Probiotics for the Prophylaxis of Migraine: A Systematic Review of Randomized Placebo Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
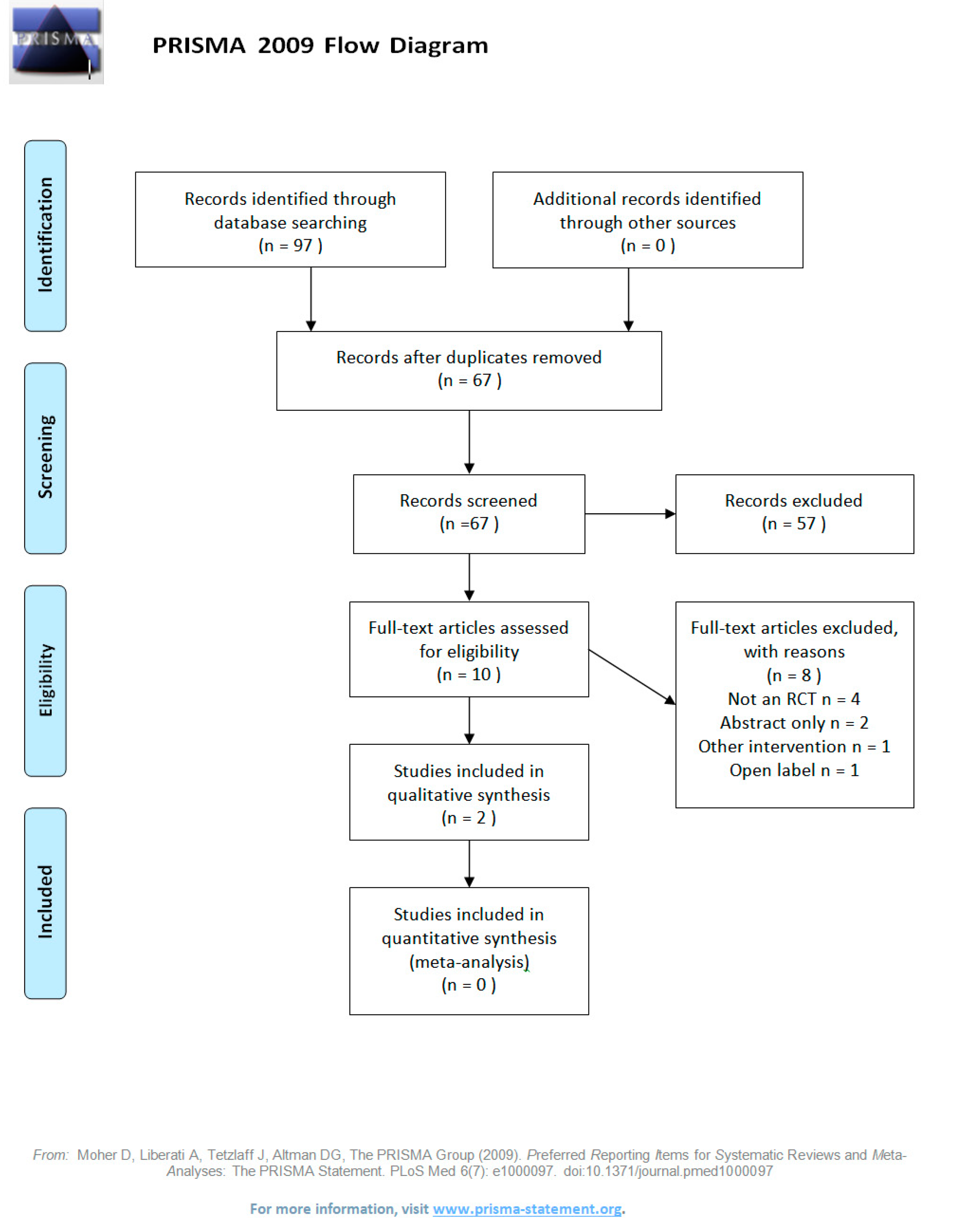
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Steiner, T.J.; Stovner, L.J.; Birbeck, G.L. Migraine: The seventh disabler. J. Headache Pain 2013, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Vincent, M.; Wang, S. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar]
- Buse, D.C.; Manack, A.N.; Fanning, K.M.; Serrano, D.; Reed, M.L.; Turkel, C.C.; Lipton, R.B. Chronic Migraine Prevalence, Disability, and Sociodemographic Factors: Results from the American Migraine Prevalence and Prevention Study. Headache 2012, 52, 1456–1470. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B. Chronic Migraine, Classification, Differential Diagnosis, and Epidemiology. Headache 2011, 51, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Goadsby, P.J.; Holland, P.R.; Martins-Oliveira, M.; Hoffmann, J.; Schankin, C.; Akerman, S. Pathophysiology of Migraine: A Disorder of Sensory Processing. Physiol. Rev. 2017, 97, 553–622. [Google Scholar] [CrossRef] [PubMed]
- Van Hemert, S.; Breedveld, A.C.; Rovers, J.M.P.; Vermeiden, J.P.W.; Witteman, B.J.M.; Smits, M.G.; de Roos, N.M. Migraine Associated with Gastrointestinal Disorders: Review of the Literature and Clinical Implications. Front. Neurol. 2014, 5, 241. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.R.; Osadchiy, V.; Kalani, A.; Mayer, E.A. The Brain-Gut-Microbiome Axis. Cell. Mol. Gastroenterol. Hepatol. 2018, 6, 133–148. [Google Scholar] [CrossRef] [Green Version]
- Cryan, J.F.; Dinan, T.G. Mind-Altering Microorganisms: The Impact of the Gut Microbiota on Brain and Behaviour. Nat. Rev. Neurosci. 2012, 13, 701–712. [Google Scholar] [CrossRef]
- Bercik, P.; Park, A.J.; Sinclair, D.; Khoshdel, A.; Lu, J.; Huang, X.; Deng, Y.; Blennerhassett, P.A.; Fahnestock, M.; Moine, D.; et al. The Anxiolytic Effect of Bifidobacterium Longum NCC3001 Involves Vagal Pathways for Gut-Brain Communication. Neurogastroenterol. Motil. 2011, 23, 1132–1139. [Google Scholar] [CrossRef]
- Gasparini, C.F.; Smith, R.A.; Griffiths, L.R. Genetic and Biochemical Changes of the Serotonergic System in Migraine Pathobiology. J. Headache Pain 2017, 18, 2163. [Google Scholar] [CrossRef]
- Dussor, G. Serotonin, 5HT1 Agonists, and Migraine: New Data, but Old Questions Still Not Answered. Curr. Opin. Support. Palliat. Care 2014, 8, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Deen, M.; Hansen, H.D.; Hougaard, A.; Nørgaard, M.; Eiberg, H.; Lehel, S.; Ashina, M.; Knudsen, G.M. High Brain Serotonin Levels in Migraine between Attacks: A 5-HT4 Receptor Binding PET Study. NeuroImage Clin. 2018, 18, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Mawe, G.M.; Hoffman, J.M. Serotonin Signalling in the Gut-Functions, Dysfunctions and Therapeutic Targets. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 564. [Google Scholar] [CrossRef]
