Ceftazidime-Avibactam Combination Therapy Compared to Ceftazidime-Avibactam Monotherapy for the Treatment of Severe Infections Due to Carbapenem-Resistant Pathogens: A Systematic Review and Network Meta-Analysis

 ,
,  , ,
, , 

Abstract
:1. Introduction
2. Methods
2.1. Study Search
2.2. Study Selection
2.3. Definition and Outcome
2.4. Data Extraction and Quality Assessment
2.5. Data Analysis
3. Results
3.1. Study Selection and Characteristics
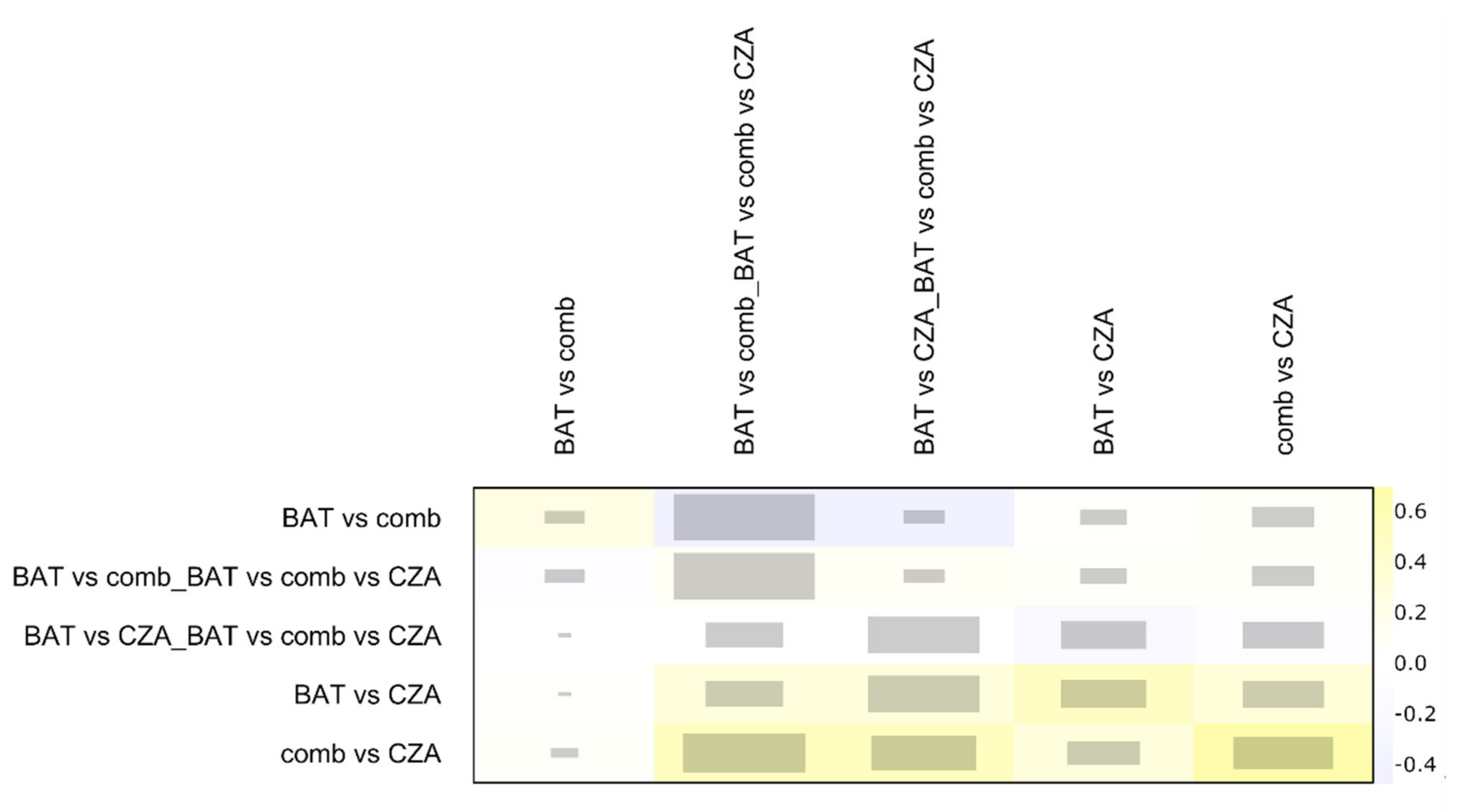
3.2. NMA Heterogeneity and Inconsistency Evaluation
3.3. Mortality
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shirley, M. Ceftazidime-Avibactam: A Review in the Treatment of Serious Gram-Negative Bacterial Infections. Drugs 2018, 78, 675–692. [Google Scholar] [CrossRef] [PubMed]
- (CDC), Centers for Disease Control and Prevention. Clinicians: Information about CRE. 2019. Available online: https://www.cdc.gov/hai/organisms/cre/cre-clinicians.html (accessed on 3 July 2020).
