Do Nonalcoholic Fatty Liver Disease and Fetuin-A Play Different Roles in Symptomatic Coronary Artery Disease and Peripheral Arterial Disease?


 and
and 
Abstract
:1. Introduction
2. Patients and Methods
3. Results
3.1. General Features of Study Population and Comparison of CAD vs. PAD Groups
3.2. Comparison of Non-NAFLD vs. NAFLD Patients
3.3. Correlations of Fetuin-A with Demographic, Anthropometric and Metabolic Parameters
3.4. Factors Associated with CAD (vs. PAD), NAFLD and Fetuin-A at Multivariate Analyses
4. Discussion
4.1. NAFLD Is Highly Prevalent among Patients with Definite Atherosclerotic Disease, though the Highest Prevalence Rates Are Found among Those Patients with PAD
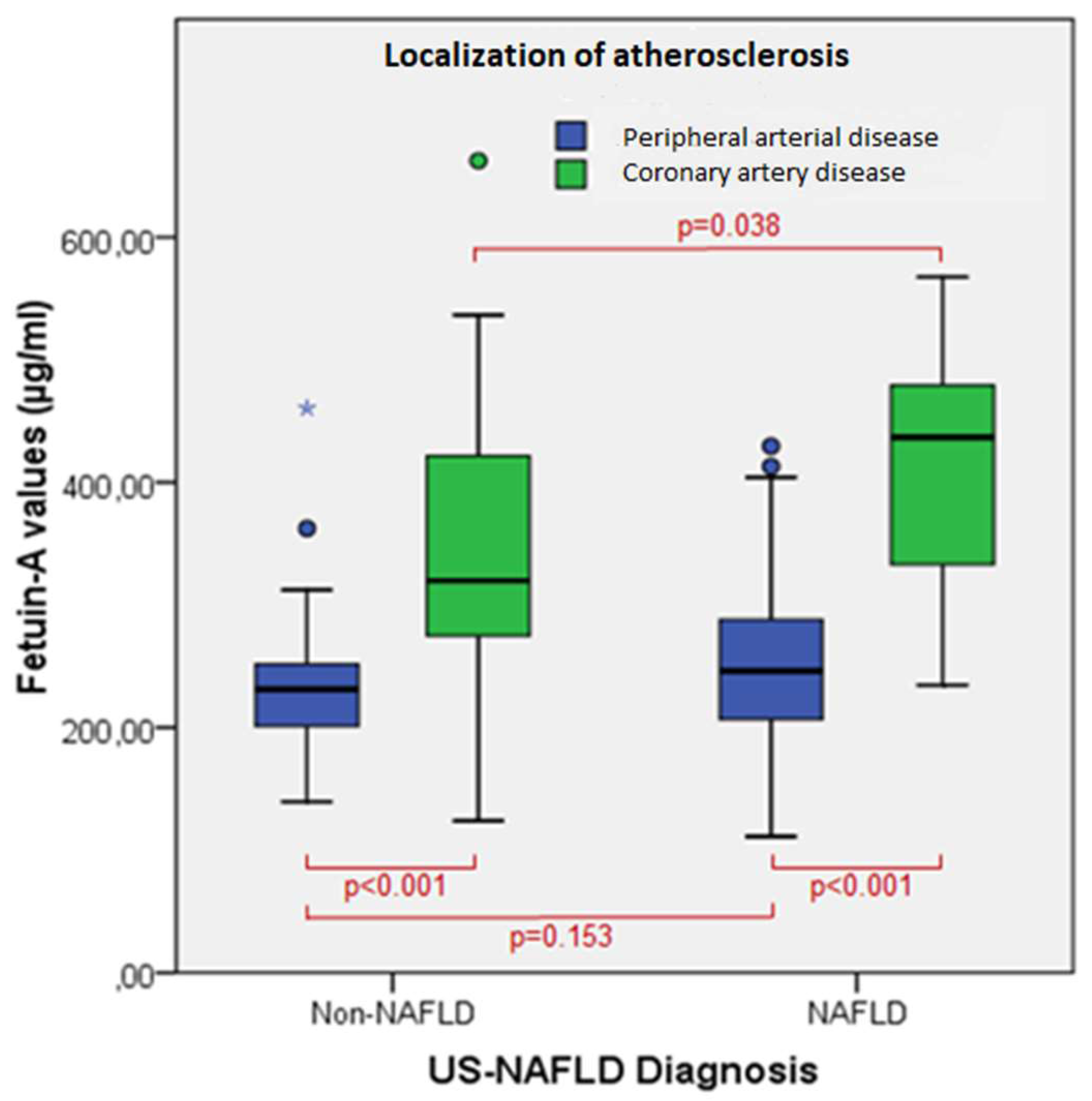
4.2. Patients with CAD Have Higher Values of Fetuin-A than Patients with PAD
4.3. Fetuin-A Is Positively Associated with NAFLD in CAD Patients
4.4. Limitations and Strengths
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| BMI | body mass index |
| CAD | coronary artery disease |
| CI | confidence interval |
| CVD | cardiovascular disease |
| eGFR | estimated glomerular filtration rate |
| HDL | high-density lipoprotein |
| HOMA-IR | homeostasis model assessment of insulin resistance |
| IR | insulin resistance |
| MS | metabolic syndrome |
| NAFLD | nonalcoholic fatty liver disease |
| OR | odds ratio |
| PAD | peripheral arterial disease |
| SE | standard error |
| T2D | type 2 diabetes |
| US-FLI | ultrasonographic-fatty liver indicator |
References
- Lonardo, A.; Nascimbeni, F.; Mantovani, A.; Targher, G. Hypertension, diabetes, atherosclerosis and NASH: Cause or consequence? J. Hepatol. 2017, 68, 335–352. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Lonardo, A.; Bonapace, S.; Byrne, C.D.; Loria, P.; Targher, G. Risk of cardiovascular, cardiac and arrhythmic complications in patients with non-alcoholic fatty liver disease. World J. Gastroenterol. 2014, 20, 1724–1745. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Ballestri, S.; Targher, G.; Loria, P. Diagnosis and management of cardiovascular risk in nonalcoholic fatty liver disease. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 629–650. [Google Scholar] [CrossRef] [PubMed]
- Loria, P.; Marchesini, G.; Nascimbeni, F.; Ballestri, S.; Maurantonio, M.; Carubbi, F.; Ratziu, V.; Lonardo, A. Cardiovascular risk, lipidemic phenotype and steatosis. A comparative analysis of cirrhotic and non-cirrhotic liver disease due to varying etiology. Atherosclerosis 2014, 232, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Haukeland, J.W.; Dahl, T.B.; Yndestad, A.; Gladhaug, I.P.; Loberg, E.M.; Haaland, T.; Konopski, Z.; Wium, C.; Aasheim, E.T.; Johansen, O.E.; et al. Fetuin A in nonalcoholic fatty liver disease: In vivo and in vitro studies. Eur. J. Endocrinol. 