- Martami, F.; Ghorbani, Z.; Abolhasani, M.; Togha, M.; Meysamie, A.; Sharifi, A.; Razeghi Jahromi, S. Comorbidity of Gastrointestinal Disorders, Migraine, and Tension-Type Headache: A Cross-Sectional Study in Iran. Neurol. Sci. 2017, 39, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Liebregts, T.; Adam, B.; Bredack, C.; Röth, A.; Heinzel, S.; Lester, S.; Downie-Doyle, S.; Smith, E.; Drew, P.; Talley, N.J.; et al. Immune Activation in Patients With Irritable Bowel Syndrome. Gastroenterology 2007, 132, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Bruno, P.P.; Carpino, F.; Carpino, G.; Zicari, A. An Overview on Immune System and Migraine. Eur. Rev. Med. Pharmacol. Sci. 2007, 11, 245. [Google Scholar]
- Kelman, L. The Triggers or Precipitants of the Acute Migraine Attack. Cephalalgia 2007, 27, 394–402. [Google Scholar] [CrossRef]
- Söderholm, J.D.; Perdue, M.H. Stress and Gastrointestinal Tract. II. Stress and Intestinal Barrier Function. Am. J. Physiol. Liver Physiol. 2001, 280, 7–13. [Google Scholar]
- Diogenes, A.; Ferraz, C.C.R.; Akopian, A.N.; Henry, M.A.; Hargreaves, K.M. LPS Sensitizes TRPV1 via Activation of TLR4 in Trigeminal Sensory Neurons. J. Dent. Res. 2011, 90, 759–764. [Google Scholar] [CrossRef]
- Sarkar, A.; Lehto, S.M.; Harty, S.; Dinan, T.G.; Cryan, J.F.; Burnet, P.W.J. Psychobiotics and the Manipulation of Bacteria–Gut–Brain Signals. Trends Neurosci. 2016, 39, 763–781. [Google Scholar] [CrossRef]
- Kato-Kataoka, A.; Nishida, K.; Takada, M.; Kawai, M.; Kikuchi-Hayakawa, H.; Suda, K.; Ishikawa, H.; Gondo, Y.; Shimizu, K.; Matsuki, T.; et al. Fermented Milk Containing Lactobacillus Casei Strain Shirota Preserves the Diversity of the Gut Microbiota and Relieves Abdominal Dysfunction in Healthy Medical Students Exposed to Academic Stress. Appl. Environ. Microbiol. 2016, 82, 3649–3658. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D.; Holland, S.; Freitag, F.; Dodick, D.W.; Argoff, C.; Ashman, E. Evidence-Based Guideline Update: Pharmacologic Treatment for Episodic Migraine Prevention in Adults Report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology 2012, 78, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Tardiolo, G.; Bramanti, P.; Mazzon, E. Migraine: Experimental Models and Novel Therapeutic Approaches. Int. J. Mol. Sci. 2019, 20, 2932. [Google Scholar] [CrossRef] [PubMed]
- Antonaci, F.; Ghiotto, N.; Wu, S.; Pucci, E.; Costa, A. Recent Advances in Migraine Therapy. SpringerPlus 2016, 5, 789. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.-J.; Wang, H.-Y.; Wang, X.-J.; Kaye, A.D.; Sun, Y.-H. Potential Beneficial Effects of Probiotics on Human Migraine Headache: A Literature Review. Pain Physician 2017, 20, E251–E255. [Google Scholar] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the Quality of Reports of Randomized Clinical Trials: Is Blinding Necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- De Roos, N.M.; Van Hemert, S.; Rovers, J.M.P.; Smits, M.G.; Witteman, B.J.M. The Effects of a Multispecies Probiotic on Migraine and Markers of Intestinal Permeability-Results of a Randomized Placebo-Controlled Study. Eur. J. Clin. Nutr. 2017, 71, 1455–1462. [Google Scholar] [CrossRef]
- Martami, F.; Togha, M.; Seifishahpar, M.; Ghorbani, Z.; Ansari, H.; Karimi, T.; Jahromi, S.R. The Effects of a Multispecies Probiotic Supplement on Inflammatory Markers and Episodic and Chronic Migraine Characteristics: A Randomized Double-Blind Controlled Trial. Cephalalgia 2019, 39, 841–853. [Google Scholar] [CrossRef]
