Three-Dimensional Identification of the Medial Longitudinal Fasciculus in the Human Brain: A Diffusion Tensor Imaging Study


Abstract
:1. Introduction
2. Methods
2.1. Subjects
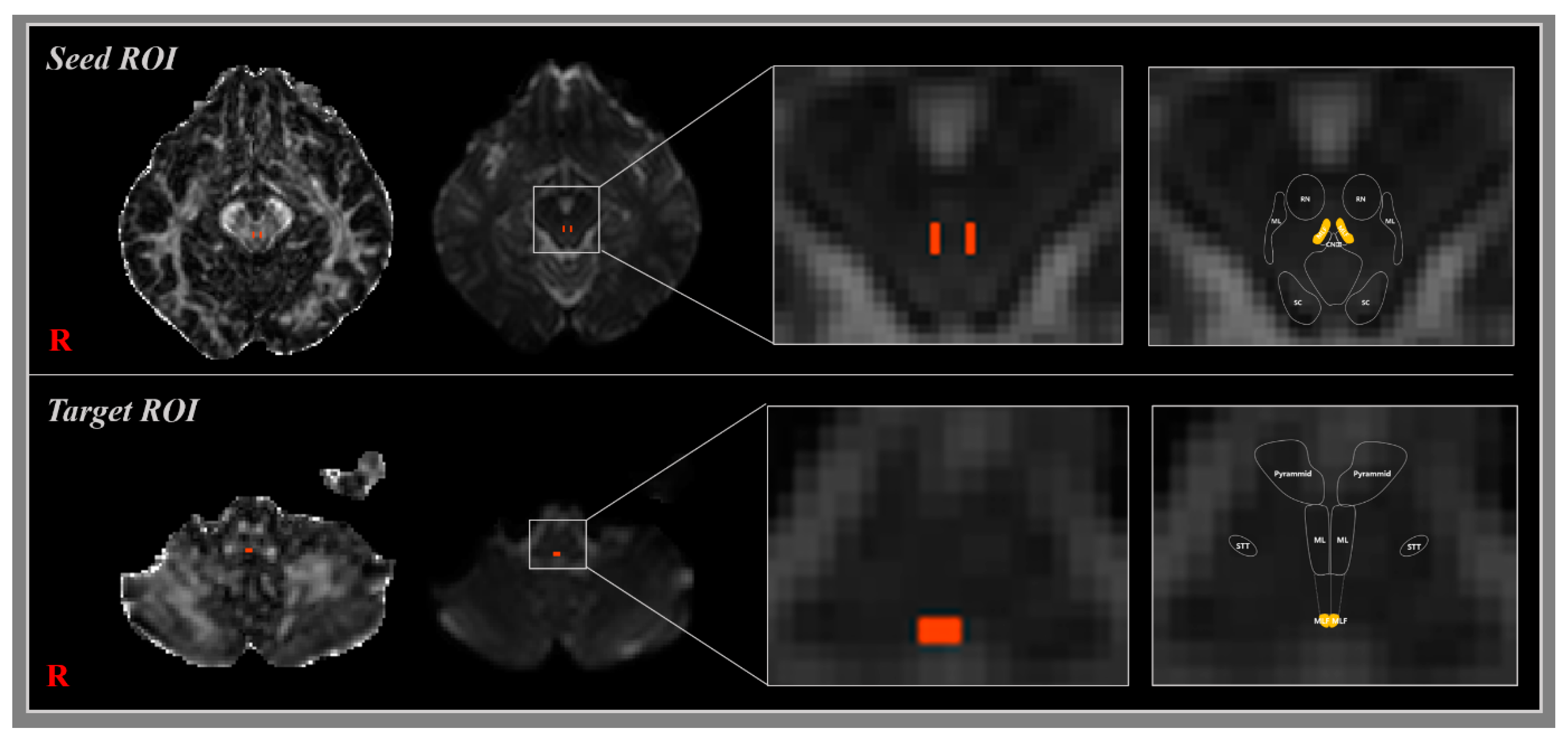
2.2. Diffusion Tensor Image Tractography
2.3. Fiber Tracking
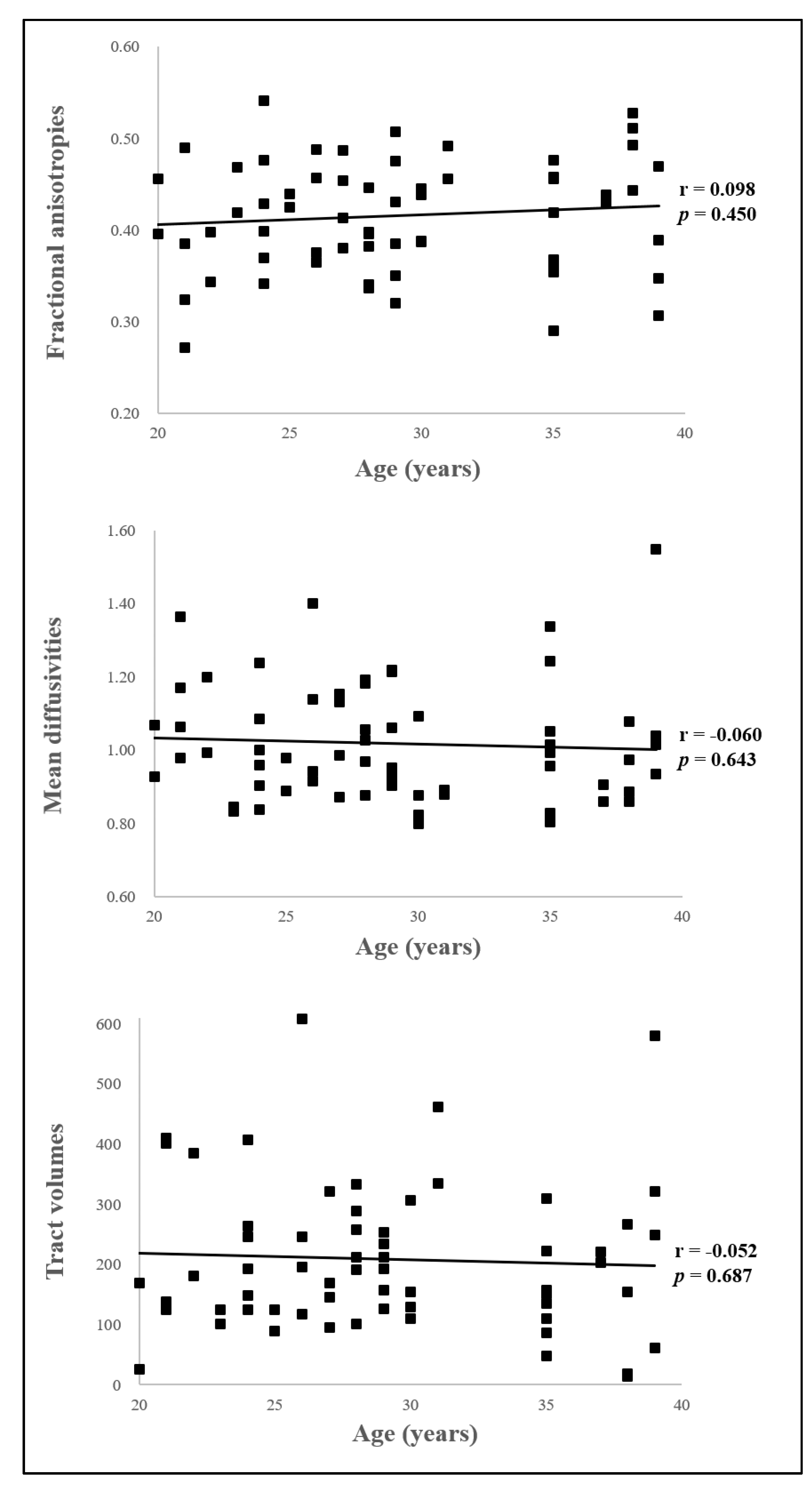
2.4. Statistical Analysis
3. Results
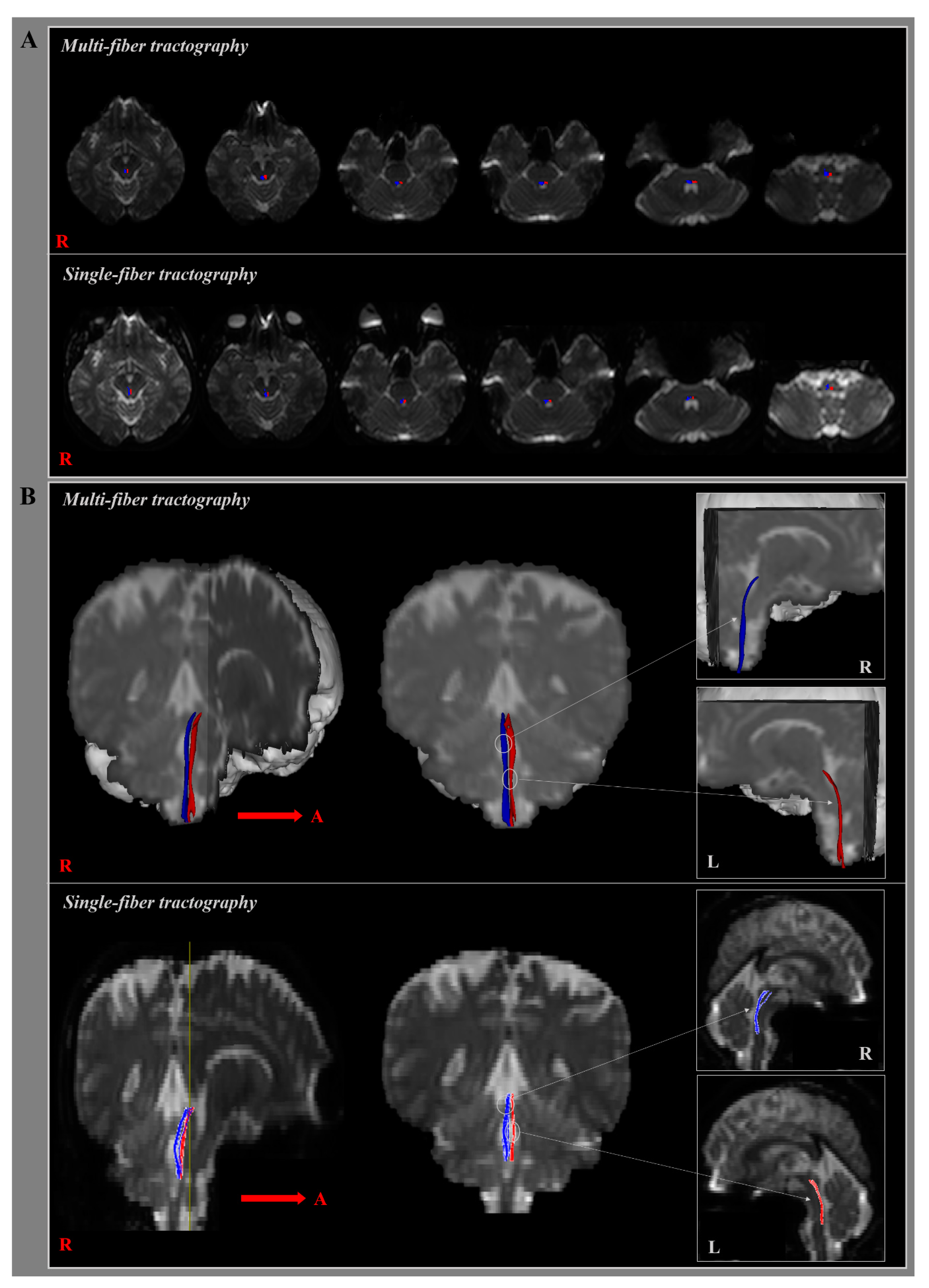
3.1. Multi-Fiber Tractography
3.2. Single-Fiber Tractography
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Sakai, K.; Yokota, H.; Akazawa, K.; Yamada, K. Brainstem White Matter Tracts and the Control of Eye Movements. Semin. UltrasoundCt Mri. 2014, 35, 517–526. [Google Scholar] [CrossRef]
- Sakaie, K.; Takahashi, M.; Remington, G.; Wang, X.; Conger, A.; Conger, D.; Dimitrov, I.; Jones, S.; Frohman, A.; Frohman, T.; et al. Correlating Function and Imaging Measures of the Medial Longitudinal Fasciculus. PLoS ONE 2016, 11, e0147863. [Google Scholar] [CrossRef] [PubMed]
- Sciacca, S.; Lynch, J.; Davagnanam, I.; Barker, R. Midbrain, Pons, and Medulla: Anatomy and Syndromes. Radiogr. A Rev. Publ. Radiol. Soc. North Am. Inc. 2019, 39, 1110–1125. [Google Scholar] [CrossRef] [PubMed]
- McNulty, J.P.; Lonergan, R.; Bannigan, J.; O’Laoide, R.; Rainford, L.A.; Tubridy, N. Visualisation of the medial longitudinal fasciculus using fibre tractography in multiple sclerosis patients with internuclear ophthalmoplegia. Ir. J. Med. Sci. 2016, 185, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Frohman, T.C.; Galetta, S.; Fox, R.; Solomon, D.; Straumann, D.; Filippi, M.; Zee, D.; Frohman, E.M. Pearls & Oy-sters: The medial longitudinal fasciculus in ocular motor physiology. Neurology 2008, 70, e57–e67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhidayasiri, R.; Plant, G.T.; Leigh, R.J. A hypothetical scheme for the brainstem control of vertical gaze. Neurology 2000, 54, 1985–1993. [Google Scholar] [CrossRef] [PubMed]
