Do Nutritional Factors Interact with Chronic Musculoskeletal Pain? A Systematic Review

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Search Strategy and Eligibility Criteria
- -
- Studies including adult human volunteers (above 18 years old);
- -
- Having at least 3 months of musculoskeletal pain or musculoskeletal system-originated chronic pain (i.e., chronic musculoskeletal pain);
- -
- Studies that solely investigate the link between nutrition and pain, and do not include any other treatment modality in experimental studies;
- -
- Studies written in English and published in internationally peer-reviewed journals;
- -
- Study types considered were randomised controlled trials, clinical trials (all phases), cohort studies, case–control studies, and cross-sectional studies.
2.3. Information Sources and Keywords
2.4. Study Selection
2.5. Data Extraction
2.6. Deviation from the Protocol
2.7. Risk of Bias Assessment
3. Results
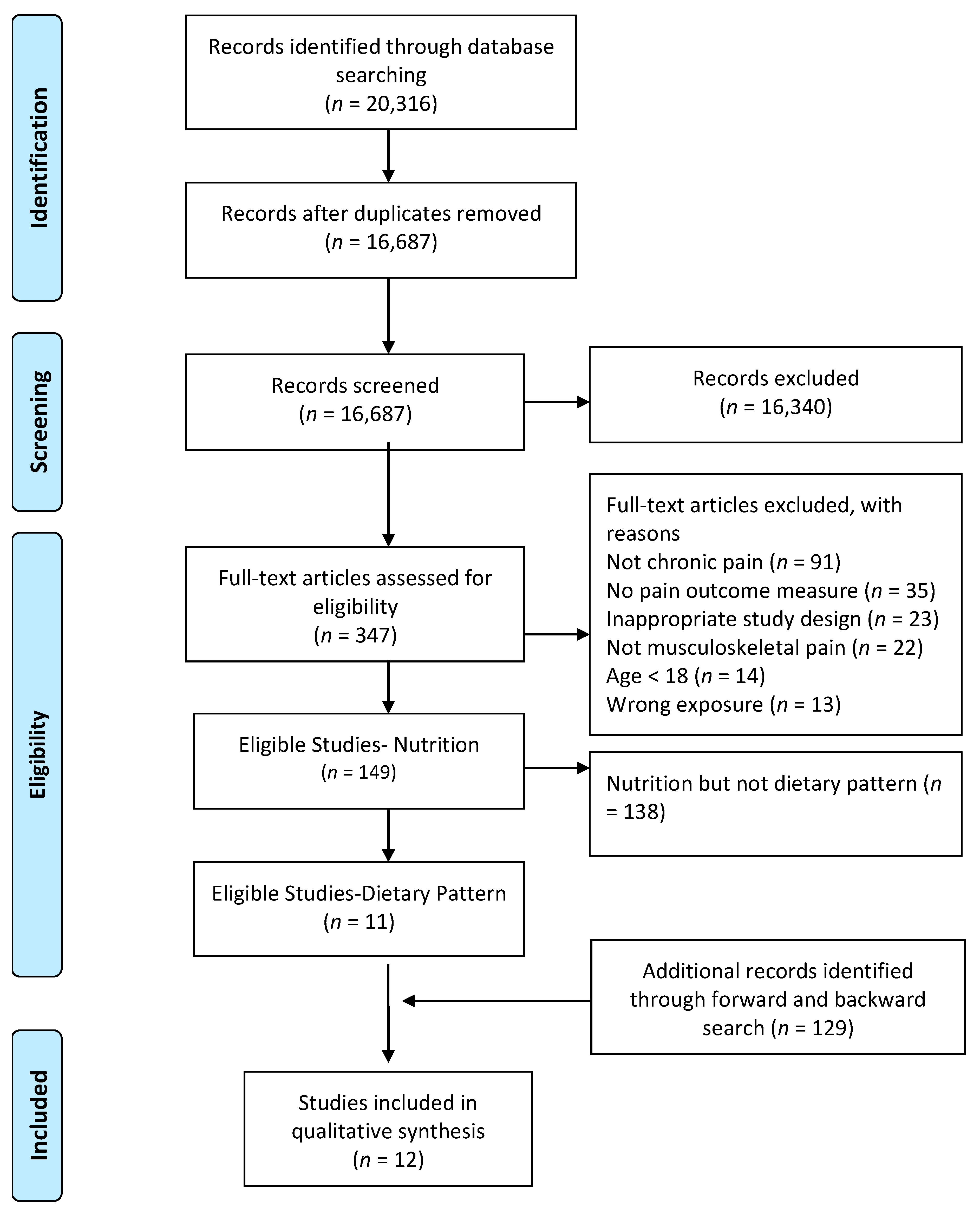
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias Assessment
3.4. Results of Individual Studies
Results from Experimental Studies: Effects of Dietary Pattern Change (i.e., Intervention) on Chronic Musculoskeletal Pain
(1) Vegetarian Diet
(2) Vegan Diet
(3) Weight Loss Diet
(4) Peptide Diet
(5) Monosodium Glutamate and Aspartame Eliminated Diet
(6) FODMAP Diet
4. Discussion
4.1. Strengths and Limitations
4.2. Recommendations for Further Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gatchel, R.J.; Peng, Y.B.; Peters, M.L.; Fuchs, P.N.; Turk, D.C. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol. Bull. 2007, 133, 581. [Google Scholar] [CrossRef] [PubMed]
- Marshall, P.W.; Schabrun, S.; Knox, M.F. Physical activity and the mediating effect of fear, depression, anxiety, and catastrophizing on pain related disability in people with chronic low back pain. PLoS ONE 2017, 12, e0180788. [Google Scholar] [CrossRef] [PubMed]
- Crofford, L.J. Psychological aspects of chronic musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 2015, 29, 147–155. [Google Scholar] [CrossRef] [Green Version]
- Lerman, S.F.; Rudich, Z.; Brill, S.; Shalev, H.; Shahar, G. Longitudinal associations between depression, anxiety, pain, and pain-related disability in chronic pain patients. Psychosom. Med. 2015, 77, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Dean, E.; Söderlund, A. What is the role of lifestyle behaviour change associated with non-communicable disease risk in managing musculoskeletal health conditions with special reference to chronic pain? Bmc Musculoskelet. Disord. 2015, 16, 87. [Google Scholar] [CrossRef] [PubMed]
- Okifuji, A.; Hare, B.D. The association between chronic pain and obesity. J. Pain Res. 2015, 8, 399–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abate, M.; Vanni, D.; Pantalone, A.; Salini, V. Cigarette smoking and musculoskeletal disorders. MusclesLigaments Tendons J. 2013, 3, 63. [Google Scholar] [CrossRef]
- Adler, G.K.; Geenen, R. Hypothalamic-pituitary-adrenal and autonomic nervous system functioning in fibromyalgia. Rheum. Dis. Clin. North Am. 2005, 31, 187–202,xi. [Google Scholar] [CrossRef]
- Snodgrass, S.J.; Heneghan, N.R.; Tsao, H.; Stanwell, P.T.; Rivett, D.A.; Van Vliet, P.M. Recognising neuroplasticity in musculoskeletal rehabilitation: A basis for greater collaboration between musculoskeletal and neurological physiotherapists. Man. Ther. 2014, 19, 614–617. [Google Scholar] [CrossRef]
- Lluch, E.; Torres, R.; Nijs, J.; Van Oosterwijck, J. Evidence for central sensitization in patients with osteoarthritis pain: A systematic literature review. Eur. J. Pain 2014, 18, 1367–1375. [Google Scholar] [CrossRef]