2012, 166, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Rametta, R.; Ruscica, M.; Dongiovanni, P.; Macchi, C.; Fracanzani, A.L.; Steffani, L.; Fargion, S.; Magni, P.; Valenti, L. Hepatic steatosis and PNPLA3 I148M variant are associated with serum Fetuin-A independently of insulin resistance. Eur. J. Clin. Investig. 2014, 44, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Hennige, A.M.; Staiger, H.; Machann, J.; Schick, F.; Krober, S.M.; Machicao, F.; Fritsche, A.; Häring, H.U. Alpha2-Heremans-Schmid glycoprotein/fetuin-A is associated with insulin resistance and fat accumulation in the liver in humans. Diabetes Care 2006, 29, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Ix, J.H.; Wassel, C.L.; Kanaya, A.M.; Vittinghoff, E.; Johnson, K.C.; Koster, A.; Cauley, J.A.; Harris, T.B.; Cummings, S.R.; Shlipak, M.G.; et al. Fetuin-A and incident diabetes mellitus in older persons. JAMA 2008, 300, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Ix, J.H.; Shlipak, M.G.; Brandenburg, V.M.; Ali, S.; Ketteler, M.; Whooley, M.A. Association between human fetuin-A and the metabolic syndrome: Data from the Heart and Soul Study. Circulation 2006, 113, 1760–1767. [Google Scholar] [CrossRef] [PubMed]
- Weikert, C.; Stefan, N.; Schulze, M.B.; Pischon, T.; Berger, K.; Joost, H.G.; Häring, H.U.; Boeing, H.; Fritsche, A. Plasma fetuin-a levels and the risk of myocardial infarction and ischemic stroke. Circulation 2008, 118, 2555–2562. [Google Scholar] [CrossRef] [PubMed]
- Ketteler, M.; Bongartz, P.; Westenfeld, R.; Wildberger, J.E.; Mahnken, A.H.; Bohm, R.; Metzger, T.; Wanner, C.; Jahnen-Dechent, W.; Floege, J. Association of low fetuin-A (AHSG) concentrations in serum with cardiovascular mortality in patients on dialysis: A cross-sectional study. Lancet 2003, 361, 827–833. [Google Scholar] [CrossRef]
- Allison, M.A.; Criqui, M.H.; Wright, C.M. Patterns and risk factors for systemic calcified atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 331–336. [Google Scholar] [CrossRef] [PubMed]
- VanderLaan, P.A.; Reardon, C.A.; Getz, G.S. Site specificity of atherosclerosis: Site-selective responses to atherosclerotic modulators. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Dalager, S.; Paaske, W.P.; Kristensen, I.B.; Laurberg, J.M.; Falk, E. Artery-related differences in atherosclerosis expression: Implications for atherogenesis and dynamics in intima-media thickness. Stroke 2007, 38, 2698–2705. [Google Scholar] [CrossRef] [PubMed]
- Herisson, F.; Heymann, M.F.; Chetiveaux, M.; Charrier, C.; Battaglia, S.; Pilet, P.; Rouillon, T.; Krempf, M.; Lemarchand, P.; Heymann, D.; et al. Carotid and femoral atherosclerotic plaques show different morphology. Atherosclerosis 2011, 216, 348–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuo, Y.; Takumi, T.; Mathew, V.; Chung, W.Y.; Barsness, G.W.; Rihal, C.S.; Gulati, R.; McCue, E.T.; Holmes, D.R.; Eeckhout, E.; et al. Plaque characteristics and arterial remodeling in coronary and peripheral arterial systems. Atherosclerosis 2012, 223, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; Howard, V.J.; et al. Heart disease and stroke statistics--2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Meschiari, E.; Baldelli, E.; Musumeci, F.E.; Romagnoli, D.; Trenti, T.; Zennaro, R.G.; Lonardo, A.; Loria, P. Relationship of serum fetuin-A levels with coronary atherosclerotic burden and NAFLD in patients undergoing elective coronary angiography. Metab. Syndr. Relat. Disord. 