- Food and Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/206494Orig1s000SumR.pdf (accessed on 3 July 2020).
- European Medicines Agency. Available online: https://www.ema.europa.eu/en/documents/product-information/zavicefta-epar-product-information_en.pdf (accessed on 3 July 2020).
- Tumbarello, M.; Trecarichi, E.M.; Corona, A.; De Rosa, F.G.; Bassetti, M.; Mussini, C.; Menichetti, F.; Viscoli, C.; Campoli, C.; Venditti, M.; et al. Efficacy of Ceftazidime-Avibactam Salvage Therapy in Patients With Infections Caused by Klebsiella pneumoniae Carbapenemase-producing K. pneumoniae. Clin. Infect. Dis. 2019, 68, 355–364. [Google Scholar] [CrossRef] [Green Version]
- Castón, J.J.; Lacort-Peralta, I.; Martín-Dávila, P.; Loeches, B.; Tabares, S.; Temkin, L.; Torre-Cisneros, J.; Paño-Pardo, J.R. Clinical efficacy of ceftazidime/avibactam versus other active agents for the treatment of bacteremia due to carbapenemase-producing Enterobacteriaceae in hematologic patients. Int. J. Infect. Dis. 2017, 59, 118–123. [Google Scholar] [CrossRef] [Green Version]
- Shields, R.K.; Nguyen, M.H.; Chen, L.; Press, E.G.; Potoski, B.A.; Marini, R.V.; Doi, Y.; Kreiswirth, B.N.; Clancy, C.J. Ceftazidime-Avibactam Is Superior to Other Treatment Regimens against Carbapenem-Resistant Klebsiella pneumoniae Bacteremia. Antimicrob. Agents Chemother. 2017, 61, e00883-00817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa, A.; Perez-Rodriguez, M.T.; Soto, A.; Rodriguez, L.; Perez-Landeiro, A.; Martinez-Lamas, L.; Nodar, A.; Crespo, M. Effectiveness of ceftazidime/avibactam as salvage therapy for treatment of infections due to OXA-48 carbapenemase-producing Enterobacteriaceae. J. Antimicrob. Chemother. 2018, 73, 3170–3175. [Google Scholar] [CrossRef] [PubMed]
- Neupane, B.; Richer, D.; Bonner, A.J.; Kibret, T.; Beyene, J. Network meta-analysis using R: A review of currently available automated packages. PLoS ONE 2014, 9, e115065. [Google Scholar] [CrossRef] [Green Version]
- Correction: Network meta-analysis using R: A review of currently available automated packages. PLoS ONE 2015, 10, e0123364. [CrossRef]
- Fiore, M.; Cortegiani, A. Ceftazidime-avibactam combination therapy compared to Ceftazidime-avibactam monotherapy for the treatment of severe infections. 2019/04/16 ed. 2019. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42019128927 (accessed on 3 July 2020).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Data collection form for intervention reviews for RCTs and non-RCTs. Available online: https://dplp.cochrane.org/data-extraction-forms (accessed on 3 July 2020).
