
Comparative Analysis on the Effect of Sarcopenia in Patients with Knee Osteoarthritis before and after Total Knee Arthroplasty

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Anthropometry
2.3. Sarcopenia Measurement
2.4. Knee Injury and Osteoarthritis Outcome Score (KOOS)
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosenberg, I.H. Sarcopenia: Origins and Clinical Relevance. J. Nutr. 1997, 127, 990S–991S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.W.; Kim, R.; Choi, H.; Lee, S.-J.; Bae, G.-U. Understanding of Sarcopenia: From Definition to Therapeutic Strategies. Arch. Pharm. Res. 2021, 44, 876–889. [Google Scholar] [CrossRef]
- Mayhew, A.J.; Amog, K.; Phillips, S.; Parise, G.; McNicholas, P.D.; de Souza, R.J.; Thabane, L.; Raina, P. The Prevalence of Sarcopenia in Community-Dwelling Older Adults, an Exploration of Differences between Studies and within Definitions: A Systematic Review and Meta-Analyses. Age Ageing 2019, 48, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Abellan Van Kan, G. Epidemiology and Consequences of Sarcopenia. J. Nutr. Health Aging 2009, 13, 708–712. [Google Scholar] [CrossRef]
- Papadopoulou, S.K.; Tsintavis, P.; Potsaki, G.; Papandreou, D. Differences in the Prevalence of Sarcopenia in Community-Dwelling, Nursing Home and Hospitalized Individuals. A Systematic Review and Meta-Analysis. J. Nutr. Health Aging 2020, 24, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Daily, J.W.; Park, S. Sarcopenia Is a Cause and Consequence of Metabolic Dysregulation in Aging Humans: Effects of Gut Dysbiosis, Glucose Dysregulation, Diet and Lifestyle. Cells 2022, 11, 338. [Google Scholar] [CrossRef] [PubMed]
- Gariballa, S.; Alessa, A. Sarcopenia: Prevalence and Prognostic Significance in Hospitalized Patients. Clin. Nutr. 2013, 32, 772–776. [Google Scholar] [CrossRef]
- Xu, J.; Wan, C.S.; Ktoris, K.; Reijnierse, E.M.; Maier, A.B. Sarcopenia Is Associated with Mortality in Adults: A Systematic Review and Meta-Analysis. Gerontology 2022, 68, 361–376. [Google Scholar] [CrossRef]
- Mesinovic, J.; Zengin, A.; De Courten, B.; Ebeling, P.R.; Scott, D. Sarcopenia and Type 2 Diabetes Mellitus: A Bidirectional Relationship. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 1057–1072. [Google Scholar] [CrossRef] [Green Version]
