Prognostic Value of the Conversion to a Shockable Rhythm in Out-of-Hospital Cardiac Arrest Patients with Initial Non-Shockable Rhythm


Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design and Data Source
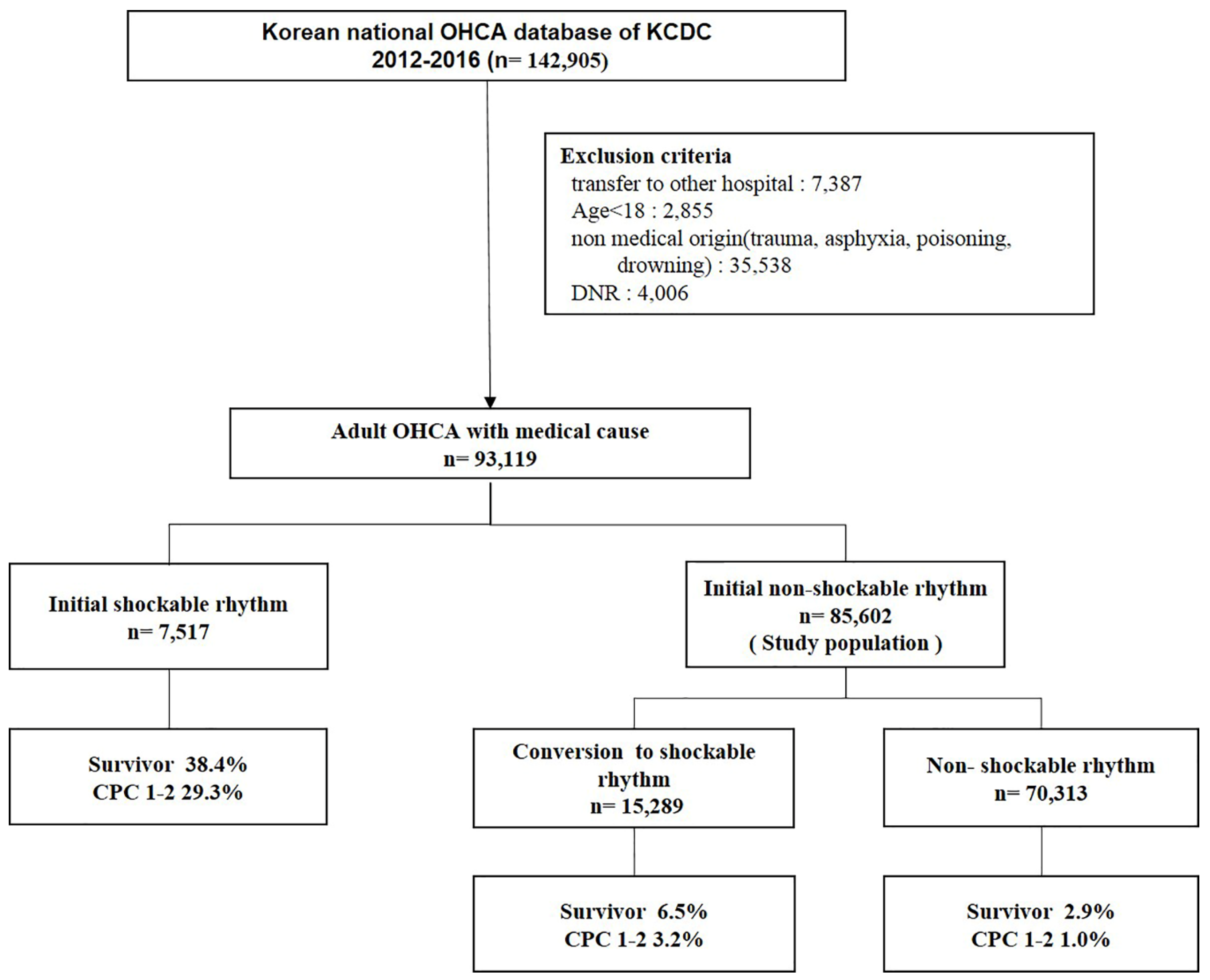
2.2. Selection of Study Patients
2.3. Outcome and Data Analysis
2.4. Statistical Analysis
3. Results
3.1. Main Categories and Outcomes of the Study Population
3.2. Comparison of Basic Characteristics according to Good Neurologic Outcome and Multiple Logistic Regression Analysis for Outcomes
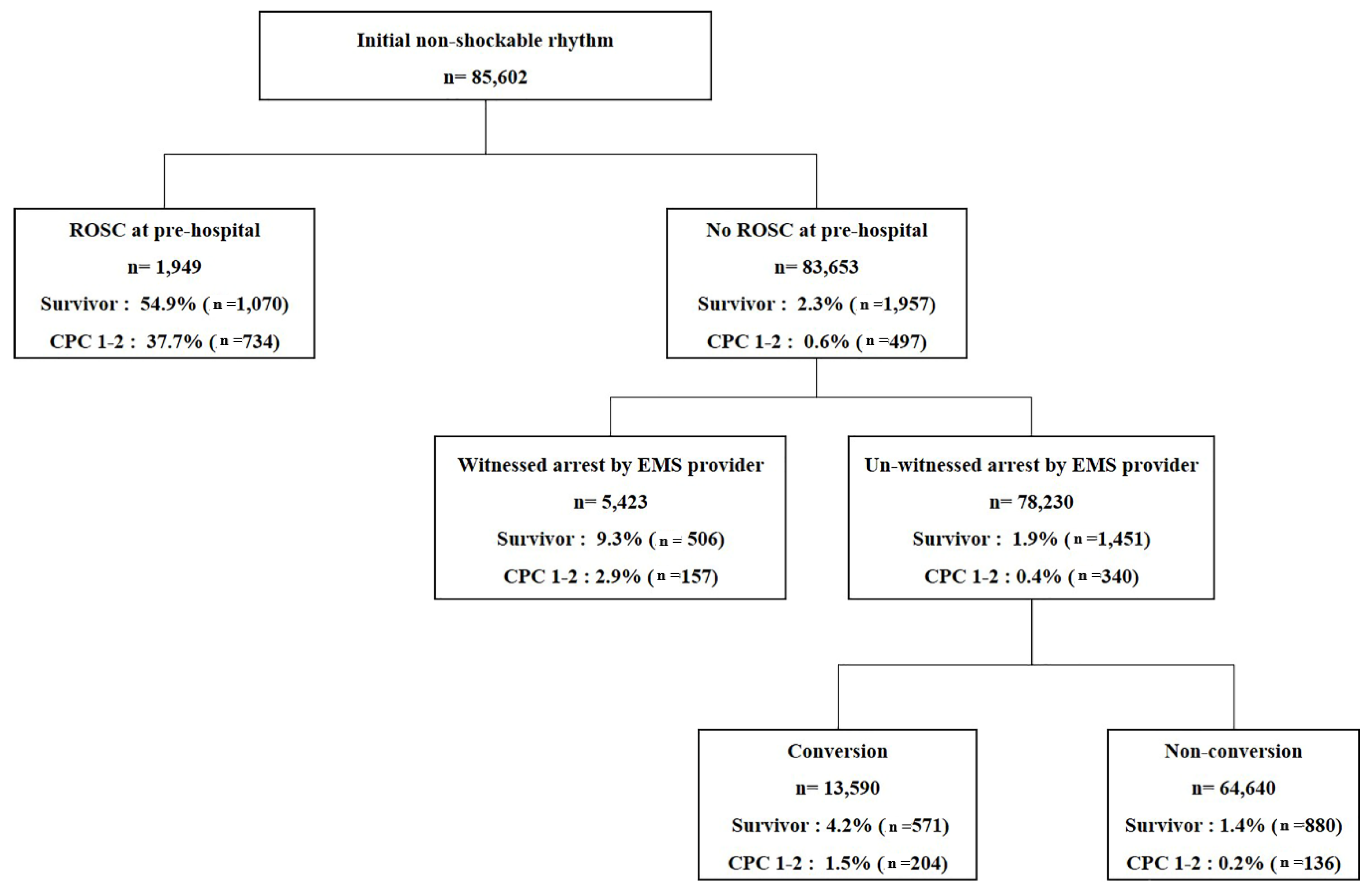
3.3. Outcomes and Logistic Regression Analysis according to Pre-Hospital Return of Spontaneous Circulation (ROSC)
3.4. Outcomes and Logistic Regression Analysis according to the State of being by an Emergency Medical Services (EMS) Provider in Patients without Pre-Hospital ROSC
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical
Data statement
References
- Nadkarni, V.M.; Larkin, G.L.; Peberdy, M.A.; Carey, S.M.; Kaye, W.; Mancini, M.E.; Nichol, G.; Lane-Truitt, T.; Potts, J.; Ornato, J.P.; et al. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. JAMA 2006, 295, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Daya, M.R.; Schmicker, R.H.; Zive, D.M.; Rea, T.D.; Nichol, G.; Buick, J.E.; Brooks, S.; Christenson, J.; Macphee, R.; Craig, A.; et al. Out-of-hospital cardiac arrest survival improving over time: Results from the Resuscitation Outcomes Consortium (ROC). Resuscitation 2015, 91, 108–115. [Google Scholar] [CrossRef]
- Chan, P.S.; McNally, B.; Tang, F.; Kellermann, A. Recent Trends in Survival from Out-of-Hospital Cardiac Arrest in the United States. Circulation 2014, 130, 1876–1882. [Google Scholar] [CrossRef] [Green Version]
- Luo, S.; Zhang, Y.; Zhang, W.; Zheng, R.; Tao, J.; Xiong, Y. Prognostic significance of spontaneous shockable rhythm conversion in adult out-of-hospital cardiac arrest patients with initial non-shockable heart rhythms: A systematic review and meta-analysis. Resuscitation 2017, 121, 1–8. [Google Scholar] [CrossRef]
- Thomas, A.J.; Newgard, C.D.; Fu, R.; Zive, D.M.; Daya, M.R. Survival in out-of-hospital cardiac arrests with initial asystole or pulseless electrical activity and subsequent shockable rhythms. Resuscitation 2013, 84, 1261–1266. [Google Scholar] [CrossRef]
- Fukuda, T.; Matsubara, T.; Doi, K.; Fukuda-Ohashi, N.; Yahagi, N. Predictors of favorable and poor prognosis in unwitnessed out-of-hospital cardiac arrest with a non-shockable initial rhythm. Int. J. Cardiol. 2014, 176, 910–915. [Google Scholar] [CrossRef]
