Fatal Outcomes of COVID-19 in Patients with Severe Acute Kidney Injury

 , ,
, ,  , , ,
, , , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
2.2. Virologic Studies
2.3. Definition
2.4. Clinical Management
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Laboratory Findings on Admission among AKI Patients
3.3. Treatment and Complications among AKI Patients
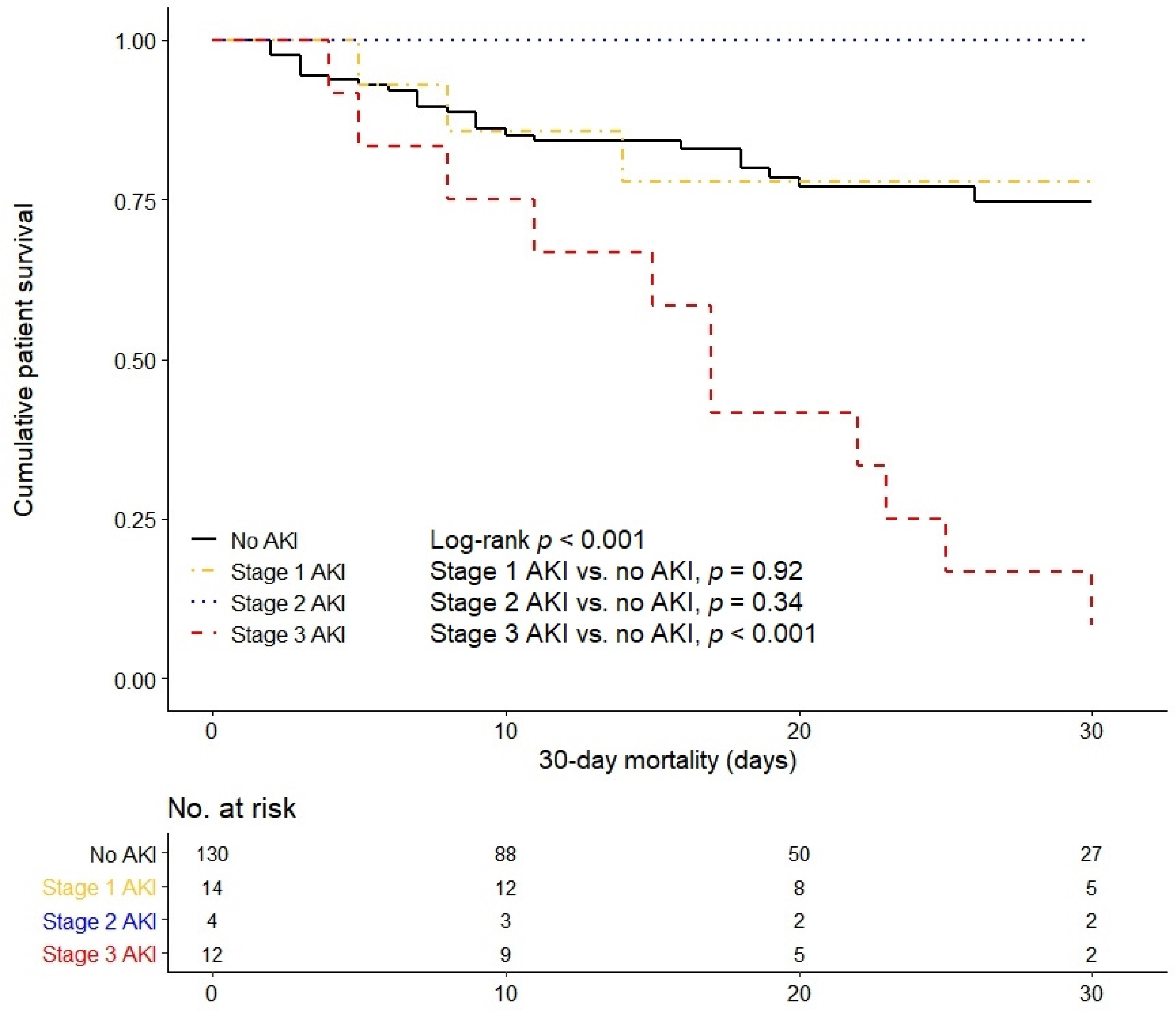
3.4. Severity of Acute Kidney Injury and In-Hospital Mortality
3.5. Predictors for Severe Acute Kidney Injury
3.6. Renal Replacement Therapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- World Health Organization. Novel Coronavirus (2019-nCoV) Situation Report—51. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf? (accessed on 26 April 2020).