- Dunne, R.F.; Loh, K.P.; Williams, G.R.; Jatoi, A.; Mustian, K.M.; Mohile, S.G. Cachexia and Sarcopenia in Older Adults with Cancer: A Comprehensive Review. Cancers 2019, 11, 1861. [Google Scholar] [CrossRef] [Green Version]
- Shachar, S.S.; Williams, G.R.; Muss, H.B.; Nishijima, T.F. Prognostic Value of Sarcopenia in Adults with Solid Tumours: A Meta-Analysis and Systematic Review. Eur. J. Cancer 2016, 57, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.M.; Song, A.; David, A.R.; Chen, V.E.; Lu, B.; Werner-Wasik, M. Impact of Sarcopenia on Survival in Patients With Early-Stage Lung Cancer Treated With Stereotactic Body Radiation Therapy. Cureus 2020, 12, e10712. [Google Scholar] [CrossRef]
- Norman, K.; Otten, L. Financial Impact of Sarcopenia or Low Muscle Mass—A Short Review. Clin. Nutr. 2019, 38, 1489–1495. [Google Scholar] [CrossRef]
- Katz, J.N.; Arant, K.R.; Loeser, R.F. Diagnosis and Treatment of Hip and Knee Osteoarthritis: A Review. JAMA 2021, 325, 568–578. [Google Scholar] [CrossRef]
- Sandell, L.J.; Aigner, T. Articular Cartilage and Changes in Arthritis: Cell Biology of Osteoarthritis. Arthritis Res. Ther. 2001, 3, 107. [Google Scholar] [CrossRef] [Green Version]
- Sohn, D.H.; Sokolove, J.; Sharpe, O.; Erhart, J.C.; Chandra, P.E.; Lahey, L.J.; Lindstrom, T.M.; Hwang, I.; Boyer, K.A.; Andriacchi, T.P.; et al. Plasma Proteins Present in Osteoarthritic Synovial Fluid Can Stimulate Cytokine Production via Toll-like Receptor 4. Arthritis Res. Ther. 2012, 14, R7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litwic, A.; Edwards, M.H.; Dennison, E.M.; Cooper, C. Epidemiology and Burden of Osteoarthritis. Br. Med. Bull. 2013, 105, 185–199. [Google Scholar] [CrossRef] [Green Version]
- Safiri, S.; Kolahi, A.-A.; Smith, E.; Hill, C.; Bettampadi, D.; Mansournia, M.A.; Hoy, D.; Ashrafi-Asgarabad, A.; Sepidarkish, M.; Almasi-Hashiani, A.; et al. Global, Regional and National Burden of Osteoarthritis 1990-2017: A Systematic Analysis of the Global Burden of Disease Study 2017. Ann. Rheum. Dis. 2020, 79, 819–828. [Google Scholar] [CrossRef]
