

Vaccine Hesitancy in Sub-Saharan Africa in the Context of COVID-19 Vaccination Exercise: A Systematic Review


Abstract
:
1. Introduction
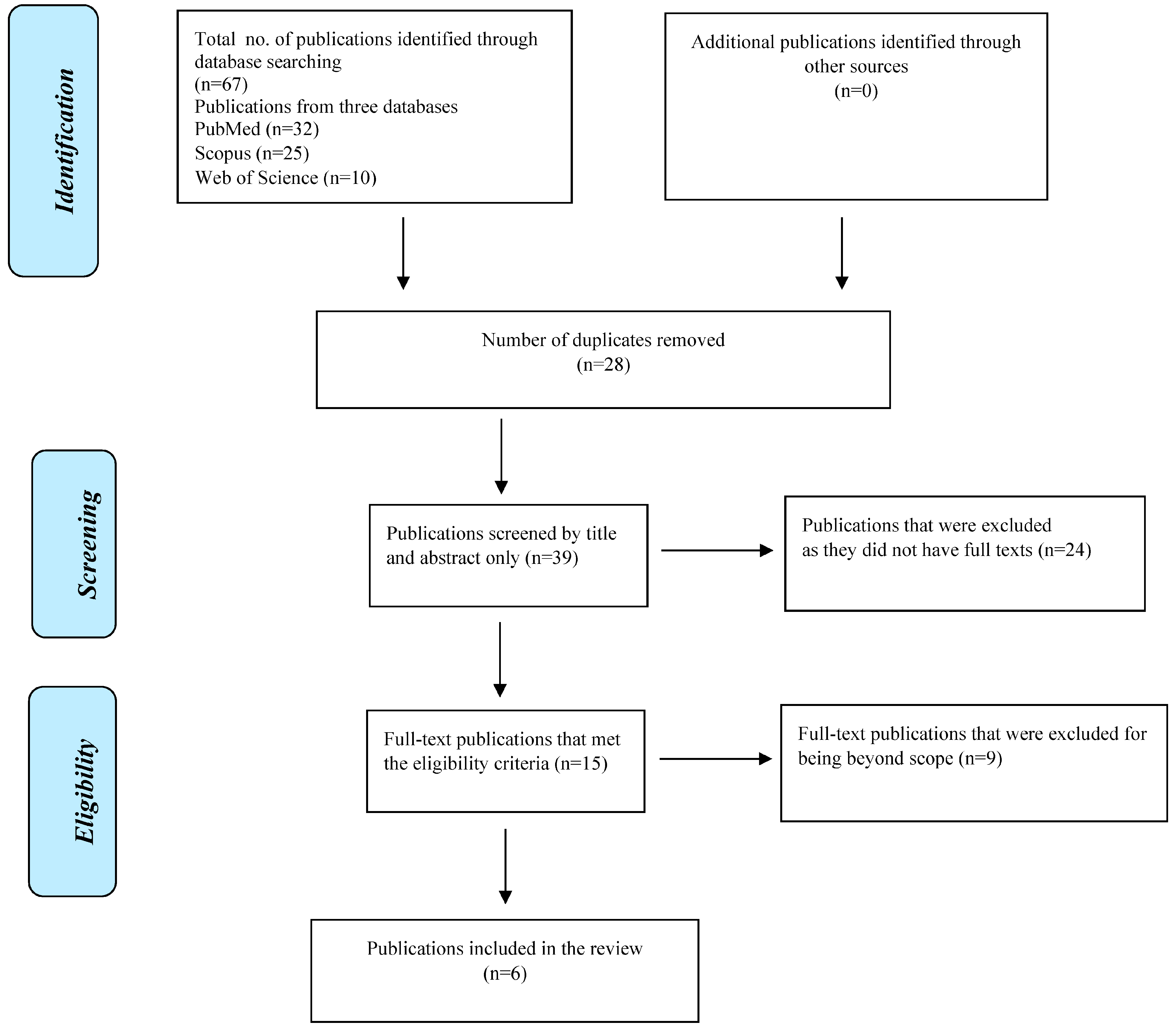
2. Methods
3. Results
4. Discussion
5. Limitations
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Naim, I. 3.0 Ethical Theories and Problem Solving Techniques. Available online: www.academia.edu (accessed on 30 October 2022).