- Fenichel, G.M. Chapter 15—Disorders of Ocular Motility. In Clinical Pediatric Neurology, 6th ed.; Fenichel, G.M., Ed.; W.B. Saunders: Philadelphia, CA, USA, 2009; pp. 313–331. [Google Scholar] [CrossRef]
- Frohman, E.M.; Dewey, R.B.; Frohman, T.C. An unusual variant of the dorsal midbrain syndrome in MS: Clinical characteristics and pathophysiologic mechanisms. Mult. Scler 2004, 10, 322–325. [Google Scholar] [CrossRef]
- Ranalli, P.J.; Sharpe, J.A. Vertical vestibulo-ocular reflex, smooth pursuit and eye-head tracking dysfunction in internuclear ophthalmoplegia. Brain A J. Neurol. 1988, 111, 1299–1317. [Google Scholar] [CrossRef]
- Choi, S.Y.; Kim, H.J.; Kim, J.S. Impaired vestibular responses in internuclear ophthalmoplegia: Association and dissociation. Neurology 2017, 89, 2476–2480. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, J.H.; Kim, J.S. Ocular vestibular evoked myogenic potentials to head tap and cervical vestibular evoked myogenic potentials to air-conducted sounds in isolated internuclear ophthalmoplegia. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2014, 125, 1042–1047. [Google Scholar] [CrossRef]
- Sakaie, K.; Takahashi, M.; Dimitrov, I.; Togao, O.; Davis, S.; Remington, G.; Conger, A.; Conger, D.; Frohman, T.; Fox, R.; et al. Diffusion tensor imaging the medial longitudinal fasciculus in INO: Opportunities and challenges. Ann. N. Y. Acad. Sci. 2011, 1233, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Kochar, P.S.; Kumar, Y.; Sharma, P.; Kumar, V.; Gupta, N.; Goyal, P. Isolated medial longitudinal fasciculus syndrome: Review of imaging, anatomy, pathophysiology and differential diagnosis. Neuroradiol. J. 2018, 31, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Fox, R.J.; McColl, R.W.; Lee, J.C.; Frohman, T.; Sakaie, K.; Frohman, E. A preliminary validation study of diffusion tensor imaging as a measure of functional brain injury. Arch. Neurol. 