
Healing Patterns of Non-Collagenated Bovine and Collagenated Porcine Xenografts Used for Sinus Floor Elevation: A Histological Study in Rabbits

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Power Calculation and Sample Size
2.3. Experimental Design
2.4. Xenografts
2.5. Surgical Procedures
2.6. Maintenance Care
2.7. Euthanasia
2.8. Histological Preparation
2.9. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buser, D.; Dula, K.; Hess, D.; Hirt, H.P.; Belser, U.C. Localized ridge augmentation with autografts and barrier membranes. Periodontology 2000 1999, 19, 151–163. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Tan, W.C.; Zwahlen, M.; Lang, N.P. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. J. Clin. Periodontol. 2008, 35 (Suppl. S8), 216–240. [Google Scholar] [CrossRef]
- Lundgren, S.; Cricchio, G.; Hallman, M.; Jungner, M.; Rasmusson, L.; Sennerby, L. Sinus floor elevation procedures to enable implant placement and integration: Techniques, biological aspects and clinical outcomes. Periodontology 2000 2017, 73, 103–120. [Google Scholar] [CrossRef]
- Kawakami, S.; Botticelli, D.; Nakajima, Y.; Sakuma, S.; Baba, S. Anatomical analyses for maxillary sinus floor augmentation with a lateral approach: A cone beam computed tomography study. Ann. Anat. 2019, 226, 29–34. [Google Scholar] [CrossRef]
- Testori, T.; Weinstein, T.; Taschieri, S.; Wallace, S.S. Risk factors in lateral window sinus elevation surgery. Periodontology 2000 2019, 81, 91–123. [Google Scholar] [CrossRef]
- Asai, S.; Shimizu, Y.; Ooya, K. Maxillary sinus augmentation model in rabbits: Effect of occluded nasal ostium on new bone formation. Clin. Oral Implant. Res. 2002, 13, 405–409. [Google Scholar] [CrossRef]
- Xu, H.; Shimizu, Y.; Asai, S.; Ooya, K. Grafting of deproteinized bone particles inhibits bone resorption after maxillary sinus floor elevation. Clin. Oral Implant. Res. 2004, 15, 126–133. [Google Scholar] [CrossRef]
- Scala, A.; Botticelli, D.; Faeda, R.S.; Garcia Rangel, I., Jr.; Américo de Oliveira, J.; Lang, N.P. Lack of influence of the Schneiderian membrane in forming new bone apical to implants simultaneously installed with sinus floor elevation: An experimental study in monkeys. Clin. Oral Implant. Res. 2012, 23, 175–181. [Google Scholar] [CrossRef]
- Shanbhag, S.; Shanbhag, V.; Stavropoulos, A. Volume changes of maxillary sinus augmentations over time: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 881–892. [Google Scholar] [CrossRef] [Green Version]
- Canellas, J.V.D.S.; Drugos, L.; Ritto, F.G.; Fischer, R.G.; Medeiros, P.J.D. Xenograft materials in maxillary sinus floor elevation surgery: A systematic review with network meta-analyses. Br. J. Oral Maxillofac. Surg. 2021, 59, 742–751. [Google Scholar] [CrossRef]