- Boldog, P.; Tekeli, T.; Vizi, Z.; Dénes, A.; Bartha, F.A.; Röst, G. Risk Assessment of Novel Coronavirus COVID-19 Outbreaks Outside China. J. Clin. Med. 2020, 9, 571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naicker, S.; Yang, C.W.; Hwang, S.J.; Liu, B.C.; Chen, J.H.; Jha, V. The Novel Coronavirus 2019 epidemic and kidneys. Kidney Int. 2020. [Google Scholar] [CrossRef]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020. [Google Scholar] [CrossRef]
- Yin, Y.; Wunderink, R.G. MERS, SARS and other coronaviruses as causes of pneumonia. Respirology 2018, 23, 130–137. [Google Scholar] [CrossRef] [Green Version]
- Chu, K.H.; Tsang, W.K.; Tang, C.S.; Lam, M.F.; Lai, F.M.; To, K.F.; Fung, K.S.; Tang, H.L.; Yan, W.W.; Chan, H.W.; et al. Acute renal impairment in coronavirus-associated severe acute respiratory syndrome. Kidney Int. 2005, 67, 698–705. [Google Scholar] [CrossRef] [Green Version]
- Alkindi, F.; Boobes, Y.; Chandrasekhar Nair, S.; Hashmey, R. SAT-028 acute kidney injury associated with middle east respiratory syndrome coronavirus (MERS-CoV) infection. Kidney Int. Rep. 2020, 5, S13. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.-W.; Lee, K.S.; Kim, K.; Lee, J.J.; Kim, J.-Y. A Brief Telephone Severity Scoring System and Therapeutic Living Centers Solved Acute Hospital-Bed Shortage during the COVID-19 Outbreak in Daegu, Korea. J. Korean Med. Sci. 2020, 35. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Malhotra, R.; Kashani, K.B.; Macedo, E.; Kim, J.; Bouchard, J.; Wynn, S.; Li, G.; Ohno-Machado, L.; Mehta, R. A risk prediction score for acute kidney injury in the intensive care unit. Nephrol. Dial. Transplant. 2017, 32, 814–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, R.K.; Zappitelli, M.; Brunner, L.; Wang, Y.; Wong, H.R.; Chawla, L.S.; Wheeler, D.S.; Goldstein, S.L. Derivation and validation of the renal angina index to improve the prediction of acute kidney injury in critically ill children. Kidney Int. 2014, 85, 659–667. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Li, X.; Chen, H.; Yan, S.; Li, D.; Li, Y.; Gong, Z. Coronavirus Disease 19 Infection Does Not Result in Acute Kidney Injury: An Analysis of 116 Hospitalized Patients from Wuhan, China. Am. J. Nephrol. 2020. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Finlay, S.; Bray, B.; Lewington, A.J.; Hunter-Rowe, C.T.; Banerjee, A.; Atkinson, J.M.; Jones, M.C. Identification of risk factors associated with acute kidney injury in patients admitted to acute medical units. Clin. Med. 2013, 13, 233–238. [Google Scholar] [CrossRef]
