

SER-109: An Oral Investigational Microbiome Therapeutic for Patients with Recurrent Clostridioides difficile Infection (rCDI)

 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
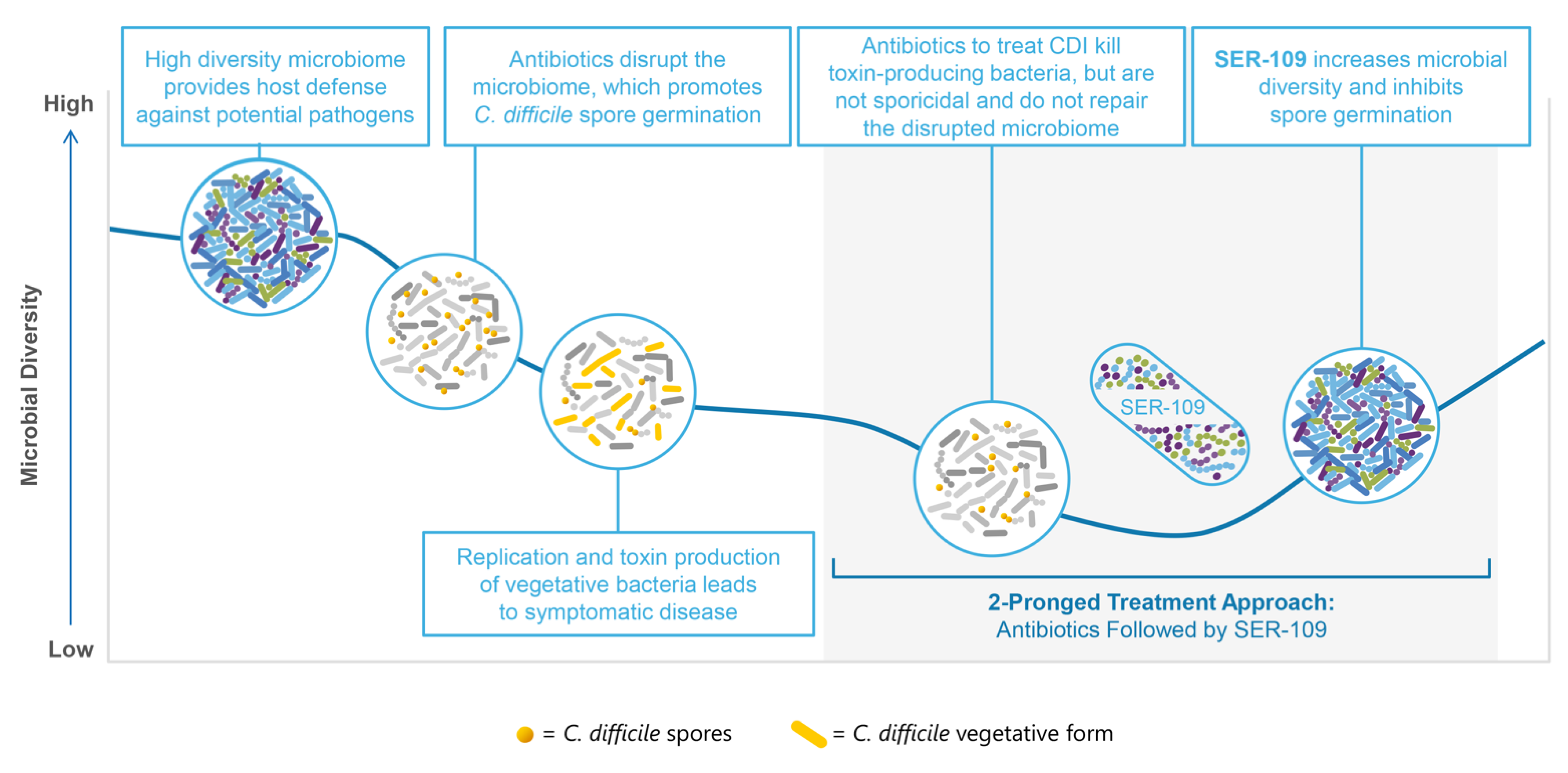
1.1. Role of the Microbiome in Recurrent CDI
1.2. Current Therapies Do Not Address the Disrupted Microbiome
1.3. Fecal Microbiota Transplantation Provides Proof of Concept of the Importance of Microbiome Repair
1.4. Safety Concerns Persist Regarding the Use of Fecal Microbiota Transplant
2. SER-109
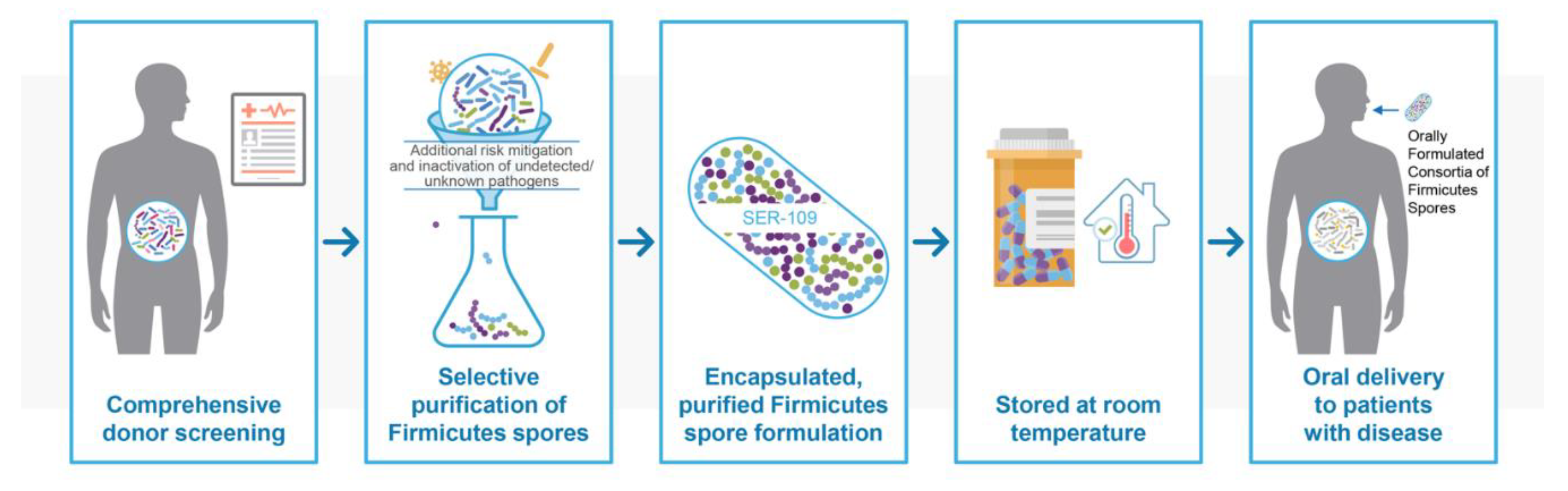
2.1. Manufacturing and Characterization of SER-109
2.2. Efficacy and Safety
2.3. Safety Profile
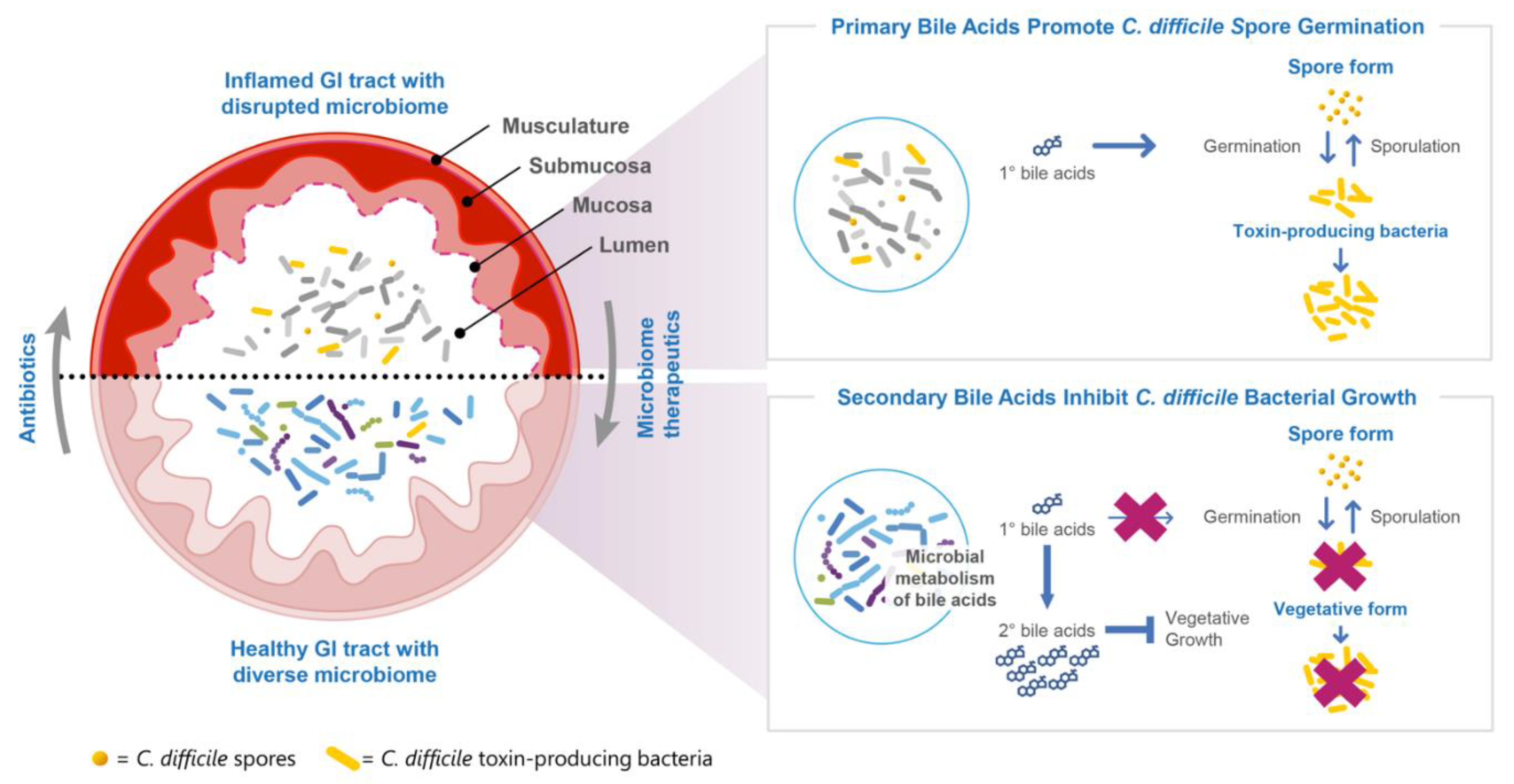
2.4. Pharmacology of SER-109
2.4.1. Race to Microbiome Repair to Achieve a Sustained Clinical Response
2.4.2. SER-109 Engraftment Drives Microbe-Associated Metabolite Changes, a Measure of the Pharmacodynamics of SER-109
2.5. Additional Potential Benefits of Restructuring the Gastrointestinal Microbiome
3. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- CDC. Antibiotic Resistance Threats in the United States; Department of Health and Human Services, CDC: Atlanta, GA, USA, 2019. Available online: www.cdc.gov/DrugResistance/Biggest-Threats.html (accessed on 27 July 2022).
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J.; et al. Multistate Point-Prevalence Survey of Health Care—Associated Infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef]
- Kwon, J.H.; Olsen, M.A.; Dubberke, E.R. The Morbidity, Mortality, and Costs Associated with Clostridium Difficile Infection. Infect. Dis. Clin. 2015, 29, 123–134. [Google Scholar] [CrossRef]
- UK Health Security Agency. Thirty-Day All-Cause Mortality Following MRSA, MSSA and Gram-Negative Bacteraemia and C. Difficile Infections, 2020 to 2021; UK Health Security Agency: London, UK, 2021. [Google Scholar]
- Guh, A.Y.; Mu, Y.; Winston, L.G.; Johnston, H.; Olson, D.; Farley, M.M.; Wilson, L.E.; Holzbauer, S.M.; Phipps, E.C.; Dumyati, G.K.; et al. Trends in U.S. Burden of Clostridioides Difficile Infection and Outcomes. N. Engl. J. Med. 2020, 382, 1320–1330. [Google Scholar] [CrossRef]
