
Personalized Antibiotic Therapy for the Critically Ill: Implementation Strategies and Effects on Clinical Outcome of Piperacillin Therapeutic Drug Monitoring—A Descriptive Retrospective Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Study Population
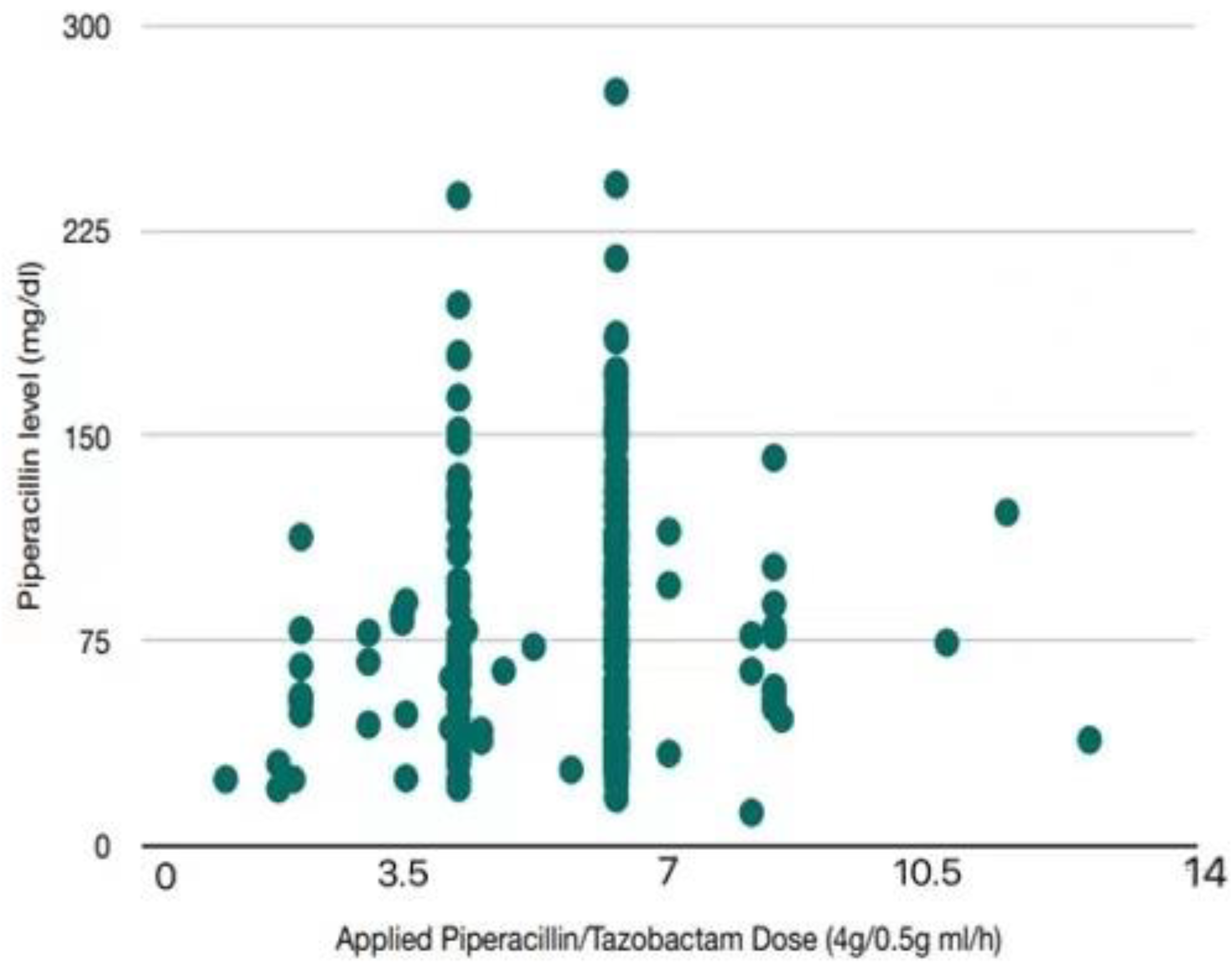
2.2. Measurement of Piperacillin Levels
2.3. Outcomes
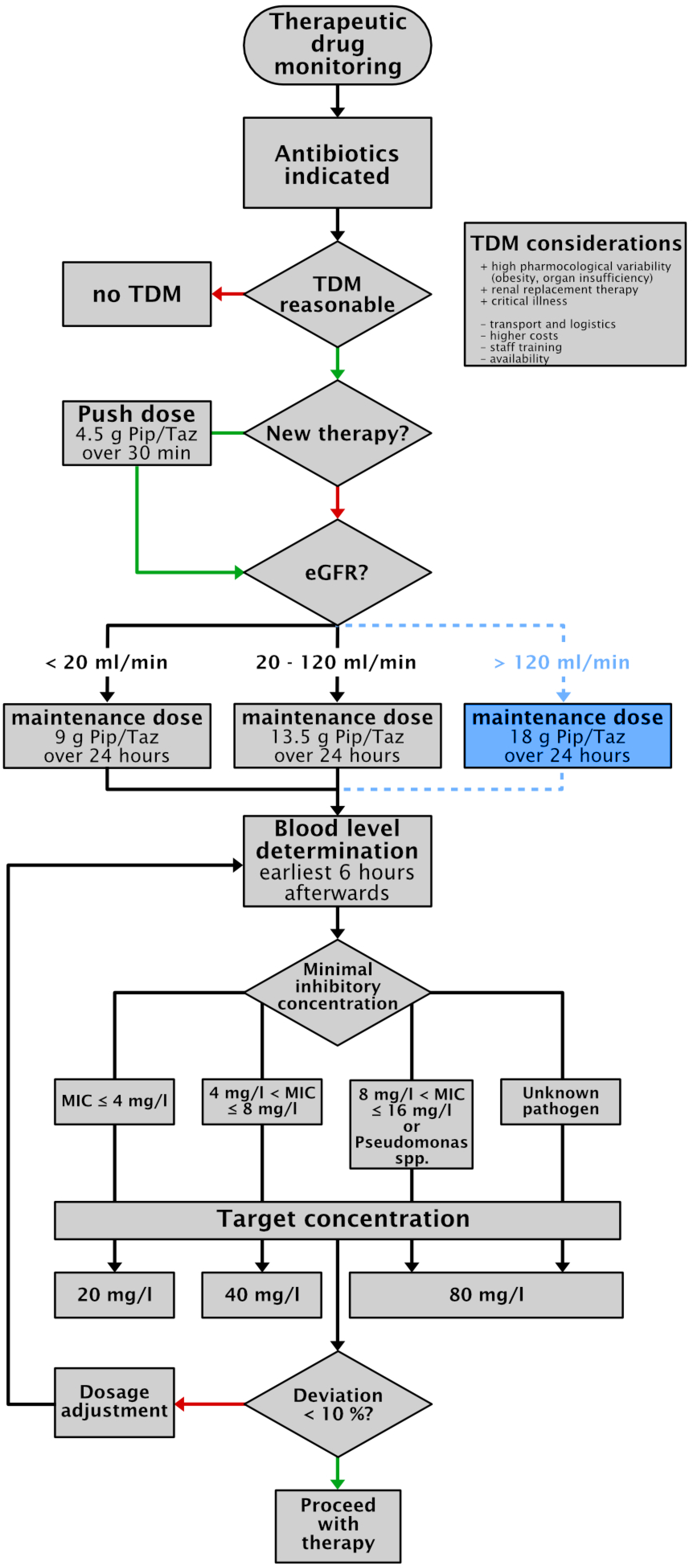
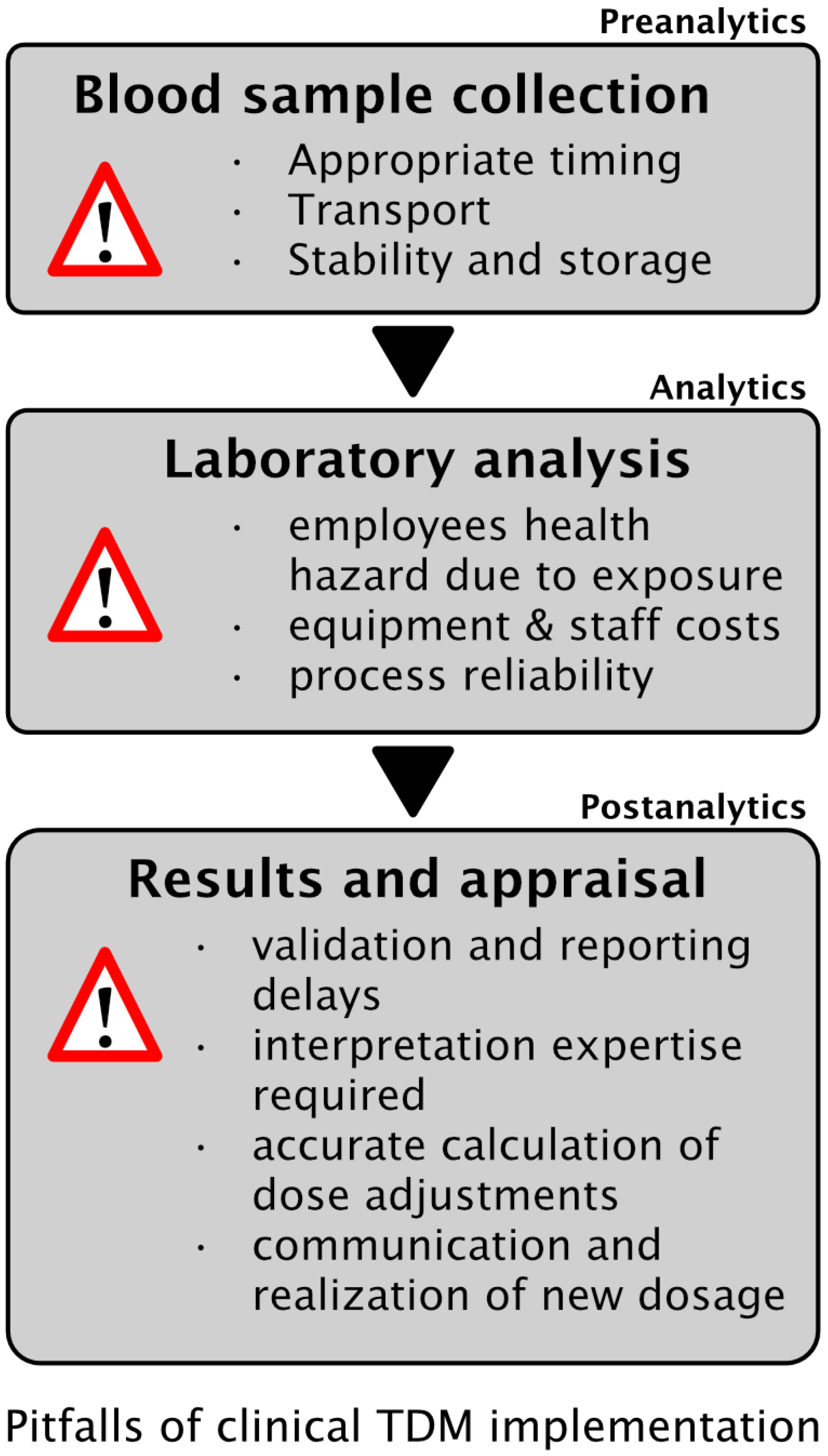
2.4. Implementation of TDM
3. Discussion
4. Materials and Methods
4.1. Study Design and Patient Population
4.2. Established TDM Concept for PIP/TAZ
4.3. Preparation and Initial Dosing of PIP/TAZ Infusion
4.4. Drug Level Measurement and Sample Collection
4.5. Pharmacokinetic and Pharmacodynamics Targets
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.C.M.; et al. The third international consensus definitions for sepsis and septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Ellis, P.; Arabi, Y.; Roberts, D.; Light, B.; Parrillo, J.E.; Dodek, P.; Wood, G.; Kumar, A.; Simon, D.; et al. Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Chest 2009, 136, 1237–1248. [Google Scholar] [CrossRef] [PubMed]
- Liu, V.X.; Fielding-Singh, V.; Greene, J.D.; Baker, J.M.; Iwashyna, T.J.; Bhattacharya, J.; Escobar, G.J. The timing of early antibiotics and hospital mortality in sepsis. Am. J. Respir. Crit. Care Med. 2017, 196, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Ince, C.; Mayeux, P.R.; Nguyen, T.; Gomez, H.; Kellum, J.A.; Ospina-Tascón, G.A.; Hernandez, G.; Murray, P.; De Backer, D. The endothelium in sepsis. Shock 2016, 45, 259–270. [Google Scholar] [CrossRef] [Green Version]
- Zander, J.; Döbbeler, G.; Nagel, D.; Maier, B.; Scharf, C.; Huseyn-Zada, M.; Jung, J.; Frey, L.; Vogeser, M.; Zoller, M. Piperacillin concentration in relation to therapeutic range in critical ill patients–a prospective study. Crit. Care 2016, 20, 79. [Google Scholar] [CrossRef] [Green Version]
- König, C.; Braune, S.; Roberts, J.; Nierhaus, A.; Steinmetz, O.M.; Baehr, M.; Frey, O.R.; Langebrake, C.; Kluge, S. Population pharmacokinetics and dosing simulation of ceftazidime in critically ill patients receiving sustained low-efficiency dialysis. J. Antimircob. Chemother. 2017, 72, 1433–1440. [Google Scholar] [CrossRef]