- Bagshaw, S.M.; Sood, M.M.; Long, J.; Fowler, R.A.; Adhikari, N.K.J.; Canadian Critical Care Trials Group H1N1 Collaborative. Acute kidney injury among critically ill patients with pandemic H1N1 influenza A in Canada: Cohort study. BMC Nephrol. 2013, 14, 123. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, J.S.; Ng, J.H.; Ross, D.W.; Sharma, P.; Shah, H.H.; Barnett, R.L.; Hazzan, A.D.; Fishbane, S.; Jhaveri, K.D.; Abate, M.; et al. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020. [Google Scholar] [CrossRef] [PubMed]
- Silver, S.A.; Harel, Z.; McArthur, E.; Nash, D.M.; Acedillo, R.; Kitchlu, A.; Garg, A.X.; Chertow, G.M.; Bell, C.M.; Wald, R. Causes of Death after a Hospitalization with AKI. J. Am. Soc. Nephrol. 2018, 29, 1001–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagshaw, S.M.; Uchino, S.; Bellomo, R.; Morimatsu, H.; Morgera, S.; Schetz, M.; Tan, I.; Bouman, C.; Macedo, E.; Gibney, N.; et al. Septic acute kidney injury in critically ill patients: Clinical characteristics and outcomes. Clin. J. Am. Soc. Nephrol. 2007, 2, 431–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.E.; Muntner, P.; Chertow, G.M.; Warnock, D.G. Acute kidney injury and mortality in hospitalized patients. Am. J. Nephrol. 2012, 35, 349–355. [Google Scholar] [CrossRef] [Green Version]
- Colson, P.; Rolain, J.M.; Lagier, J.C.; Brouqui, P.; Raoult, D. Chloroquine and hydroxychloroquine as available weapons to fight COVID-19. Int. J. Antimicrob. Agents 2020, 105932. [Google Scholar] [CrossRef]
- Li, W.; Zhang, C.; Sui, J.; Kuhn, J.H.; Moore, M.J.; Luo, S.; Wong, S.K.; Huang, I.C.; Xu, K.; Vasilieva, N.; et al. Receptor and viral determinants of SARS-coronavirus adaptation to human ACE2. EMBO J. 2005, 24, 1634–1643. [Google Scholar] [CrossRef] [Green Version]
- Wrapp, D.; Wang, N.; Corbett, K.S.; Goldsmith, J.A.; Hsieh, C.-L.; Abiona, O.; Graham, B.S.; McLellan, J.S. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science 2020, 367, 1260–1263. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Wu, M.; Guo, J.; Yao, J.; Liao, X.; Song, S.; Han, M.; Li, J.; Duan, G.; Zhou, Y.; et al. Caution on Kidney Dysfunctions of 2019-nCoV Patients. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Farkash, E.A.; Wilson, A.M.; Jentzen, J.M. Ultrastructural Evidence for Direct Renal Infection with SARS-CoV-2. J. Am. Soc. Nephrol. 2020. [Google Scholar] [CrossRef]