- Zhang, D.; Prabhu, V.S.; Marcella, S.W. Attributable Healthcare Resource Utilization and Costs for Patients with Primary and Recurrent Clostridium Difficile Infection in the United States. Clin. Infect. Dis. 2018, 66, 1326–1332. [Google Scholar] [CrossRef]
- McGovern, B.H.; Ford, C.B.; Henn, M.R.; Pardi, D.S.; Khanna, S.; Hohmann, E.L.; O’Brien, E.J.; Desjardins, C.A.; Bernardo, P.; Wortman, J.R.; et al. SER-109, an Investigational Microbiome Drug to Reduce Recurrence after Clostridioides Difficile Infection: Lessons Learned from a Phase 2 Trial. Clin. Infect. Dis. 2020, 72, 2132–2140. [Google Scholar] [CrossRef]
- Feuerstadt, P.; Louie, T.J.; Lashner, B.; Wang, E.E.L.; Diao, L.; Bryant, J.A.; Sims, M.; Kraft, C.S.; Cohen, S.H.; Berenson, C.S.; et al. SER-109, an Oral Microbiome Therapy for Recurrent Clostridioides Difficile Infection. N. Engl. J. Med. 2022, 386, 220–229. [Google Scholar] [CrossRef]
- Theriot, C.M.; Young, V.B. Interactions between the Gastrointestinal Microbiome and Clostridium Difficile. Annu. Rev. Microbiol. 2015, 69, 445–461. [Google Scholar] [CrossRef]
- Ianiro, G.; Tilg, H.; Gasbarrini, A. Antibiotics as Deep Modulators of Gut Microbiota: Between Good and Evil. Gut 2016, 65, 1906. [Google Scholar] [CrossRef]
- Lessa, F.C.; Mu, Y.; Bamberg, W.M.; Beldavs, Z.G.; Dumyati, G.K.; Dunn, J.R.; Farley, M.M.; Holzbauer, S.M.; Meek, J.I.; Phipps, E.C.; et al. Burden of Clostridium Difficile Infection in the United States. N. Engl. J. Med. 2015, 372, 825–834. [Google Scholar] [CrossRef]
- Freedberg, D.E.; Abrams, J.A. Does Confounding Explain the Association Between PPIs and Clostridium Difficile -Related Diarrhea? Am. J. Gastroenterol. 2013, 108, 278–279. [Google Scholar] [CrossRef]
- Garey, K.W.; Sethi, S.; Yadav, Y.; DuPont, H.L. Meta-Analysis to Assess Risk Factors for Recurrent Clostridium Difficile Infection. J. Hosp. Infect. 2008, 70, 298–304. [Google Scholar] [CrossRef]
- Deshpande, A.; Pasupuleti, V.; Thota, P.; Pant, C.; Rolston, D.D.K.; Hernandez, A.V.; Donskey, C.J.; Fraser, T.G. Risk Factors for Recurrent Clostridium Difficile Infection: A Systematic Review and Meta-Analysis. Infect. Control Hosp. Epidemiol. 2015, 36, 452–460. [Google Scholar] [CrossRef]