- Meeus, M.; Nijs, J. Central sensitization: A biopsychosocial explanation for chronic widespread pain in patients with fibromyalgia and chronic fatigue syndrome. Clin. Rheumatol. 2007, 26, 465–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giesecke, T.; Gracely, R.H.; Grant, M.A.; Nachemson, A.; Petzke, F.; Williams, D.A.; Clauw, D.J. Evidence of augmented central pain processing in idiopathic chronic low back pain. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 2004, 50, 613–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holton, K.F.; Kindler, L.L.; Jones, K.D. Potential dietary links to central sensitization in fibromyalgia: Past reports and future directions. Rheum. Dis. Clin. North Am. 2009, 35, 409–420. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Loggia, M.L.; Polli, A.; Moens, M.; Huysmans, E.; Goudman, L.; Meeus, M.; Vanderweeën, L.; Ickmans, K.; Clauw, D. Sleep disturbances and severe stress as glial activators: Key targets for treating central sensitization in chronic pain patients? Expert Opin. Ther. Targets 2017, 21, 817–826. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Diet, Nutrition, and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation; World Health Organization: Geneva, Switzerland, 2003; Volume 916. [Google Scholar]
- Boros, S. The Role of Nutrition in The Treatment of Chronic Musculoskeletal Diseases. Nutr. J. 2013, 12, 146. [Google Scholar] [CrossRef]
- Bell, R.F.; Borzan, J.; Kalso, E.; Simonnet, G. Food, pain, and drugs: Does it matter what pain patients eat? Pain 2012, 153, 1993–1996. [Google Scholar] [CrossRef]
- Bell, R.F. Food and Pain: Should We Be More Interested in What Our Patients Eat? LWW: Philadelphia, PA, USA, 2007. [Google Scholar]
- Wolff, A.E.; Jones, A.N.; Hansen, K.E. Vitamin D and musculoskeletal health. Nat. Rev. Rheumatol. 2008, 4, 580. [Google Scholar] [CrossRef]
- Mangano, K.M.; Sahni, S.; Kiel, D.P.; Tucker, K.L.; Dufour, A.B.; Hannan, M.T. Dietary protein is associated with musculoskeletal health independently of dietary pattern: The Framingham Third Generation Study. Am. J. Clin. Nutr. 2017, 105, 714–722. [Google Scholar] [CrossRef] [Green Version]
- Brain, K.; Burrows, T.; Rollo, M.; Chai, L.; Clarke, E.; Hayes, C.; Hodson, F.; Collins, C. A systematic review and meta-analysis of nutrition interventions for chronic noncancer pain. J. Hum. Nutr. Diet. 2018. [Google Scholar] [CrossRef]
- Rondanelli, M.; Faliva, M.A.; Miccono, A.; Naso, M.; Nichetti, M.; Riva, A.; Guerriero, F.; De Gregori, M.; Peroni, G.; Perna, S. Food pyramid for subjects with chronic pain: Foods and dietary constituents as anti-inflammatory and antioxidant agents. Nutr Res Rev 2018, 1–21. [Google Scholar] [CrossRef]
- Tick, H. Nutrition and pain. Phys. Med. Rehabil. Clin. N. Am. 2015, 26, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Di Lollo, A.C.; Guzzo, M.P.; Giacomelli, C.; Atzeni, F.; Bazzichi, L.; Di Franco, M. Fibromyalgia and nutrition: What news. Clin. Exp. Rheumatol 2015, 33, S117–S125. [Google Scholar] [PubMed]
- Ursini, F.; Naty, S.; Grembiale, R.D. Fibromyalgia and obesity: The hidden link. Rheumatol. Int. 2011, 31, 1403–1408. [Google Scholar] [CrossRef]
- Arranz, L.-I.; Canela, M.-Á.; Rafecas, M. Fibromyalgia and nutrition, what do we know? Rheumatol. Int. 2010, 30, 1417–1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadam, U.; Jordan, K.; Croft, P. Clinical comorbidity in patients with osteoarthritis: A case-control study of general practice consulters in England and Wales. Ann. Rheum. Dis. 2004, 63, 408–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiri, R.; Karppinen, J.; Leino-Arjas, P.; Solovieva, S.; Viikari-Juntura, E. The association between obesity and low back pain: A meta-analysis. Am. J. Epidemiol. 2010, 171, 135–154. [Google Scholar] [CrossRef] [Green Version]
- Stallings, S.P.; Kasdan, M.L.; Soergel, T.M.; Corwin, H.M. A case-control study of obesity as a risk factor for carpal tunnel syndrome in a population of 600 patients presenting for independent medical examination. J. Hand Surg. 1997, 22, 211–215. [Google Scholar] [CrossRef]