- Su, H.; Yang, M.; Wan, C.; Yi, L.-X.; Tang, F.; Zhu, H.-Y.; Yi, F.; Yang, H.-C.; Fogo, A.B.; Nie, X.; et al. Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. 2020. [Google Scholar] [CrossRef]
- Peerapornratana, S.; Manrique-Caballero, C.L.; Gómez, H.; Kellum, J.A. Acute kidney injury from sepsis: Current concepts, epidemiology, pathophysiology, prevention and treatment. Kidney Int. 2019, 96, 1083–1099. [Google Scholar] [CrossRef] [PubMed]
- Han, S.J.; Lee, H.T. Mechanisms and therapeutic targets of ischemic acute kidney injury. Kidney Res. Clin. Pract. 2019, 38, 427–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gautret, P.; Lagier, J.C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Non-AKI (n = 130) | All AKI (n = 30) | AKI Stage 1 (n = 14) | AKI Stage 2 (n = 4) | AKI Stage 3 (n = 12) |
|---|---|---|---|---|---|
| Median age (range), y | 67.0 (24.0–92.0) | 75.0 (60.0–98.0) * | 75.0 (60.0–98.0) * | 73.0 (63.0–86.0) | 77.0 (61.0–87.0) |
| Sex, male, n (%) | 66 (50.8) | 20 (66.7) | 8 (57.1) | 3 (75.0) | 9 (75.0) |
| Body mass index, kg/m2 | 23.4 (21.0–26.3) | 24.5 (22.1–27.1) | 25.6 (22.8–29.4) | 24.0 (22.1–26.0) | 23.4 (20.0–27.1) |
| Comorbid conditions, n (%) | |||||
| Any comorbidity | 96 (73.8) | 28 (93.3) * | 14 (100.0) * | 3 (75.0) | 11 (91.7) |
| Hypertension | 59 (45.4) | 18 (60.0) | 11 (78.6) * | 2 (50.0) | 5 (41.7) |
| Diabetes | 36 (27.7) | 14 (46.7) * | 7 (50.0) | 1 (25.0) | 6 (50.0) |
| Cardiovascular disease | 16 (12.3) | 5 (16.7) | 2 (14.3) | 0 | 3 (25.0) |
| Congestive heart failure | 8 (6.2) | 2 (6.7) | 0 | 0 | 2 (16.7) |
| Chronic lung disease | 12 (9.2) | 4 (13.3) | 0 | 1 (25.0) | 3 (25.0) |
| Cognitive disorder | 26 (20.0) | 4 (13.3) | 3 (21.4) | 0 | 1 (8.3) |
| Malignancy | 19 (14.6) | 7 (23.3) | 2 (14.3) | 1 (25.0) | 4 (33.3) |
| Signs and symptoms, n (%) | |||||
| Fever | 93 (71.5) | 18 (60.0) | 9 (64.3) | 3 (75.0) | 6 (50.0) |
| Chill | 60 (46.2) | 16 (53.3) | 9 (64.3) | 1 (25.0) | 6 (50.0) |
| Myalgia | 40 (30.,8) | 9 (30.0) | 5 (35.7) | 0 | 4 (33.3) |
| Fatigue | 63 (48.5) | 20 (66.7) | 10 (71.4) | 2 (50.0) | 8 (66.7) |
| Cough | 45 (34.6) | 16 (53.3) | 7 (50.0) | 1 (25.0) | 8 (66.7) |
| Sputum | 35 (26.9) | 14 (46.7) * | 6 (42.9) | 1 (25.0) | 7 (58.3) * |
| Dyspnea | 58 (44.6) | 17 (56.7) | 8 (57.1) | 2 (50.0) | 7 (58.3) |
| Rhinorrhea | 10 (7.7) | 2 (6.7) | 0 | 1 (25.0) | 1 (8.3) |
