
Short and Concise Peer-to-Peer Teaching—Example of a Successful Antibiotic Stewardship Intervention to Increase Iv to Po Conversion

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Step 1—Plan
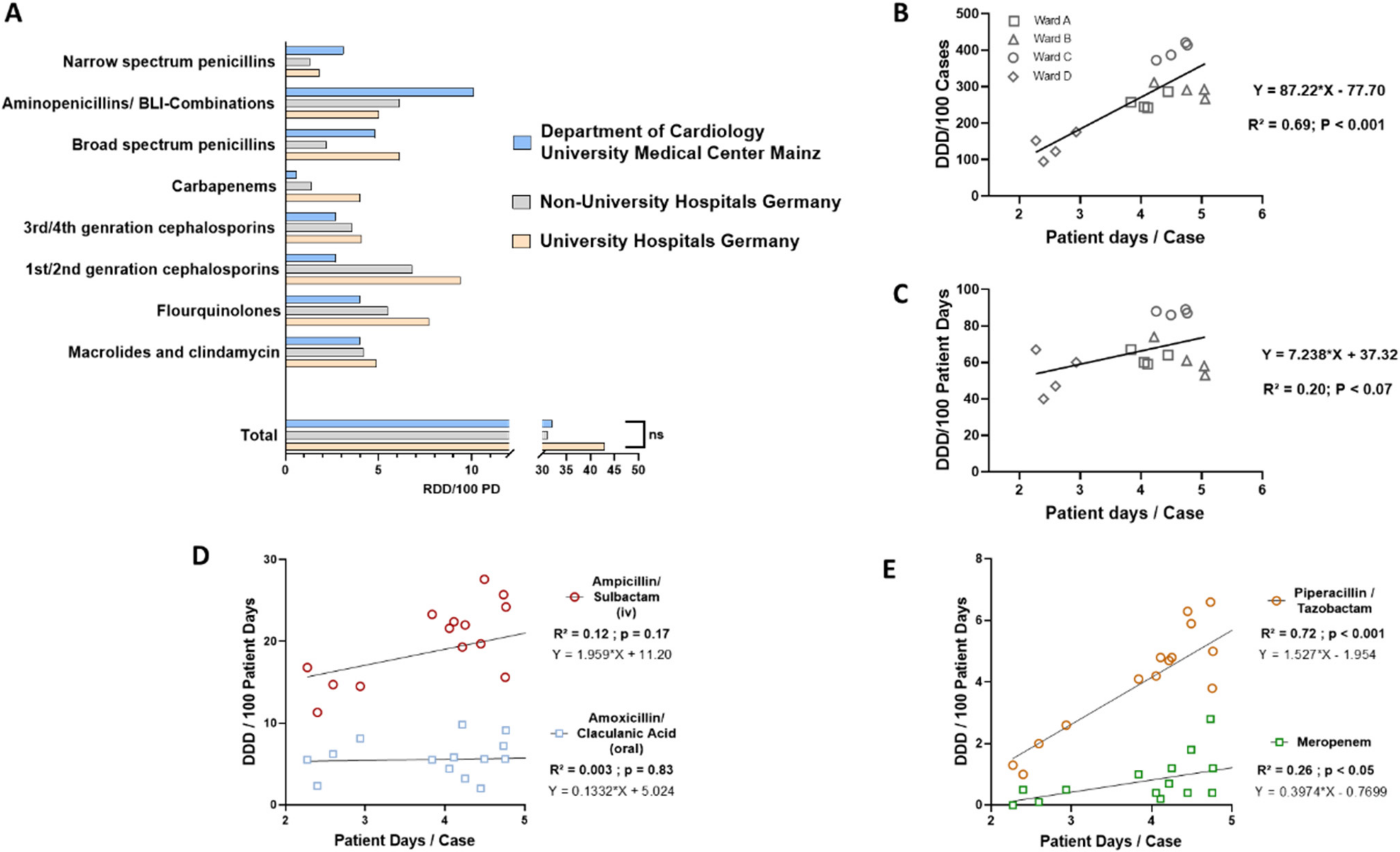
2.1.1. Comparative Characterization and Identification of Determinants of Antibiotic Use
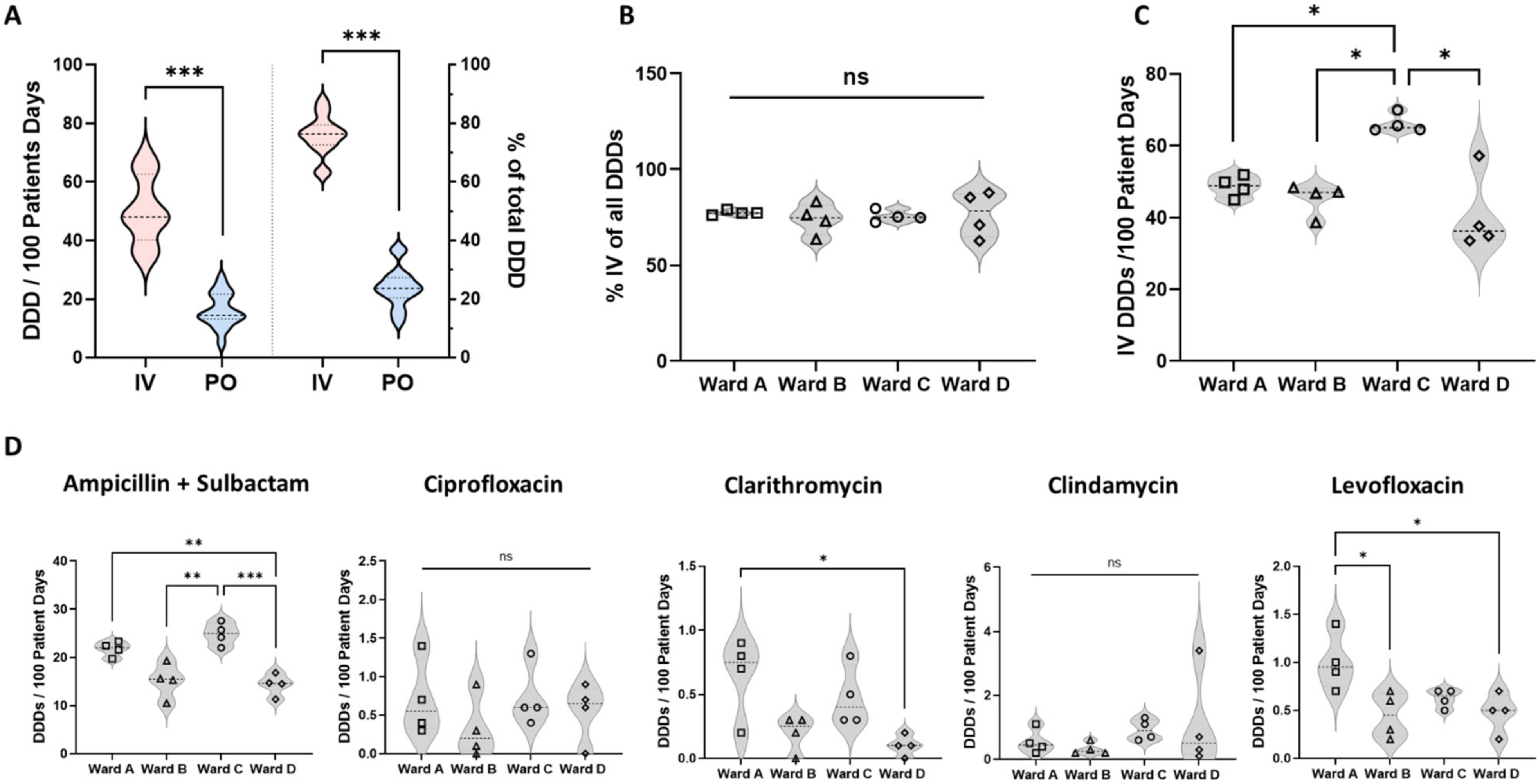
2.1.2. Identification of Excessive Iv Administration Reflecting Low Iv to Po Conversion Rates as Target for an ABS Intervention
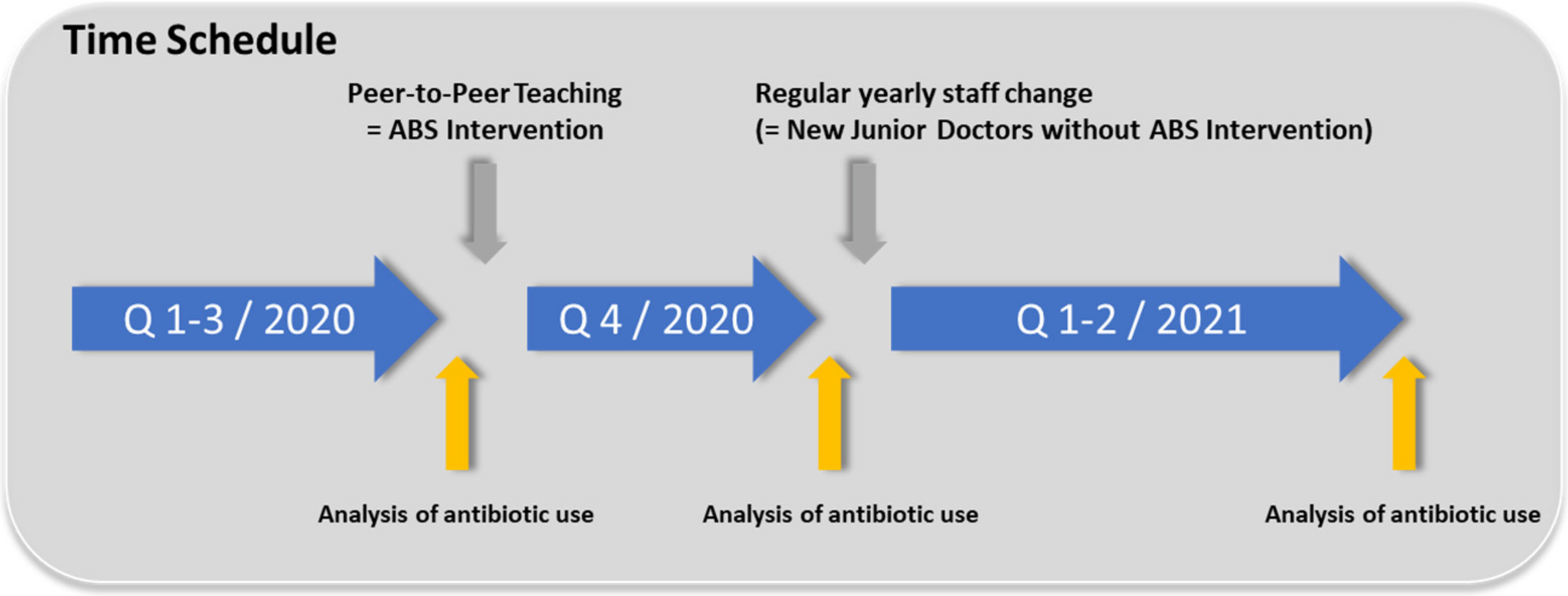
2.2. Step 2: Do: Design and Implementation of a Single Quick and Simple Peer-to-Peer Teaching Session to Foster Iv to Po Conversion
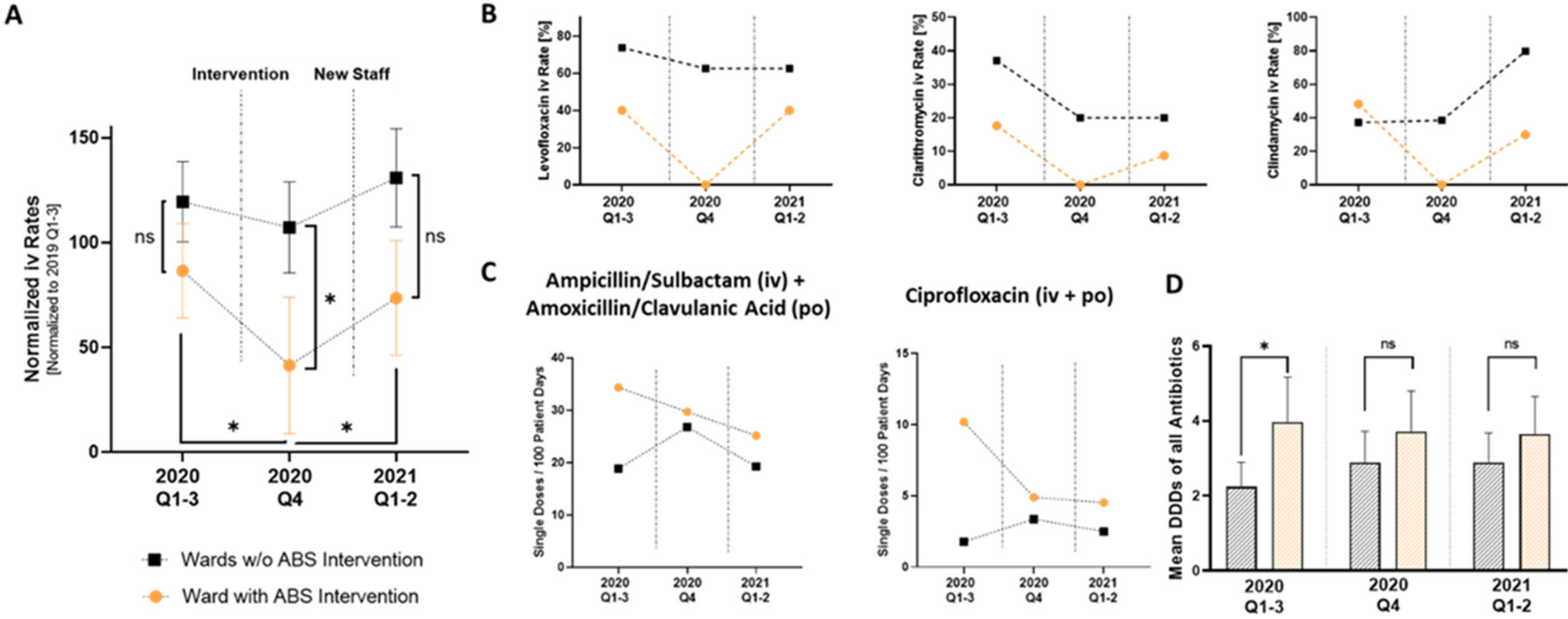
2.3. Step 3: Check: Antibiotic Use Metrics Prove Significant Reduction in Iv Antibiotic Administration after Peer-to-Peer Teaching
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Study Design and Data Source
5.2. Measures of Antibiotic Use
5.3. Design and Execution of the Peer-to-Peer Teaching ABS Intervention
5.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goff, D.A. Antimicrobial stewardship: Bridging the gap between quality care and cost. Curr. Opin. Infect. Dis. 2011, 24, S11–S20. [Google Scholar] [CrossRef]
- Van Duijn, P.J.; Dautzenberg, M.J.; Oostdijk, E.A. Recent trends in antibiotic resistance in European ICUs. Curr. Opin. Crit. Care 2011, 17, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Marston, H.D.; Dixon, D.M.; Knisely, J.M.; Palmore, T.N.; Fauci, A.S. Antimicrobial Resistance. JAMA J. Am. Med. Assoc. 2016, 316, 1193–1204. [Google Scholar] [CrossRef] [Green Version]