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011. [Google Scholar]
- Rücker, G.; Krahn, U.; König, J.; Efthimiou, O.; Schwarzer, G. Netmeta: Network Meta-Analysis using Frequentist Methods (R Package Version 0.9-8). Available online: https://cran.r-project.org/web/packages/netmeta/index.html (accessed on 3 July 2020).
- Konig, J.; Krahn, U.; Binder, H. Visualizing the flow of evidence in network meta-analysis and characterizing mixed treatment comparisons. Stat. Med. 2013, 32, 5414–5429. [Google Scholar] [CrossRef]
- Krahn, U.; Binder, H.; König, J. A graphical tool for locating inconsistency in network meta-analyses. BMC Med. Res. Methodol. 2013, 13, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carmeli, Y.; Armstrong, J.; Laud, P.J.; Newell, P.; Stone, G.; Wardman, A.; Gasink, L.B. Ceftazidime-avibactam or best available therapy in patients with ceftazidime-resistant Enterobacteriaceae and Pseudomonas aeruginosa complicated urinary tract infections or complicated intra-abdominal infections (REPRISE): A randomised, pathogen-directed, phase 3 study. Lancet Infect. Dis. 2016, 16, 661–673. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Zhong, N.; Pachl, J.; Timsit, J.F.; Kollef, M.; Chen, Z.; Song, J.; Taylor, D.; Laud, P.J.; Stone, G.G.; et al. Ceftazidime-avibactam versus meropenem in nosocomial pneumonia, including ventilator-associated pneumonia (REPROVE): A randomised, double-blind, phase 3 non-inferiority trial. Lancet Infect. Dis. 2018, 18, 285–295. [Google Scholar] [CrossRef] [Green Version]
- Lucasti, C.; Popescu, I.; Ramesh, M.K.; Lipka, J.; Sable, C. Comparative study of the efficacy and safety of ceftazidime/avibactam plus metronidazole versus meropenem in the treatment of complicated intra-abdominal infections in hospitalized adults: Results of a randomized, double-blind, Phase II trial. J. Antimicrob. Chemother. 2013, 68, 1183–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, X.; Tran, B.G.; Kim, M.J.; Wang, L.; Nguyen, D.A.; Chen, Q.; Song, J.; Laud, P.J.; Stone, G.G.; Chow, J.W. A randomised, double-blind, phase 3 study comparing the efficacy and safety of ceftazidime/avibactam plus metronidazole versus meropenem for complicated intra-abdominal infections in hospitalised adults in Asia. Int. J. Antimicrob. Agents 2017, 49, 579–588. [Google Scholar] [CrossRef]
- Mazuski, J.E.; Gasink, L.B.; Armstrong, J.; Broadhurst, H.; Stone, G.G.; Rank, D.; Llorens, L.; Newell, P.; Pachl, J. Efficacy and Safety of Ceftazidime-Avibactam Plus Metronidazole Versus Meropenem in the Treatment of Complicated Intra-abdominal Infection: Results From a Randomized, Controlled, Double-Blind, Phase 3 Program. Clin. Infect. Dis. 2016, 62, 1380–1389. [Google Scholar] [CrossRef] [PubMed]
- Vazquez, J.A.; Gonzalez Patzan, L.D.; Stricklin, D.; Duttaroy, D.D.; Kreidly, Z.; Lipka, J.; Sable, C. Efficacy and safety of ceftazidime-avibactam versus imipenem-cilastatin in the treatment of complicated urinary tract infections, including acute pyelonephritis, in hospitalized adults: Results of a prospective, investigator-blinded, randomized study. Curr. Med. Res. Opin. 2012, 28, 1921–1931. [Google Scholar] [CrossRef]
- Wagenlehner, F.M.; Sobel, J.D.; Newell, P.; Armstrong, J.; Huang, X.; Stone, G.G.; Yates, K.; Gasink, L.B. Ceftazidime-avibactam Versus Doripenem for the Treatment of Complicated Urinary Tract Infections, Including Acute Pyelonephritis: RECAPTURE, a Phase 3 Randomized Trial Program. Clin. Infect. Dis. 2016, 63, 754–762. [Google Scholar] [CrossRef] [Green Version]
