Rapid Induction and Maintenance of Remission in Refractory Ulcerative Colitis with Ustekinumab


{kind=link}
{kind=link}
Abstract
:1. Introduction
Inflammatory Bowel Disease
2. Materials and Methods
2.1. Bioethics
2.2. Informed Consent
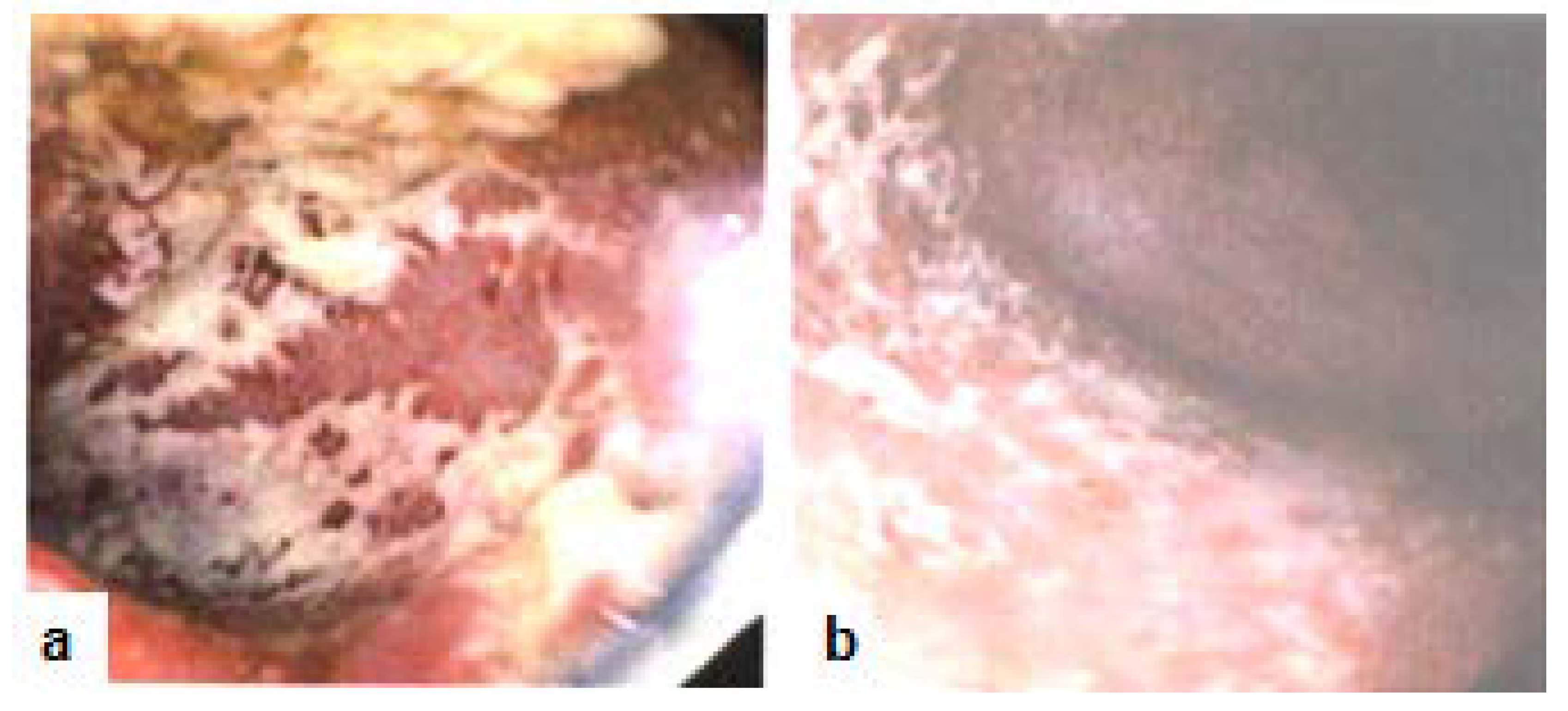
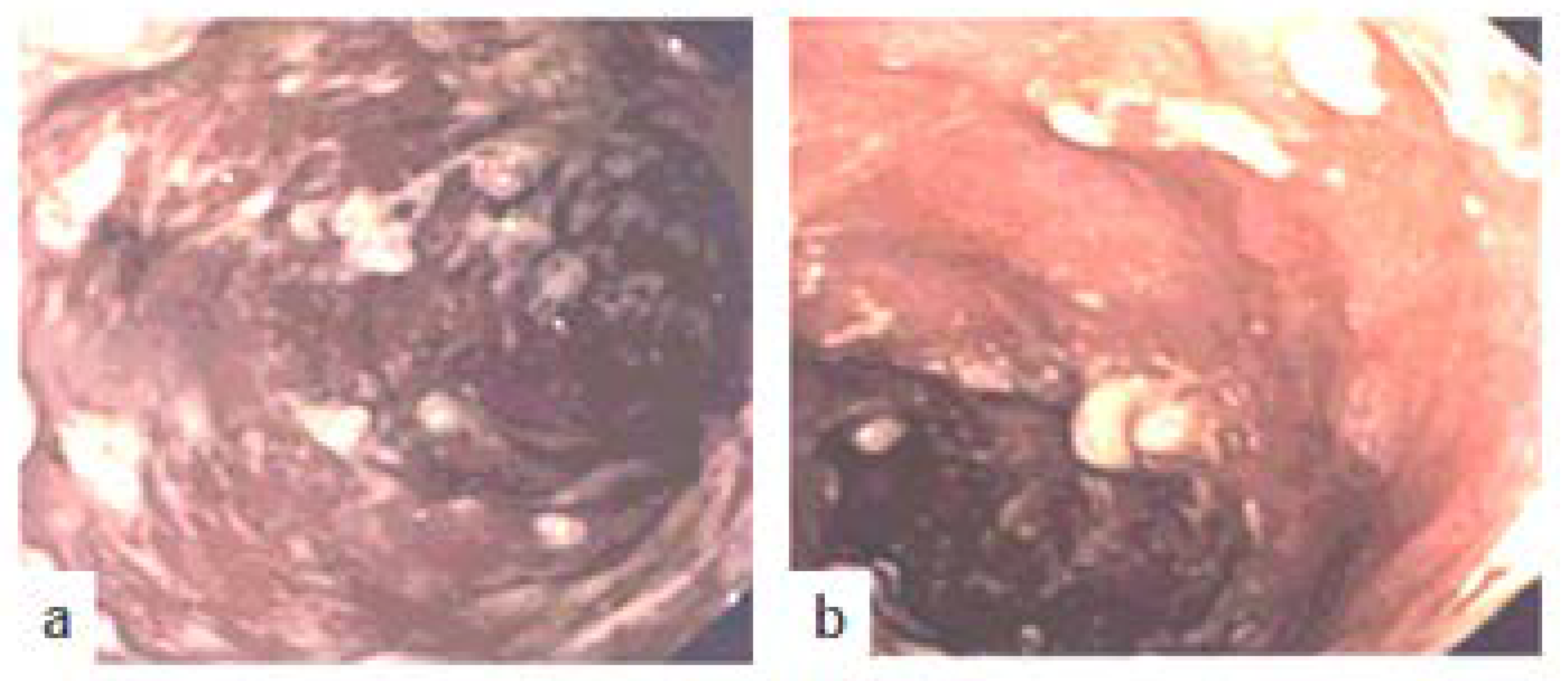
2.3. Colonoscopy Procedure
3. Background: Case Presentation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Uko, V.; Thangada, S.; Radhakr-Ishnan, K. Liver disorders in inflammatory bowel disease. Gastroenterol. Res. Pract. 2012. [Google Scholar] [CrossRef] [PubMed]
- Linares, V.; Alonso, V.; Domingo, J.L. Oxidative stress as a mechanism underlying sulfasalazine-inducedtoxicity. Expert Opin. Drug. Saf. 2011, 10, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Oz, H.S.; Chen, T.; de Villiers, W. Green Tea Polyphenols and Sulfasalazine have Parallel Anti-inflammatory Properties in Colitis Models. Front. Immunol. 2013, 4, 132. [Google Scholar] [CrossRef] [PubMed]
- Katsanos, K.H.; Papamichael, K.; Feuerstein, J.D.; Christodoulou, D.K.; Cheifetz, A.S. Biological therapies in inflammatory bowel disease: Beyond anti-TNF therapies. Clin. Immunol. 2018. [Google Scholar] [CrossRef] [PubMed]
- De Souza, H.S.; Fiocchi, C. Immunopathogenesis of IBD: Current state of the art. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Oz, H.S.; Ebersole, J.L. Application of prodrugs to inflammatory diseases of the gut. Molecules 2008, 13, 452–474. [Google Scholar] [CrossRef] [PubMed]
- Anser IFX (Infliximab) Drug Level—UI Health Care—University of Iowa. Available online: https://www.healthcare.uiowa.edu/path_handbook/handbook/test3182.html (accessed on 9 May 2018).