- Gerding, D.N.; Kelly, C.P.; Rahav, G.; Lee, C.; Dubberke, E.R.; Kumar, P.N.; Yacyshyn, B.; Kao, D.; Eves, K.; Ellison, M.C.; et al. Bezlotoxumab for Prevention of Recurrent Clostridium Difficile Infection in Patients at Increased Risk for Recurrence. Clin. Infect. Dis. 2018, 67, 649–656. [Google Scholar] [CrossRef]
- Allegretti, J.R.; Kearney, S.; Li, N.; Bogart, E.; Bullock, K.; Gerber, G.K.; Bry, L.; Clish, C.B.; Alm, E.; Korzenik, J.R. Recurrent Clostridium Difficile Infection Associates with Distinct Bile Acid and Microbiome Profiles. Aliment. Pharm. Therap. 2016, 43, 1142–1153. [Google Scholar] [CrossRef]
- Crobach, M.J.T.; Vernon, J.J.; Loo, V.G.; Kong, L.Y.; Péchiné, S.; Wilcox, M.H.; Kuijper, E.J. Understanding Clostridium Difficile Colonization. Clin. Microbiol. Rev. 2018, 31, e00021-17. [Google Scholar] [CrossRef]
- Smits, W.K.; Lyras, D.; Lacy, D.B.; Wilcox, M.H.; Kuijper, E.J. Clostridium Difficile Infection. Nat. Rev. Dis. Primers 2016, 2, 16020. [Google Scholar] [CrossRef]
- Thorpe, C.M.; Kane, A.V.; Chang, J.; Tai, A.; Vickers, R.J.; Snydman, D.R. Enhanced Preservation of the Human Intestinal Microbiota by Ridinilazole, a Novel Clostridium Difficile-Targeting Antibacterial, Compared to Vancomycin. PLoS ONE 2018, 13, e0199810. [Google Scholar] [CrossRef]
- Louie, T.J.; Miller, M.A.; Mullane, K.M.; Weiss, K.; Lentnek, A.; Golan, Y.; Gorbach, S.; Sears, P.; Shue, Y.-K.; Group, O.-. 80-003 C.S. Fidaxomicin versus Vancomycin for Clostridium Difficile Infection. N. Engl. J. Med. 2011, 364, 422–431. [Google Scholar] [CrossRef]
- Cornely, O.A.; Miller, M.A.; Louie, T.J.; Crook, D.W.; Gorbach, S.L. Treatment of First Recurrence of Clostridium Difficile Infection: Fidaxomicin versus Vancomycin. Clin. Infect. Dis. 2012, 55, S154–S161. [Google Scholar] [CrossRef]
- Dubberke, E.R.; Lee, C.H.; Orenstein, R.; Khanna, S.; Hecht, G.; Gerding, D.N. Results From a Randomized, Placebo-Controlled Clinical Trial of a RBX2660—A Microbiota-Based Drug for the Prevention of Recurrent Clostridium Difficile Infection. Clin. Infect. Dis. 2018, 67, 1198–1204. [Google Scholar] [CrossRef] [Green Version]