2013, 11, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Morisco, F.; Pagliaro, L.; Caporaso, N.; Bianco, E.; Sagliocca, L.; Fargion, S.; Smedile, A.; Salvagnini, M.; Mele, A.; University of Naples Federico II, Italy. Consensus recommendations for managing asymptomatic persistent non-virus non-alcohol related elevation of aminotransferase levels: Suggestions for diagnostic procedures and monitoring. Dig. Liver Dis. 2008, 40, 585–598. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2010, 33 (Suppl. 1), S62–S69. [Google Scholar]
- ESH/ESC Task Force for the Management of Arterial Hypertension. 2013 Practice guidelines for the management of arterial hypertension of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC): ESH/ESC Task Force for the Management of Arterial Hypertension. J. Hypertens. 2013, 31, 1925–1938. [Google Scholar]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed]
- Ballestri, S.; Lonardo, A.; Romagnoli, D.; Carulli, L.; Losi, L.; Day, C.P.; Loria, P. Ultrasonographic fatty liver indicator, a novel score which rules out NASH and is correlated with metabolic parameters in NAFLD. Liver Int. 2012, 32, 1242–1252. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Romagnoli, D.; Nascimbeni, F.; Francica, G.; Lonardo, A. Role of ultrasound in the diagnosis and treatment of nonalcoholic fatty liver disease and its complications. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 603–627. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Nascimbeni, F.; Baldelli, E.; Marrazzo, A.; Romagnoli, D.; Targher, G.; Lonardo, A. Ultrasonographic fatty liver indicator detects mild steatosis and correlates with metabolic/histological parameters in various liver diseases. Metabolism 2017, 72, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.C.; Hung, H.F.; Lu, C.W.; Chang, H.H.; Lee, L.T.; Huang, K.C. Association of Non-alcoholic Fatty Liver Disease with Metabolic Syndrome Independently of Central Obesity and Insulin Resistance. Sci. Rep. 2016, 6, 27034. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Bertolini, L.; Padovani, R.; Rodella, S.; Tessari, R.; Zenari, L.; Day, C.; Arcaro, G. Prevalence of nonalcoholic fatty liver disease and its association with cardiovascular disease among type 2 diabetic patients. Diabetes Care 2007, 30, 1212–1218. [Google Scholar] [CrossRef] [PubMed]
- Arslan, U.; Turkoglu, S.; Balcioglu, S.; Tavil, Y.; Karakan T and Cengel, A. Association between nonalcoholic fatty liver disease and coronary artery disease. Coron. Artery Dis. 2007, 18, 433–436. [Google Scholar] [CrossRef] [PubMed]