- Trimmel, B.; Gede, N.; Hegyi, P.; Szakács, Z.; Mezey, G.A.; Varga, E.; Kivovics, M.; Hanák, L.; Rumbus, Z.; Szabó, G. Relative performance of various biomaterials used for maxillary sinus augmentation: A Bayesian network meta-analysis. Clin. Oral Implant. Res. 2021, 32, 135–153. [Google Scholar] [CrossRef] [PubMed]
- Corbella, S.; Taschieri, S.; Weinstein, R.; Del Fabbro, M. Histomorphometric outcomes after lateral sinus floor elevation procedure: A systematic review of the literature and meta-analysis. Clin. Oral Implant. Res. 2016, 27, 1106–1122. [Google Scholar] [CrossRef] [PubMed]
- Lie, S.A.N.; Claessen, R.M.M.A.; Leung, C.A.W.; Merten, H.A.; Kessler, P.A.W.H. Non-grafted versus grafted sinus lift procedures for implantation in the atrophic maxilla: A systematic review and meta-analysis of randomized controlled trials. Int. J. Oral Maxillofac. Surg. 2022, 51, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Ellegaard, B.; Kølsen-Petersen, J.; Baelum, V. Implant therapy involving maxillary sinus lift in periodontally compromised patients. Clin. Oral Implant. Res. 1997, 8, 305–315. [Google Scholar] [CrossRef]
- Lundgren, S.; Andersson, S.; Gualini, F.; Sennerby, L. Bone reformation with sinus membrane elevation: A new surgical technique for maxillary sinus floor augmentation. Clin. Implant Dent. Relat. Res. 2004, 6, 165–173. [Google Scholar] [CrossRef]
- Cricchio, G.; Sennerby, L.; Lundgren, S. Sinus bone formation and implant survival after sinus membrane elevation and implant placement: A 1- to 6-year follow-up study. Clin. Oral Implant. Res. 2011, 22, 1200–1212. [Google Scholar] [CrossRef]
- Scala, A.; Botticelli, D.; Rangel, I.G., Jr.; de Oliveira, J.A.; Okamoto, R.; Lang, N.P. Early healing after elevation of the maxillary sinus floor applying a lateral access: A histological study in monkeys. Clin. Oral Implant. Res. 2010, 21, 1320–1326. [Google Scholar] [CrossRef]
- Jungner, M.; Cricchio, G.; Salata, L.A.; Sennerby, L.; Lundqvist, C.; Hultcrantz, M.; Lundgren, S. On the Early Mechanisms of Bone Formation after Maxillary Sinus Membrane Elevation: An Experimental Histological and Immunohistochemical Study. Clin. Implant Dent. Relat. Res. 2015, 17, 1092–1102. [Google Scholar] [CrossRef]
- Ellegaard, B.; Baelum, V.; Kølsen-Petersen, J. Non-grafted sinus implants in periodontally compromised patients: a time-to-event analysis. Clin. Oral Implants Res. 2006, 17, 156–164. [Google Scholar] [CrossRef]
- Starch-Jensen, T.; Schou, S. Maxillary Sinus Membrane Elevation with Simultaneous Installation of Implants without the Use of a Graft Material: A Systematic Review. Implant Dent. 2017, 26, 621–633. [Google Scholar] [CrossRef]
- Moraschini, V.; Uzeda, M.G.; Sartoretto, S.C.; Calasans-Maia, M.D. Maxillary sinus floor elevation with simultaneous implant placement without grafting materials: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 636–647. [Google Scholar] [CrossRef] [PubMed]