- Zoller, M.; Maier, B.; Hornuss, C.; Neugebauer, C.; Döbbeler, G.; Nagel, D.; Holdt, L.M.; Bruegel, M.; Weig, T.; Grabein, B.; et al. Variability of linezolid concentrations after standard dosing in critical ill patients: A prospective observational study. Crit. Care 2014, 18, R148. [Google Scholar] [CrossRef] [Green Version]
- Ishihara, N.; Nishimura, N.; Ikawa, K.; Karino, F.; Miura, K.; Tamaki, H.; Yano, T.; Isobe, T.; Morikawa, N.; Naora, K. Population pharmacokinetic modeling and pharmacodynamics target attainment simulation of piperacillin/Tazobactam for dosing optimization in late elderly patients with pneumonia. Antibiotics 2020, 9, 113. [Google Scholar] [CrossRef] [Green Version]
- Abdul-Aziz, M.-H.; Alffenaar, J.-W.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.-A.; Pea, F.; Sjovall, F.; et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: A Position Paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef]
- Drusano, G.L. Antimicrobial pharmacodynamics: Critical interactions of bug and drug. Nat. Rev. Microbiol. 2004, 2, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Paul, S.K.; Akova, M.; Bassetti, M.; De Waele, J.J.; Dimopoulos, G.; Kaukonen, K.-M.; Koulenti, D.; Martin, C.; Montravers, P.; et al. Defining antibiotic levels in intensive care unit patients. Are current beta-lactam antibiotic doses sufficient for critically ill patients? Clin. Infect. Dis. 2014, 58, 1072–1083. [Google Scholar] [CrossRef]
- Taccone, F.S.; Laterre, P.-F.; Dugernier, T.; Spapen, H.; Delattre, I.; Wittebole, X.; De Backer, D.; Layeux, B.; Wallemacq, P.; Vincent, J.-L.; et al. Insufficient beta-lactam concentrations in the early phase of severe sepsis and septic shock. Crit. Care 2010, 14, R126. [Google Scholar] [CrossRef] [Green Version]
- Arroyo-Currás, N.; Somerson, J.; Vieira, P.; Ploense, K.L.; Kippin, T.E.; Plaxco, K.W. Real-time measurement of small molecules directly in awake, ambulatory animals. Proc. Natl. Acad. Sci. USA 2017, 114, 645–650. [Google Scholar] [CrossRef] [Green Version]