- Morrison, L.J.; Visentin, L.M.; Kiss, A.; Theriault, R.; Eby, D.; Vermeulen, M.; Sherbino, J.; Verbeek, P.R. Validation of a rule for termination of resuscitation in out-of-hospital cardiac arrest. New Engl. J. Med. 2006, 355, 478–487. [Google Scholar] [CrossRef]
- Drennan, I.R.; Case, E.; Verbeek, P.R.; Reynolds, J.C.; Goldberger, Z.D.; Jasti, J.; Charleston, M.; Herren, H.; Idris, A.H.; Leslie, P.R.; et al. A comparison of the universal TOR Guideline to the absence of prehospital ROSC and duration of resuscitation in predicting futility from out-of-hospital cardiac arrest. Resuscitation 2017, 111, 96–102. [Google Scholar] [CrossRef]
- Sasson, C.; Hegg, A.J.; Macy, M.; Park, A.; Kellermann, A.; McNally, B.; CARES Surveillance Group. Prehospital Termination of Resuscitation in Cases of Refractory Out-of-Hospital Cardiac Arrest. JAMA 2008, 300, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Korean Centers for Disease Control and Prevention (KCDC) Home Page. Available online: http://www.cdc.go.kr/CDC/contents/CdcKrContentView.jsp?cid=102714&menuIds=HOME006-MNU2802-MNU2895 (accessed on 9 May 2019).