- Gurian, M.B.F.; Mitidieri, A.M.d.S.; da Silva, J.B.; Silva, A.P.M.d.; Pazin, C.; Poli-Neto, O.B.; Nogueira, A.A.; dos Reis, F.J.C.; Rosa-e-Silva, J.C. Measurement of pain and anthropometric parameters in women with chronic pelvic pain. J. Eval. Clin. Pract. 2015, 21, 21–27. [Google Scholar] [CrossRef]
- Lee, R.; Kean, W.F. Obesity and knee osteoarthritis. Inflammopharmacology 2012, 20, 53–58. [Google Scholar] [CrossRef]
- Hussain, S.M.; Urquhart, D.M.; Wang, Y.; Shaw, J.E.; Magliano, D.J.; Wluka, A.E.; Cicuttini, F.M. Fat mass and fat distribution are associated with low back pain intensity and disability: Results from a cohort study. Arthritis Res. 2017, 19, 26. [Google Scholar] [CrossRef] [Green Version]
- Neumann, L.; Lerner, E.; Glazer, Y.; Bolotin, A.; Shefer, A.; Buskila, D. A cross-sectional study of the relationship between body mass index and clinical characteristics, tenderness measures, quality of life, and physical functioning in fibromyalgia patients. Clin. Rheumatol. 2008, 27, 1543–1547. [Google Scholar] [CrossRef] [PubMed]
- Yunus, M.B.; Arslan, S.; Aldag, J.C. Relationship between body mass index and fibromyalgia features. Scand. J. Rheumatol. 2002, 31, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Lotfi, A.; Abdel-Nasser, A.M.; Hamdy, A.; Omran, A.A.; El-Rehany, M.A. Hypovitaminosis D in female patients with chronic low back pain. Clin. Rheumatol. 2007, 26, 1895–1901. [Google Scholar] [CrossRef] [PubMed]
- Vormann, J.; Worlitschek, M.; Goedecke, T.; Silver, B. Supplementation with alkaline minerals reduces symptoms in patients with chronic low back pain. J. Trace Elem. Med. Biol. 2001, 15, 179–183. [Google Scholar] [CrossRef]
- Ruggiero, C.; Lattanzio, F.; Lauretani, F.; Gasperini, B.; Andres-Lacueva, C.; Cherubini, A. Ω-3 polyunsaturated fatty acids and immune-mediated diseases: Inflammatory bowel disease and rheumatoid arthritis. Curr. Pharm. Des. 2009, 15, 4135–4148. [Google Scholar] [CrossRef]
- Bjørklund, G.; Dadar, M.; Chirumbolo, S.; Aaseth, J. Fibromyalgia and nutrition: Therapeutic possibilities? Biomed. Pharmacother. 2018, 103, 531–538. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Tapsell, L.C.; Neale, E.P.; Satija, A.; Hu, F.B. Foods, nutrients, and dietary patterns: Interconnections and implications for dietary guidelines. Adv. Nutr. 2016, 7, 445–454. [Google Scholar] [CrossRef]
- Tindall, A.M.; Petersen, K.S.; Kris-Etherton, P.M. Dietary patterns affect the gut microbiome—the link to risk of cardiometabolic diseases. J. Nutr. 2018, 148, 1402–1407. [Google Scholar] [CrossRef] [Green Version]
- Calle, M.C.; Andersen, C.J. Assessment of Dietary Patterns Represents a Potential, Yet Variable, Measure of Inflammatory Status: A Review and Update. Dis. Markers 2019, 2019, 3102870. [Google Scholar]
- Lahoz, C.; Castillo, E.; Mostaza, J.M.; de Dios, O.; Salinero-Fort, M.A.; González-Alegre, T.; García-Iglesias, F.; Estirado, E.; Laguna, F.; Sanchez, V. Relationship of the Adherence to a Mediterranean Diet and Its Main Components with CRP Levels in the Spanish Population. Nutrients 2018, 10, 379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbaresko, J.; Koch, M.; Schulze, M.B.; Nöthlings, U. Dietary pattern analysis and biomarkers of low-grade inflammation: A systematic literature review. Nutr. Rev. 2013, 71, 511–527. [Google Scholar] [CrossRef] [PubMed]
- Wirth, M.D.; Hébert, J.R.; Shivappa, N.; Hand, G.A.; Hurley, T.G.; Drenowatz, C.; McMahon, D.; Shook, R.P.; Blair, S.N. Anti-inflammatory Dietary Inflammatory Index scores are associated with healthier scores on other dietary indices. Nutr. Res. 2016, 36, 214–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reedy, J.; Lerman, J.L.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the healthy eating index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prospero Database Web Page. Available online: https://www.crd.york.ac.uk/PROSPERO/ (accessed on 3 March 2020).