- Sookoian, S.; Pirola, C.J. Non-alcoholic fatty liver disease is strongly associated with carotid atherosclerosis: A systematic review. J. Hepatol. 2008, 49, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Wong, G.L.; Yip, G.W.; Lo, A.O.; Limquiaco, J.; Chu, W.C.; Chim, A.M.; Yu, C.M.; Yu, J.; Chan, F.K.; et al. Coronary artery disease and cardiovascular outcomes in patients with non-alcoholic fatty liver disease. Gut 2011, 60, 1721–1727. [Google Scholar] [CrossRef] [PubMed]
- Choi, D.H.; Lee, S.J.; Kang, C.D.; Park, M.O.; Choi, D.W.; Kim, T.S.; Lee, W.; Cho, B.R.; Kim, Y.H.; Lee, B.K.; et al. Nonalcoholic fatty liver disease is associated with coronary artery disease in Koreans. World J. Gastroenterol. 2013, 19, 6453–6457. [Google Scholar] [CrossRef] [PubMed]
- Non-Alcoholic Fatty Liver Disease Study Group; Lonardo, A.; Bellentani, S.; Argo, C.K.; Ballestri, S.; Byrne, C.D.; Caldwell, S.H.; Cortez-Pinto, H.; Grieco, A.; Machado, M.V.; et al. Epidemiological modifiers of non-alcoholic fatty liver disease: Focus on high-risk groups. Dig. Liver Dis. 2015, 47, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Dunn, W.; Xu, R.; Wingard, D.L.; Rogers, C.; Angulo, P.; Younossi, Z.M.; Schwimmer, J.B. Suspected nonalcoholic fatty liver disease and mortality risk in a population-based cohort study. Am. J. Gastroenterol. 2008, 103, 2263–2271. [Google Scholar] [CrossRef] [PubMed]
- Bertolotti, M.; Lonardo, A.; Mussi, C.; Baldelli, E.; Pellegrini, E.; Ballestri, S.; Romagnoli, D.; Loria, P. Nonalcoholic fatty liver disease and aging: Epidemiology to management. World J. Gastroenterol. 2014, 20, 14185–14204. [Google Scholar] [CrossRef] [PubMed]
- Pal, D.; Dasgupta, S.; Kundu, R.; Maitra, S.; Das, G.; Mukhopadhyay, S.; Ray, S.; Majumdar, S.S.; Bhattacharya, S. Fetuin-A acts as an endogenous ligand of TLR4 to promote lipid-induced insulin resistance. Nat. Med. 2012, 18, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, P.; Seal, S.; Mukherjee, S.; Kundu, R.; Mukherjee, S.; Ray, S.; Mukhopadhyay, S.; Majumdar, S.S.; Bhattacharya, S. Adipocyte fetuin-A contributes to macrophage migration into adipose tissue and polarization of macrophages. J. Biol. Chem. 2013, 288, 28324–28330. [Google Scholar] [CrossRef] [PubMed]
- Trepanowski, J.F.; Mey, J.; Varady, K.A. Fetuin-A: A novel link between obesity and related complications. Int. J. Obes. 2015, 39, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Reinehr, T.; Roth, C.L. Fetuin-A and its relation to metabolic syndrome and fatty liver disease in obese children before and after weight loss. J. Clin. Endocrinol. Metab. 2008, 93, 4479–4485. [Google Scholar] [CrossRef] [PubMed]
- Malin, S.K.; Mulya, A.; Fealy, C.E.; Haus, J.M.; Pagadala, M.R.; Scelsi, A.R.; Huang, H.; Flask, C.A.; McCullough, A.J.; Kirwan, J.P. Fetuin-A is linked to improved glucose tolerance after short-term exercise training in nonalcoholic fatty liver disease. J. Appl. Physiol. 2013, 115, 988–994. [Google Scholar] [CrossRef] [PubMed]