- Friedman, N.; Temkin, E.; Carmeli, Y. The negative impact of antibiotic resistance. Clin. Microbiol. Infect. 2016, 22, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Scheckler, W.E.; Bennett, J.V. Antibiotic usage in seven community hospitals. JAMA J. Am. Med. Assoc. 1970, 213, 264–267. [Google Scholar] [CrossRef]
- Neidell, M.J.; Cohen, B.; Furuya, Y.; Hill, J.; Jeon, C.Y.; Glied, S.; Larson, E.L. Costs of Healthcare- and Community-Associated Infections with Antimicrobial-Resistant Versus Antimicrobial-Susceptible Organisms. Clin. Infect. Dis. 2012, 55, 807–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantón, R.; Gijón, D.; Ruiz-Garbajosa, P. Antimicrobial resistance in ICUs: An update in the light of the COVID-19 pandemic. Curr. Opin. Crit. Care 2020, 26, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Gerding, D.N. The Search for Good Antimicrobial Stewardship. Jt. Comm. J. Qual. Improv. 2001, 27, 403–404. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Antimicrobial Stewardship Interventions; A Practical Guide; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Resman, F. Antimicrobial stewardship programs; a two-part narrative review of step-wise design and issues of controversy Part I: Step-wise design of an antimicrobial stewardship program. Ther. Adv. Infect. Dis. 2020, 7, 2049936120933187. [Google Scholar] [CrossRef] [PubMed]
- Santarossa, M.; Kilber, E.N.; Wenzler, E.; Albarillo, F.S.; Sterk, E.J. BundlED Up: A Narrative Review of Antimicrobial Stewardship Initiatives and Bundles in the Emergency Department. Pharmacy 2019, 7, 145. [Google Scholar] [CrossRef] [Green Version]