- Loeser, R.F. Age-Related Changes in the Musculoskeletal System and the Development of Osteoarthritis. Clin. Geriatr. Med. 2010, 26, 371–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verma, D.K.; Kumari, P.; Kanagaraj, S. Engineering Aspects of Incidence, Prevalence, and Management of Osteoarthritis: A Review. Ann. Biomed. Eng. 2022, 50, 237–252. [Google Scholar] [CrossRef]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, Regional Prevalence, Incidence and Risk Factors of Knee Osteoarthritis in Population-Based Studies. EClinicalMedicine 2020, 29–30, 100587. [Google Scholar] [CrossRef] [PubMed]
- Losina, E.; Weinstein, A.M.; Reichmann, W.M.; Burbine, S.A.; Solomon, D.H.; Daigle, M.E.; Rome, B.N.; Chen, S.P.; Hunter, D.J.; Suter, L.G.; et al. Lifetime Risk and Age at Diagnosis of Symptomatic Knee Osteoarthritis in the US. Arthritis Care Res. 2013, 65, 703–711. [Google Scholar] [CrossRef] [Green Version]
- Jordan, J.M.; Helmick, C.G.; Renner, J.B.; Luta, G.; Dragomir, A.D.; Woodard, J.; Fang, F.; Schwartz, T.A.; Abbate, L.M.; Callahan, L.F.; et al. Prevalence of Knee Symptoms and Radiographic and Symptomatic Knee Osteoarthritis in African Americans and Caucasians: The Johnston County Osteoarthritis Project. J. Rheumatol. 2007, 34, 172–180. [Google Scholar] [PubMed]
- Pickering, M.-E.; Chapurlat, R. Where Two Common Conditions of Aging Meet: Osteoarthritis and Sarcopenia. Calcif. Tissue Int. 2020, 107, 203–211. [Google Scholar] [CrossRef]
- Misra, D.; Fielding, R.A.; Felson, D.T.; Niu, J.; Brown, C.; Nevitt, M.; Lewis, C.E.; Torner, J.; Neogi, T.; the MOST study. Risk of Knee Osteoarthritis With Obesity, Sarcopenic Obesity, and Sarcopenia. Arthritis Rheumatol. 2019, 71, 232–237. [Google Scholar] [CrossRef] [Green Version]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Ardeljan, A.D.; Polisetty, T.S.; Palmer, J.; Vakharia, R.M.; Roche, M.W. Comparative Analysis on the Effects of Sarcopenia Following Primary Total Knee Arthroplasty: A Retrospective Matched-Control Analysis. J. Knee Surg. 2022, 35, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Cram, P.; Lu, X.; Kates, S.L.; Singh, J.A.; Li, Y.; Wolf, B.R. Total Knee Arthroplasty Volume, Utilization, and Outcomes among Medicare Beneficiaries, 1991–2010. JAMA 2012, 308, 1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hossain, F.; Patel, S.; Haddad, F.S. Midterm Assessment of Causes and Results of Revision Total Knee Arthroplasty. Clin. Orthop. 