- Ro, Y.S.; Shin, S.D.; Song, K.J.; Lee, E.J.; Kim, J.Y.; Ahn, K.O.; Chung, S.P.; Kim, Y.T.; Hong, S.O.; Choi, J.A.; et al. A trend in epidemiology and outcomes of out-of-hospital cardiac arrest by urbanization level: A nationwide observational study from 2006 to 2010 in South Korea. Resuscitation 2013, 84, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, I.; Nadkarni, V.; Bahr, J.; Berg, R.A.; Billi, J.E.; Bossaert, L.; Cassan, P.; Coovadia, A.; D’Este, K.; Finn, J.; et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: Update and simplification of the Utstein templates for resuscitation registries: A statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Councils of Southern Africa). Circulation 2004, 110, 3385–3397. [Google Scholar] [CrossRef]
- Hallstrom, A.; Rea, T.D.; Mosesso, V.N.; Cobb, L.A.; Anton, A.R.; Van Ottingham, L.; Sayre, M.R.; Christenson, J. The relationship between shocks and survival in out-of-hospital cardiac arrest patients initially found in PEA or asystole. Resuscitation 2007, 74, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Olasveengen, T.M.; Samdal, M.; Steen, P.A.; Wik, L.; Sunde, K. Progressing from initial non-shockable rhythms to a shockable rhythm is associated with improved outcome after out-of-hospital cardiac arrest. Resuscitation 2009, 80, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Kajino, K.; Iwami, T.; Daya, M.; Nishiuchi, T.; Hayashi, Y.; Ikeuchi, H.; Tanaka, H.; Shimazu, T.; Sugimoto, H. Subsequent ventricular fibrillation and survival in out-of-hospital cardiac arrests presenting with PEA or asystole. Resuscitation 2008, 79, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Herlitz, J.; Svensson, L.; Engdahl, J.; Silfverstolpe, J. Characteristics and outcome in out-of-hospital cardiac arrest when patients are found in a non-shockable rhythm. Resuscitation 2008, 76, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Rajan, S.; Folke, F.; Hansen, S.M.; Hansen, C.M.; Kragholm, K.; Gerds, T.A.; Lippert, F.K.; Karlsson, L.; Møller, S.; Køber, L.; et al. Incidence and survival outcome according to heart rhythm during resuscitation attempt in out-of-hospital cardiac arrest patients with presumed cardiac etiology. Resuscitation 2017, 114, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Wah, W.; Wai, K.L.; Pek, P.P.; Ho, A.F.W.; Alsakaf, O.; Chia, M.Y.C.; Noor, J.M.; Kajino, K.; De Souza, N.N.A.; Ong, M.E.H.; et al. Conversion to shockable rhythms during resuscitation and survival for out-of hospital cardiac arrest. Am. J. Emerg. Med. 2017, 35, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Zheng, R.; Luo, S.; Liao, J.; Liu, Z.; Xu, J.; Zhan, H.; Liao, X.; Xiong, Y.; Idris, A. Conversion to shockable rhythms is associated with better outcomes in out-of-hospital cardiac arrest patients with initial asystole but not in those with pulseless electrical activity. Resuscitation 2016, 107, 88–93. [Google Scholar] [CrossRef]