2008, 65, 1179–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galons, J.P. Diffusion weighted and diffusion tensor imaging: A clinical guide. J. Magn. Reson. Imaging JMRI 2017. [Google Scholar] [CrossRef] [PubMed]
- Takeshige, H.; Ueno, Y.; Kamagata, K.; Sasaki, F.; Yamashiro, K.; Tanaka, R.; Aoki, S.; Hattori, N. Pathways Linked to Internuclear Ophthalmoplegia on Diffusion-Tensor Imaging in a Case with Midbrain Infarction. J. Stroke Cerebrovasc. Dis. 2016, 25, 2575–2579. [Google Scholar] [CrossRef] [PubMed]
- Salama, G.R.; Heier, L.A.; Patel, P.; Ramakrishna, R.; Magge, R.; Tsiouris, A.J. Diffusion Weighted/Tensor Imaging, Functional MRI and Perfusion Weighted Imaging in Glioblastoma-Foundations and Future. Front. Neurol. 2017, 8, 660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razek, A.; Taman, S.E.; El Regal, M.E.; Megahed, A.; Elzeny, S.; El Tantawi, N. Diffusion Tensor Imaging of Microstructural Changes in the Gray and White Matter in Patients With Crigler-Najjar Syndrome Type I. J. Comput Assist. Tomogr 2020, 25, 1008. [Google Scholar] [CrossRef]
- Jang, S.H.; Kwon, J.W.; Yeo, S.S. Three Dimensional Identification of Medial and Lateral Vestibulospinal Tract in the Human Brain: A Diffusion Tensor Imaging Study. Front. Hum. Neurosci. 2018, 12, 229. [Google Scholar] [CrossRef]
- Xie, G.; Zhang, F.; Leung, L.; Mooney, M.A.; Epprecht, L.; Norton, I.; Rathi, Y.; Kikinis, R.; Al-Mefty, O.; Makris, N.; et al. Anatomical assessment of trigeminal nerve tractography using diffusion MRI: A comparison of acquisition b-values and single- and multi-fiber tracking strategies. Neuroimage Clin. 2020, 25, 8. [Google Scholar] [CrossRef]