2010, 468, 1221–1228. [Google Scholar] [CrossRef] [Green Version]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M.; et al. The FNIH Sarcopenia Project: Rationale, Study Description, Conference Recommendations, and Final Estimates. J. Gerontol. Ser. A 2014, 69, 547–558. [Google Scholar] [CrossRef]
- Wang, H.; Wang, N.; Wang, Y.; Li, H. Association between Sarcopenia and Osteoarthritis: A Protocol for Meta-Analysis. PLoS ONE 2022, 17, e0272284. [Google Scholar] [CrossRef] [PubMed]
- Abu Khaled, M.; McCutcheon, M.J.; Reddy, S.; Pearman, P.L.; Hunter, G.R.; Weinsier, R.L. Electrical Impedance in Assessing Human Body Composition: The BIA Method. Am. J. Clin. Nutr. 1988, 47, 789–792. [Google Scholar] [CrossRef] [PubMed]
- Scafoglieri, A.; Clarys, J.P.; Bauer, J.M.; Verlaan, S.; Malderen, L.V.; Vantieghem, S.; Cederholm, T.; Sieber, C.C.; Mets, T.; Bautmans, I. Predicting Appendicular Lean and Fat Mass with Bioelectrical Impedance Analysis in Older Adults with Physical Function Decline—The PROVIDE Study. Clin. Nutr. 2017, 36, 869–875. [Google Scholar] [CrossRef] [Green Version]
- Vermeiren, S.; Beckwée, D.; Vella-Azzopardi, R.; Beyer, I.; Knoop, V.; Jansen, B.; Delaere, A.; Antoine, A.; Bautmans, I.; Scafoglieri, A.; et al. Evaluation of Appendicular Lean Mass Using Bio Impedance in Persons Aged 80+: A New Equation Based on the BUTTERFLY-Study. Clin. Nutr. 2019, 38, 1756–1764. [Google Scholar] [CrossRef]
- Roos, E.M.; Toksvig-Larsen, S. Knee Injury and Osteoarthritis Outcome Score (KOOS)—Validation and Comparison to the WOMAC in Total Knee Replacement. Health Qual. Life Outcomes 2003, 1, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moutzouri, M.; Tsoumpos, P.; Billis, E.; Papoutsidakis, A.; Gliatis, J. Cross-Cultural Translation and Validation of the Greek Version of the Knee Injury and Osteoarthritis Outcome Score (KOOS) in Patients with Total Knee Replacement. Disabil. Rehabil. 