- Rawson, T.M.; Gowers, S.A.N.; Freeman, D.M.E.; Wilson, R.C.; Sharma, S.; Gilchrist, M.; MacGowan, A.; Lovering, A.; Bayliss, M.; Kyriakides, M.; et al. Microneedle biosensors for real-time, minimally invasive drug monitoring of phenoxymethylpenecillin: A first-in-human evaluation in healthy volunteers. Lancet Digit. Health 2019, 7, E335–E343. [Google Scholar] [CrossRef] [Green Version]
- Mabilat, C.; Gros, M.F.; Nicolau, D.; Mouton, J.W.; Textoris, J.; Roberts, J.A.; Cotta, M.O.; Van Belkum, A.; Caniaux, I. Diagnostic and medical needs for therapeutic drug monitoring of antibiotics. Eur. J. Clin. Micro. Infect. Dis. 2020, 39, 791–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawson, T.M.; Wilson, R.C.; O’Hare, D.; Herrero, P.; Kambugu, A.; Lamorde, M.; Ellington, M.; Georgiou, P.; Cass, A.; Hope, W.W.; et al. Optimizing antimicrobial use: Challenges, advances and opportunities. Nat. Rev. Microbiol. 2021, 19, 747–758, epub ahead of print. [Google Scholar] [CrossRef]
- El-Najjar, N.; Jantsch, J.; Gessner, A. The use of liquid chromotography-tandem mass spectrometry for therapeutic drug monitoring of antibiotics in cancer patients. Clin. Chem. Lab. Med. 2017, 55, 1246–1261. [Google Scholar] [CrossRef] [Green Version]
- Vogeser, M. Liquid chromotography–tandem mass sprectrometry–applicaton in clinical laboratory. Clin. Chem. Lab. Med. 2003, 41, 117–126. [Google Scholar] [CrossRef] [Green Version]
- Roberts, J.; Kirkpatrick, C.; Roberts, M.; Robertson, T.; Dalley, A.; Lipman, J. Meropenem dosing in critically ill patients with sepsis and without renal dysfunction: Intermittent bolus versus continuous administration? Monte Carlo dosing simulations and subcutaneous tissue distribution. J. Antimicrob. Chemother. 2009, 54, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Abdul-Aziz, M.H.; Sulaiman, H.; Mat-Nor, M.; Rai, V.; Wong, K.K.; Hasan, M.S.; Abd Rahman, A.N.; Jamal, J.A.; Wallis, S.C.; Lipman, J.; et al. Beta-Lactam infusion in severe sepsis (BLISS): A prospective, two centre, open-labelled randomized controlled trial of continuous versus intermittent beta-lactam infusion in critically ill patients with severe sepsis. Intensive Care Med. 2016, 42, 1535–1545. [Google Scholar] [CrossRef] [PubMed]