- Armuzzi, A.; Ardizzone, S.; Biancone, L.; Castiglione, F.; Danese, S.; Gionchetti, P.; Orlando, A.; Rizzello, F.; Scribano, M.L.; Vecchi, M.; et al. Ustekinumab in the management of Crohn’s disease: Expert opinion. Dig. Liver Dis. 2018, 50, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Sandborn, W.J.; Gasink, C.; Jacobstein, D.; Lang, Y.; Friedman, J.R.; Blank, M.A.; Johanns, J.; Gao, Lo.; Mia, Y.; et al. Ustekinumab as induction and maintenance therapy for Crohn’s Disease. N. Engl. J. Med. 2016, 375, 1946–1960. [Google Scholar] [CrossRef] [PubMed]
- Sands, B.E.; Chen, J.; Feagan, B.G.; Penney, M.; Rees, W.A.; Danese, S.; Higgins, P.D.R.; Newbold, P.; Faggioni, R.; Patra, K.; et al. Efficacy and safety of MEDI2070, an antibody against interleukin 23, in patients with moderate to severe Crohn’s Disease: A phase 2a study. Gastroenterology 2017, 153, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Sands, B.E.; Sandborn, W.J.; Panaccione, R.; O’Brien, C.; Zhang, H.; Johanns, J.; Peyrin-Biroulet, L.; van Assche, G.; Danese, S.; Targan, S.; et al. Safety and efficacy of ustekinumab induction therapy in patients with moderate to severe ulcerative colitis: Results from the Phase 3 UNIFI study. In Proceedings of the American College of Gastroenterology (ACG) Annual Scientific Meeting, Philadelphia, PN, USA, 5–10 October 2018. [Google Scholar]
- Wong, U.; Cross, R.K. Expert opinion on interleukin-12/23 and interleukin-23 antagonists as potential therapeutic options for the treatment of inflammatory bowel disease. Expert Opin. Investig. Drugs 2019, 18. [Google Scholar] [CrossRef] [PubMed]
- FDA approves Stelara® (ustekinumab) for treatment of adults with moderately to severely active Crohn’s disease. First Biologic that Targets Interleukin-12 and Interleukin-23 Cytokines for the Treatment of Crohn’s Disease. Available online: http://www.multivu.com/players/English/7883551-janssen-stelara-crohn-s-fda-approval/ (accessed on 26 September 2019).
- Ezzedine, K.; Visseaux, L.; Cadiot, G.; Brixi, H.; Bernard, P.; Reguiai, Z. Ustekinumab for skin reactions associated with anti-tumor necrosis factor-α agents in patients with inflammatory bowel diseases: A single-center retrospective study. J. Dermatol. 2019. [Google Scholar] [CrossRef] [PubMed]
- European Commission Approves Expanded Use of Janssen’s STELARA® (ustekinumab) for the Treatment of Moderately to Severely Active Ulcerative Colitis in the European Union. Business wire, Berkshire Hathaway Company. Available online: https://www.businesswire.com/news/home/20190904005566/en/European-Commission-Approves-Expanded-Janssen%E2%80%99s-STELARA%C2%AE-ustekinumab (accessed on 4 September 2019).


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, A.-Y.; Oz, H.S. Rapid Induction and Maintenance of Remission in Refractory Ulcerative Colitis with Ustekinumab. Diseases 2019, 7, 55. https://doi.org/10.3390/diseases7040055
Chen A-Y, Oz HS. Rapid Induction and Maintenance of Remission in Refractory Ulcerative Colitis with Ustekinumab. Diseases. 2019; 7(4):55. https://doi.org/10.3390/diseases7040055
Chicago/Turabian StyleChen, An-Yu, and Helieh S. Oz. 2019. "Rapid Induction and Maintenance of Remission in Refractory Ulcerative Colitis with Ustekinumab" Diseases 7, no. 4: 55. https://doi.org/10.3390/diseases7040055
APA StyleChen, A. -Y., & Oz, H. S. (2019). Rapid Induction and Maintenance of Remission in Refractory Ulcerative Colitis with Ustekinumab. Diseases, 7(4), 55. https://doi.org/10.3390/diseases7040055