2015, 37, 1477–1483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyman, S.; Lee, Y.-Y.; Franklin, P.D.; Li, W.; Cross, M.B.; Padgett, D.E. Validation of the KOOS, JR: A Short-Form Knee Arthroplasty Outcomes Survey. Clin. Orthop. 2016, 474, 1461–1471. [Google Scholar] [CrossRef] [Green Version]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)—Development of a Self-Administered Outcome Measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef]
- Mazziotta, C.; Pellielo, G.; Tognon, M.; Martini, F.; Rotondo, J.C. Significantly Low Levels of IgG Antibodies Against Oncogenic Merkel Cell Polyomavirus in Sera From Females Affected by Spontaneous Abortion. Front. Microbiol. 2021, 12, 3542. [Google Scholar] [CrossRef]
- He, Z.; Cai, J.; Wang, X.; Lu, D. Clinical and Functional Outcomes of Total Knee Arthroplasty in Sarcopenia: A Case–Control Retrospective Cohort Study. J. Knee Surg. 2021. [Google Scholar] [CrossRef]
- Ho, K.K.-W.; Lau, L.C.-M.; Chau, W.-W.; Poon, Q.; Chung, K.-Y.; Wong, R.M.-Y. End-Stage Knee Osteoarthritis with and without Sarcopenia and the Effect of Knee Arthroplasty—A Prospective Cohort Study. BMC Geriatr. 2021, 21, 2. [Google Scholar] [CrossRef] [PubMed]
- Jin, W.S.; Choi, E.J.; Lee, S.Y.; Bae, E.J.; Lee, T.-H.; Park, J. Relationships among Obesity, Sarcopenia, and Osteoarthritis in the Elderly. J. Obes. Metab. Syndr. 2017, 26, 36–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, C.-D.; Chen, H.-C.; Huang, S.-W.; Liou, T.-H. Impact of Sarcopenia on Rehabilitation Outcomes after Total Knee Replacement in Older Adults with Knee Osteoarthritis. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Goldhahn, S.; Takeuchi, R.; Nakamura, N.; Nakamura, R.; Sawaguchi, T. Responsiveness of the Knee Injury and Osteoarthritis Outcome Score (KOOS) and the Oxford Knee Score (OKS) in Japanese Patients with High Tibial Osteotomy. J. Orthop. Sci. 2017, 22, 862–867. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Non-Sarcopenic (n = 15) | Sarcopenic (n = 5) | p-Value |
|---|---|---|---|
| Age (years) | 64.8 ± 10.51 | 76.4 ± 8.05 | 0.038 * |
| Body Mass Index | 29.39 ± 4.18 | 29.54 ± 6.20 | 0.953 |
| Body Weight (kg) | 84.14 ± 18.84 | 83.26 ± 14.14 | 0.925 |