- Yeo, S.S.; Jang, S.; Kwon, J.W. Central vestibular disorder due to ischemic injury on the parieto-insular vestibular cortex in patients with middle cerebral artery territory infarction: Observational study. Medicine 2017, 96, e9349. [Google Scholar] [CrossRef]
- Smith, S.M.; Jenkinson, M.; Woolrich, M.W.; Beckmann, C.F.; Behrens, T.E.; Johansen-Berg, H.; Bannister, P.R.; De Luca, M.; Drobnjak, I.; Flitney, D.E.; et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 2004, 23, 051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, M.; Wang, S.M. Neuroanatomy, Interstitial Nucleus of Cajal. In StatPearls; Treasure Island (FL): Petersburg, FL, USA, 2020. [Google Scholar]
- Bogousslavsky, J.; Miklossy, J.; Regli, F.; Janzer, R. Vertical gaze palsy and selective unilateral infarction of the rostral interstitial nucleus of the medial longitudinal fasciculus (riMLF). J. Neurol. Neurosurg. Psychiatry 1990, 53, 67–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, T.H.; Oh, S.Y.; Kwak, K.; Lee, J.M.; Shin, B.S.; Jeong, S.K. Topology of brainstem lesions associated with subjective visual vertical tilt. Neurology 2014, 82, 1968–1975. [Google Scholar] [CrossRef] [PubMed]
- Baier, B.; Thomke, F.; Wilting, J.; Heinze, C.; Geber, C.; Dieterich, M. A pathway in the brainstem for roll-tilt of the subjective visual vertical: Evidence from a lesion-behavior mapping study. J. Neurosci. 2012, 32, 14854–14858. [Google Scholar] [CrossRef] [Green Version]
- Bae, Y.J.; Kim, J.H.; Choi, B.S.; Jung, C.; Kim, E. Brainstem pathways for horizontal eye movement: Pathologic correlation with MR imaging. Radiogr. A Rev. Publ. Radiol. Soc. North. Am. Inc. 2013, 33, 47–59. [Google Scholar] [CrossRef]