- Richter, D.; Dietrich, M.; Lalev, L.; Schmitt, F.; Fiedler, M.; Bruckner, T.; Stoerzinger, D.; Chiriac, U.; Klein, S.; Hackert, T.; et al. Prolonged infusion of β-Lactams decreases mortality in patients with septic shock: A retrospective before-after Study. Antibiotics 2021, 10, 687. [Google Scholar] [CrossRef] [PubMed]
- Allerberger, F.; Amann, S.; Apfalter, P.; Brodt, H.-R.; Eckmanns, T.; Fellhauer, M.; Geiss, H.K.; Janata, O.; Krause, R.; Lemmen, S.; et al. Strategies to enhance rational use of antibiotics in hospital: A guideline by the German Society for Infection diseases. Infection 2016, 44, 395–439. [Google Scholar]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C.; et al. Optimization of the treatment with beta-lactam antibiotics in critically ill patients–guidelines from the French Society of Pharmacology and Therapeutics and the French Society of Anaesthesia and Intensive Care Medicine. Crit. Care 2019, 23, 104. [Google Scholar] [CrossRef] [Green Version]
- Abdulla, A.; Dijkstra, A.; Hunfeld, N.G.M.; Endeman, H.; Bahmany, S.; Ewoldt, T.M.J.; Muller, A.E.; Van Gelder, T.; Gommers, D.; Koch, B.C.P. Failure of target attainment of beta-lactam in critically ill patients and associated risk factors: A two-center prospective study (EXPAT). Crit. Care 2020, 24, 1–24. [Google Scholar] [CrossRef]
- Chiriac, U.; Richter, D.; Frey, O.; Röhr, A.; Helbig, S.; Preisenberger, J.; Hagel, S.; Roberts, J.; Weigand, M.; Brinkmann, A. Personalized piperacillin dosing for critically ill: A retrospective analysis of clinical experience with dosing software and therapeutic drug monitoring to optimize antimicrobial dosing. Antibiotics 2021, 10, 667. [Google Scholar] [CrossRef]
- Ehmann, L.; Zoller, M.; Minichmayr, I.K.; Scharf, C.; Maier, B.; Schmitt, M.V.; Hartung, N.; Huisinga, W.; Vogeser, M.; Frey, L.; et al. Role of renal function in risk assessment of target non-attainment after standard dosing of meropenem in critically ill patients: A prospective observational study. Crit. Care 2017, 21, 263. [Google Scholar] [CrossRef] [Green Version]
- Abdul-Aziz, M.-H.; Lipman, J.; Mouton, J.W.; Hope, W.; Roberts, J.A. Applying pharmacokinetic/pharmacodynamics principles in critically ill patients optimizing efficacy and reducing resistance development. Semin. Respir. Crit. Care Med. 2015, 36, 136–153. [Google Scholar] [CrossRef] [Green Version]