- Kelly, C.P. Can We Identify Patients at High Risk of Recurrent Clostridium Difficile Infection? Clin. Microbiol. Infect. 2012, 18, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Madoff, S.E.; Urquiaga, M.; Alonso, C.D.; Kelly, C.P. Prevention of Recurrent Clostridioides Difficile Infection: A Systematic Review of Randomized Controlled Trials. Anaerobe 2020, 61, 102098. [Google Scholar] [CrossRef] [PubMed]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical Practice Guidelines for Clostridium Difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin. Infect. Dis. 2018, 66, e1–e48. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, M.H.; McGovern, B.H.; Hecht, G.A. The Efficacy and Safety of Fecal Microbiota Transplant for Recurrent Clostridium Difficile Infection: Current Understanding and Gap Analysis. In Open Forum Infectious Diseases; Oxford University Press: Oxford, MI, USA, 2020; Volume 7, p. ofaa114. [Google Scholar] [CrossRef]
- Smith, M.B.; Kelly, C.; Alm, E.J. Policy: How to Regulate Faecal Transplants. Nature 2014, 506, 290–291. [Google Scholar] [CrossRef] [PubMed]
- Staley, C.; Kelly, C.R.; Brandt, L.J.; Khoruts, A.; Sadowsky, M.J. Complete Microbiota Engraftment Is Not Essential for Recovery from Recurrent Clostridium Difficile Infection Following Fecal Microbiota Transplantation. Mbio 2016, 7, e01965-16. [Google Scholar] [CrossRef]
- Jiang, Z.D.; Ajami, N.J.; Petrosino, J.F.; Jun, G.; Hanis, C.L.; Shah, M.; Hochman, L.; Ankoma-Sey, V.; DuPont, A.W.; Wong, M.C.; et al. Randomised Clinical Trial: Faecal Microbiota Transplantation for Recurrent Clostridum Difficile Infection—Fresh, or Frozen, or Lyophilised Microbiota from a Small Pool of Healthy Donors Delivered by Colonoscopy. Aliment. Pharm. Therap. 2017, 45, 899–908. [Google Scholar] [CrossRef]
- Blount, K.F.; Shannon, W.D.; Deych, E.; Jones, C. Restoration of Bacterial Microbiome Composition and Diversity among Treatment Responders in a Phase 2 Trial of RBX2660: An Investigational Microbiome Restoration Therapeutic. In Open Forum Infectious Diseases; Oxford University Press: Oxford, MI, USA, 2019; Volume 6, p. ofz095. [Google Scholar] [CrossRef]