- Kakeda, S.; Korogi, Y.; Yoneda, T.; Nishimura, J.; Sato, T.; Hiai, Y.; Ohnari, N.; Okada, K.; Hayashi, H.; Matsusue, E.; et al. A novel tract imaging technique of the brainstem using phase difference enhanced imaging: Normal anatomy and initial experience in multiple system atrophy. Eur Radiol. 2011, 21, 2202–2210. [Google Scholar] [CrossRef]
- Pierrot-Deseilligny, C.; Tilikete, C. New insights into the upward vestibulo-oculomotor pathways in the human brainstem. Prog. Brain Res. 2008, 171, 509–518. [Google Scholar]
- Huma, Z.; Du Beau, A.; Brown, C.; Maxwell, D.J. Origin and neurochemical properties of bulbospinal neurons projecting to the rat lumbar spinal cord via the medial longitudinal fasciculus and caudal ventrolateral medulla. Front. Neural. Circuits 2014, 8, 40. [Google Scholar] [CrossRef] [Green Version]
- Zwergal, A.; Strupp, M.; Brandt, T.; Buttner-Ennever, J.A. Parallel ascending vestibular pathways: Anatomical localization and functional specialization. Ann. N. Y. Acad. Sci. 2009, 1164, 51–59. [Google Scholar] [CrossRef]
- Wang, C.; Paling, D.; Chen, L.; Hatton, S.N.; Lagopoulos, J.; Aw, S.T.; Kiernan, M.C.; Barnett, M.H. Axonal conduction in multiple sclerosis: A combined magnetic resonance imaging and electrophysiological study of the medial longitudinal fasciculus. Mult. Scler. 2015, 21, 905–915. [Google Scholar] [CrossRef]
- Wakai, S.; Watanabe, Y.; Ichiki, T.; Watanabe, T.; Numata, K.; Tachi, N.; Matsumoto, H.; Chiba, S. Childhood multiple sclerosis: MR images and clinical variations in four Japanese cases. Brain Dev. 1994, 16, 52–56. [Google Scholar] [CrossRef]
- Lee, S.H.; Nam, T.K.; Park, Y.S.; Kwon, J.T. A Case of Traumatic Unilateral Internuclear Ophthalmoplegia: Clinical Significance of Susceptibility-Weighted Imaging. Korean J. Neurotrauma 2016, 12, 140–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.T.; Lin, T.K.; Hsieh, T.C. Isolated Internuclear Ophthalmoplegia After Massive Supratentorial Epidural Hematoma: A Case Report and Review of the Literature. World Neurosurg. 2017, 100, e713. [Google Scholar] [CrossRef] [PubMed]