- Cricchio, G.; Palma, V.C.; Faria, P.E.; de Oliveira, J.A.; Lundgren, S.; Sennerby, L.; Salata, L.A. Histological findings following the use of a space-making device for bone reformation and implant integration in the maxillary sinus of primates. Clin. Implant Dent. Relat. Res. 2009, 11 (Suppl. S1), e14–e22. [Google Scholar] [CrossRef] [PubMed]
- Cricchio, G.; Palma, V.C.; Faria, P.E.; de Olivera, J.A.; Lundgren, S.; Sennerby, L.; Salata, L.A. Histological outcomes on the development of new space-making devices for maxillary sinus floor augmentation. Clin. Implant Dent. Relat. Res. 2011, 13, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Johansson, L.Å.; Isaksson, S.; Adolfsson, E.; Lindh, C.; Sennerby, L. Bone regeneration using a hollow hydroxyapatite space-maintaining device for maxillary sinus floor augmentation—A clinical pilot study. Clin. Implant Dent. Relat. Res. 2012, 14, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Schweikert, M.; Botticelli, D.; de Oliveira, J.A.; Scala, A.; Salata, L.A.; Lang, N.P. Use of a titanium device in lateral sinus floor elevation: An experimental study in monkeys. Clin. Oral Implant. Res. 2012, 23, 100–105. [Google Scholar] [CrossRef]
- Caneva, M.; Lang, N.P.; Garcia Rangel, I.J.; Ferreira, S.; Caneva, M.; De Santis, E.; Botticelli, D. Sinus mucosa elevation using Bio-Oss(®) or Gingistat(®) collagen sponge: An experimental study in rabbits. Clin. Oral Implant. Res. 2017, 28, e21–e30. [Google Scholar] [CrossRef]
- De Santis, E.; Lang, N.P.; Ferreira, S.; Rangel Garcia, I., Jr.; Caneva, M.; Botticelli, D. Healing at implants installed concurrently to maxillary sinus floor elevation with Bio-Oss(®) or autologous bone grafts. A histo-morphometric study in rabbits. Clin. Oral Implant. Res. 2017, 28, 503–511. [Google Scholar] [CrossRef]
- Iida, T.; Carneiro Martins Neto, E.; Botticelli, D.; Apaza Alccayhuaman, K.A.; Lang, N.P.; Xavier, S.P. Influence of a collagen membrane positioned subjacent the sinus mucosa following the elevation of the maxillary sinus. A histomorphometric study in rabbits. Clin. Oral Implant. Res. 2017, 28, 1567–1576. [Google Scholar] [CrossRef]
- Iida, T.; Silva, E.R.; Lang, N.P.; Apaza Alccayhuaman, K.A.; Botticelli, D.; Xavier, S.P. Histological and micro-computed tomography evaluations of newly formed bone after maxillary sinus augmentation using a xenograft with similar density and mineral content of bone: An experimental study in rabbits. Clin. Exp. Dent. Res. 2018, 4, 284–290. [Google Scholar] [CrossRef] [Green Version]
- Iida, T.; Baba, S.; Botticelli, D.; Masuda, K.; Xavier, S.P. Comparison of histomorphometry and microCT after sinus augmentation using xenografts of different particle sizes in rabbits. Oral. Maxillofac. Surg. 2020, 24, 57–64. [Google Scholar] [CrossRef]