- Van Nood, E.; Vrieze, A.; Nieuwdorp, M.; Fuentes, S.; Zoetendal, E.G.; de Vos, W.M.; Visser, C.E.; Kuijper, E.J.; Bartelsman, J.F.W.M.; Tijssen, J.G.P.; et al. Duodenal Infusion of Donor Feces for Recurrent Clostridium Difficile. N. Engl. J. Med. 2013, 368, 407–415. [Google Scholar] [CrossRef]
- Millan, B.; Park, H.; Hotte, N.; Mathieu, O.; Burguiere, P.; Tompkins, T.A.; Kao, D.; Madsen, K.L. Fecal Microbial Transplants Reduce Antibiotic-Resistant Genes in Patients With Recurrent Clostridium Difficile Infection. Clin. Infect. Dis. 2016, 62, 1479–1486. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Z.-D.; Jenq, R.R.; Ajami, N.J.; Petrosino, J.F.; Alexander, A.A.; Ke, S.; Iqbal, T.; DuPont, A.W.; Muldrew, K.; Shi, Y.; et al. Safety and Preliminary Efficacy of Orally Administered Lyophilized Fecal Microbiota Product Compared with Frozen Product given by Enema for Recurrent Clostridium Difficile Infection: A Randomized Clinical Trial. PLoS ONE 2018, 13, e0205064. [Google Scholar] [CrossRef]
- Shahinas, D.; Silverman, M.; Sittler, T.; Chiu, C.; Kim, P.; Allen-Vercoe, E.; Weese, S.; Wong, A.; Low, D.E.; Pillai, D.R. Toward an Understanding of Changes in Diversity Associated with Fecal Microbiome Transplantation Based on 16S RRNA Gene Deep Sequencing. Mbio 2012, 3, e00338-12. [Google Scholar] [CrossRef]
- Tariq, R.; Pardi, D.S.; Bartlett, M.G.; Khanna, S. Low Cure Rates in Controlled Trials of Fecal Microbiota Transplantation for Recurrent Clostridium Difficile Infection: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2018, 68, 1351–1358. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.; Lavergne, V.; Skinner, A.M.; Gonzales-Luna, A.J.; Garey, K.W.; Kelly, C.P.; Wilcox, M.H. Clinical Practice Guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 Focused Update Guidelines on Management of Clostridioides Difficile Infection in Adults. Clin. Infect. Dis. 2021, 73, ciab549. [Google Scholar] [CrossRef] [PubMed]