- Dhaese, S.A.M.; Thooft, A.D.J.; Farkas, A.; Lipman, J.; Verstraete, A.G.; Stove, V.; Roberts, J.A.; De Waele, J.J. Early target attainment of continuous infusion piperacillin/tazobactam and meropenem in critically ill patients: A prospective oberservational study. J. Crit. Care 2019, 52, 75–79. [Google Scholar] [CrossRef]
- Richter, D.C.; Frey, O.; Rhr, A.; Roberts, J.A.; Kberer, A.; Fuchs, T.; Papadimas, N.; Heinzel-Gutenbrunner, M.; Brenner, T.; Lichtenstern, C.; et al. Therpeutic drug monitoring-guided continuous infusion of piperacillin/tazobactam significantly improves pharmacokinetic target attainment in critically ill patients: A retrospective analysis of four years of clinical experience. Infection 2019, 47, 1001–1011. [Google Scholar] [CrossRef] [Green Version]
- Scharf, C.; Liebchen, U.; Paal, M.; Taubert, M.; Vogeser, M.; Irlbeck, M.; Zoller, M.; Schroeder, I. The higher the better? Defining the optimal beta-lactam target for critically ill patients to reach infection resolution and improve outcome. J. Intensive Care 2020, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Kuti, J.L.; Nightingale, C.H.; Mansfield, D.L.; Dana, A.; Nicolau, D.P. Population pharmacokinetics and pharmacodynamics of piperacillin/tazobactam in patients with complicated intra-abdominal infection. J. Antimicrob. Chemother. 2005, 56, 388–395. [Google Scholar] [CrossRef]
- Dhaese, S.A.M.; Colin, P.; Willems, H.; Heffernan, A.; Gadeyne, B.; Van Vooren, S.; Depuydt, P.; Hoste, E.; Stove, V.; Verstraete, A.G.; et al. Saturable elimination of piperacillin in critically ill patients: Implications for continous infusion. Int. Antimicrob. Agents 2019, 54, 741–749. [Google Scholar] [CrossRef]
- Landersdorfer, C.B.; Bulitta, J.B.; Kirkpatrick, C.M.J.; Kinzig, M.; Holzgrabe, U.; Drusano, G.L.; Stephan, U.; Sörgel, F. Population pharmacokinetics of piperacillin at two dose levels: Influence of nonlinear pharmacokinetics on the pharmacodynamic profile. Antimicrob. Agents Chemother. 2021, 56, 5715–5723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felton, T.W.; Hope, W.; Lomaestro, B.M.; Butterfield, J.M.; Kwa, A.L.; Drusano, G.L.; Lodise, T.P. Population pharmacokinetics of extended infusion piperacillin-tazobactam in hospitalized patients with nosocomial infections. Antimicrob. Agents Chemother. 