- Masuda, K.; Silva, E.R.; Botticelli, D.; Apaza Alccayhuaman, K.A.; Xavier, S.P. Antrostomy Preparation for Maxillary Sinus Floor Augmentation Using Drills or a Sonic Instrument: A Microcomputed Tomography and Histomorphometric Study in Rabbits. Int. J. Oral Maxillofac. Implant. 2019, 34, 819–827. [Google Scholar] [CrossRef]
- Figueiredo, M.; Henriques, J.; Martins, G.; Guerra, F.; Judas, F.; Figueiredo, H. Physicochemical characterization of biomaterials commonly used in dentistry as bone substitutes—Comparison with human bone. J. Biomed. Mater. Res. B Appl. Biomater. 2010, 92, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, S.; Lang, N.P.; Ferri, M.; Apaza Alccayhuaman, K.A.; Botticelli, D. Influence of the height of the antrostomy in sinus floor elevation assessed by cone beam computed tomography—A randomized clinical trial. Int. J. Oral Maxillofac. Implant. 2019, 34, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, S.; Lang, N.P.; Iida, T.; Ferri, M.; Apaza Alccayhuaman, K.A.; Botticelli, D. Influence of the position of the antrostomy in sinus floor elevation assessed with cone-beam computed tomography: A randomized clinical trial. J. Investig. Clin. Dent. 2018, 9, e12362. [Google Scholar] [CrossRef] [PubMed]
- Sapata, V.M.; Llanos, A.H.; Cesar Neto, J.B.; Jung, R.E.; Thoma, D.S.; Hämmerle, C.H.F.; Pannuti, C.M.; Romito, G.A. Deproteinized bovine bone mineral is non-inferior to deproteinized bovine bone mineral with 10% collagen in maintaining the soft tissue contour post-extraction: A randomized trial. Clin. Oral Implant. Res. 2020, 31, 294–301. [Google Scholar] [CrossRef]
- Scala, A.; Lang, N.P.; Velez, J.U.; Favero, R.; Bengazi, F.; Botticelli, D. Effects of a collagen membrane positioned between augmentation material and the sinus mucosa in the elevation of the maxillary sinus floor. An experimental study in sheep. Clin. Oral Implant. Res. 2016, 27, 1454–1461. [Google Scholar] [CrossRef]
- Favero, V.; Lang, N.P.; Canullo, L.; Urbizo Velez, J.; Bengazi, F.; Botticelli, D. Sinus floor elevation outcomes following perforation of the Schneiderian membrane. An experimental study in sheep. Clin. Oral Implant. Res. 2016, 27, 233–240. [Google Scholar] [CrossRef]
- Omori, Y.; Ricardo Silva, E.; Botticelli, D.; Apaza Alccayhuaman, K.A.; Lang, N.P.; Xavier, S.P. Reposition of the bone plate over the antrostomy in maxillary sinus augmentation: A histomorphometric study in rabbits. Clin. Oral Implant. Res. 2018, 29, 821–834. [Google Scholar] [CrossRef]
- Godoy, E.P.; Alccayhuaman, K.A.A.; Botticelli, D.; Amaroli, A.; Balan, V.F.; Silva, E.R.; Xavier, S.P. Osteoconductivity of Bovine Xenograft Granules of Different Sizes in Sinus Lift: A Histomorphometric Study in Rabbits. Dent. J. 2021, 9, 61. [Google Scholar] [CrossRef]
- Busenlechner, D.; Huber, C.D.; Vasak, C.; Dobsak, A.; Gruber, R.; Watzek, G. Sinus augmentation analysis revised: The gradient of graft consolidation. Clin. Oral Implant. Res. 2009, 20, 1078–1083. [Google Scholar] [CrossRef] [PubMed]