- Bafeta, A.; Yavchitz, A.; Riveros, C.; Batista, R.; Ravaud, P. Methods and Reporting Studies Assessing Fecal Microbiota Transplantation: A Systematic Review. Ann. Intern. Med. 2017, 167, 34. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug Administration. Safety Alert Regarding Use of Fecal Microbiota for Transplantation and Risk of Serious Adverse Events Likely Due to Transmission of Pathogenic Organisms. 2020. Available online: https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/safety-alert-regarding-use-fecal-microbiota-transplantation-and-risk-serious-adverse-events-likely (accessed on 27 July 2022).
- US Food and Drug Administration. Important Safety Alert Regarding Use of Fecal Microbiota for Transplantation and Risk of Serious Adverse Reactions Due to Transmission of Multi-Drug Resistant Organisms. 2019. Available online: https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/important-safety-alert-regarding-use-fecal-microbiota-transplantation-and-risk-serious-adverse (accessed on 27 July 2022).
- DeFilipp, Z.; Bloom, P.P.; Soto, M.T.; Mansour, M.K.; Sater, M.R.A.; Huntley, M.H.; Turbett, S.; Chung, R.T.; Chen, Y.-B.; Hohmann, E.L. Drug-Resistant E. Coli Bacteremia Transmitted by Fecal Microbiota Transplant. N. Engl. J. Med. 2019, 381, 2043–2050. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug Administration. Information Pertaining to Additional Safety Protections Regarding Use of Fecal Microbiota for Transplantation—Screening Donors for COVID-19 and Exposure to SARS-CoV-2 and Testing for SARS-CoV-2. 2020. Available online: https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/information-pertaining-additional-safety-protections-regarding-use-fecal-microbiota-transplantation-1 (accessed on 27 July 2022).
- Blaser, M.J. Fecal Microbiota Transplantation for Dysbiosis—Predictable Risks. N. Engl. J. Med. 2019, 381, 2064–2066. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Safety Alert Regarding Use of Fecal Microbiota for Transplantation and Additional Safety Protections Pertaining to SARS-CoV-2 and COVID-19. 2020. Available online: https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/safety-alert-regarding-use-fecal-microbiota-transplantation-and-additional-safety-protections (accessed on 27 July 2022).