- Berman, L.; Raval, M.V.; Goldin, A. Process improvement strategies: Designing and implementing quality improvement research. Semin. Pediatr. Surg. 2018, 27, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Qiu, H.; Du, W. Evaluation of the Effect of PDCA in Hospital Health Management. J. Health Eng. 2021, 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, V.A.; Van Werkhoven, C.H.; Baño, J.R.; Bielicki, J.; Harbarth, S.; Hulscher, M.; Huttner, B.; Islam, J.; Little, P.; Pulcini, C.; et al. Optimizing design of research to evaluate antibiotic stewardship interventions: Consensus recommendations of a multinational working group. Clin. Microbiol. Infect. 2020, 26, 41–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.Y.; Bradley, N. A Peer Educational Tool to Promote Antimicrobial Stewardship on a University Campus. Pharmacy 2021, 9, 199. [Google Scholar] [CrossRef]
- Satterfield, J.; Miesner, A.; Percival, K. The role of education in antimicrobial stewardship. J. Hosp. Infect. 2020, 105, 130–141. [Google Scholar] [CrossRef]
- Kern, W.V.; Fellhauer, M.; Hug, M.; Hoppe-Tichy, T.; Forst, G.; Steib-Bauert, M.; De With, K. Antibiotika-Anwendung 2012/13 in 109 deutschen Akutkrankenhäusern. DMW Dtsch. Med. Wochenschr. 2015, 140, e237–e246. [Google Scholar] [CrossRef] [Green Version]
- Dalhoff, K.; Abele-Horn, M.; Andreas, S.; Deja, M.; Ewig, S.; Gastmeier, P.; Gatermann, S.; Gerlach, H.; Grabein, B.; Heußel, C.P.; et al. Epidemiologie, Diagnostik und Therapie erwachsener Patienten mit nosokomialer Pneumonie—Update 2017. Pneumologie 2018, 72, 15–63. [Google Scholar] [CrossRef]
- Przybylski, K.G.; Rybak, M.J.; Martin, P.R.; Weingarten, C.M.; Zaran, F.K.; Stevenson, J.G.; Levine, D.P. A pharmacist-initiated program of intravenous to oral antibiotic conversion. Pharmacother. J. Hum. Pharmacol. Drug Ther. 1997, 17, 271–276. [Google Scholar]