- Dogru, T.; Genc, H.; Tapan, S.; Aslan, F.; Ercin, C.N.; Ors, F.; Kara, M.; Sertoglu, E.; Karslioglu, Y.; Bagci, S.; et al. Plasma fetuin-A is associated with endothelial dysfunction and subclinical atherosclerosis in subjects with nonalcoholic fatty liver disease. Clin. Endocrinol. 2013, 78, 712–717. [Google Scholar] [CrossRef] [PubMed]
- Ix, J.H.; Chertow, G.M.; Shlipak, G.M.; Brandenburg, V.M.; Ketteler, M.; Whooley, M.A. Fetuin-A and kidney function in persons with coronary artery disease—Data from the Heart and Soul Study. Nephrol. Dial. Transplant. 2006, 21, 2144–2151. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | Overall Study Population (n = 149) | Coronary Artery Disease Group (n =4 5) | Peripheral Arterial Disease Group (n = 104) | p |
|---|---|---|---|---|
| Age (years) | 72 (40–89) | 69 (40–89) | 73 (53–89) | 0.040 |
| Male sex (n (%)) | 116 (78) | 34 (76) | 82 (79) | 0.657 |
| BMI (Kg/m2) | 27 (19–43) | 27 (19–43) | 26 (20–35) | 0.211 |
| Waist circumference (cm) | 101 (70–133) | 100 (70–132) | 102 (76–133) | 0.447 |
| Type 2 diabetes mellitus (n (%)) | 53 (36) | 10 (22) | 43 (41) | 0.025 |
| Arterial hypertension (n (%)) | 138 (93) | 39 (87) | 99 (95) | 0.068 |
| Lipid lowering drugs (n (%)) | 92 (62) | 31 (69) | 61 (59) | 0.265 |
| Metabolic syndrome (n (%)) | 74 (50) | 19 (42) | 55 (53) | 0.232 |
| Smoking status (n (%)) Non-smokers Ex-smokers Active smokers | 30 (20) 62 (42) 57 (38) | 15 (33) 1 (2) 29 (64) | 15 (14) 61 (59) 28 (27) | <0.001 |
| US-FLI | 2 (0–8) | 0 (0–8) | 2 (0–8) | 0.038 |
| NAFLD (US-FLI ≥ 2) (n (%)) | 80 (54) | 19 (42) | 61 (59) | 0.065 |
| Glucose (mg/dL) | 103 (44–275) | 98 (64–197) | 108 (44–275) | 0.181 |
| HOMA-IR (mg/dL × μIU/mL) | 1.6 (0.2–18.5) | 1.3 (0.3–7.3) | 1.8 (0.2–18.5) | 0.009 |
| Total cholesterol (mg/dL) | 161 (68–296) | 175 (123–280) | 156 (68–296) | 0.023 |
| HDL cholesterol (mg/dL) | 40 (16–90) | 41 (16–77) | 40 (20–90) | 0.988 |
| Triglycerides (mg/dL) | 118 (37–451) | 116 (37–287) | 118 (57–451) | 0.291 |
| ALT (U/l) | 17 (1–268) | 23 (7–268) | 14 (1–74) | <0.001 |
| AST (U/l) | 19 (6–395) | 21 (12–395) | 19 (6–80) | 0.020 |
| GGT (U/l) | 30 (8–348) | 27 (13–105) | 34 (8–348) | 0.259 |
| Alkaline phospatase (U/l) | 77 (36–502) | 70 (36–502) | 82 (38–257) | 0.003 |
| Creatinine (mg/dL) | 1.0 (0.4–11.1) | 0.9 (0.6–3.0) | 1.0 (0.4–11.1) | 0.420 |
| eGFR (mL/min/1.73 m2) Cockroft–Gault equation eGFR ≥ 60 eGFR ≥ 30 and < 60 eGFR < 30 | 72 (4–170) 97 (66) 38 (26) 13 (9) | 79 (18–170) 34 (76) 7 (16) 4 (9) | 67 (4–145) 63 (61) 31 (30) 9 (9) | 0.070 0.168 |
| Platelets (1000/mL) | 198 (89–668) | 182 (104–320) | 207 (89–668) | 0.084 |
| Fetuin-A values (µg/mL) | 256 (111–662) | 378 (124–662) | 236 (111–461) | <0.001 |
| Parameter | OR (95% CI) | p |
|---|---|---|
| Fetuin-A * | 1.02 (1.01–1.02) | <0.001 |
| NAFLD (US-FLI ≥ 2) ** | 0.16 (0.05–0.50) | 0.002 |
| Age * | 0.96 (0.92–1.01) | 0.154 |