| Nausea or vomiting | 10 (7.7) | 2 (6.7) | 0 | 1 (25.0) | 1 (8.3) |
| Diarrhea | 19 (14.6) | 3 (10.0) | 2 (14.3) | 1 (25.0) | 0 |
| Days from symptom onset to diagnosis | 5.0 (3.0–10.0) | 4.0 (3.0–7.5) | 3.5 (1.0–6.3) | 4.5 (1.0–6.5) | 5.5 (3.5–10.5) |
| Days from symptom onset to admission | 6.0 (3.0–10.0) | 6.5 (4.0–12.0) | 5.5 (3.0–10.0) | 7.5 (4.5–12.0) | 8.5 (5.0–15.0) |
| Days from symptom onset to diagnosis of AKI | 10.0 (5.8–19.0) | 8.0 (4.0–13.0) a | 8.5 (5.0–27.8) a,b | 17.5 (9.8–25.0) b | |
| Length of hospital stay, days | 16.0 (9.0–25.0) | 20.0 (12.0–31.0) | 23.5 (14.0–36.0) | 34.0 (10.5–57.5) | 17.0 (8.8–24.5) |
| In-hospital death | 27 (20.8) | 17 (56.7) * | 4 (28.6) a | 1 (25.0) b | 12 (100.0) *,c |
| Vital signs | |||||
| Systolic BP, mmHg | 133.5 (116.5–148.0) | 134.0 (109.8–155.5) | 115.0 (106.0–145.5) | 134.5 (128.0–155.3) | 150.0 (115.5–169.3) |
| Diastolic BP, mmHg | 78.0 (68.0–86.5) | 71.0 (60.0–91.3) | 66.5 (59.3–84.5) | 79.5 (70.5–90.0) | 73.5 (59.0–98.0) |
| Heart rate, beats/min | 88.0 (79.0–102.0) | 86.0 (79.0–108.0) | 79.5 (76.5–95.3) | 86.5 (83.5–103.0) | 91.5 (80.0–109.5) |
| Body temperature, °C | 36.9 (36.4–37.5) | 37.3 (36.8–37.9) | 37.2 (36.7–38.0) | 37.4 (37.0–37.7) | 37.2 (36.5–38.0) |
| Chest radiography findings, n (%) | |||||
| Patchy consolidation | 73 (56.2) | 16 (53.3) | 9 (64.3) | 1 (25.0) | 6 (50.0) |
| Ground glass opacity | 64 (49.2) | 15 (50.0) | 6 (42.9) | 2 (50.0) | 7 (58.3) |
| No active lung lesion | 24 (18.5) | 4 (13.3) | 2 (14.3) | 1 (25.0) | 1 (8.3) |
| Laboratory Findings | All AKI (n = 30) | AKI Stage 1 (n = 14) | AKI Stage 2 (n = 4) | AKI Stage 3 (n = 12) |
|---|---|---|---|---|
| White blood cell count, ×109/L | 7.1 (5.8–11.9) | 7.1 (5.5–10.1) | 6.0 (4.4–8.2) | 9.9 (6.7–14.4) |
| Absolute neutrophil count, ×109/L | 6.3 (4.0–10.8) | 5.9 (3.9–8.8) | 4.9 (3.6–7.1) | 9.5 (5.6–14.2) |
| Lymphocyte count, ×109/L | 0.7 (0.5–0.9) | 0.9 (0.7–1.1) | 0.6 (0.5–0.7) | 0.6 (0.5–0.9) |
| Monocyte count, ×109/L | 0.3 (0.2–0.4) | 0.3 (0.3–0.4) | 0.2 (0.2–0.3) | 0.3 (0.1–0.6) |
| Hemoglobin, g/dL | 12.3 (10.9–13.9) | 12.3 (10.9–13.2) | 13.3 (10.8–14.7) | 12.2 (10.6–13.8) |
| Platelet count, ×109/L | 241.0 (179.5–296.8) | 255.5 (208.0–296.0) | 204.5 (170.0–351.8) | 214.0 (140.5–302.8) |
| hs-CRP, mg/dL | 10.3 (6.1–20.9) | 6.8 (4.9–16.3) | 14.4 (5.8–24.4) | 17.4 (8.6–26.0) |
| Procalcitonin, ng/mL (n = 16) | 0.18 (0.09–0.70) | 0.03 (0.02–0.19) | 0.10 (0.09–0.16) | 0.22 (0.15–0.91) |