- Stacchi, C.; Rapani, A.; Lombardi, T.; Bernardello, F.; Nicolin, V.; Berton, F. Does new bone formation vary in different sites within the same maxillary sinus after lateral augmentation? A prospective histomorphometric study. Clin. Oral Implant. Res. 2022, 33, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Gruber, R.; Kandler, B.; Fuerst, G.; Fisher, M.B.; Watzek, G. Porcine sinus mucosa holds cells that respond to bone morphogenetic protein (BMP)-6 and BMP-7 with increased osteogenic differentiation in vitro. Clin. Oral Implant. Res. 2004, 15, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Srouji, S.; Ben-David, D.; Lotan, R.; Riminucci, M.; Livne, E.; Bianco, P. The innate osteogenic potential of the maxillary sinus (Schneiderian) membrane: An ectopic tissue transplant model simulating sinus lifting. Int. J. Oral Maxillofac. Surg. 2010, 39, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.M.; Botticelli, D.; Moses, O.; Omori, Y.; Fujiwara, S.; Silva, E.R.; Xavier, S.P. Maxillary Sinus Augmentation Using Ceramic Alloplastic Granules or Paste: An Experimental Study in Rabbits. Dent. J. 2021, 9, 65. [Google Scholar] [CrossRef] [PubMed]
- Cordaro, L.; Bosshardt, D.D.; Palattella, P.; Rao, W.; Serino, G.; Chiapasco, M. Maxillary sinus grafting with Bio-Oss or Straumann Bone Ceramic: Histomorphometric results from a randomized controlled multicenter clinical trial. Clin. Oral Implant. Res. 2008, 19, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Kotsu, M.; Apaza Alccayhuaman, K.A.; Ferri, M.; Iezzi, G.; Piattelli, A.; Fortich Mesa, N.; Botticelli, D. Osseointegration at Implants Installed in Composite Bone: A Randomized Clinical Trial on Sinus Floor Elevation. J. Funct. Biomater. 2022, 13, 22. [Google Scholar] [CrossRef]
- Hirota, A.; Iezzi, G.; Piattelli, A.; Ferri, M.; Tanaka, K.; Apaza Alccayhuaman, K.A.; Botticelli, D. Influence of the position of the antrostomy in sinus floor elevation on the healing of mini-implants: A randomized clinical trial. Oral Maxillofac. Surg. 2020, 24, 299–308. [Google Scholar] [CrossRef]
- Imai, H.; Iezzi, G.; Piattelli, A.; Ferri, M.; Apaza Alccayhuaman, K.A.; Botticelli, D. Influence of the Dimensions of the Antrostomy on Osseointegration of Mini-implants Placed in the Grafted Region After Sinus Floor Elevation: A Randomized Clinical Trial. Int. J. Oral Maxillofac. Implant. 2020, 35, 591–598. [Google Scholar] [CrossRef]
- Morimoto, A.; Kobayashi, N.; Ferri, M.; Iezzi, G.; Piattelli, A.; Fortich Mesa, N.; Botticelli, D. Influence on Implant Bone Healing of a Collagen Membrane Placed Subjacent the Sinus Mucosa-A Randomized Clinical Trial on Sinus Floor Elevation. Dent. J. 2022, 10, 105. [Google Scholar] [CrossRef]