| Adipose Tissue (%) | 37.55 ± 11.49 | 31.30 ± 5.47 | 0.125 |
| Adipose Tissue (kg) | 31.31 ± 10.48 | 25.78 ± 6.96 | 0.290 |
| Fat Mass (kg) | 52.77 ± 16.50 | 53.88 ± 8.30 | 0.888 |
| Resting Metabolic Rate (kcal) | 1618 ± 414 | 1655 ± 201 | 0.853 |
| Waist/Hip Ratio | 0.89 ± 0.18 | 0.71 ± 0.30 | 0.553 |
| Nutritional Index | 0.45 ± 0.02 | 0.45 ± 0.03 | 0.529 |
| Disease Index | 0.80 ± 0.08 | 0.84 ± 0.01 | 0.197 |
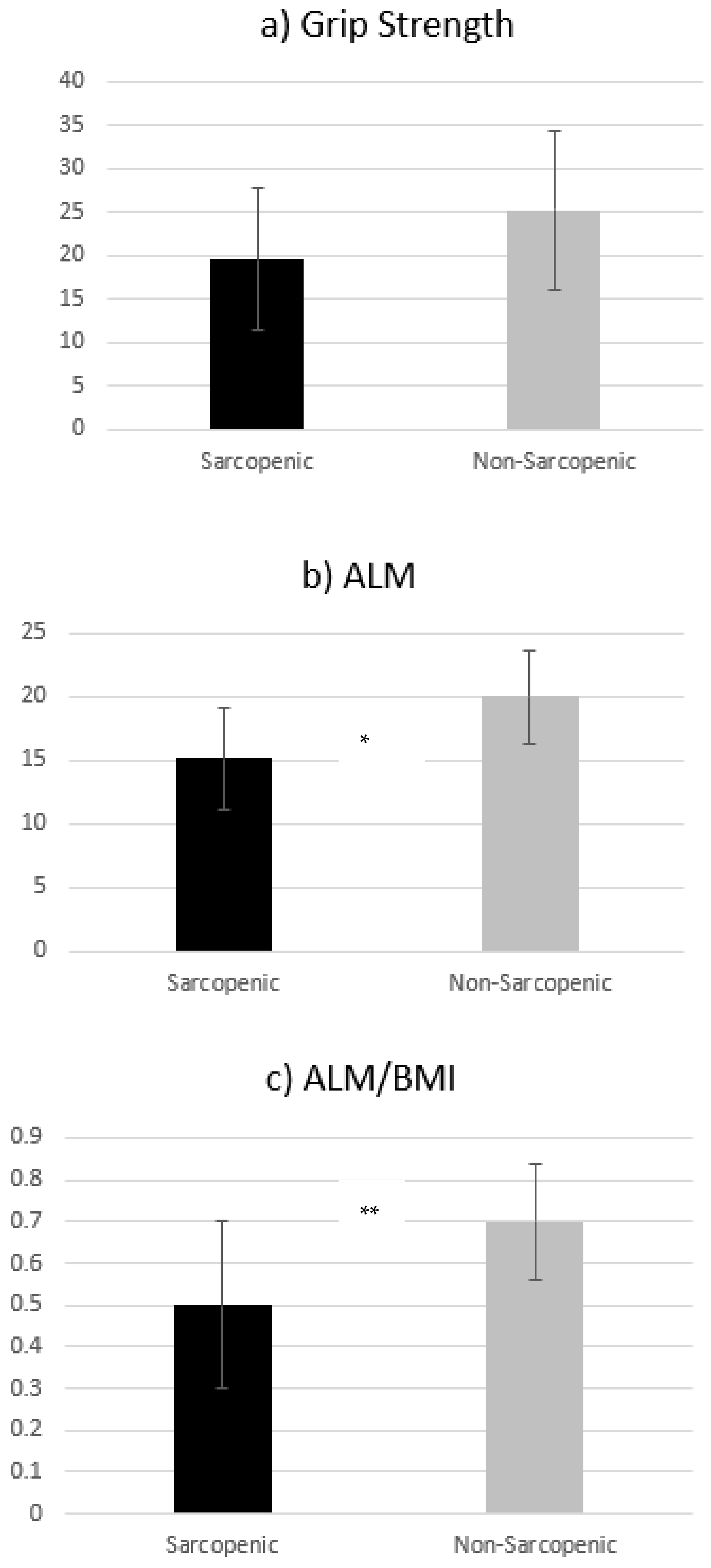
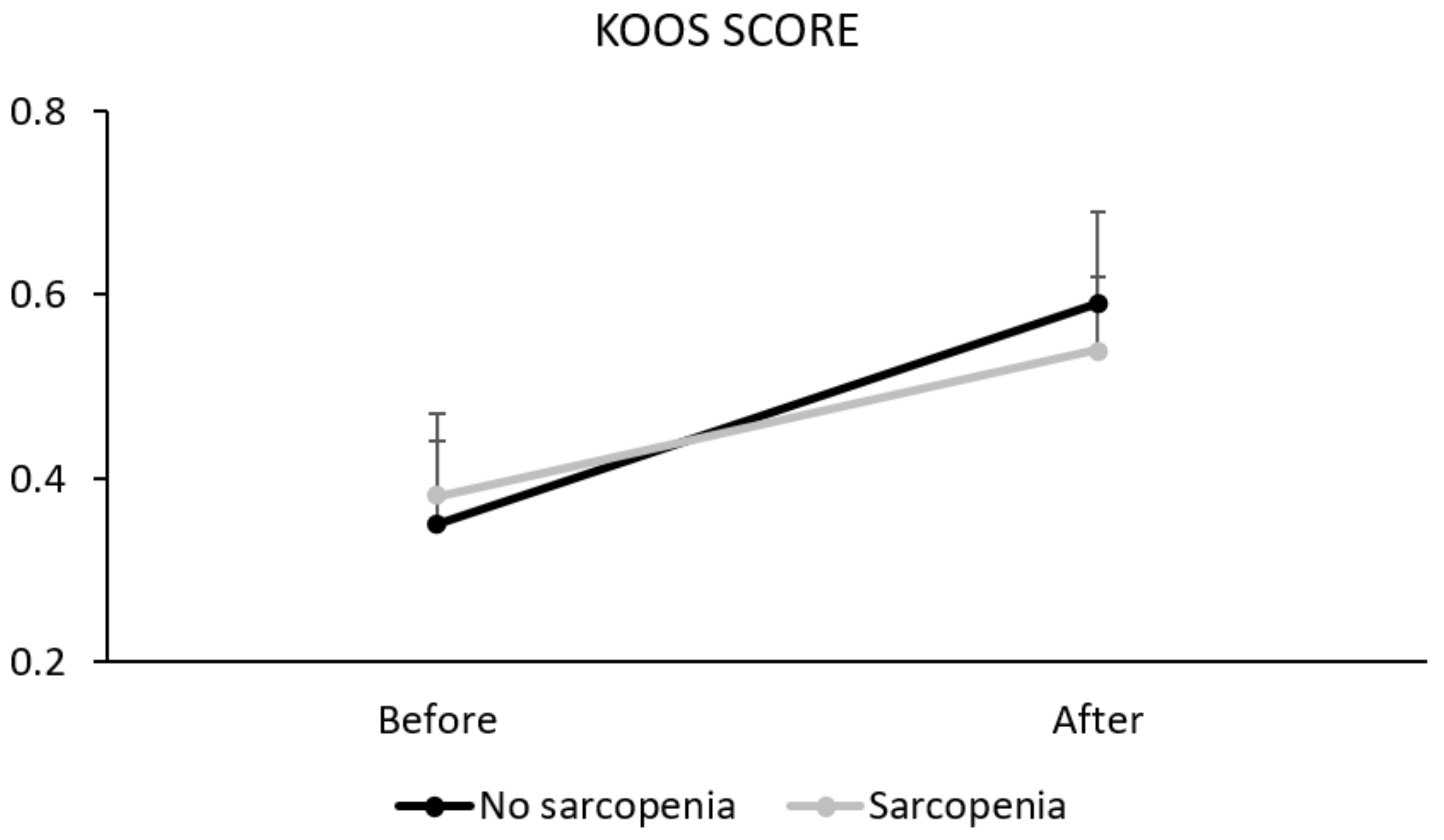
| Parameters | Non-Sarcopenic | Sarcopenic | p-Value | ||||
|---|---|---|---|---|---|---|---|
| KOOS | Before | After | Before | After | T | G | T * G |
| 0.35 ± 0.09 | 0.59 ± 0.10 * | 0.38 ± 0.09 | 0.54 ± 0.08 * | <0.01 | 0.74 | 0.03 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tzartza, C.L.; Karapalis, N.; Voulgaridou, G.; Zidrou, C.; Beletsiotis, A.; Chatziprodromidou, I.P.; Giaginis, C.; Papadopoulou, S.K. Comparative Analysis on the Effect of Sarcopenia in Patients with Knee Osteoarthritis before and after Total Knee Arthroplasty. Diseases 2023, 11, 36. https://doi.org/10.3390/diseases11010036
Tzartza CL, Karapalis N, Voulgaridou G, Zidrou C, Beletsiotis A, Chatziprodromidou IP, Giaginis C, Papadopoulou SK. Comparative Analysis on the Effect of Sarcopenia in Patients with Knee Osteoarthritis before and after Total Knee Arthroplasty. Diseases. 2023; 11(1):36. https://doi.org/10.3390/diseases11010036
Chicago/Turabian StyleTzartza, Chrysanthi Liliana, Nikolaos Karapalis, Gavriela Voulgaridou, Christiana Zidrou, Anastasios Beletsiotis, Ioanna P. Chatziprodromidou, Constantinos Giaginis, and Sousana K. Papadopoulou. 2023. "Comparative Analysis on the Effect of Sarcopenia in Patients with Knee Osteoarthritis before and after Total Knee Arthroplasty" Diseases 11, no. 1: 36. https://doi.org/10.3390/diseases11010036
APA StyleTzartza, C. L., Karapalis, N., Voulgaridou, G., Zidrou, C., Beletsiotis, A., Chatziprodromidou, I. P., Giaginis, C., & Papadopoulou, S. K. (2023). Comparative Analysis on the Effect of Sarcopenia in Patients with Knee Osteoarthritis before and after Total Knee Arthroplasty. Diseases, 11(1), 36. https://doi.org/10.3390/diseases11010036