- Gonzalez, A.; Hyde, E.; Sangwan, N.; Gilbert, J.A.; Viirre, E.; Knight, R. Migraines Are Correlated with Higher Levels of Nitrate-, Nitrite-, and Nitric Oxide-Reducing Oral Microbes in the American Gut Project Cohort. mSystems 2016, 1, e00105–e00116. [Google Scholar] [CrossRef]
- Artero-Morales, M.; González-Rodríguez, S.; Ferrer-Montiel, A. TRP Channels as Potential Targets for Sex-Related Differences in Migraine Pain. Front. Mol. Biosci. 2018, 5, 73. [Google Scholar] [CrossRef] [Green Version]
- Iyengar, S.; Johnson, K.W.; Ossipov, M.H.; Aurora, S.K. CGRP and the Trigeminal System in Migraine. Headache 2019, 59, 659–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgescu, D.; Reisz, D.; Gurban, C.V.; Georgescu, L.A.; Ionita, I.; Ancusa, O.E.; Lighezan, D. Migraine in Young Females with Irritable Bowel Syndrome: Still a Challenge. Neuropsychiatr. Dis. Treat. 2018, 14, 21. [Google Scholar] [CrossRef] [PubMed]
- Linde, M.; Wm, M.; Ep, C.; Dc, M.; Linde, M.; Mulleners, W.M.; Chronicle, E.P.; Mccrory, D.C. Topiramate for the Prophylaxis of Episodic Migraine in Adults ( Review ) Topiramate for the Prophylaxis of Episodic Migraine in Adults. Cochrane Database Syst. Rev. 2014, 90, 24. [Google Scholar]
- Khera, A.; McGuire, D.K.; Murphy, S.A.; Stanek, H.G.; Das, S.R.; Vongpatanasin, W.; Wians, F.H.; Grundy, S.M.; De Lemos, J.A. Race and Gender Differences in C-Reactive Protein Levels. J. Am. Coll. Cardiol. 2005, 46, 464–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schürks, M.; Rist, P.M.; Zee, R.Y.; Chasman, D.I.; Kurth, T. Tumour Necrosis Factor Gene Polymorphisms and Migraine: A Systematic Review and Meta-Analysis. Cephalalgia 2011, 31, 1381–1404. [Google Scholar] [CrossRef] [PubMed]
- Bogaty, P.; Dagenais, G.R.; Joseph, L.; Boyer, L.; Leblanc, A.; Bélisle, P.; Brophy, J.M. Time Variability of C-Reactive Protein: Implications for Clinical Risk Stratification. PLoS ONE 2013, 8, e60759. [Google Scholar] [CrossRef] [PubMed]
- Ouwehand, A.C. A Review of Dose-Responses of Probiotics in Human Studies. Benef. Microbes 2017, 8, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Douillard, F.P.; Ribbera, A.; Kant, R.; Pietilä, T.E.; Järvinen, H.M.; Messing, M.; Randazzo, C.L.; Paulin, L.; Laine, P.; Ritari, J.; et al. Comparative Genomic and Functional Analysis of 100 Lactobacillus Rhamnosus Strains and Their Comparison with Strain GG. PLoS Genet. 2013, 9, e1003683. [Google Scholar] [CrossRef] [PubMed]
- Aamodt, A.H.; Stovner, L.J.; Hagen, K.; Zwart, J.A. Comorbidity of Headache and Gastrointestinal Complaints. The Head-HUNT Study. Cephalalgia 2008, 28, 144–151. [Google Scholar]
- Drummond, P.D. Tryptophan Depletion Increases Nausea, Headache and Photophobia in Migraine Sufferers. Cephalalgia 2006, 26, 1225–1233. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| De Roos 2017 [27] | Martami 2019 Chronic [28] | Martami 2019 Episodic [28] | |
|---|---|---|---|
| Design | Double blind RCT | Double blind RCT | Double blind RCT |