- Tanaka, K.; Iezzi, G.; Piattelli, A.; Ferri, M.; Mesa, N.F.; Apaza Alccayhuaman, K.A.; Botticelli, D. Sinus Floor Elevation and Antrostomy Healing: A Histomorphometric Clinical Study in Humans. Implant Dent. 2019, 28, 537–542. [Google Scholar] [CrossRef]
- Masuda, K.; Silva, E.R.; Apaza Alccayhuaman, K.A.; Botticelli, D.; Xavier, S.P. Histologic and Micro-CT Analyses at Implants Placed Immediately After Maxillary Sinus Elevation Using Large or Small Xenograft Granules: An Experimental Study in Rabbits. Int. J. Oral Maxillofac. Implant. 2020, 35, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Sivaraj, K.K.; Adams, R.H. Blood vessel formation and function in bone. Development 2016, 143, 2706–2715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saghiri, M.A.; Asatourian, A.; Garcia-Godoy, F.; Sheibani, N. The role of angiogenesis in implant dentistry part II: The effect of bone-grafting and barrier membrane materials on angiogenesis. Med. Oral Patol. Oral Cir. Buccal 2016, 21, e526–e537. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Kerns, D.G. Mechanisms of guided bone regeneration: A review. Open Dent. J. 2014, 8, 56–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nesti, M.; Carli, E.; Giaquinto, C.; Rampon, O.; Nastasio, S.; Giuca, M.R. Correlation between viral load, plasma levels of CD4–CD8 T lymphocytes and AIDS-related oral diseases: A multicenter study on 30 HIV+ children in the HAART era. J. Biol. Regul. Homeost. Agents 2012, 26, 527–537. [Google Scholar]
- Yang, N.; Liu, Y. The Role of the Immune Microenvironment in Bone Regeneration. Int. J. Med. Sci. 2021, 18, 3697–3707. [Google Scholar] [CrossRef]
- El Khassawna, T.; Serra, A.; Bucher, C.H.; Petersen, A.; Schlundt, C.; Könnecke, I.; Malhan, D.; Wendler, S.; Schell, H.; Volk, H.D.; et al. T Lymphocytes Influence the Mineralization Process of Bone. Front. Immunol. 2017, 8, 562. [Google Scholar] [CrossRef]
- Trindade, R.; Albrektsson, T.; Galli, S.; Prgomet, Z.; Tengvall, P.; Wennerberg, A. Osseointegration and foreign body reaction: Titanium implants activate the immune system and suppress bone resorption during the first 4 weeks after implantation. Clin. Implant Dent. Relat. Res. 2018, 20, 82–91. [Google Scholar] [CrossRef]
- Scala, A.; Lang, N.P.; de Carvalho Cardoso, L.; Pantani, F.; Schweikert, M.; Botticelli, D. Sequential healing of the elevated sinus floor after applying autologous bone grafting: An experimental study in minipigs. Clin. Oral Implant. Res. 2015, 26, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Scharf, D.R.; Tarnow, D.P. Success rates of osseointegration for implants placed under sterile versus clean conditions. J. Periodontol. 1993, 64, 954–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friberg, B. Sterile operating conditions for the placement of intraoral implants. J. Oral Maxillofac. Surg. 1996, 54, 1334–1336. [Google Scholar] [CrossRef]