- Dawson, A. Herd protection as a public good: Vaccination and our obligations to others. Ethics Prev. Public Health 2007, 160, 163. [Google Scholar]
- Giubilini, A.; Douglas, T.; Savulescu, J. The Moral Obligation to Be Vaccinated: Utilitarianism, Contractualism, and Collective Easy Rescue. Med. Health Care Philos. 2018, 21, 547–560. [Google Scholar] [CrossRef]
- Giubilini, A. Vaccination Ethics. Br. Med. Bull. 2020, 137, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Nihlén Fahlquist, J. Vaccine Hesitancy and Trust. Ethical Aspects of Risk Communication. Scand. J. Public Health 2017, 46, 182–188. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- WHO. WHO Strategic Advisory Group of Experts (SAGE) on Immunization: Request for Nominations. Vaccine 2014, 32, 1774. [Google Scholar] [CrossRef]
- Larson, H.J.; Cooper, L.Z.; Eskola, J.; Katz, S.L.; Ratzan, S. Addressing the Vaccine Confidence Gap. Lancet 2011, 378, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Williamson, L.; Glaab, H. Addressing Vaccine Hesitancy Requires an Ethically Consistent Health Strategy. BMC Med. Ethics 2018, 19, 84. [Google Scholar] [CrossRef] [PubMed]
- Saint-Victor, D.S.; Omer, S.B. Vaccine Refusal and the Endgame: Walking the Last Mile First. Philos. Trans. R. Soc. B Biol. Sci. 2013, 368, 20120148. [Google Scholar] [CrossRef]
- Wolfe, R.M. Anti-Vaccinationists Past and Present. BMJ 2002, 325, 430–432. [Google Scholar] [CrossRef]
- Blume, S. Anti-Vaccination Movements and Their Interpretations. Soc. Sci. Med. 2006, 62, 628–642. [Google Scholar] [CrossRef] [PubMed]
- Afolabi, A.A.; Ilesanmi, O.S. Dealing with Vaccine Hesitancy in Africa: The Prospective COVID-19 Vaccine Context. Pan Afr. Med. J. 2021, 38, 3. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Rus, M.; Groselj, U. Ethics of Vaccination in Childhood—A Framework Based on the Four Principles of Biomedical Ethics. Vaccines 2021, 9, 113. [Google Scholar] [CrossRef] [PubMed]
- Kaseje, N.; Oruenjo, K.; Kaseje, D.; Evans, T.G.; Tanner, M.; Haines, A.; Nyikal, J. Leveraging Latent Assets to Strengthen the COVID-19 Response and Vaccine Roll-out in Africa. BMJ Global Health 2021, 6, e006289. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. A Global Database of COVID-19 Vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef] [PubMed]
- WHO. COVAX: Working for Global Equitable Access to COVID-19 VACCINES. 2022. Available online: https://www.who.int/initiatives/act-accelerator/covax (accessed on 12 November 2022).
- Ekwebelem, O.C.; Yunusa, I.; Onyeaka, H.; Ekwebelem, N.C.; Nnorom-Dike, O. COVID-19 Vaccine Rollout: Will It Affect the Rates of Vaccine Hesitancy in Africa? Public Health 2021, 197, e18. [Google Scholar] [CrossRef]
- Flint, K. “Africa Isn’t a Testing Lab”: Considering COVID Vaccine Trials in a History of Biomedical Experimentation and Abuse. J. West Afr. Hist. 2020, 6, 126. [Google Scholar] [CrossRef]
- Harrison, E.A.; Wu, J.W. Vaccine Confidence in the Time of COVID-19. Eur. J. Epidemiol. 2020, 35, 325–330. [Google Scholar] [CrossRef]
- Trogen, B.; Pirofski, L. Understanding Vaccine Hesitancy in COVID-19. Med 2021, 2, 498–501. [Google Scholar] [CrossRef]
- Mtolo, T.M.; Motloba, P.D.; Wood, N.H. Mandatory COVID-19 Vaccination for Oral Health Professionals (OHPs)—Ethical Appraisal. S. Afr. Dent. J. 2021, 76, 42–45. [Google Scholar] [CrossRef]
- Africa CDC. Africa CDC COVID-19 Vaccine Dashboard. 2022. Available online: https://africacdc.org/covid-19-vaccination/ (accessed on 17 November 2022).