- Mok, M.; Kinkade, A.; Tung, A.; Tejani, A.M. Identification of Patients Eligible for IV-to-PO Conversion: A Cost-Minimization Study. Can. J. Hosp. Pharm. 2016, 69, 301–305. [Google Scholar] [CrossRef] [Green Version]
- Van den Bosch, C.M.A.; Hulscher, M.E.J.L.; Akkermans, R.P.; Wille, J.; Geerlings, S.E.; Prins, J.M. Appropriate antibiotic use reduces length of hospital stay. J. Antimicrob. Chemother. 2017, 72, 923–932. [Google Scholar] [CrossRef]
- Wilf-Miron, R.; Ron, N.; Ishai, S.; Chory, H.; Abboud, L.; Peled, R. Reducing the Volume of Antibiotic Prescriptions: A Peer Group Intervention Among Physicians Serving a Community with Special Ethnic Characteristics. J. Manag. Care Pharm. 2012, 18, 324–328. [Google Scholar] [CrossRef] [Green Version]
- Regev-Yochay, G.; Raz, M.; Dagan, R.; Roizin, H.; Morag, B.; Hetman, S.; Ringel, S.; Ben-Israel, N.; Varon, M.; Somekh, E.; et al. Reduction in Antibiotic Use Following a Cluster Randomized Controlled Multifaceted Intervention: The Israeli Judicious Antibiotic Prescription Study. Clin. Infect. Dis. 2011, 53, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Pronovost, P.; Needham, D.; Berenholtz, S.; Sinopoli, D.; Chu, H.; Cosgrove, S.; Sexton, B.; Hyzy, R.; Welsh, R.; Roth, G.; et al. An Intervention to Decrease Catheter-Related Bloodstream Infections in the ICU. N. Engl. J. Med. 2006, 355, 2725–2732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, M.J.; McNicholas, C.; Nicolay, C.; Darzi, A.; Bell, D.; Reed, J.E. Systematic review of the application of the plan–do–study—Act method to improve quality in healthcare. BMJ Qual. Saf. 2013, 23, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Brotherton, A.L. Metrics of Antimicrobial Stewardship Programs. Med. Clin. N. Am. 2018, 102, 965–976. [Google Scholar] [CrossRef] [PubMed]