| Ferritin, ng/mL (n = 19) | 531.0 (255.0–868.0) | 483.7 (193.3–657.6) | 868.0 (484.0–920.0) | 520.8 (309.0–7450.0) |
| AST, U/L | 48.0 (36.0–63.3) | 47.0 (34.5–69.3) | 48.5 (38.8–50.8) | 50.0 (33.0–70.5) |
| ALT, U/L | 26.0 (17.8–34.5) | 27.5 (16.3–38.3) | 19.5 (19.0–24.5) | 27.5 (20.3–35.5) |
| Total bilirubin, mg/dL | 0.6 (0.4–0.9) | 0.5 (0.4–0.8) | 1.1 (0.6–1.4) | 0.7 (0.5–0.9) |
| Total protein, g/dL | 6.7 (6.4–7.1) | 6.9 (6.6 –7.4) | 6.6 (6.4–6.9) | 6.5 (6.1–7.0) |
| Albumin, g/dL | 3.3 (3.0–3.5) | 3.5 (3.2–3.7) a | 3.5 (3.2–3.8) a,b | 3.2 (2.7–3.3) b |
| BUN, mg/dL | 23.7 (15.7–32.0) | 23.7 (18.7–39.3) | 23.3 (12.1–25.1) | 23.8 (14.6–41.5) |
| Creatinine, mg/dL | 1.1 (0.8–1.6) | 1.1 (1.0–1.4) | 1.1 (0.7–1.6) | 1.1 (0.7–1.9) |
| eGFR, mL/min/1.73 m2 | 60.0 (41.5–82.0) | 53.5 (41.5–69.8) | 67.0 (33.8–97.3) | 61.5 (38.0–86.5) |
| LDH, U/L (n = 25) | 481.0 (286.0–593.0) | 481.0 (249.0–589.5) | 475.5 (277.0–475.5) | 492.5 (306.0–592.5) |
| CPK, U/L (n = 17) | 135.0 (72.5–533.5) | 102.0 (63.5–436.8) | 220.0 (68.0–220.0) | 494.0 (177.0–837.5) |
| D-dimer, µg/mL (n = 16) | 2.1 (0.8–3.2) | 2.1 (1.0–2.6) | 1.2 (0.2–1.2) | 2.0 (0.8–6.9) |
| Sodium, mEq/L | 135.5 (133.0–139.3) | 137.0 (132.8–142.0) | 135.0 (132.5–137.5) | 133.5 (133.0–138.5) |
| Potassium, mEq/L | 4.0 (3.3–4.7) | 3.8 (3.5–4.9) a | 3.2 (3.1–3.3) b | 4.4 (3.6–5.2) a,b |
| Lactate, mEq/L | 1.9 (1.4–2.5) | 1.9 (1.5–2.5) | 1.1 (1.1–1.9) | 2.0 (1.4–3.2) |
| Prothrombin time, s | 12.4 (11.9–13.0) | 12.2 (11.7–12.6) | 12.6 (12.2–13.0) | 12.1 (11.8–15.1) |
| Activated partial thromboplastin time, s | 31.4 (28.7–33.5) | 31.2 (26.1–34.4) | 30.0 (28.6–31.2) | 32.2 (30.9–34.3) |
| Variables | All AKI (n = 30) | AKI Stage 1 (n = 14) | AKI Stage 2 (n = 4) | AKI Stage 3 (n = 12) |
|---|---|---|---|---|
| Treatments, n (%) | ||||
| Lopinavir/ritonavir or darunavir/cobicistat | 29 (96.7) | 14 (100.0) | 4 (100.0) | 11 (91.7) |
| Hydroxychloroquine | 25 (83.3) | 12 (85.7) | 4 (100.0) | 9 (75.0) |
| Antibiotics | 29 (96.7) | 13 (92.9) | 4 (100.0) | 12 (100.0) |
| Glucocorticoid | 18 (60.0) | 6 (42.9) | 2 (50.0) | 10 (83.3) |
| Intravenous immunoglobulin | 5 (16.7) | 1 (7.1) | 0 | 4 (33.3) |
| Inotropic agents | 17 (56.7) | 5 (35.7) a | 2 (50.0) a,b | 10 (83.3) b |
| Oxygen therapy | 29 (96.7) | 13 (92.9) | 4 (100.0) | 12 (100.0) |
| Low-flow oxygen | 5 (16.7) | 3 (21.4) | 2 (50.0) | 0 |
| High-flow oxygen | 8 (26.7) | 5 (35.7) | 0 | 3 (25.0) |
| Invasive mechanical ventilation | 16 (53.3) | 5 (35.7) | 2 (50.0) | 9 (75.0) |