- King, M.; Heil, E.; Kuriakose, S.; Bias, T.; Huang, V.; El-Beyrouty, C.; McCoy, D.; Hiles, J.; Richards, L.; Gardner, J.; et al. Multicenter Study of Outcomes with Ceftazidime-Avibactam in Patients with Carbapenem-Resistant Enterobacteriaceae Infections. Antimicrob. Agents Chemother. 2017, 61. [Google Scholar] [CrossRef] [Green Version]
- Alraddadi, B.M.; Saeedi, M.; Qutub, M.; Alshukairi, A.; Hassanien, A.; Wali, G. Efficacy of ceftazidime-avibactam in the treatment of infections due to Carbapenem-resistant Enterobacteriaceae. BMC Infect. Dis. 2019, 19, 772. [Google Scholar] [CrossRef] [Green Version]
- Octavia, S.; Lan, R. The Family Enterobacteriaceae. In The Prokaryotes: Gammaproteobacteria; Rosenberg, E., DeLong, E.F., Lory, S., Stackebrandt, E., Thompson, F., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 225–286. [Google Scholar]
- Schwarzer, G.; Carpenter, J.R.; Rücker, G. Meta-Analysis with R; Springer: Cham, Switzerland, 2015; pp. 187–216. [Google Scholar] [CrossRef]
- Plot for direct evidence proportions in a network meta-analysis using netmeta. Available online: https://dmetar.protectlab.org/reference/direct.evidence.plot.html (accessed on 3 July 2020).
- Iovene, M.R.; Pota, V.; Galdiero, M.; Corvino, G.; Di Lella, F.M.; Stelitano, D.; Passavanti, M.B.; Pace, M.C.; Alfieri, A.; Di Franco, S.; et al. First Italian outbreak of VIM-producing Serratia marcescens in an adult polyvalent intensive care unit, August-October 2018: A case report and literature review. World J. Clin. Cases 2019, 7, 3535–3548. [Google Scholar] [CrossRef]
- Park, Y.; Choi, Q.; Kwon, G.C.; Koo, S.H. Emergence and transmission of New Delhi metallo-beta-lactamase-5-producing Escherichia coli Sequence Type 361 in a Tertiary Hospital in South Korea. J. Clin. Lab. Anal. 2019, e23041. [Google Scholar] [CrossRef] [PubMed]
- Dubendris, H.; MacFarquhar, J.; Kornegay, R.; Gable, P.; Boyd, S.; Walters, M.; Greene, S. Imipenemase-producing carbapenem-resistant Enterobacteriaceae transmission in a long-term-care facility during a community-wide multidrug resistant organism outbreak-North Carolina, 2017. Am. J. Infect. Control 2019. [Google Scholar] [CrossRef] [PubMed]
- Cuzon, G.; Bentchouala, C.; Vogel, A.; Hery, M.; Lezzar, A.; Smati, F.; Dortet, L.; Naas, T. First outbreak of OXA-48-positive carbapenem-resistant Klebsiella pneumoniae isolates in Constantine, Algeria. Int. J. Antimicrob. Agents 2015, 46, 725–727. [Google Scholar] [CrossRef] [PubMed]
- Infectious Diseases Society of America; Spellberg, B.; Blaser, M.; Guidos, R.J.; Boucher, H.W.; Bradley, J.S.; Eisenstein, B.I.; Gerding, D.; Lynfield, R.; Reller, L.B.; et al. Combating antimicrobial resistance: Policy recommendations to save lives. Clin. Infect. Dis. 2011, 52 (Suppl. 5), S397–S428. [Google Scholar] [CrossRef] [PubMed]
- Timsit, J.F.; de Kraker, M.E.A.; Sommer, H.; Weiss, E.; Bettiol, E.; Wolkewitz, M.; Nikolakopoulos, S.; Wilson, D.; Harbarth, S.; On Behalf of the COMBACTE-NET Consortium. Appropriate endpoints for evaluation of new antibiotic therapies for severe infections: A perspective from COMBACTE’s STAT-Net. Intensive Care Med. 2017, 43, 1002–1012. [Google Scholar] [CrossRef] [Green Version]
- Leone, S.; Cascella, M.; Pezone, I.; Fiore, M. New antibiotics for the treatment of serious infections in intensive care unit patients. Curr. Med. Res. Opin. 2019, 35, 1331–1334. [Google Scholar] [CrossRef]
- Handbook-5-1. cochrane. Chapter 13: Including non-randomized studies. Available online: https://handbook-5-1.cochrane.org/index.htm#chapter_13/13_including_non_randomized_studies.htm (accessed on 3 July 2020).