2012, 56, 4087–4094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagel, S.; Fiedler, S.; Hohn, A.; Brinkmann, A.; Frey, O.R.; Hoyer, H.; Schlattmann, P.; Kiehntopf, M.; Roberts, J.A.; Pletz, M.W. on behalf of the TARGET Study Group. Therapeutic drug monitoring-based dose optimisation of piperacillin/tazobactam to improve outcome in patients with sepsis (TARGET): A prospective, multi-centre, randomised controlled trial. Trials 2019, 20, 330. [Google Scholar] [CrossRef] [Green Version]
- Carrie, C.; Legeron, R.; Petit, L.; Ollivier, J.; Cottenceau, V.; d’Houdain, N.; Boyer, P.; Lafitte, M.; Xuereb, F.; Sztark, F.; et al. Higher than standard dosing regimen are needed to achieve optimal antibiotic exposure in critically ill patients with augmented renal clearance receiving piperacillin-tazobactam administered by continous infusion. J. Crit. Care 2018, 48, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Besnard, T.; Carrié, C.; Petit, L.; Biais, M. Increased dosing regimens of piperacillin-tazobactam are needed to avoid subtherapeutic exposure in critically ill patients with augmented renal clearance. Crit. Care 2019, 23, 13. [Google Scholar] [CrossRef] [Green Version]
- Wong, G.; Brinkman, A.; Benefield, R.J.; Carlier, M.; De Waele, J.; El Helali, N.; Frey, O.; Harbarth, S.; Huttner, A.; McWhinney, B.; et al. An international, multicenter survey of beta-lactam antibiotic therapeutic drug monitoring practice in intensive care units. J. Antimicrob. Chemother. 2014, 69, 1416–1423. [Google Scholar] [CrossRef] [Green Version]
- Wong, G.; Briscoe, S.; McWhinney, B.; Ally, M.; Ungerer, J.; Lipman, J.; Roberts, J.A. Therapeutic drug monitoring of beta-lactam antibiotics in the critically ill: Direct measurements of unbound drug concentrations to achieve appropriate drug exposures. J. Antimicrob. Chemother. 2018, 73, 3087–3094. [Google Scholar] [CrossRef] [Green Version]
- Quinton, M.-C.; Bodeau, S.; Kontar, L.; Zerbib, Y.; Maizel, J.; Slama, M.; Masmoudi, K.; Lemaire-Hurtel, A.-S.; Bennis, Y. Neurotoxic concentration of piperacillin during continuous infusion in critically ill patients. Antimicrob. Agents Chemother. 2017, 61, e0065417. [Google Scholar] [CrossRef] [Green Version]