| Continuous renal replacement therapy | 5 (16.7) | 0 a | 0 a,b | 5 (41.7) b |
| Extracorporeal membrane oxygenation | 1 (3.3) | 0 | 0 | 1 (8.3) |
| ICU admission | 20 (66.7) | 8 (57.1) | 2 (50.0) | 10 (83.3) |
| Duration of medication used, days (IQR) | ||||
| Lopinavir/ritonavir or darunavir/cobicistat | 8.0 (5.0–10.0) | 7.5 (5.0–10.0) | 10.5 (8.0–12.0) | 8.0 (4.0–9.5) |
| Hydroxychloroquine | 5.0 (2.0–10.0) | 5.0 (2.0–10.0) | 6.5 (3.0–9.5) | 4.0 (1.5–9.5) |
| Complications, n (%) | ||||
| ARDS | 17 (56.7) | 5 (35.7) a | 2 (50.0) a,b | 10 (83.3) b |
| Septic shock | 14 (46.7) | 4 (28.6) | 1 (25.0) | 9 (75.0) |
| Arrhythmia | 2 (6.7) | 1 (7.1) | 0 | 1 (8.3) |
| DIC | 2 (6.7) | 0 | 0 | 2 (16.7) |
| Variables | Univariate | Model 1 † | Model 2 ‡ | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| AKIN | ||||||
| No AKI | Reference | Reference | Reference | |||
| Stage 1 | 0.98 (0.34–2.81) | 0.97 | 0.68 (0.23–1.98) | 0.48 | 0.59 (0.20–1.75) | 0.34 |
| Stage 2 | 0.63 (0.08–4.76) | 0.65 | 0.45 (0.06–3.42) | 0.45 | 0.42 (0.06–3.26) | 0.41 |
| Stage 3 | 5.28 (2.65–10.55) | <0.001 | 3.77 (1.84–7.71) | <0.001 | 3.62 (1.75–7.48) | 0.001 |
| Age | 1.04 (1.01–1.06) | 0.003 | 1.04 (1.01–1.07) | 0.003 | 1.04 (1.01–1.07) | 0.003 |
| Sex (ref: F) | 1.52 (0.82–2.80) | 0.19 | 0.63 (0.33–1.20) | 0.16 | 0.61 (0.32–1.16) | 0.13 |
| Hypertension | 1.44 (0.79–2.63) | 0.24 | 1.34 (0.71–2.52) | 0.36 | ||
| Diabetes | 1.55 (0.85–2.83) | 0.15 | 1.35 (0.72–2.56) | 0.35 | ||
| Variables | Univariate | Model 1 † | Model 2 ‡ | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| AKIN | ||||||
| Stage 1 | Reference | Reference | Reference | |||
| Stage 2 | 0.46 (0.05–4.42) | 0.50 | 0.46 (0.05–4.41) | 0.50 | 0.07 (0.004–1.30) | 0.08 |
| Stage 3 | 7.58 (2.04–28.24) | 0.003 | 7.66 (2.03–28.86) | 0.003 | 15.65 (2.43–100.64) | 0.004 |
| Age | 0.99 (0.94–1.05) | 0.75 | 1.01 (0.94–1.07) | 0.97 | 1.01 (0.93–1.10) | 0.77 |
| Sex (ref: F) | 1.22 (0.44–3.37) | 0.70 | 1.04 (0.33–3.26) | 0.98 | 0.60 (0.17–2.09) | 0.42 |
| Days from symptom onset to AKI diagnosis | 1.03 (0.98–1.07) | 0.28 | ||||
| Hypertension | 0.94 (0.36–2.49) | 0.94 | ||||
| Diabetes | 1.21 (0.45–3.22) | 0.71 | ||||
| ARDS | 5.56 (1.57–19.75) | 0.01 | 12.24 (1.87–79.92) | 0.01 | ||
| Septic shock | 1.94 (0.72–5.21) | 0.19 | 11.42 (1.59–82.25) | 0.02 | ||
| Variables | Univariate | Multivariate † | ||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Age | 0.98 (0.90–1.07) | 0.65 | 1.01 (0.87–1.16) | 0.91 |