| Total completed n (F/M) Probiotic n (F/M) Placebo n (F/M) | 60 (56/4) 31 (28/3) 29 (28/1) | 40 (35/15) 23 (15/7) 18 (13/5) | 39 (37/13) 21 (17/4) 18 (12/6) |
| Drop-out rate % | 5% 3/63 (all placebo arm) | 20% 10/50 (3 probiotic, 7 placebo) | 22% 11/50 (4 probiotic, 7 placebo) |
| Follow-up | 12 weeks | 8 weeks | 10 weeks |
| Migraine diagnostic criteria | ICHD-II | ICHD-III beta | ICHD-III beta |
| Migraine subtypes included | Episodic migraine | Chronic migraine | Episodic migraine |
| Probiotic | Ecologic Barrier, Winclove Bifidobacterium bifidum W23 Bifidobacterium lactis W52 Lactobacillus acidophilus W37 Lactobacillus brevis W63 Lactobacillus casei W56 Lactobacillus salivarius W24 Lactococcus lactis W19 Lactococcus lactis W58 | Bio-Kult, Protexin Bacillus subtilis PXN 21 Bifidobacterium bifidum PXN 23 Bifidobacterium breve PXN 25 Bifidobacterium infantis PXN 27 Bifidobacterium longum PXN 30 Lactobacillus acidophilus PXN 35 Lactobacillus delbrueckii ssp. bulgaricus PXN 39 Lactobacillus casei PXN 37 Lactobacillus plantarum PXN 47 Lactobacillus rhamnosus PXN 54 Lactobacillus helveticus PXN 45 Lactobacillus salivarius PXN 57 Lactococcus lactis ssp. lactis PXN 63 Streptococcus thermophilus PXN 66 | Bio-Kult, Protexin Bacillus subtilis PXN 21 Bifidobacterium bifidum PXN 23 Bifidobacterium breve PXN 25 Bifidobacterium infantis PXN 27 Bifidobacterium longum PXN 30 Lactobacillus acidophilus PXN 35 Lactobacillus delbrueckii ssp. bulgaricus PXN 39 Lactobacillus casei PXN 37 Lactobacillus plantarum PXN 47 Lactobacillus rhamnosus PXN 54 Lactobacillus helveticus PXN 45 Lactobacillus salivarius PXN 57 Lactococcus lactis ssp. lactis PXN 63 Streptococcus thermophilus PXN 66 |
| Dose | 2.5 × 109 CFU/g, one sachet 2 g | 2 × 109 CFU/capsule, 2 capsules | 2 × 109 CFU/capsule, 2 capsules |
| Intake | Daily | Daily | Daily |
| Use of medications | Continued as usual | Continued as usual | Continued as usual |
| Outcomes measured | Migraine questionnaires and diaries (MIDAS, HDI); inflammation markers (IL, CRP, TNF); intestinal permeability (lactulose/mannitol test, zonulin levels in feces and serum) | Migraine questionnaires and diaries (migraine duration, severity, frequency, use of abortive medications); inflammation markers (CRP, TNF) | Migraine questionnaires and diaries (migraine duration, severity, frequency, use of abortive medications); inflammation markers (CRP, TNF) |
| De Roos 2017 [27] | Martami 2019 Chronic [28] | Martami 2019 Episodic [28] | ||||
|---|---|---|---|---|---|---|
| Probiotic | Placebo | Probiotic | Placebo | Probiotic | Placebo | |
| TNF before (pg/mL) | 2.45 ± 0.55 | 2.70 ± 1.2 | 5.90 ± 6.25 | 3.12 ± 3.46 | 2.97 ± 5.09 | 2.31 ± 3.51 |
| TNF after (pg/mL) | 2.57 ± 0.55 | 2.63 ± 0.67 | 8.18 ± 7.89 | 5.73 ± 5.38 | 2.73 ± 5.25 | 5.05 ± 6.94 |
| CRP before (mg/dL) | 2.0 ± 2.9 | 2.6 ± 3.3 | 1.77 ± 2.90 | 0.57 ± 0.73 | 1.09 ± 1.87 | 0.55 ± 0.4 |
| CRP after (mg/dL) | 1.8 ± 2.5 | 2.4 ± 3.1 | 2.70 ± 4.03 * | 0.74 ± 1.01 | 0.83 ± 1.19 | 0.73 ± 0.33 |
| Recommendations for future probiotic trials in migraine sufferers |
|---|
| Exclusion criteria |
| Standardized exclusion criteria: use of medications with well-acknowledged impacts on the gut microbiome should be considered (e.g., antibiotics, antidepressants, proton pump inhibitors), as well as duration of the period free from antibiotics and probiotics. |