- De With, K.; Bergner, J.; Bühner, R.; Dörje, F.; Gonnermann, C.; Haber, M.; Hartmann, M.; Rothe, U.; Strehl, E.; Steib-Bauert, M.; et al. Antibiotikaanwendung an deutschen Hochschulkliniken (Projekt INTERUNI-II). Med. Klin. 2004, 99, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Eber, M.R.; Laxminarayan, R.; Perencevich, E.N.; Malani, A. Clinical and Economic Outcomes Attributable to Health Care—Associated Sepsis and Pneumonia. Arch. Intern. Med. 2010, 170, 347–353. [Google Scholar] [CrossRef] [Green Version]
- Ewig, S.; Kolditz, M.; Pletz, M.; Altiner, A.; Albrich, W.; Drömann, D.; Flick, H.; Gatermann, S.; Krüger, S.; Nehls, W.; et al. Behandlung von erwachsenen Patienten mit ambulant erworbener Pneumonie—Update 2021. Pneumologie 2021, 75, 665–729. [Google Scholar] [CrossRef]
- Fischer, M.A.; Solomon, D.H.; Teich, J.M.; Avorn, J. Conversion from Intravenous to Oral Medications: Assessment of a computerized intervention for hospitalized patients. Arch. Intern. Med. 2003, 163, 2585–2589. [Google Scholar] [CrossRef] [Green Version]
- Thompson, C.; Zahradnik, M.; Brown, A.; Fleming, D.G.; Law, M. The use of an IV to PO clinical intervention form to improve antibiotic administration in a community based hospital. BMJ Qual. Improv. Rep. 2015, 4, u200786–w2247. [Google Scholar] [CrossRef]
- Ilges, D.; Ritchie, D.J.; Krekel, T.; Neuner, E.A.; Hampton, N.; Kollef, M.H.; Micek, S. Assessment of Antibiotic De-escalation by Spectrum Score in Patients with Nosocomial Pneumonia: A Single-Center, Retrospective Cohort Study. Open Forum Infect. Dis. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, J.A.; Srinath, L.; Ahkee, S.; Huang, A.; Raff, M.J. Early Switch from Intravenous to Oral Cephalosporins in the Treatment of Hospitalized Patients with Community-Acquired Pneumonia. Arch. Intern. Med. 1995, 155, 1273. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, J.; Vargas, S.; Ritter, G.W.; Brier, M.E.; Wright, A.; Smith, S.; Newman, D.; Burke, J.; Mushtaq, M.; Huang, A. Early Switch from Intravenous to Oral Antibiotics and Early Hospital Discharge: A prospective observational study of 200 consecutive patients with community-acquired pneumonia. Arch. Intern. Med. 1999, 159, 2449–2454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohan, J.; Remington, R.; Jones, M.; Samore, M.; Madaras-Kelly, K. Outcomes Associated with Antimicrobial De-escalation of Treatment for Pneumonia Within the Veterans Healthcare Administration. Open Forum Infect. Dis. 2017, 4, ofw244. [Google Scholar] [CrossRef] [Green Version]
- Lau, B.D.; Pinto, B.L.; Thiemann, D.R.; Lehmann, C.U. Budget Impact Analysis of Conversion from Intravenous to Oral Medication When Clinically Eligible for Oral Intake. Clin. Ther. 2011, 33, 1792–1796. [Google Scholar] [CrossRef]
- Sallach-Ruma, R.; Nieman, J.; Sankaranarayanan, J.; Reardon, T. Correlates and Economic and Clinical Outcomes of an Adult IV to PO Antimicrobial Conversion Program at an Academic Medical Center in Midwest United States. J. Pharm. Pr. 2015, 28, 238–248. [Google Scholar] [CrossRef]
- Huang, C. The COVID-19 Pandemic and the Incidence of the Non-COVID-19 Pneumonia in Adults. Front. Med. 2021, 8. [Google Scholar] [CrossRef]