- Batista, E.D.; Andretta, A.; de Miranda, R.C.; Nehring, J.; Dos Santos Paiva, E.; Schieferdecker, M.E. Food intake assessment and quality of life in women with fibromyalgia. Rev. Bras. Reum. Engl. Ed. 2016, 56, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Choi, K.W.; Somers, T.J.; Babyak, M.A.; Sikkema, K.J.; Blumenthal, J.A.; Keefe, F.J. The relationship between pain and eating among overweight and obese individuals with osteoarthritis: An ecological momentary study. Pain Res. Manag. 2014, 19, e159–e163. [Google Scholar] [CrossRef]
- Hejazi, J.; Mohtadinia, J.; Kolahi, S.; Bakhtiyari, M.; Delpisheh, A. Nutritional status of Iranian women with rheumatoid arthritis: An assessment of dietary intake and disease activity. Women’s Health (Lond. Engl.) 2011, 7, 599–605. [Google Scholar] [CrossRef]
- Bellare, N.; Argekar, H.; Bhagwat, A.; Situt, V.; Pandita, N. Glucosamine and chondroitin sulphate supplementation along with diet therapy provides better symptomatic relief in osteoarthritic patients as compared to diet therapy alone. Int. J. Pharm. Sci. Rev. Res. 2014, 24, 215–223. [Google Scholar]
- Holst-Jensen, M.; Pfeiffer-Jensen, M.; Monsrud, U.; Tarp, A.; Buus, I.; Hessov, E.; Thorling, K.; Stengaard-Pedersen, S.E. Treatment of rheumatoid arthritis with a peptide diet: A randomized, controlled trial. Scand. J. Rheumatol. 1998, 27, 329–336. [Google Scholar] [CrossRef]
- Riecke, B.F.; Christensen, R.; Christensen, P.; Leeds, A.R.; Boesen, M.; Lohmander, L.S.; Astrup, A.; Bliddal, H. Comparing two low-energy diets for the treatment of knee osteoarthritis symptoms in obese patients: A pragmatic randomized clinical trial. Osteoarthr. Cartil. 2010, 18, 746–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sköldstam, L.; Larsson, L.; Lindström, F.D. Effects of fasting and lactovegetarian diet on rheumatoid arthritis. Scand. J. Rheumatol. 1979, 8, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Vellisca, M.Y.; Latorre, J.I. Monosodium glutamate and aspartame in perceived pain in fibromyalgia. Rheumatol. Int. 2014, 34, 1011–1013. [Google Scholar] [CrossRef] [PubMed]
- Kaartinen, K.; Lammi, K.; Hypen, M.; Nenonen, M.; Hänninen, O.; Rauma, A.-L. Vegan diet alleviates fibromyalgia symptoms. Scand. J. Rheumatol. 2000, 29, 308–313. [Google Scholar] [CrossRef]
- Marum, A.P.; Moreira, C.; Tomas-Carus, P.; Saraiva, F.; Guerreiro, C.S. A low fermentable oligo-di-mono-saccharides and polyols (FODMAP) diet is a balanced therapy for fibromyalgia with nutritional and symptomatic benefits. Nutr Hosp 2017, 34, 667–674. [Google Scholar] [CrossRef]
- McDougall, J.; Bruce, B.; Spiller, G.; Westerdahl, J.; McDougall, M. Effects of a very low-fat, vegan diet in subjects with rheumatoid arthritis. J. Altern. Complementary Med. 2002, 8, 71–75. [Google Scholar] [CrossRef]
- Towery, P.; Guffey, J.S.; Doerflein, C.; Stroup, K.; Saucedo, S.; Taylor, J. Chronic musculoskeletal pain and function improve with a plant-based diet. Complement. Med. 2018, 40, 64–69. [Google Scholar] [CrossRef]
- Escott-Stump, S.; Mahan, L.K. Krause’s Food & Nutrition Therapy; Saunders/Elsevier: St. Louis, Mo, USA, 2008. [Google Scholar]
- Clarys, P.; Deriemaeker, P.; Huybrechts, I.; Hebbelinck, M.; Mullie, P. Dietary pattern analysis: A comparison between matched vegetarian and omnivorous subjects. Nutr. J. 2013, 12, 82. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Chen, J.; Wirth, M.; Shivappa, N.; Hebert, J. Lower dietary inflammatory index scores are associated with lower glycemic index scores among college students. Nutrients 2018, 10, 182. [Google Scholar] [CrossRef] [Green Version]
- Steck, S.; Shivappa, N.; Tabung, F.; Harmon, B.; Wirth, M.; Hurley, T.; Hebert, J. The dietary inflammatory index: A new tool for assessing diet quality based on inflammatory potential. Digest 2014, 49, 1–10. [Google Scholar]
- Briggs, M.S.; Givens, D.L.; Schmitt, L.C.; Taylor, C.A. Relations of C-reactive protein and obesity to the prevalence and the odds of reporting low back pain. Arch. Phys. Med. Rehabil. 2013, 94, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Ortega, E.; García, J.; Bote, M.; Martin-Cordero, L.; Escalante, Y.; Saavedra, J.; Northoff, H.; Giraldo, E. Exercise in fibromyalgia and related inflammatory disorders: Known effects and unknown chances. Exerc. Immunol. Rev. 2009, 15, 42–44. [Google Scholar] [PubMed]
- Gerber, N.L.; Sikdar, S.; Hammond, J.; Shah, J. A brief overview and update of myofascial pain syndrome and myofascial trigger points. J. Spinal Res. Found. Spring 2011, 6. [Google Scholar]
- Stürmer, T.; Brenner, H.; Koenig, W.; Günther, K. Severity and extent of osteoarthritis and low grade systemic inflammation as assessed by high sensitivity C reactive protein. Ann. Rheum. Dis. 2004, 63, 200–205. [Google Scholar] [CrossRef] [Green Version]
- Barbe, M.F.; Barr, A.E. Inflammation and the pathophysiology of work-related musculoskeletal disorders. BrainBehav. Immun. 2006, 20, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Seaman, D.R. The diet-induced proinflammatory state. J. Manip. Physiol. Ther. 2002, 25, 168–179. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.M.; An, J. Cytokines, inflammation, and pain. Int. Anesth. Clin. 2007, 45, 27–37. [Google Scholar] [CrossRef] [Green Version]
- Nijs, J.; Van Houdenhove, B.; Oostendorp, R.A. Recognition of central sensitization in patients with musculoskeletal pain: Application of pain neurophysiology in manual therapy practice. Man. Ther. 2010, 15, 135–141. [Google Scholar] [CrossRef]