- Guo, M.; Tao, W.; Flavell, R.A.; Zhu, S. Potential Intestinal Infection and Faecal–Oral Transmission of SARS-CoV-2. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 269–283. [Google Scholar] [CrossRef]
- Zhang, Y.; Cen, M.; Hu, M.; Du, L.; Hu, W.; Kim, J.J.; Dai, N. Prevalence and Persistent Shedding of Fecal SARS-CoV-2 RNA in Patients With COVID-19 Infection: A Systematic Review and Meta-Analysis. Clin. Transl. Gastroenterol. 2021, 12, e00343. [Google Scholar] [CrossRef]
- Coryell, M.P.; Iakiviak, M.; Pereira, N.; Murugkar, P.P.; Rippe, J.; Williams, D.B.; Heald-Sargent, T.; Sanchez-Pinto, L.N.; Chavez, J.; Hastie, J.L.; et al. A Method for Detection of SARS-CoV-2 RNA in Healthy Human Stool: A Validation Study. Lancet Microbe 2021, 2, e259–e266. [Google Scholar] [CrossRef]
- Baker, J.M.; Buchfellner, M.; Britt, W.; Sanchez, V.; Potter, J.L.; Ingram, L.A.; Shiau, H.; Sanchez, L.H.G.; Saaybi, S.; Kelly, D.; et al. Acute Hepatitis and Adenovirus Infection Among Children—Alabama, October 2021–February 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 638–640. [Google Scholar] [CrossRef]
- Khanna, S.; Pardi, D.S.; Kelly, C.R.; Kraft, C.S.; Dhere, T.; Henn, M.R.; Lombardo, M.-J.; Vulic, M.; Ohsumi, T.; Winkler, J.; et al. A Novel Microbiome Therapeutic Increases Gut Microbial Diversity and Prevents Recurrent Clostridium Difficile Infection. J. Infect. Dis. 2016, 214, 173–181. [Google Scholar] [CrossRef]
- Louie, T.J.; Sims, M.; Nathan, R.; O’Marro, S.; Kumar, P.N.; Wang, E.E.; Stevens, R.; Brady, K.; McGovern, B.; von Moltke, L. 639. Time to Recurrence of Clostridioides Difficile Infection (RCDI) Is Rapid Following Completion of Standard of Care Antibiotics: Results from ECOSPOR-III, a Phase 3 Double-Blind, Placebo-Controlled Randomized Trial of SER-109, an Investigational Microbiome Therapeutic. In Open Forum Infectious Diseases; Oxford University Press: Oxford, MI, USA, 2021; Volume 8, p. S422. [Google Scholar] [CrossRef]
- McGovern, B.H.; Louie, T.; Cohen, S.; Sims, M.; Wang, E.; Wu, H.; Brady, K.; von Moltke, L. Investigational Microbiome Therapeutic SER-109 Reduces Recurrence of Clostridioides DifficileInfection (CDI) Compared to Placebo, Regardless of Presence or Absence of Comorbidities Including Chronic Obstructive Disease (COPD) and Asthma. In B39. COPD Management: From Pharmacologic Treatment to Novel Therapies; American Thoracic Society: New York, NY, USA, 2022; p. A2792. [Google Scholar] [CrossRef]
- Paskovaty, A.; Berenson, C.S.; Louie, T.J.; Wang, E.; Lombardi, D.A.; Moltke, L. von Efficacy and Safety of SER-109, an Investigational Microbiome Therapeutic for Recurrent Clostridioides Difficile Infection: Data from ECOSPOR III, a Phase 3 Randomized Trial. J. Clin. Oncol. 2022, 40, 12113. [Google Scholar] [CrossRef]
- Cohen, S.H.; Louie, T.J.; Sims, M.; Pullman, J.; Wang, E.E.; Wu, H.; McGovern, B.; Brady, K.; von Moltke, L. 634. Investigational Microbiome Therapeutic SER-109 Reduces Recurrence of Clostridioides Difficile Infection (CDI) Compared to Placebo, Regardless of Risk Factors for Recurrence. In Open Forum Infectious Diseases; Oxford University Press: Oxford, MI, USA, 2021; Volume 8, p. S420. [Google Scholar] [CrossRef]
- Korman, L.; Lashner, B.; Feuerstadt, P.; Wang, E.; Wu, H.; Hampton, K.; Lawrence, K.; Brady, K.; von Moltke, L. Investigational Microbiome Therapeutic SER-109 Reduces the Risk of Recurrent Clostridioides Difficile Infection (RCDI) Compared to Placebo in Patients with Risk Factors for Recurrence, Including Acid-Reducing Medications (Late-Breaking Abstract); College of Gastroenterology: Bethesda, MD, USA, 26 October 2021. [Google Scholar]