- Naim, H.; Rizvi, M.; Gupta, R.; Azam, M.; Taneja, N.; Shukla, I.; Khan, H.M. Drug Resistance and Molecular Epidemiology of Carbapenem Resistant Gram-negative Bacilli Isolates. J. Glob. Infect. Dis. 2018, 10, 133–139. [Google Scholar] [CrossRef]
- Onorato, L.; Di Caprio, G.; Signoriello, S.; Coppola, N. Efficacy of ceftazidime/avibactam in monotherapy or combination therapy against carbapenem-resistant Gram-negative bacteria: A meta-analysis. Int. J. Antimicrob. Agents 2019, 54, 735–740. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants | Intervention | Comparison | Outcomes | Study Design |
|---|---|---|---|---|
| Adult patients in any setting with confirmed bacterial infection | Ceftazidime-avibactam in association with another antibiotic/s | Ceftazidime-avibactam alone | Primary outcomes: all-cause mortality Secondary outcomes: (a) not clinical improvement, (b) not microbiological improvement | Randomized controlled trials and observational studies (including cohort andcase–control studies) |
| Author (Published Year) [ref.] | Journal | Study Design | Time Spam | Pathogen | Septic Focus | Evaluation Time Points | ||
|---|---|---|---|---|---|---|---|---|
| Mortality | Clinical | Microbiological | ||||||
| Sousa (2018) [8] | J Antimicrob Chemother | RC | 04/16–12/17 | CRE (KPC: 95%) | Mix | 30-days | 7-days | 7-days |
| King (2017) [26] | Antimicrob Agents Chemother | RC | 03/05–04/16 | CRE (KPC: 83%) | Mix | In Hospital | end of therapy | end of therapy |
| Alraddadi (2019) [27] | BMC Infectious Diseases | RC | 01/17–08/18 | CRE (KPC: 79%) | Mix | 30-days | 30-days | 30-days |
| Caston (2017) [6] | Int J Infect Dis | RC | 06/12–03/16 | CRE (KPC: 80%) | Bacteremia | 30-days | 14-days | - |
| Shields (2017) [7] | Antimicrob Agents Chemother | RC | 01/09–02/17 | CRE (KPC: 100%) | Bacteremia | 30-days | - | - |
| Tumbarello (2019) [5] | Clin Infect Dis | RC | 04/16–12/17 | CRE(KPC: 100%) | Bacteremia | 30-days | - | In Hospital* |
| Carmeli (2016) [19] | Lancet Infect Dis | RCT | 01/13–08/14 | MIX | cIAI / cUTI | 28-days | 7–10 days | 21/25-days |
| Lucasti (2013) [21] | J Antimicrob Chemother | RCT | 03/09–12/09 | MIX | cIAI | - | 14-days | 14-days |
| Qin (2017) [22] | Int J Antimicrob Agents | RCT | 01/13–03/15 | MIX | cIAI | - | 28–35 days | - |
| Mazuski (2016) [23] | Clin Infect Dis | RCT | 03/12–04/13 | MIX | cIAI | - | 28–35 days | 28–35 days |
| Vazquez (2012) [24] | Curr Med Res Opin | RCT | 11/08–06/10 | MIX | cUTI | - | 5–9 days | 5–9 days |