- Iglesias-González, J.J.; Muñoz-García, M.T.; Rodrigues-de-Souza, D.P.; Alburquerque-Sendín, F.; Fernández-de-Las-Peñas, C. Myofascial trigger points, pain, disability, and sleep quality in patients with chronic nonspecific low back pain. Pain Med. 2013, 14, 1964–1970. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Simons, D.G.; Cuadrado, M.L.; Pareja, J.A. The role of myofascial trigger points in musculoskeletal pain syndromes of the head and neck. Curr. Pain Headache Rep. 2007, 11, 365–372. [Google Scholar] [CrossRef]
- Ge, H.-Y.; Nie, H.; Madeleine, P.; Danneskiold-Samsøe, B.; Graven-Nielsen, T.; Arendt-Nielsen, L. Contribution of the local and referred pain from active myofascial trigger points in fibromyalgia syndrome. PAIN® 2009, 147, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.P.; Danoff, J.V.; Desai, M.J.; Parikh, S.; Nakamura, L.Y.; Phillips, T.M.; Gerber, L.H. Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Arch. Phys. Med. Rehabil. 2008, 89, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Mense, S. The pathogenesis of muscle pain. Curr. Pain Headache Rep. 2003, 7, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Srbely, J.; Vadasz, B.; Shah, J.; Gerber, N.L.; Sikdar, S.; Kumbhare, D. Central sensitization: A clinical conundrum. Clin. J. Pain 2016, 32, 1011–1013. [Google Scholar] [CrossRef]
- Simopoulos, A.P. The Mediterranean diets: What is so special about the diet of Greece? The scientific evidence. J. Nutr. 2001, 131, 3065S–3073S. [Google Scholar] [CrossRef]
- Tomova, A.; Bukovsky, I.; Rembert, E.; Yonas, W.; Alwarith, J.; Barnard, N.D.; Kahleova, H. The Effects of Vegetarian and Vegan Diets on Gut Microbiota. Front. Nutr. 2019, 6, 47. [Google Scholar] [CrossRef] [Green Version]
- Pimentel, G.D.; Micheletti, T.O.; Pace, F.; Rosa, J.C.; Santos, R.V.; Lira, F.S. Gut-central nervous system axis is a target for nutritional therapies. Nutr. J. 2012, 11, 22. [Google Scholar] [CrossRef] [Green Version]
- Hakansson, A.; Molin, G. Gut microbiota and inflammation. Nutrients 2011, 3, 637–682. [Google Scholar] [CrossRef]
- Ronti, T.; Lupattelli, G.; Mannarino, E. The endocrine function of adipose tissue: An update. Clin. Endocrinol. 2006, 64, 355–365. [Google Scholar] [CrossRef]
- Peniston, J.H. A review of pharmacotherapy for chronic low back pain with considerations for sports medicine. Physician Sportsmed. 2012, 40, 21–32. [Google Scholar] [CrossRef]
- Gore, M.; Tai, K.S.; Sadosky, A.; Leslie, D.; Stacey, B.R. Use and costs of prescription medications and alternative treatments in patients with osteoarthritis and chronic low back pain in community-based settings. Pain Pract. 2012, 12, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Griffith, J.A.; Chasan-Taber, L.; Olendzki, B.C.; Jackson, E.; Stanek III, E.J.; Li, W.; Pagoto, S.L.; Hafner, A.R.; Ockene, I.S. Association between dietary fiber and serum C-reactive protein. Am. J. Clin. Nutr. 2006, 83, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Lowe, G.D.; Rumley, A.; Bruckdorfer, K.R.; Whincup, P.H. Associations of vitamin C status, fruit and vegetable intakes, and markers of inflammation and hemostasis. Am. J. Clin. Nutr. 2006, 83, 567–574. [Google Scholar] [CrossRef]
- Murphy, R.T.; Foley, J.B.; Tome, M.-T.; Mulvihill, N.T.; Murphy, A.; McCarroll, N.; Crean, P.; Walsh, M.J. Vitamin E modulation of C-reactive protein in smokers with acute coronary syndromes. Free Radic. Biol. Med. 2004, 36, 959–965. [Google Scholar] [CrossRef]
- Ferrucci, L.; Cherubini, A.; Bandinelli, S.; Bartali, B.; Corsi, A.; Lauretani, F.; Martin, A.; Andres-Lacueva, C.; Senin, U.; Guralnik, J.M. Relationship of plasma polyunsaturated fatty acids to circulating inflammatory markers. J. Clin. Endocrinol. Metab. 2006, 91, 439–446. [Google Scholar] [CrossRef]
- Castro-Quezada, I.; Román-Viñas, B.; Serra-Majem, L. The Mediterranean diet and nutritional adequacy: A review. Nutrients 2014, 6, 231–248. [Google Scholar] [CrossRef] [Green Version]
- Galland, L. Diet and inflammation. Nutr. Clin. Pract. 2010, 25, 634–640. [Google Scholar] [CrossRef]
- Zeisel, S.H. Is there a new component of the Mediterranean diet that reduces inflammation? Am. J. Clin. Nutr. 2008, 87, 277–278. [Google Scholar] [CrossRef] [Green Version]
- Hodge, A.M.; Bassett, J.K.; Dugué, P.-A.; Shivappa, N.; Hébert, J.R.; Milne, R.; English, D.R.; Giles, G.G. Dietary inflammatory index or Mediterranean diet score as risk factors for total and cardiovascular mortality. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 461–469. [Google Scholar] [CrossRef]
- Forsyth, C.; Kouvari, M.; D’Cunha, N.M.; Georgousopoulou, E.N.; Panagiotakos, D.B.; Mellor, D.D.; Kellett, J.; Naumovski, N. The effects of the Mediterranean diet on rheumatoid arthritis prevention and treatment: A systematic review of human prospective studies. Rheumatol. Int. 2018, 38, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Sköldstam, L.; Hagfors, L.; Johansson, G. An experimental study of a Mediterranean diet intervention for patients with rheumatoid arthritis. Ann. Rheum. Dis. 2003, 62, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Joustra, M.L.; Minovic, I.; Janssens, K.A.; Bakker, S.J.; Rosmalen, J.G. Vitamin and mineral status in chronic fatigue syndrome and fibromyalgia syndrome: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0176631. [Google Scholar] [CrossRef] [Green Version]
- Kjeldsen-Kragh, J.; Haugen, M.; Førre, Ø.; Laache, H.; Malt, U. Vegetarian diet for patients with rheumatoid arthritis: Can the clinical effects be explained by the psychological characteristics of the patients? Rheumatology 1994, 33, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, P.; Yadav, R.K. Measuring pain in clinical trials: Pain scales, endpoints, and challenges. Int. J. Clin. Exp. Physiol. 2015, 2, 151–156. [Google Scholar] [CrossRef]