- Hai, S.; Elkbuli, A.; Kinslow, K.; McKenney, M.; Boneva, D. When “looks” can be deceiving – Internuclear ophthalmoplegia after mild traumatic brain injury: Case report and literature review. Int. J. Surg. Case Rep. 2019, 63, 19–22. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Normal Healthy Subjects (n = 31) | |
|---|---|
| Age (years) | 29.13 (5.74) |
| Gender (Male/Female) | 17/14 |
| Education (years) | 16.35 (1.05) |
| MMSE (score) | 29.94 (0.36) |
| Multi-Fiber Tractography | Single-Fiber Tractography | |
|---|---|---|
| FA | 0.42 (0.06) | 0.50 (0.05) |
| MD | 1.02 (0.16) | 0.80 (0.08) |
| Tract volume (voxel number) | 208.79 (123.81) | 68.37 (38.65) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeo, S.S.; Jang, S.H.; Kwon, J.W.; Cho, I.H. Three-Dimensional Identification of the Medial Longitudinal Fasciculus in the Human Brain: A Diffusion Tensor Imaging Study. J. Clin. Med. 2020, 9, 1340. https://doi.org/10.3390/jcm9051340
Yeo SS, Jang SH, Kwon JW, Cho IH. Three-Dimensional Identification of the Medial Longitudinal Fasciculus in the Human Brain: A Diffusion Tensor Imaging Study. Journal of Clinical Medicine. 2020; 9(5):1340. https://doi.org/10.3390/jcm9051340
Chicago/Turabian StyleYeo, Sang Seok, Sung Ho Jang, Jung Won Kwon, and In Hee Cho. 2020. "Three-Dimensional Identification of the Medial Longitudinal Fasciculus in the Human Brain: A Diffusion Tensor Imaging Study" Journal of Clinical Medicine 9, no. 5: 1340. https://doi.org/10.3390/jcm9051340
APA StyleYeo, S. S., Jang, S. H., Kwon, J. W., & Cho, I. H. (2020). Three-Dimensional Identification of the Medial Longitudinal Fasciculus in the Human Brain: A Diffusion Tensor Imaging Study. Journal of Clinical Medicine, 9(5), 1340. https://doi.org/10.3390/jcm9051340