- Funada, A.; Goto, Y.; Tada, H.; Teramoto, R.; Shimojima, M.; Hayashi, K.; Yamagishi, M. Age-specific differences in prognostic significance of rhythm conversion from initial non-shockable to shockable rhythm and subsequent shock delivery in out-of-hospital cardiac arrest. Resuscitation 2016, 108, 61–67. [Google Scholar] [CrossRef]
- Wampler, D.A.; Collett, L.; Manifold, C.A.; Velasquez, C.; McMullan, J.T. Cardiac arrest survival is rare without prehospital return of spontaneous circulation. Prehosp. Emerg. Care 2012, 16, 451–455. [Google Scholar] [CrossRef]
- Varvarousi, G.; Chalkias, A.; Stefaniotou, A.; Pliatsika, P.; Varvarousis, D.; Koutsovasilis, A.; Xanthos, T. Intraarrest Rhythms and Rhythm Conversion in Asphyxial Cardiac Arrest. Acad. Emerg. Med. 2015, 22, 518–524. [Google Scholar] [CrossRef] [Green Version]
- Goto, Y.; Maeda, T.; Nakatsu-Goto, Y. Prognostic implications of conversion from nonshockable to shockable rhythms in out-of-hospital cardiac arrest. Crit. Care 2014, 18, 528. [Google Scholar] [CrossRef] [Green Version]
- Kitamura, N.; on behalf of the SOS-KANTO 2012 Study Group; Nakada, T.-A.; Shinozaki, K.; Tahara, Y.; Sakurai, A.; Yonemoto, N.; Nagao, K.; Yaguchi, A.; Morimura, N. Subsequent shock deliveries are associated with increased favorable neurological outcomes in cardiac arrest patients who had initially non-shockable rhythms. Crit. Care 2015, 19, 322. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | All (n = 85,602) | CPC 1–2 (n = 1231, 1.4%) | CPC 3–5 (n = 84,371, 98.6%) | p-Value |
|---|---|---|---|---|
| Age (year), median (IQR) | 73(60–81) | 56 (48–66) | 73(60–81) | <0.001 |
| Age group (years) | <0.001 | |||
| 18~44 | 5282 (6.2) | 198 (16.1) | 5084 (6.0) | |
| 45~64 | 21,828 (25.5) | 681 (55.3) | 21,147 (25.1) | |
| 65~74 | 18,763 (24.9) | 216 (17.5) | 18,547 (22.0) | |
| ≥75 | 39,729 (46.4) | 136 (11.0) | 39,593 (46.9) | |
| Sex, male | 52,292 (61.1) | 916 (74.4) | 51,376 (60.9) | <0.001 |
| Witnessed arrest | 36,174 (42.3) | 1004(81.6) | 35,170 (41.7) | <0.001 |
| Witnessed by EMS | 5771 (6.7) | 299(24.3) | 5472 (6.5) | <0.001 |
| Witnessed by lay rescuer | 30,403 (35.5) | 705 (57.3) | 29,698 (35.2) | <0.001 |
| Arrest location at public place | 9203 (10.8) | 300 (24.4) | 8903 (10.6) | <0.001 |
| Bystander CPR | 10,555 (12.3) | 347 (28.2) | 10,208 (12.1) | <0.001 |
| Initial rhythm | <0.001 | |||
| PEA | 5535 (6.5) | 170 (13.8) | 5365 (6.4) | |
| asystole | 80,067 (93.5) | 1061 (86.2) | 79,006 (93.6) | |
| Presumed cardiac origin | 79,579 (93.0) | 1159 (94.2) | 78,420 (92.9) | 0.106 |
| Coronary reperfusion treatment | 1123 (1.3) | 368 (29.9) | 755 (0.9) | <0.001 |
| TTM | 1593 (1.9) | 220 (17.9) | 1373 (1.6) | <0.001 |
| ECMO | 410 (0.5) | 20 (1.6) | 390 (0.5) | <0.001 |
| Pre-hospital ROSC | 1949 (2.3) | 734 (59.6) | 1215 (1.4) | <0.001 |
| Conversion | 15,289 (17.9) | 495 (40.2) | 14,794 (17.5) | <0.001 |
| Variable | Good Neurologic Outcome at Hospital Discharge | |||
|---|---|---|---|---|
| Adjusted OR | 95% CI | p-Value | ||
| Age (years) | 0.959 | 0.955 | 0.963 | <0.001 |
| Sex, male | 1.230 | 1.055 | 1.434 | 0.008 |
| Witnessed arrest | 3.413 | 2.904 | 4.010 | <0.001 |