- Ahlers, S.J.; van Gulik, L.; van der Veen, A.M.; van Dongen, H.P.; Bruins, P.; Belitser, S.V.; de Boer, A.; Tibboel, D.; Knibbe, C.A. Comparison of different pain scoring systems in critically ill patients in a general ICU. Crit. Care 2008, 12, R15. [Google Scholar] [CrossRef] [Green Version]
- Wagemakers, S.H.; van der Velden, J.M.; Gerlich, A.S.; Hindriks-Keegstra, A.W.; van Dijk, J.F.; Verhoeff, J.J. A Systematic Review of Devices and Techniques that Objectively Measure Patients’ Pain. Pain Physician 2019, 22, 1–13. [Google Scholar]


{kind=link}
| Author (Year) (Reference) and Condition | Design and Duration | Participant Number (Female), Age, Body Mass Index | Intervention (or Case) Group | Control Group | Outcome Measures | Findings |
|---|---|---|---|---|---|---|
| Observational Studies | ||||||
| Batista et al. (2016) [49] and FB | CC | FB: 43 (43 F) 49 ± 7.92 26.96 ± 4.64 C: 44 (44 F) 46.8 ± 10.36 25.72 ± 3.76 | Three-day dietary record was used to find out intake of total calories, carbohydrates, lipids, vitamins (A, C, B12, D, and K), and minerals (folate, selenium, zinc, iron, calcium, and magnesium). Additionally, in order to investigate the association between nutrient intake and pain severity, pain pressure threshold was used, and measurement area was right trapezius muscle. | Healthy people | Three-day food diary PPTs | Healthy control group showed significantly higher caloric intake and intake of carbohydrates, proteins, lipids, vitamin A, vitamin E, vitamin K, folate, selenium, and calcium. There was no significant difference in intake of iron. Additionally, there was only a significant positive correlation between protein intake and pain. |
| Choi et al. (2014) [50] and OA | CS | OA: 54 (49 F) 62.7 ± 9.3 32.6 ± 4.8 | Two-day dietary record used in order to measure the food intake of patients. Additionally, VAS pain scale used in order to assess the pain intensity and its relationship with food and nutrient intake. | No control group | Food diary VAS | Among obese or overweight OA patients who have chronic pain, pain severity is positively correlated with calorie and fat intake. Patients who have severe pain reported more intake of sugar and fat. |
| Hejazi et al. (2011) [51] and RA | CS | I: 90 (90 F) 47.47 ± 13.68 23.9 ± 1.59 | Patients’ dietary and nutrient intakes were analysed and compared with the standard dietary reference intake values. | No control group | Three-day food diary VAS | Intake of energy and micronutrients including calcium, folic acid, zinc, magnesium, and vitamin B6 were considerably lower compared with the dietary reference values. On the other hand, intake of protein, copper, and vitamin E met or exceeded the recommended dietary reference value in most of the patients. Pain severity did not show any significant correlation with any nutrient intakes. |
| Interventional Studies | ||||||
| Bellare et al. (2014) [52] and OA | RCT and 1 year | I: 61 (50 F) 59.98 ± 8.81 27.36 ± 3.71 C: 56 (40 F) 60.70 ± 8.31 27.68 ± 3.03 | Weight loss diet alone and with supplement: Intervention group, diet, and supplement group were supplemented with glucosamine (1500 mg) and chondroitin (1200 mg) sulphate per day, in addition to the same diet therapy as diet-only group (weight lose diet). Control group and diet-only group received weight loss diet which is a balanced energy-controlled diet supplying 1200–1400 kcal per day (carbohydrate 50%–55%, protein 15%–25%, fat < 30%). | Weight loss diet alone | VAS (0 to 10) WOMAC pain | A total of 16 patients from diet-only group and 12 patients from diet and supplementation group withdrew. Both diet-only and diet with supplement group showed significant decrease in pain after 6 months and 1 year (p ≤ 0.05). However, pain better improved according to the VAS and WOMAC scores in the supplement group after 1 year. Additionally, in the first 6 months, improvements in pain were faster than the second 6 months. |
| Holst-Jensen (1998) [53] and RA | RCT and 6 months | I: 15 (10 F) Mean age = 56 (range 34–70) BMI = NR C: 15 (14 F) Mean age = 46 (range 29–72) BMI = NR | eptide diet: Patients were explained the artificial elemental diet and were given a commercialised liquid diet (TU). The liquid diet contained soy protein, methionine, tryptophan, vitamins, and trace elements. The diet lasted 4 weeks and then patients were followed for 6 months in total from the baseline until the end. During the peptide diet, patients were not allowed to eat and drink any other foods or beverages except for water and plain soda water. | Normal food intake | VAS (0 to 10) | A total of 2 and 1 patients withdrew from the intervention and control group, respectively. Pain now, average pain, and worst pain during the last week were measured. Only average pain during the last week significantly improved after the 4 weeks of intervention from 5(1.4/7.0) to 4(1.4/6.6) (p = 0.02). However, this effect disappeared at the 3 month follow up, and there was no between-group differences. |