- Neely, M.N.; Youn, G.; Jones, B.; Jelliffe, R.W.; Drusano, G.L.; Rodvold, K.A.; Lodise, T.P. Are Vancomycin trough concentrations adequate for optimal dosing? Antimicrob. Agents Chemother. 2014, 58, 309–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avent, M.L.; Rogers, B.A. Optimising antimicrobial therapy through the use of baysian dosing programs. Int. J. Clin. Pharm. 2019, 41, 1121–1130. [Google Scholar] [CrossRef] [PubMed]
- Ates, H.C.; Roberts, J.A.; Lipman, J.; Cass, A.E.; Urban, G.A.; Dincer, C. On-site therapeutic drug monitoring. Trends Biotechnol. 2020, 38, 11. [Google Scholar] [CrossRef]
- Heil, E.L.; Nicolau, D.P.; Farkas, A.; Roberts, J.A.; Thom, K.A. Pharmacodynamic target attainment for cefepime, meropenem and piperacillin/tazobactam using a pharmacokinetic /pharmcodynamic based dosing calculator in critically ill paitents. Antimicrob. Agents Chemother. 2018, 62, e01008–e01018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neely, M.; Philippe, M.; Rushing, T.; Fu, X.; Van Guilder, M.; Bayard, D.; Schumitzky, A.; Bleyzac, N.; Goutelle, S. Accurately achieving target busulfan exposure in children and adolescents with very limited sampling and the Best-dose software. Ther. Drug Monit. 2016, 38, 332–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neely, M.N.; Kato, L.; Youn, G.; Kraler, L.; Bayard, D.; van Guilder, M.; Schumitzky, A.; Yamada, W.; Jones, B.; Minejima, E. Prospective trial on the use of trough concentration versus area under the curve to determine therapeutic vancomycin dosing. Antimicrob. Agents Chemother. 2018, 62, e02042-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul-Ehrlich-Gesellschaft für Chemotherapie e.V. Kalkulierte Parenterale Initialtherapie Bakterieller Erkrankungen Bei Erwachsenen—Update 2018. Available online: https://www.awmf.org/uploads/tx_szleitlinien/082-0061_S2k_parenterale_antibiotika_2019-08.pdf (accessed on 31 August 2021).
- European Committee on Antimicrobial Susceptibility Testing. Available online: https://eucast.org/clinical_breakpoints/ (accessed on 28 July 2021).