| Initial rhythm (PEA) | 1.153 | 0.941 | 1.414 | 0.170 |
| Arrest location at public place | 1.422 | 1.204 | 1.680 | <0.001 |
| Bystander CPR | 1.457 | 1.242 | 1.709 | <0.001 |
| Pre-hospital ROSC | 72.777 | 63.182 | 83.828 | <0.001 |
| Conversion | ||||
| Conversion group | 2.604 | 2.248 | 3.015 | <0.001 |
| Non-conversion group | reference | |||
| Variable | Conversion Group (n = 15,289) | Non-Conversion Group (n = 70,313) | p-Value |
|---|---|---|---|
| Age (year ± SD) | 65.25 ± 14.87 | 71.32 ± 14.86 | <0.001 |
| Age group (years) | <0.001 | ||
| 18~44 | 1381(9.0) | 3901(5.5) | |
| 45~64 | 5500(36.0) | 16328(23.2) | |
| 65~74 | 3629(23.7) | 15134(21.5) | |
| ≥75 | 4779(31.3) | 34950(49.7) | |
| Sex, male | 10516(68.8) | 41776(59.4) | <0.001 |
| Witnessed arrest | 8583(56.1) | 27591(39.2) | <0.001 |
| Witnessed by EMS | 1343(8.9) | 4428(6.3) | <0.001 |
| Witnessed by lay rescuer | 7240 (47.4) | 23163 (32.9) | <0.001 |
| Arrest location at public place | 2948(19.3) | 2385(10.9) | <0.001 |
| Bystander CPR | 2493(16.3) | 8062(11.5) | <0.001 |
| Initial rhythm | <0.001 | ||
| PEA | 1353(8.8) | 4182(5.9) | |
| Asystole | 13936(91.2) | 66131(94.1) | |
| Presumed cardiac origin | 14453(94.5) | 65126(92.6) | <0.001 |
| Coronary reperfusion treatment | 579(3.8) | 226(1.0) | <0.001 |
| TTM | 540(3.5) | 1053(1.5) | <0.001 |
| ECMO | 222(1.5) | 188(0.3) | <0.001 |
| Pre-hospital ROSC | 414(2.7) | 1535(2.2) | <0.001 |
| Survival discharge | 997(6.5) | 2030(2.9) | <0.001 |
| CPC 1–2 | 495(3.2) | 736(1.0) | <0.001 |
| Variable | Pre-Hospital ROSC(+) | Pre-Hospital ROSC(-) | ||||
|---|---|---|---|---|---|---|
| CPC 1–2 (n = 734) | CPC 3–5 (n = 1215) | p-Value | CPC 1–2 (n = 497) | CPC 3–5 (n = 83156) | p-Value | |
| Age (year), median (IQR) | 56 (49–66) | 67(55–78) | <0.001 | 56(47–66) | 74(60–81) | <0.001 |
| Age group (years) | <0.001 | <0.001 | ||||
| 18~44 | 101 (13.8) | 108 (8.9) | 97 (19.5) | 4976 (6.0) | ||
| 45~64 | 423 (57.6) | 444 (36.5) | 258 (51.9) | 20703 (24.9) | ||
| 65~74 | 130 (17.7) | 240(19.8) | 86 (17.3) | 18307(22.0) | ||
| ≥75 | 80 (10.9) | 423 (34.8) | 56 (11.3) | 39170 (47.1) | ||
| Sex, male | 548 (74.7) | 776 (63.9) | <0.001 | 368 (74.0) | 50600(6.8) | <0.001 |
| Witnessed arrest | 596 (81.2) | 822 (67.7) | <0.001 | 408(82.1) | 34348 (41.3) | <0.001 |
| Witnessed by EMS | 142(19.3) | 206(17.0) | 0.200 | 157(31.6) | 5266(6.3) | <0.001 |
| Witnessed by lay rescuer | 454 (61.9) | 280 (38.1) | <0.001 | 251 (50.5) | 29082 (35.0) | <0.001 |
| Arrest location at public place | 193 (26.3) | 188 (15.5) | <0.001 | 107 (21.5) | 8715 (10.5) | <0.001 |
| Bystander CPR | 229 (31.2) | 233 (19.2) | <0.001 | 118 (23.7) | 9975 (12.0) | <0.001 |
| Initial rhythm | 0.301 | <0.001 | ||||
| PEA | 105 (14.3) | 196 (16.1) | 65 (13.1) | 5169(6.2) | ||
| asystole | 629 (85.7) | 1019 (83.9) | 432 (86.9) | 77987 (93.8) | ||
| Cardiac etiology | 690 (94.0) | 970 (79.8) | <0.001 | 469 (94.4) | 77450 (93.1) | 0.327 |
| Conversion | 248 (33.8) | 166 (13.7) | <0.001 | 247 (49.7) | 14628 (17.6) | <0.001 |
| Survival discharge | 734 (100) | 336 (27.7) | - | 497 (100) | 1460 (1.8) | - |