| Riecke et al. (2010) [54] and OA | RCT and 16 weeks | I: 96 (78 F) 61.8 ± 6.4 37.5 ± 5.4 C: 96 (77 F) 63.3 ± 6.3 37.1 ± 4.1 | Very low energy diet: Patients (BMI > 30 kg/m2) were expected to follow a very low energy diet (415 kcal/day) in the intervention group and were expected to follow a low energy diet (810 kcal/day) in the control group for 8 weeks. After that, both groups followed a hypo-energetic diet (1200 kcal/day) for a second 8 weeks. | Low-energy diet | VAS (0 to 100) | A total of 10 patients from the very low energy diet group and 7 patients from the low energy diet group withdrew. Pain significantly decreased in both groups after 16 weeks, with a pooled average for pain 9.72 (95% CI: 7.72–11.72; p < 0.001). However, there were no significant difference between the groups. |
| Sköldstam, Larsson, and Lindström (1979) [55] and RA | RCT and 10 weeks | I: 16 (10 F) Mean Age = 52 (range = 35–66) BMI = NR C: 10 (9 F) Mean age = 54 (range = 43–65) BMI = NR | Fasting and lactovegetarian diet: After fasting for 7–10 days, participants followed a lactovegetarian dietary pattern for the following 9 weeks with a 1 week resting period between fasting and vegetarian diet. During fasting, daily energy supply was 800 kJ. During the lactovegetarian period, no animal or fish protein, egg, alcohol, tobacco, coffee, or tea allowed. | Normal diet | VAS (0 to 10) | One patient during the fasting and one patient during the vegetarian diet withdrew from the study. After fasting, only five patients showed significant improvement in pain. However, there was no significant difference in pain after the lactovegetarian dietary pattern. |
| Vellisca and Latorre (2014) [56] and FB | RCT and 3 months | I: 36 (36 F) 42.33 ± 8.43 NR C: 36 (36 F) 39.64 ± 8.16 NR | Monosodium glutamate and aspartame eliminated diet: Patients were educated to detect and eliminate the monosodium glutamate and aspartame from their diet. They were expected to follow this diet for 3 months. | Normal diet | NPRS (0 to 7) | Monosodium glutamate and aspartame eliminated diet did not show a significant effect compared to normal dietary pattern (p = 0.178). |
| Kaartinen et al. (2000) [57] and FB | NCT and 3 months | I: 18 (18 F) mean age = 51 mean BMI = 28 C: 15 (15 F) mean age = 52 mean BMI = 28 | Vegan diet: Patients were educated to prepare their diet according to the rules of the dietary pattern for 3 months. After 3 months, they continued their normal omnivorous diet, the diet that they wanted to follow. | Omnivorous Diet | VAS | The results revealed significant improvements in visual analogue scale of pain after 3 months of vegan diet (p = 0.005). However, this significant improvement disappeared after shifting to omnivorous diet gradually. |
| Marum et al. (2017) [58] and FB | UCT and 8 weeks | I: 38 (38 F) mean age = 51 27.4 ± 4.6 | A low fermentable oligo-di-monosaccharides and polyols (FODMAP) diet: Subjects were educated according to the FODMAP diet and were expected to follow this diet as an intervention for 8 weeks. | No control group | VAS (0 to 10) | Seven participants withdrew from the study. Pain measurement showed a statistically significant decrease after the fourth week. This significance did not exist between the fourth and eighth week. However, compared to baseline, pain significantly decreased after 8 weeks (week 0 = 6.6, week 4 = 4.9, week 8 = 5.4) (p < 0.01). |
| McDougall et al. (2002) [59] and RA | UCT and 4 weeks | I: 24 (23) 56 ± 11 NR | Very low fat vegan diet: Four meetings held in order to teach a low-fat vegan diet to the participants. They were expected to follow a low-fat vegan diet for 4 weeks. The diet contained no animal products or added fats and oils of any kind. | No control group | VAS (0 TO 100) | No one withdrew from the study. Pain significantly decreased compared to baseline from 49 ± 20 to 34 ± 20 (p < 0.04). |
| Towery et al. (2018) [60] and MSK | UCT and 8 weeks | I: 14 (12 F) 48.07 ± 16.92 36.13 ± 10.45 | Lacto-ovo vegetarian diet: Patients have been given an education on plant-based diet and were expected to follow this dietary pattern for 8 weeks. Meat, poultry, seafood, and fish were not allowed. | No control group | NPRS (0 TO 10) SF-36 pain | No drop outs. Pain rating significantly decreased with an average of 3.14 point in NPRS (p = 0.0001). Pain rate in SF-36 significantly decreased an average of 25.53 points (p = 0.0001). |
| Author (Year) | Selection Bias | Performance Bias | Detection Bias | Attrition Bias | Reporting Bias | Other Bias | Total | |
|---|---|---|---|---|---|---|---|---|
| Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Anything Else, Ideally Prespecified | Good Fair Poor | |
| Bellare et al. (2014) [52] | Unclear | Unclear | High | High | Unclear | Low | Poor | |
| Riecke et al. (2010) [54] | Low | Low | Low | Low | Low | Low | Good | |
| Holst-Jensen (1998) [53] | Low | Low | Unclear | Unclear | Low | Low | Fair | |
| Sköldstam, Larsson, and Lindström (1979) [55] | Unclear | Unclear | Unclear | Unclear | High | Low | Poor | |
| Vellisca and Latorre (2014) [56] | Unclear | Unclear | Unclear | Unclear | Low | Low | Poor | |
| Selection Bias | ||||||||
| - Criterion 1: Selection bias (biased allocation to interventions) due to inadequate generation of a randomised sequence. | ||||||||
| - Criteria 2: Selection bias (biased allocation to interventions) due to inadequate concealment of allocations prior to assignment. | ||||||||
| Performance Bias | ||||||||
| - Criterion 1: Performance bias due to knowledge of the allocated interventions by participants and personnel during the study. | ||||||||
| Detection Bias | ||||||||
| - Criterion 1: Detection bias due to knowledge of the allocated interventions by outcome assessors. | ||||||||
| Attrition Bias | ||||||||
| - Criterion 1: Attrition bias due to amount, nature, or handling of incomplete outcome data. | ||||||||
| Reporting Bias | ||||||||