- Valenti, C.; Pagano, S.; Bozza, S.; Ciurnella, E.; Lomurno, G.; Capobianco, B.; Coniglio, M.; Cianetti, S.; Marinucci, L. Use of the Er:YAG Laser in Conservative Dentistry: Evaluation of the Microbial Population in Carious Lesions. Materials 2021, 14, 2387. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Botticelli, D.; Canullo, L.; Baba, S.; Xavier, S.P. New bone ingrowth into β-TCP/HA graft activated with argon plasma: A histomorphometric study on sinus lifting in rabbits. Int. J. Implant Dent. 2020, 6, 36. [Google Scholar] [CrossRef] [PubMed]
- Skallevold, H.E.; Rokaya, D.; Khurshid, Z.; Zafar, M.S. Bioactive Glass Applications in Dentistry. Int. J. Mol. Sci. 2019, 20, 5960. [Google Scholar] [CrossRef] [Green Version]
- Perini, A.; Viña-Almunia, J.; Carda, C.; Martín de Llano, J.J.; Botticelli, D.; Peñarrocha-Diago, M. Influence of the Use of a Collagen Membrane Placed on the Bone Window after Sinus Floor Augmentation-An Experimental Study in Rabbits. Dent. J. 2021, 9, 131. [Google Scholar] [CrossRef]
- Scala, A.; Viña-Almunia, J.; Carda, C.; Martín de Llano, J.J.; Soto-Peñaloza, D.; Peñarrocha-Diago, M.; Peñarrocha-Diago, M.; Botticelli, D. Sequential healing of the elevated sinus floor with different size of antrostomy: A histomorphometric study in rabbits. Oral Maxillofac. Surg. 2020, 24, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, D.; Lang, N.P. Dynamics of osseointegration in various human and animal models—A comparative analysis. Clin. Oral Implant. Res. 2017, 28, 742–748. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
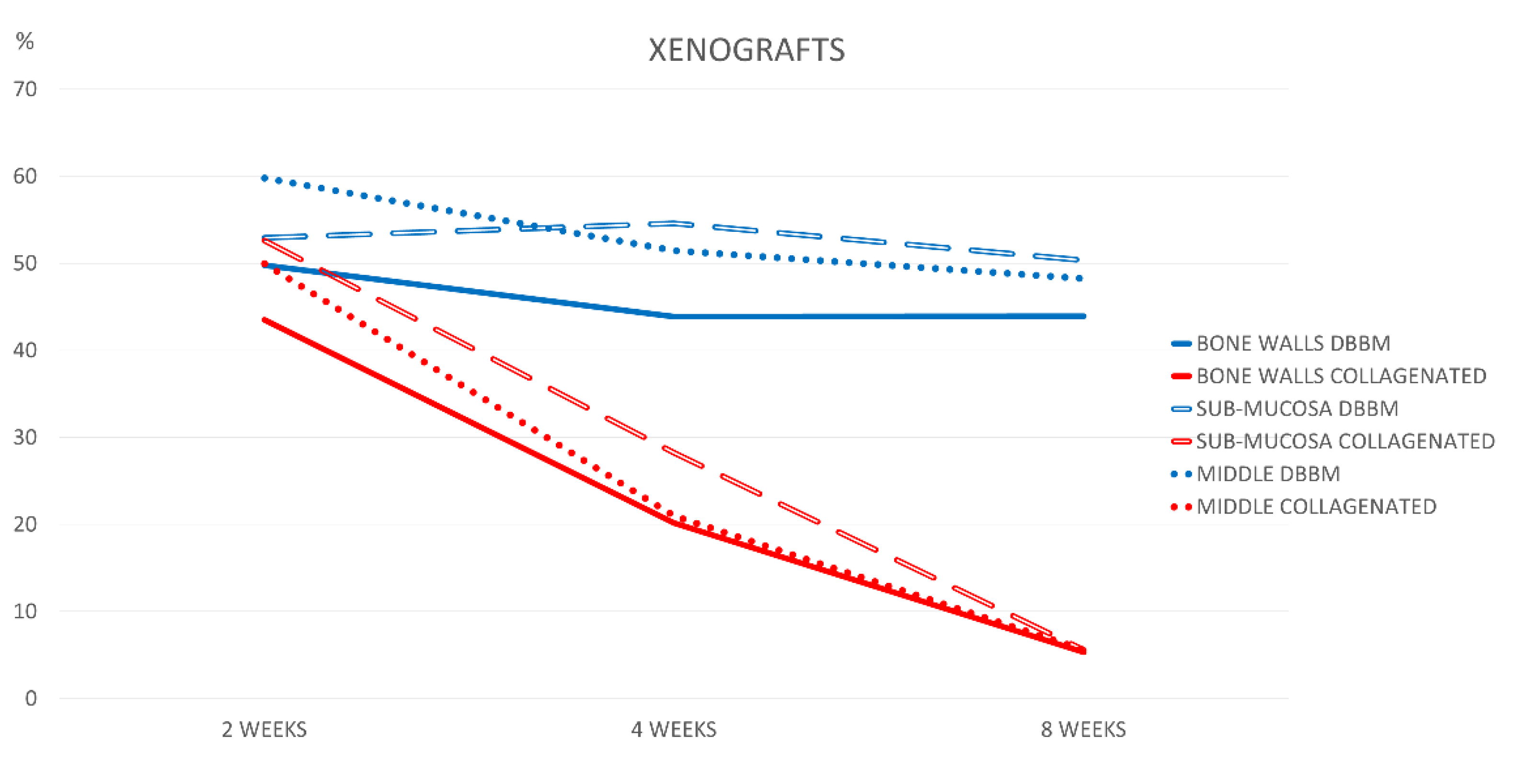
| New Bone | Xenograft | Soft Tissues | Osteoclastic Zones | Vessels | Inflammatory Infiltrate | |
|---|---|---|---|---|---|---|
| 2 Weeks DBBM | 11.5 ± 7.6 * | 49.8 ± 5.3 * | 33.9 ± 7.5 * | 0.7 ± 0.9 * | 4.2 ± 3.8 | 0.0 ± 0.0 * |
| 2 Weeks Collagenated | 1.6 ± 1.7 * | 43.5 ± 4.3 * | 48.8 ± 3.5 * | 2.7 ± 0.8 * | 2.6 ± 1.5 | 0.7 ± 0.6 * |
| p value | 0.011 | 0.048 | 0.001 | 0.010 | 0.810 | 0.002 |
| 4 Weeks DBBM | 24.7 ± 6.2 | 43.9 ± 4.1 * | 26.8 ± 6.6 * | 0.0 ± 0.1 * | 4.6 ± 1.3 | 0.0 ± 0.0 * |
| 4 Weeks Collagenated | 20.4 ± 15.2 | 20.2 ± 12.9 * | 44.4 ± 7.3 * | 5.3 ± 2.6 * | 8.7 ± 5.0 | 0.9 ± 1.0 * |
| p value | 0.535 | 0.002 | 0.001 | 0.003 | 0.079 | 0.007 |
| 8 Weeks DBBM | 28.6 ± 5.3 * | 43.9 ± 4.4 * | 26.3 ± 2.5 * | 0.0 ± 0.0 * | 0.9 ± 0.7 * | 0.2 ± 0.5 |
| 8 Weeks Collagenated | 41.6 ± 6.5 * | 5.3 ± 4.3 * | 43.1 ± 5.5 * | 0.6 ± 0.5 * | 9.4 ± 3.1 * | 0.1 ± 0.3 |
| p value | 0.004 | 0.004 | 0.004 | 0.002 | <0.0001 | 0.902 |
| New Bone | Xenograft | Soft Tissues | Osteoclastic Zones | Vessels | Inflammatory Infiltrate | |
|---|---|---|---|---|---|---|
| 2 Weeks DBBM | 5.6 ± 13.6 | 53.0 ± 10.7 | 37.5 ± 5.5 | 0.6 ± 0.8 * | 3.4 ± 3.1 | 0.0 ± 0.0 |
| 2 Weeks Collagenated | 0.0 ± 0.0 | 52.6 ± 5.5 | 42.8 ± 4.6 | 2.0 ± 1.0 * | 2.3 ± 1.4 | 0.3 ± 0.4 |
| p value | 0.317 | 0.631 | 0.100 | 0.024 | 0.457 | 0.059 |