| Variable | Patients with Pre-Hospital ROSC (n = 1949) | Patients without Pre-Hospital ROSC (n = 83,653) | ||
|---|---|---|---|---|
| Survival at Discharge | CPC 1 or 2 at Discharge | Survival at Discharge | CPC 1 or 2 at Discharge | |
| Adjusted OR (95% CI) | Adjusted OR (95% CI) | Adjusted OR (95% CI) | Adjusted OR (95% CI) | |
| Age (year) | 0.974 (0.967–0.980) | 0.968 (0.962–0.975) | 0.971 (0.968–0.973) | 0.954 (0.948–0.959) |
| Sex, male | 1.105 (0.900–1.358) | 1.302 (1.045–1.623) | 1.105 (0.999–1.223) | 1.170 (0.952–1.438) |
| Witnessed arrest | 1.512 (1.221–1.872) | 1.872 (1.479–2.369) | 4.355 (3.905–4.858) | 5.313 (4.203–6.716) |
| Initial rhythm (PEA) | 0.845 (0.650–1.099) | 0.882 (0.669–1.163) | 2.011 (1.768–2.288) | 1.469 (1.122–1.922) |
| Arrest location at public place | 1.386 (1.079–1.781) | 1.462 (1.145–1.867) | 1.603 (1.425–1.804) | 1.364 (1.091–1.704) |
| Bystander CPR | 1.424 (1.126–1.800) | 1.477 (1.118–1.885) | 1.365 (1.219–1.529) | 1.406 (1.135–1.741) |
| Conversion | ||||
| Conversion group | 2.827 (2.171–3.680) | 2.325 (1.821–2.935) | 1.549 (1.403–1.711) | 2.607 (2.170–3.131) |
| Non-conversion group | reference | reference | ||
| Variable | Adjusted OR (95% CI) for CPC 1 or 2 at Discharge in Patients without Pre-Hospital ROSC | |
|---|---|---|
| Patients with Witnessed by EMS Provider (n = 5423) | Patients with Un-Witnessed by EMS Provider (n = 78,230) | |
| Age (year) | 0.954 (0.944–0.963) | 0.954 (0.948–0.961) |
| Sex, male | 1.052 (0.749–1.477) | 1.297 (0.996–1.688) |
| Arrest witnessed by lay rescuer | - | 3.573 (2.787–4.581) |
| Initial rhythm (PEA) | 1.222 (0.805–1.855) | 1.326 (0.929–1.892) |
| Arrest location at public place | 0.508 (0.159–1.623) | 1.812 (1.423–2.306) |
| Bystander CPR | 1.204 (0.805–1.855) | 1.309 (1.001–1.712) |
| Rhythm conversion | ||
| Conversion group | 1.052 (0.732–1.511) | 3.972 (3.167–4.983) |
| Non-conversion group | reference | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, K.S.; Lee, S.W.; Lee, E.J.; Kim, S.J. Prognostic Value of the Conversion to a Shockable Rhythm in Out-of-Hospital Cardiac Arrest Patients with Initial Non-Shockable Rhythm. J. Clin. Med. 2019, 8, 644. https://doi.org/10.3390/jcm8050644
Han KS, Lee SW, Lee EJ, Kim SJ. Prognostic Value of the Conversion to a Shockable Rhythm in Out-of-Hospital Cardiac Arrest Patients with Initial Non-Shockable Rhythm. Journal of Clinical Medicine. 2019; 8(5):644. https://doi.org/10.3390/jcm8050644
Chicago/Turabian StyleHan, Kap Su, Sung Woo Lee, Eui Jung Lee, and Su Jin Kim. 2019. "Prognostic Value of the Conversion to a Shockable Rhythm in Out-of-Hospital Cardiac Arrest Patients with Initial Non-Shockable Rhythm" Journal of Clinical Medicine 8, no. 5: 644. https://doi.org/10.3390/jcm8050644
APA StyleHan, K. S., Lee, S. W., Lee, E. J., & Kim, S. J. (2019). Prognostic Value of the Conversion to a Shockable Rhythm in Out-of-Hospital Cardiac Arrest Patients with Initial Non-Shockable Rhythm. Journal of Clinical Medicine, 8(5), 644. https://doi.org/10.3390/jcm8050644