- Wilcox, M.H.; Gerding, D.N.; Poxton, I.R.; Kelly, C.; Nathan, R.; Birch, T.; Cornely, O.A.; Rahav, G.; Bouza, E.; Lee, C.; et al. Bezlotoxumab for Prevention of Recurrent Clostridium Difficile Infection. N. Engl. J. Med. 2017, 376, 305–317. [Google Scholar] [CrossRef] [PubMed]
- Weiss, K.; Allgren, R.L.; Sellers, S. Safety Analysis of Fidaxomicin in Comparison With Oral Vancomycin for Clostridium Difficile Infections. Clin. Infect. Dis. 2012, 55, S110–S115. [Google Scholar] [CrossRef]
- Marcella, C.; Cui, B.; Kelly, C.R.; Ianiro, G.; Cammarota, G.; Zhang, F. Systematic Review: The Global Incidence of Faecal Microbiota Transplantation-related Adverse Events from 2000 to 2020. Aliment. Pharm. Therap. 2021, 53, 33–42. [Google Scholar] [CrossRef]
- Lee, C.H.; Steiner, T.; Petrof, E.O.; Smieja, M.; Roscoe, D.; Nematallah, A.; Weese, J.S.; Collins, S.; Moayyedi, P.; Crowther, M.; et al. Frozen vs Fresh Fecal Microbiota Transplantation and Clinical Resolution of Diarrhea in Patients With Recurrent Clostridium Difficile Infection: A Randomized Clinical Trial. JAMA 2016, 315, 142–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, T.-L.; Shu, C.-C.; Chen, Y.-M.; Lu, J.-J.; Wu, T.-S.; Lai, W.-F.; Tzeng, C.-M.; Lai, H.-C.; Lu, C.-C. Like Cures Like: Pharmacological Activity of Anti-Inflammatory Lipopolysaccharides from Gut Microbiome. Front. Pharmacol. 2020, 11, 554. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, F.A.; Koren, O.; Goodrich, J.K.; Johansson, M.E.V.; Nalbantoglu, I.; Aitken, J.D.; Su, Y.; Chassaing, B.; Walters, W.A.; González, A.; et al. Transient Inability to Manage Proteobacteria Promotes Chronic Gut Inflammation in TLR5-Deficient Mice. Cell Host Microbe 2012, 12, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Straub, T.J.; Diao, L.; Ford, C.; Sims, M.; Louie, T.J.; Berenson, C.; Kraft, C.S.; Cohen, S.H.; Paskovaty, A.; Lombardo, M.-J.; et al. LB15. SER-109, an Investigational Microbiome Therapeutic, Reduces Abundance of Antimicrobial Resistance Genes in Patients with Recurrent Clostridioides Difficile Infection (RCDI) after Standard-of-Care Antibiotics. In Open Forum Infectious Diseases; Oxford University Press: Oxford, MI, USA, 2021; Volume 8, pp. S812–S813. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khanna, S.; Sims, M.; Louie, T.J.; Fischer, M.; LaPlante, K.; Allegretti, J.; Hasson, B.R.; Fonte, A.T.; McChalicher, C.; Ege, D.S.; et al. SER-109: An Oral Investigational Microbiome Therapeutic for Patients with Recurrent Clostridioides difficile Infection (rCDI). Antibiotics 2022, 11, 1234. https://doi.org/10.3390/antibiotics11091234
Khanna S, Sims M, Louie TJ, Fischer M, LaPlante K, Allegretti J, Hasson BR, Fonte AT, McChalicher C, Ege DS, et al. SER-109: An Oral Investigational Microbiome Therapeutic for Patients with Recurrent Clostridioides difficile Infection (rCDI). Antibiotics. 2022; 11(9):1234. https://doi.org/10.3390/antibiotics11091234
Chicago/Turabian StyleKhanna, Sahil, Matthew Sims, Thomas J. Louie, Monika Fischer, Kerry LaPlante, Jessica Allegretti, Brooke R. Hasson, Allyson T. Fonte, Christopher McChalicher, David S. Ege, and et al. 2022. "SER-109: An Oral Investigational Microbiome Therapeutic for Patients with Recurrent Clostridioides difficile Infection (rCDI)" Antibiotics 11, no. 9: 1234. https://doi.org/10.3390/antibiotics11091234
APA StyleKhanna, S., Sims, M., Louie, T. J., Fischer, M., LaPlante, K., Allegretti, J., Hasson, B. R., Fonte, A. T., McChalicher, C., Ege, D. S., Bryant, J. A., Straub, T. J., Ford, C. B., Henn, M. R., Wang, E. E. L., von Moltke, L., & Wilcox, M. H. (2022). SER-109: An Oral Investigational Microbiome Therapeutic for Patients with Recurrent Clostridioides difficile Infection (rCDI). Antibiotics, 11(9), 1234. https://doi.org/10.3390/antibiotics11091234