| 4 Weeks DBBM | 5.7 ± 7.8 | 54.6 ± 9.4 * | 36.9 ± 8.9 * | 1.3 ± 1.4 * | 1.5 ± 1.3 | 0.0 ± 0.0 * |
| 4 Weeks Collagenated | 5.7 ± 11.2 | 28.2 ± 1.8 * | 50.1 ± 10.7 * | 9.6 ± 7.5 * | 3.9 ± 3.9 | 2.5 ± 2.2 * |
| p value | 0.494 | 0.002 | 0.042 | 0.024 | 0.186 | 0.007 |
| 8 Weeks DBBM | 28.6 ± 14.0 | 50.3 ± 4.6 * | 20.2 ± 10.4 * | 0.3 ± 0.9 | 0.4 ± 1.1 * | 0.0 ± 0.0 * |
| 8 Weeks Collagenated | 28.1 ± 16.4 | 5.6 ± 4.4 * | 54.6 ± 21.5 * | 2.3 ± 3.4 | 8.8 ± 5.0 * | 0.7 ± 0.6 * |
| p value | 0.950 | <0.0001 | 0.006 | 0.216 | 0.003 | 0.022 |
| New Bone | Xenograft | Soft Tissues | Osteoclastic Zones | Vessels | Inflammatory Infiltrate | |
|---|---|---|---|---|---|---|
| 2 Weeks DBBM | 1.8 ± 4.5 | 59.8 ± 8.6 * | 34.3 ± 6.9 * | 1.6 ± 1.6 | 2.1 ± 1.8 | 0.3 ± 0.9 |
| 2 Weeks Collagenated | 0.1 ± 0.2 | 50.0 ± 6.3 * | 46.0 ± 6.5 * | 1.2 ± 0.5 | 2.4 ± 1.1 | 0.4 ± 0.4 |
| p value | 0.902 | 0.048 | 0.032 | 0.571 | 0.470 | 0.210 |
| 4 Weeks DBBM | 11.9 ± 6.0 | 51.5 ± 14.9 * | 31.3 ± 7.5 * | 0.0 ± 0.0 * | 5.4 ± 4.1 | 0.0 ± 0.0 * |
| 4 Weeks Collagenated | 10.2 ± 18.2 | 21.0 ± 19.7 * | 55.8 ± 16.2 * | 5.2 ± 2.8 * | 6.5 ± 5.9 | 1.4 ± 1.4 * |
| p value | 0.149 | 0.013 | 0.007 | 0.002 | 0.719 | 0.022 |
| 8 Weeks DBBM | 23.2 ± 12.8 | 48.3 ± 7.0 * | 27.8 ± 7.0 * | 0.2 ± 0.4 | 0.6 ± 0.8 * | 0.0 ± 0.0 * |
| 8 Weeks Collagenated | 25.1 ± 8.0 | 5.6 ± 3.2 * | 56.2 ± 12.8 * | 1.3 ± 2.5 | 10.1 ± 4.9 * | 1.6 ± 2.0 * |
| p value | 0.764 | <0.0001 | 0.001 | 0.216 | 0.006 | 0.022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyauchi, Y.; Izutani, T.; Teranishi, Y.; Iida, T.; Nakajima, Y.; Xavier, S.P.; Baba, S. Healing Patterns of Non-Collagenated Bovine and Collagenated Porcine Xenografts Used for Sinus Floor Elevation: A Histological Study in Rabbits. J. Funct. Biomater. 2022, 13, 276. https://doi.org/10.3390/jfb13040276
Miyauchi Y, Izutani T, Teranishi Y, Iida T, Nakajima Y, Xavier SP, Baba S. Healing Patterns of Non-Collagenated Bovine and Collagenated Porcine Xenografts Used for Sinus Floor Elevation: A Histological Study in Rabbits. Journal of Functional Biomaterials. 2022; 13(4):276. https://doi.org/10.3390/jfb13040276
Chicago/Turabian StyleMiyauchi, Yuhei, Takayuki Izutani, Yuki Teranishi, Takahisa Iida, Yasushi Nakajima, Samuel Porfirio Xavier, and Shunsuke Baba. 2022. "Healing Patterns of Non-Collagenated Bovine and Collagenated Porcine Xenografts Used for Sinus Floor Elevation: A Histological Study in Rabbits" Journal of Functional Biomaterials 13, no. 4: 276. https://doi.org/10.3390/jfb13040276
APA StyleMiyauchi, Y., Izutani, T., Teranishi, Y., Iida, T., Nakajima, Y., Xavier, S. P., & Baba, S. (2022). Healing Patterns of Non-Collagenated Bovine and Collagenated Porcine Xenografts Used for Sinus Floor Elevation: A Histological Study in Rabbits. Journal of Functional Biomaterials, 13(4), 276. https://doi.org/10.3390/jfb13040276