{kind=link}
{kind=link}
{kind=link}
| TDM-Level | >100 mg/L (n = 71) | >22.5–<100 mg/L (n = 194) | <22.5 mg/L (n = 6) |
|---|---|---|---|
| Infusion rate (4 g/0.5 g) [mL/h] | 5.88 ± 1.29 (min. 2.1, max. 11.5) | 5.68 ± 1.54 (min. 1.1, max. 12.6) | 5.5 ± 2.19 (min. 4.2, max. 8.1) |
| Age [a] | 66 ± 22 (min. 42, max. 92) | 62 ± 14 (min. 21, max 92) | 47 ± 10 (min 40, max. 65) # |
| Height [cm] | 175 ± 11 (min. 150, max. 195) | 174 ± 10 (min. 152, max. 195) | 181 ± 9 cm (min. 165, max. 193) |
| Weight [kg] | 90 ± 21 (min. 47, max. 140) | 91 ± 25 (min. 53, max. 184) | 98 ± 19 kg (min. 77, max. 130) |
| BMI [kg/m²] | 30 ± 8 (min. 15, max. 62) | 30 ± 8 (min. 15, max. 57) | 30 ± 6 (min. 24, max. 40) |
| Creatinine [mg/dL] | 2.19 ± 0.97 (min. 0.58, max. 4.30) § | 1.41 ± 0.84 (min. 0.27, max. 4.26) | 0.92 ± 0.56 (min. 12.1, max. 2.01) |
| GFR [mL/min/1.73 m²] | 40.9 ± 26.7 (min. 12, max. 150) § | 75.4 ± 51.8 (min. 8.6, max. 280) | 120.5 ± 70.5 (min. 38, max 252) |
| Hemoglobin [g/dL] | 8.6 ± 1.0 (min. 6.9, max. 12.1) | 8.9 ± 1.8 (min. 6.3, max. 24.6) | 10.2 ± 2.3 (min. 6.9, max. 13.1) |
| Leukocytes [* 1000/µL] | 15.7 ± 8.4 (min. 3.3, max. 42.1) | 12.9 ± 6.1 (min. 0.4, max. 32.5) | 14.2 ± 6.0 (min. 6.0 max. 23.8) |
| Thrombocytes [* 1000/µL] | 180 ± 99 (min. 42, max. 476) | 228 ± 140 (min. 37, max. 968) | 246 ± 81 (min. 118, max. 368) |
| CRP [mg/dL] | 20.2 ± 11.7 (min. 1.1, max. 52.5) § | 16.9 ± 12.0 (min. 0.9, max. 60.5) | 5.8 ± 5.1 (min. 1.1, max. 14.1) # |
| Procalcitonin [ng/mL] | 18.8 ± 36.6 (min. 0.2, max. 189.5) § | 4.8 ± 11.2 (min. 0.1, max. 94.4) | n.d. |
| Interleukin-6 [pg/mL] | 453 ± 717 (min. 7, max. 4025) | 510 ± 2866 (min. 4, max. 35,500) | 49 ± 69 (min. 8, max. 172) # |
| Norepinephrine [µg/min] | 8.1 ± 9.3 (min. 0, max. 33) | 5.5 ± 9.8 (min. 0, max. 56) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikolas, S.; Thorsten, R.; Max, K.; Patrick, M.; Markus, K.; Güzin, S.; Oliver, S.-C.; Alexander, S.; Andreas, P.; Kerstin, H. Personalized Antibiotic Therapy for the Critically Ill: Implementation Strategies and Effects on Clinical Outcome of Piperacillin Therapeutic Drug Monitoring—A Descriptive Retrospective Analysis. Antibiotics 2021, 10, 1452. https://doi.org/10.3390/antibiotics10121452
Nikolas S, Thorsten R, Max K, Patrick M, Markus K, Güzin S, Oliver S-C, Alexander S, Andreas P, Kerstin H. Personalized Antibiotic Therapy for the Critically Ill: Implementation Strategies and Effects on Clinical Outcome of Piperacillin Therapeutic Drug Monitoring—A Descriptive Retrospective Analysis. Antibiotics. 2021; 10(12):1452. https://doi.org/10.3390/antibiotics10121452
Chicago/Turabian StyleNikolas, Schrader, Riese Thorsten, Kurlbaum Max, Meybohm Patrick, Kredel Markus, Surat Güzin, Scherf-Clavel Oliver, Strate Alexander, Pospiech Andreas, and Hoppe Kerstin. 2021. "Personalized Antibiotic Therapy for the Critically Ill: Implementation Strategies and Effects on Clinical Outcome of Piperacillin Therapeutic Drug Monitoring—A Descriptive Retrospective Analysis" Antibiotics 10, no. 12: 1452. https://doi.org/10.3390/antibiotics10121452
APA StyleNikolas, S., Thorsten, R., Max, K., Patrick, M., Markus, K., Güzin, S., Oliver, S. -C., Alexander, S., Andreas, P., & Kerstin, H. (2021). Personalized Antibiotic Therapy for the Critically Ill: Implementation Strategies and Effects on Clinical Outcome of Piperacillin Therapeutic Drug Monitoring—A Descriptive Retrospective Analysis. Antibiotics, 10(12), 1452. https://doi.org/10.3390/antibiotics10121452