| Sex (ref: F) | 1.91 (0.38–9.59) | 0.43 | 1.17 (0.15–9.09) | 0.88 |
| Days from symptom onset to AKI diagnosis | 1.11 (1.00–1.23) | 0.04 | ||
| Hypertension | 0.28 (0.06–1.29) | 0.10 | ||
| Diabetes | 1.25 (0.29–5.41) | 0.77 | ||
| ARDS | 7.86 (1.31–47.04) | 0.02 | 9.05 (1.05–78.14) | 0.04 |
| Septic shock | 7.80 (1.48–41.21) | 0.02 | ||
| Serum albumin on admission | 0.05 (0.004–0.69) | 0.03 | 0.02 (0.001–0.87) | 0.04 |
| Patient No. | Age | Sex | SAPS | SOFA | APACHEII | Indication | Screat on CRRT Initiation (mg/dL) | Admission to CRRT Initiation (days) | Anticoagulation | Duration (hrs) | Effluent Flow Rate (mL/kg/h) | Outcome | Change to HD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 67 | M | 72 | 12 | 28 | Hyperkalemia | 1.29 | 6 | Heparin | 155 | 11 | Death | No |
| 2 | 75 | F | 83 | 19 | 34 | Hypervolemia | 5.03 | 9 | Heparin | 560 | 33 | Death | No |
| 3 | 60 | M | 79 | 15 | 30 | Hypervolemia and acidosis | 3.47 | 6 | Heparin | 237 | 28 | Death | No |
| 4 | 67 | F | 57 | 10 | 19 | Hypervolemia | 2.82 | 2 | Nafamostat | 26 | 29 | Death | No |
| 5 | 78 | M | 58 | 10 | 23 | Hyperkalemia | 2.90 | 7 | Nafamostat | 21 | 25 | Death | No |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, J.-H.; Park, S.-H.; Jeon, Y.; Cho, J.-H.; Jung, H.-Y.; Choi, J.-Y.; Kim, C.-D.; Lee, Y.-H.; Seo, H.; Lee, J.; et al. Fatal Outcomes of COVID-19 in Patients with Severe Acute Kidney Injury. J. Clin. Med. 2020, 9, 1718. https://doi.org/10.3390/jcm9061718
Lim J-H, Park S-H, Jeon Y, Cho J-H, Jung H-Y, Choi J-Y, Kim C-D, Lee Y-H, Seo H, Lee J, et al. Fatal Outcomes of COVID-19 in Patients with Severe Acute Kidney Injury. Journal of Clinical Medicine. 2020; 9(6):1718. https://doi.org/10.3390/jcm9061718
Chicago/Turabian StyleLim, Jeong-Hoon, Sun-Hee Park, Yena Jeon, Jang-Hee Cho, Hee-Yeon Jung, Ji-Young Choi, Chan-Duck Kim, Yong-Hoon Lee, Hyewon Seo, Jaehee Lee, and et al. 2020. "Fatal Outcomes of COVID-19 in Patients with Severe Acute Kidney Injury" Journal of Clinical Medicine 9, no. 6: 1718. https://doi.org/10.3390/jcm9061718
APA StyleLim, J. -H., Park, S. -H., Jeon, Y., Cho, J. -H., Jung, H. -Y., Choi, J. -Y., Kim, C. -D., Lee, Y. -H., Seo, H., Lee, J., Kwon, K. T., Kim, S. -W., Chang, H. -H., & Kim, Y. -L. (2020). Fatal Outcomes of COVID-19 in Patients with Severe Acute Kidney Injury. Journal of Clinical Medicine, 9(6), 1718. https://doi.org/10.3390/jcm9061718