| - Criterion 1: Reporting bias due to selective outcome reporting. | ||||||||
| Other Bias | ||||||||
| - Criterion 1: Bias due to problems not covered elsewhere in the table. | ||||||||
| ASSESSMENT CRITERIA Non-Randomised Controlled Trials Uncontrolled Clinical Trials | Kaartinen et al. (2000) [57] | Marum et al. (2017) [58] | Towery et al. (2018) [60] | McDougall et al. (2002) [59] |
|---|---|---|---|---|
| 1. Question/objective sufficiently described? | YES | YES | YES | YES |
| 2. Study design evident and appropriate? | YES | YES | PARTIAL | PARTIAL |
| 3. Method of subject/comparison group selection or source of information/input variables described and appropriate? | PARTIAL | YES | YES | YES |
| 4. Subject (and comparison group, if applicable) characteristics sufficiently described? | YES | YES | YES | YES |
| 5. If interventional and random allocation was possible, was it described? | NO | N/A | N/A | N/A |
| 6. If interventional and blinding of investigators was possible, was it reported? | NO | N/A | N/A | PARTIAL |
| 7. If interventional and blinding of subjects was possible, was it reported? | N/A | N/A | N/A | N/A |
| 8. Outcome and (if applicable) exposure measure(s) well defined and robust to measurement/misclassification bias? Means of assessment reported? | YES | YES | YES | YES |
| 9. Sample size appropriate? | PARTIAL | PARTIAL | PARTIAL | PARTIAL |
| 10. Analytic methods described/justified and appropriate? | YES | YES | YES | YES |
| 11. Some estimate of variance is reported for the main results? | YES | YES | YES | PARTIAL |
| 12. Controlled for confounding? | PARTIAL | YES | YES | PARTIAL |
| 13. Results reported in sufficient detail? | YES | YES | YES | YES |
| 14. Conclusions supported by the results? | YES | YES | YES | YES |
| TOTAL | 0.73 | 0.90 | 0.90 | 0.79 |
| Author (Year) and Study Design | Selection | Comparability | EXPOSURE for Case Control Studies/or OUTCOME for Cross Sectional Studies | Total Stars | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| S1 | S2 | S3 | S4 | C1 | C2 | E1/O1 | E2/O2 | E3 | ||
| Choi et al. (2014) [50] and cross-sectional | * | * | - | N/A | * | * | - | * | N/A | 5/7 |
| Hejazi et al. (2011) [51] and cross-sectional | * | * | * | N/A | * | * | - | * | N/A | 5/7 |
| Batista et al. (2016) [49] and case–control | * | - | * | * | * | * | * | * | - | 7/9 |
| Selection | ||||||||||
| - S1 for case–control studies; is the case definition adequate? | ||||||||||
| - S1 for cross-sectional studies; representativeness of the sample. | ||||||||||
| - S2 for case–control studies; representativeness of the cases. | ||||||||||
| - S2 for cross-sectional studies; non-respondents. | ||||||||||
| - S3 for case–control studies; selection of the controls. | ||||||||||
| - S3 for cross-sectional studies; ascertainment of the exposure. | ||||||||||
| - S4 for case–control studies; definition of the control. | ||||||||||
| Comparability | ||||||||||
| - C1 for case–control studies; study controls for most important factor. | ||||||||||
| - C1 for cross-sectional studies; study controls for most important factor. | ||||||||||
| - C2 for case–control studies; study controls for any additional factors. | ||||||||||
| - C2 for cross-sectional studies; study controls for any additional factors. | ||||||||||
| Exposure | ||||||||||
| - E1; ascertainment of exposure. | ||||||||||
| - E2; same method of ascertainment of cases and controls. | ||||||||||
| - E3; non-response rate. | ||||||||||
| Outcome | ||||||||||
| - O1; assessment of outcome. | ||||||||||
| - O2; statistical analysis. | ||||||||||
| Level of Evidence | Intervention |
|---|---|
| A1 | Systematic review of at least two studies conducted independently from each other of evidence level A2. |
| A2 | Randomised double-blinded comparative clinical research of good quality and efficient size |
| B | Comparative research, but not with all characteristics mentioned for A2. This also includes patient– control research and cohort research. |
| C | Non-comparative research. |
| D | Opinion of experts. |
| Level of Conclusion | Conclusion Based on |
|---|---|
| 1 | Research of evidence level A1 or at least two independently conducted studies of evidence level A2. |
| 2 | One research of evidence level A2 or at least two independently conducted studies of evidence level B. |
| 3 | One research of evidence level B or C. |
| 4 | Opinion of experts or inconclusive or inconsistent results between various studies. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elma, Ö.; Yilmaz, S.T.; Deliens, T.; Coppieters, I.; Clarys, P.; Nijs, J.; Malfliet, A. Do Nutritional Factors Interact with Chronic Musculoskeletal Pain? A Systematic Review. J. Clin. Med. 2020, 9, 702. https://doi.org/10.3390/jcm9030702
Elma Ö, Yilmaz ST, Deliens T, Coppieters I, Clarys P, Nijs J, Malfliet A. Do Nutritional Factors Interact with Chronic Musculoskeletal Pain? A Systematic Review. Journal of Clinical Medicine. 2020; 9(3):702. https://doi.org/10.3390/jcm9030702
Chicago/Turabian StyleElma, Ömer, Sevilay Tümkaya Yilmaz, Tom Deliens, Iris Coppieters, Peter Clarys, Jo Nijs, and Anneleen Malfliet. 2020. "Do Nutritional Factors Interact with Chronic Musculoskeletal Pain? A Systematic Review" Journal of Clinical Medicine 9, no. 3: 702. https://doi.org/10.3390/jcm9030702
APA StyleElma, Ö., Yilmaz, S. T., Deliens, T., Coppieters, I., Clarys, P., Nijs, J., & Malfliet, A. (2020). Do Nutritional Factors Interact with Chronic Musculoskeletal Pain? A Systematic Review. Journal of Clinical Medicine, 9(3), 702. https://doi.org/10.3390/jcm9030702