- Stamm, P.; Sagoschen, I.; Weise, K.; Plachter, B.; Münzel, T.; Gori, T.; Vosseler, M. Influenza and RSV incidence during COVID-19 pandemic—an observational study from in-hospital point-of-care testing. Med. Microbiol. Immunol. 2021, 210, 277–282. [Google Scholar] [CrossRef]
- Nef, H.M.; Elsässer, A.; Möllmann, H.; Abdel-Hadi, M.; Bauer, T.; Brück, M.; Eggebrecht, H.; Ehrlich, J.R.; Ferrari, M.W.; Fichtlscherer, S. Impact of the COVID-19 pandemic on cardiovascular mortality and catherization activity during the lockdown in central Germany: An observational study. Clin. Res. Cardiol. 2021, 110, 292–301. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wild, J.; Siegrist, B.; Hobohm, L.; Münzel, T.; Schwanz, T.; Sagoschen, I. Short and Concise Peer-to-Peer Teaching—Example of a Successful Antibiotic Stewardship Intervention to Increase Iv to Po Conversion. Antibiotics 2022, 11, 402. https://doi.org/10.3390/antibiotics11030402
Wild J, Siegrist B, Hobohm L, Münzel T, Schwanz T, Sagoschen I. Short and Concise Peer-to-Peer Teaching—Example of a Successful Antibiotic Stewardship Intervention to Increase Iv to Po Conversion. Antibiotics. 2022; 11(3):402. https://doi.org/10.3390/antibiotics11030402
Chicago/Turabian StyleWild, Johannes, Bettina Siegrist, Lukas Hobohm, Thomas Münzel, Thomas Schwanz, and Ingo Sagoschen. 2022. "Short and Concise Peer-to-Peer Teaching—Example of a Successful Antibiotic Stewardship Intervention to Increase Iv to Po Conversion" Antibiotics 11, no. 3: 402. https://doi.org/10.3390/antibiotics11030402
APA StyleWild, J., Siegrist, B., Hobohm, L., Münzel, T., Schwanz, T., & Sagoschen, I. (2022). Short and Concise Peer-to-Peer Teaching—Example of a Successful Antibiotic Stewardship Intervention to Increase Iv to Po Conversion. Antibiotics, 11(3), 402. https://doi.org/10.3390/antibiotics11030402