| Wagenlehner (2016) [25] | Clin Infect Dis | RCT | 10/10–08/14 | MIX | cUTI | - | 21–25 days | 21–25 days |
| Torres (2018) [20] | Lancet Infect Dis | RCT | 04/13–02/15 | MIX | NP | 21–25 days | 21–25 days | 21–25 days |
| Author (Published Year) [ref.] | N° of patients Enrolled | N° of Bacteremia (%) | N° of Patients Treated with CZA Alone | N° of Patients Treated with CZA Association | N° of Patients Treated with BAT | BAT | CZA-Associated Antibiotic | Medical Ward |
|---|---|---|---|---|---|---|---|---|
| Sousa (2018) [8] | 57 | 26 (46) | 46 | 11 | X | X | # | NS |
| King (2017) [26] | 60 | 23 (38) | 33 | 27 | X | X | ^ | Mix ICU (59%) |
| Alraddadi (2019) [27] | 38 | 22 (58) | 10 | X | 28 | § | X | NS |
| Caston (2017) [6] | 31 | 31 (100) | X | 8 | 23 | ^^ | ^^ | Mix ICU (10%) |
| Shields (2017) [7] | 109 | 109 (100) | 8 | 5 | 96 | ++ | <> | Mix ICU (50%) |
| Tumbarello (2019) [5] | 208 | 208 (100) | 22 | 82 | 104 | §§ | ## | Mix ICU (33.3%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiore, M.; Alfieri, A.; Di Franco, S.; Pace, M.C.; Simeon, V.; Ingoglia, G.; Cortegiani, A. Ceftazidime-Avibactam Combination Therapy Compared to Ceftazidime-Avibactam Monotherapy for the Treatment of Severe Infections Due to Carbapenem-Resistant Pathogens: A Systematic Review and Network Meta-Analysis. Antibiotics 2020, 9, 388. https://doi.org/10.3390/antibiotics9070388
Fiore M, Alfieri A, Di Franco S, Pace MC, Simeon V, Ingoglia G, Cortegiani A. Ceftazidime-Avibactam Combination Therapy Compared to Ceftazidime-Avibactam Monotherapy for the Treatment of Severe Infections Due to Carbapenem-Resistant Pathogens: A Systematic Review and Network Meta-Analysis. Antibiotics. 2020; 9(7):388. https://doi.org/10.3390/antibiotics9070388
Chicago/Turabian StyleFiore, Marco, Aniello Alfieri, Sveva Di Franco, Maria Caterina Pace, Vittorio Simeon, Giulia Ingoglia, and Andrea Cortegiani. 2020. "Ceftazidime-Avibactam Combination Therapy Compared to Ceftazidime-Avibactam Monotherapy for the Treatment of Severe Infections Due to Carbapenem-Resistant Pathogens: A Systematic Review and Network Meta-Analysis" Antibiotics 9, no. 7: 388. https://doi.org/10.3390/antibiotics9070388
APA StyleFiore, M., Alfieri, A., Di Franco, S., Pace, M. C., Simeon, V., Ingoglia, G., & Cortegiani, A. (2020). Ceftazidime-Avibactam Combination Therapy Compared to Ceftazidime-Avibactam Monotherapy for the Treatment of Severe Infections Due to Carbapenem-Resistant Pathogens: A Systematic Review and Network Meta-Analysis. Antibiotics, 9(7), 388. https://doi.org/10.3390/antibiotics9070388