| Type 2 diabetes mellitus ** | 0.83 (0.28–2.40) | 0.723 |
| Total cholesterol * | 1.01 (1.00–1.02) | 0.111 |
| Parameter | Overall Study Population | Coronary Artery Disease Group | Peripheral Arterial Disease Group | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Fetuin-A * | 1.01 (1.00–1.01) | 0.024 | 1.01 (1.00–1.02) | 0.020 | 1.00 (1.00–1.01) | 0.353 |
| Coronary artery disease **§ | 0.16 (0.05–0.53) | 0.003 | - | - | - | - |
| Age * | 0.96 (0.92–1.00) | 0.067 | 0.94 (0.88–1.01) | 0.100 | 0.97 (0.92–1.03) | 0.294 |
| BMI * | 1.18 (1.06–1.31) | 0.003 | 1.40 (1.05–1.88) | 0.024 | 1.14 (1.00–1.29) | 0.045 |
| Type 2 diabetes mellitus ** | 3.40 (1.49–7.75) | 0.004 | 5.32 (0.75–37.75) | 0.094 | 3.09 (1.23–7.78) | 0.017 |
| Parameter | Overall Study Population | Coronary Artery Disease Group | Peripheral Arterial Disease Group | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Beta Coefficient | SE | p | Beta Coefficient | SE | p | Beta Coefficient | SE | p | |
| Coronary artery disease **§ | 131.36 | 16.52 | <0.001 | - | - | - | - | - | - |
| NAFLD (US-FLI ≥ 2) ** | 34.63 | 16.44 | 0.037 | 77.77 | 42.49 | 0.075 | 10.41 | 12.47 | 0.406 |
| Age * | −0.690 | 0.801 | 0.390 | −0.074 | 1.747 | 0.967 | −0.844 | 0.702 | 0.232 |
| BMI * | 0.059 | 1.939 | 0.976 | - | - | - | - | - | - |
| Total cholesterol * | −0.005 | 0.184 | 0.977 | - | - | - | - | - | - |
| Type 2 diabetes mellitus ** | −16.43 | 16.05 | 0.308 | −25.88 | 48.75 | 0.598 | −32.80 | 13.07 | 0.014 |
| Metabolic syndrome ** | - | - | - | 6.452 | 40.04 | 0.873 | 52.33 | 12.66 | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nascimbeni, F.; Romagnoli, D.; Ballestri, S.; Baldelli, E.; Lugari, S.; Sirotti, V.; Giampaoli, V.; Lonardo, A. Do Nonalcoholic Fatty Liver Disease and Fetuin-A Play Different Roles in Symptomatic Coronary Artery Disease and Peripheral Arterial Disease? Diseases 2018, 6, 17. https://doi.org/10.3390/diseases6010017
Nascimbeni F, Romagnoli D, Ballestri S, Baldelli E, Lugari S, Sirotti V, Giampaoli V, Lonardo A. Do Nonalcoholic Fatty Liver Disease and Fetuin-A Play Different Roles in Symptomatic Coronary Artery Disease and Peripheral Arterial Disease? Diseases. 2018; 6(1):17. https://doi.org/10.3390/diseases6010017
Chicago/Turabian StyleNascimbeni, Fabio, Dante Romagnoli, Stefano Ballestri, Enrica Baldelli, Simonetta Lugari, Valentina Sirotti, Valentina Giampaoli, and Amedeo Lonardo. 2018. "Do Nonalcoholic Fatty Liver Disease and Fetuin-A Play Different Roles in Symptomatic Coronary Artery Disease and Peripheral Arterial Disease?" Diseases 6, no. 1: 17. https://doi.org/10.3390/diseases6010017
APA StyleNascimbeni, F., Romagnoli, D., Ballestri, S., Baldelli, E., Lugari, S., Sirotti, V., Giampaoli, V., & Lonardo, A. (2018). Do Nonalcoholic Fatty Liver Disease and Fetuin-A Play Different Roles in Symptomatic Coronary Artery Disease and Peripheral Arterial Disease? Diseases, 6(1), 17. https://doi.org/10.3390/diseases6010017