age (years) | 69 | 67 | 54 | 69 | 76 |
| Etiology of CMP | ischemic | ischemic | non-ischemic | ischemic | ischemic |
| Prior MI | yes | yes | no | no | yes |
| Prior CABG | no | no | no | yes | no |
| Hypertension | no | no | no | yes | yes |
| Diabetes mellitus | yes | no | no | yes | no |
| Creatinine clearance (mL/min) | 78.9 | 60.3 | 60.6 | 88.9 | 44.1 |
| QRS width (msec) | 120 | 130 | 160 | 130 | 120 |
| Baseline medication | |||||
| Beta blockers | yes | yes | yes | yes | yes |
| ACE inhibitor/ARB | yes | yes | no | no | no |
| Sacubitril valsartan | no | no | no | yes | yes |
| Aldosterone inhibitor | yes | yes | yes | yes | yes |
| Diuretic | yes | yes | yes | yes | yes |
| Digoxin | no | no | yes | no | no |
| Anticoagulant | yes | yes | yes | yes | yes |
| Statin | yes | no | no | yes | yes |
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | |
|---|---|---|---|---|---|
| CRT/ICD device | MAXIMO IIVRD284VRC, MEDTRONIC | MAXIMO II DR, MEDTRONIC | LUMAX 340 HF-T, BIOTRONIK | IFORIA 3 HF-T, BIOTRONIK | IFORIA 3 DR-T, BIOTRONIK |
| CCM stimulation (therapy time per day) | 10 h | 10 h | 10 h | 8 h | 8 h |
| CCM timing | 1 h stimulation/1.23 h pause | 1 h stimulation/1.23 h pause | 1 h stimulation/1.23 h pause | 1 h stimulation/1.59 h pause | 1 h stimulation/1.59 h pause |
| CCM pacing voltage | 7.5 V | 7.5 V | 6 V | 7.5 V | 5 V |
| Maximum rate for CCM inhibition | 110 b/min | 98 b/min | 98 b/min | 110 b/min | 98 b/min |
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | |
|---|---|---|---|---|---|
| LVEF (%) at implantation | 20 | 22 | 20 | 35 | 30 |
| LVEF (%) at 6-month follow-up | 26 | 34 | NA | 37 | 36 |
| NYHA class at implantation | III | IV | IV | III | III |
| NYHA class at 6-month follow-up | II | II | NA | II | II |
| 6MWT at implantation | 290 | 350 | 210 | 380 | 320 |
| 6MWT at 6-month follow-up | 467 | 460 | NA | 497 | 440 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tint, D.; Florea, R.; Micu, S. New Generation Cardiac Contractility Modulation Device—Filling the Gap in Heart Failure Treatment. J. Clin. Med. 2019, 8, 588. https://doi.org/10.3390/jcm8050588
Tint D, Florea R, Micu S. New Generation Cardiac Contractility Modulation Device—Filling the Gap in Heart Failure Treatment. Journal of Clinical Medicine. 2019; 8(5):588. https://doi.org/10.3390/jcm8050588
Chicago/Turabian StyleTint, Diana, Roxana Florea, and Sorin Micu. 2019. "New Generation Cardiac Contractility Modulation Device—Filling the Gap in Heart Failure Treatment" Journal of Clinical Medicine 8, no. 5: 588. https://doi.org/10.3390/jcm8050588
APA StyleTint, D., Florea, R., & Micu, S. (2019). New Generation Cardiac Contractility Modulation Device—Filling the Gap in Heart Failure Treatment. Journal of Clinical Medicine, 8(5), 588. https://doi.org/10.3390/jcm8050588