{kind=link}
{kind=link}
| Article | Search | Selection Criteria | Information Retrieval | Quality Assessment | Major Outcomes | |
|---|---|---|---|---|---|---|
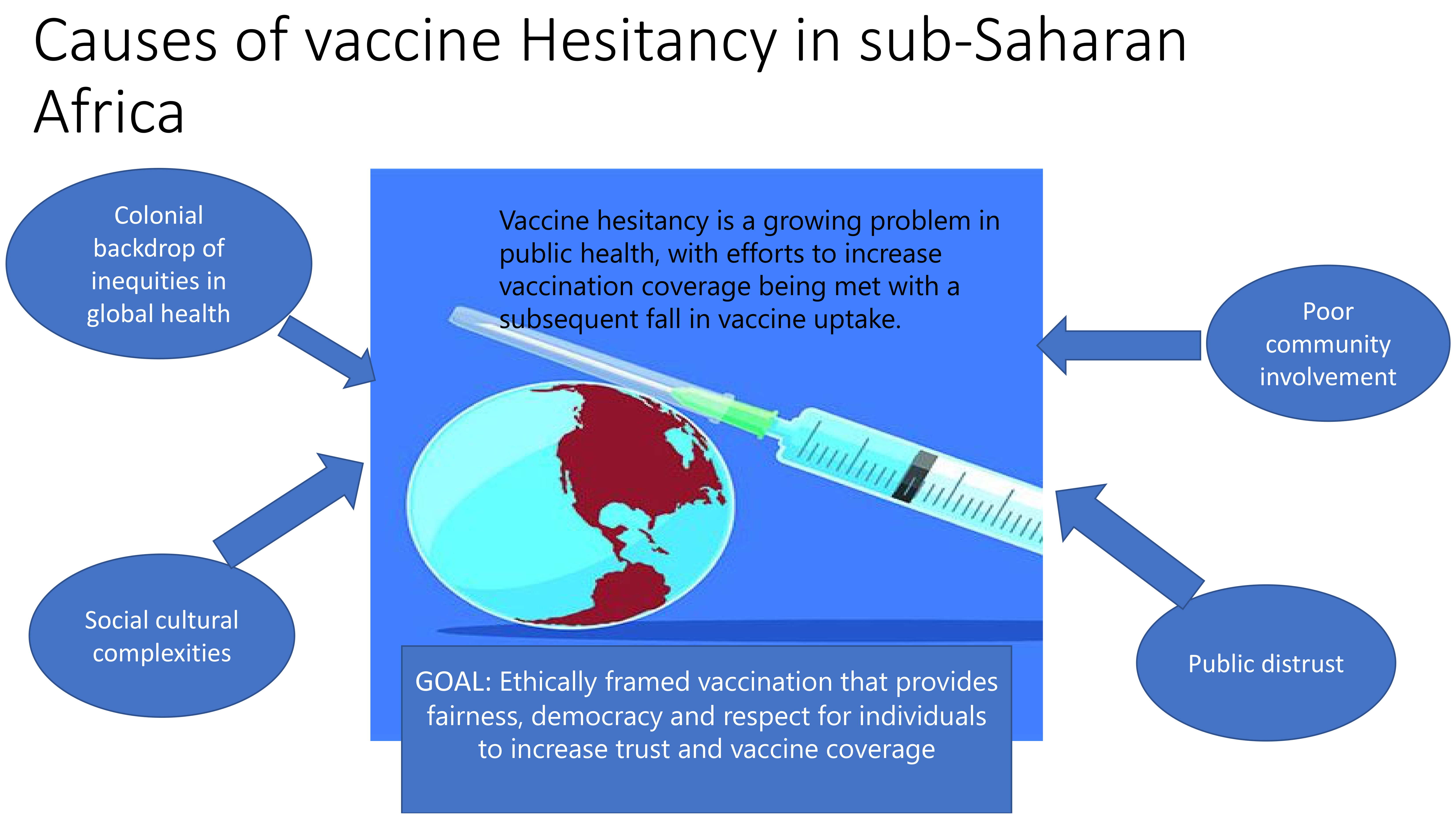
| 1. | Afolabi and Ilesanmi [13] | PubMed (Journal article—Primary source) | COVID-19 vaccine hesitancy in Africa | Vaccine hesitancy is not a new concept in SSA. There is need for measures to be put in place to prevent COVID-19 vaccine hesitancy, for example, involving the community in the delivery of the vaccines. | The paper advocates for the integration of COVID-19 vaccines into the routine immunization schedule to improve vaccine uptake. | Possible causes of COVID-19 vaccine hesitancy in Africa include public distrust; delayed emergency response in the continent, i.e., laxity in border closures and the subsequent importation of the virus to Africa; and a lack of community involvement in the contexts of social distancing, handwashing and masking, among other measures. African governments also did little to debunk social and traditional media theories that the African continent is “immune” to the virus due to the climatic conditions. As a result of these reasons, many Africans lacked confidence in the manner in which the virus was being reported and handled in the continent. |
| 2. | Ekwebelem et al. [19] | Science Direct Letter to the Editor (Opinion piece) | COVID-19 vaccine and vaccine hesitancy in Africa | In 2019, vaccine hesitancy was listed by WHO as one of the top threats to health and wellbeing. Vaccine hesitancy is driven by cultural, social, historical, political and individual factors such as values, risk perceptions, emotions, knowledge or beliefs. | Africa is a multicultural and diverse continent. Sociocultural complexity has contributed immensely to sporadic vaccine hesitancy. As a result, hesitancy toward COVID-19 vaccines is expected to ultimately vary in different contexts. | There are fears, misinformation and conspiracy theories being spread by social influencers, religious leaders, anti-vaccinists and political leaders that the vaccine is being used to reduce the rising population and also to track people’s lives through microchips. |
| 3. | Flint [20] | JSTOR (Journal article—Primary source) | COVID vaccine trials in Africa | COVID vaccine trials are happening in contexts where there is a history of biomedical experimentation and abuse, such as in the African continent. Vaccine hesitancy in Africa stems from the colonial geography, structural adjustment programs of the 1980s and 1990s, the HIV/AIDs pandemic, clinical trials involving pharmaceutical companies and the influence of iniquities in global health field. | The backdrop of colonialism is important in understanding the resistance to COVID-19 vaccine trials. | There is a need to rethink more equitable relations within global health. |