| Pregnancy and breastfeeding (due to the influence of hormonal changes). |
| Inclusion criteria |
| Studies should explicitly focus on chronic or episodic migraine sufferers and clearly indicate which group was studied. |
| Studies should focus on migraine with aura and without aura and clearly indicate which group was studied. |
| Gender factor should be considered. Many studies had only small proportion of male participants. Single gender studies could also be considered. |
| Standardized evaluation of the symptoms in the defined period prior to enrolment, minimum one month history. Ideally, to avoid reliance on patients’ memory, the first month of the trial would not include the intervention and allow for observation of the symptoms. |
| Intervention |
| Convenient and easy-to-use formulations should be chosen, to ensure good compliance. |
| Duration of intervention should be no less than two months. |
| Washout period should be studied to establish for each formulation how long after treatment cessation effects starts to diminish. |
| General |
| Use of validated standardized migraine symptom questionnaires/diaries for recording of migraine frequency (frequency of migraine onsets), duration (hours), and severity (validated scale or a comparable 10-point visual analogue scale (VAS)). |
| Validated Quality of Life tools. |
| If applicable, sub-group analysis comparing the effect of intervention in groups with different severities of migraine symptoms. |
| Inclusion of standard reporting metrics, such as 50% responder rates. |
| Standardized reporting on the use of medications pre and post intervention (number of doses per week, with the information what a standard local dose is). |
| Sub-group analysis for responders and non-responders, with explicit definition of responders (e.g., reduction of migraine duration by over 2 days per month). |
| Preferably, microbiome analysis pre- and post-intervention. |
| Consider inclusion of metabolomics outcomes such as lipopolysaccharides (LPS) and tryptophan. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naghibi, M.M.; Day, R.; Stone, S.; Harper, A. Probiotics for the Prophylaxis of Migraine: A Systematic Review of Randomized Placebo Controlled Trials. J. Clin. Med. 2019, 8, 1441. https://doi.org/10.3390/jcm8091441
Naghibi MM, Day R, Stone S, Harper A. Probiotics for the Prophylaxis of Migraine: A Systematic Review of Randomized Placebo Controlled Trials. Journal of Clinical Medicine. 2019; 8(9):1441. https://doi.org/10.3390/jcm8091441
Chicago/Turabian StyleNaghibi, Malwina M., Richard Day, Samantha Stone, and Ashton Harper. 2019. "Probiotics for the Prophylaxis of Migraine: A Systematic Review of Randomized Placebo Controlled Trials" Journal of Clinical Medicine 8, no. 9: 1441. https://doi.org/10.3390/jcm8091441
APA StyleNaghibi, M. M., Day, R., Stone, S., & Harper, A. (2019). Probiotics for the Prophylaxis of Migraine: A Systematic Review of Randomized Placebo Controlled Trials. Journal of Clinical Medicine, 8(9), 1441. https://doi.org/10.3390/jcm8091441