| 4. | Harrison and Wu [21] | Scopus (Opinion piece) | Vaccine confidence in the time of COVID-19 | A need to reexamine whether the COVID-19 pandemic will ease the historical origins of vaccine hesitancy/refusal in sub-Saharan Africa. | A push for vaccine confidence as a means of conceptualizing and responding to the COVID-19 pandemic in a mutual manner. | A call for a public health culture that embraces vaccine safety. The concept of public health programs must be broader than the delivery of the vaccine (biomedical supply chain). |
| 5. | Nihlén [5] | PubMed (Journal article—Primary source) | Vaccine hesitancy and trust | The paper analyzes vaccination policy from an ethical perspective against the backdrop of growing vaccine hesitancy. | The paper looks into examples of vaccination programs such as those for measles and H1N1 and associated side effects that propel hesitancy. | Vaccine skeptics should not be treated as ill-informed or less educated, but their concerns should be addressed respectfully. Furthermore, the public should trust the message and count on the government to take responsibility for individuals affected by vaccine side effects. |
| 6. | Trogen and Pirofski [22] | Web of Science (Commentary) | Understanding vaccine hesitancy in COVID-19 | The initial concerns about the scarcity of COVID-19 vaccines increased public demand, but as supply meets demand, vaccine hesitancy is becoming a defining theme of the pandemic. | The paper differentiates vaccine hesitancy from vaccine refusal. Vaccine refusal carries with it deep political, cultural and emotional underpinnings that are difficult to overcome. Individuals in this group are often described as anti-vaxxers (also known as anti-vaccinists). | Overcoming vaccine hesitancy requires a multipronged approach, especially when the vaccine benefits outweigh the risks. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ochola, E.A. Vaccine Hesitancy in Sub-Saharan Africa in the Context of COVID-19 Vaccination Exercise: A Systematic Review. Diseases 2023, 11, 32. https://doi.org/10.3390/diseases11010032
Ochola EA. Vaccine Hesitancy in Sub-Saharan Africa in the Context of COVID-19 Vaccination Exercise: A Systematic Review. Diseases. 2023; 11(1):32. https://doi.org/10.3390/diseases11010032
Chicago/Turabian StyleOchola, Elizabeth A. 2023. "Vaccine Hesitancy in Sub-Saharan Africa in the Context of COVID-19 Vaccination Exercise: A Systematic Review" Diseases 11, no. 1: 32. https://doi.org/10.3390/diseases11010032
APA StyleOchola, E. A. (2023). Vaccine Hesitancy in Sub-Saharan Africa in the Context of COVID-19 Vaccination Exercise: A Systematic Review. Diseases, 11(1), 32. https://doi.org/10.3390/diseases11010032