Metabolomic Analysis of Severe Osteoarthritis in a Spanish Population of Women Compared to Healthy and Osteoporotic Subjects

 , , , , and
, , , , and 
Abstract
:
1. Introduction
2. Results
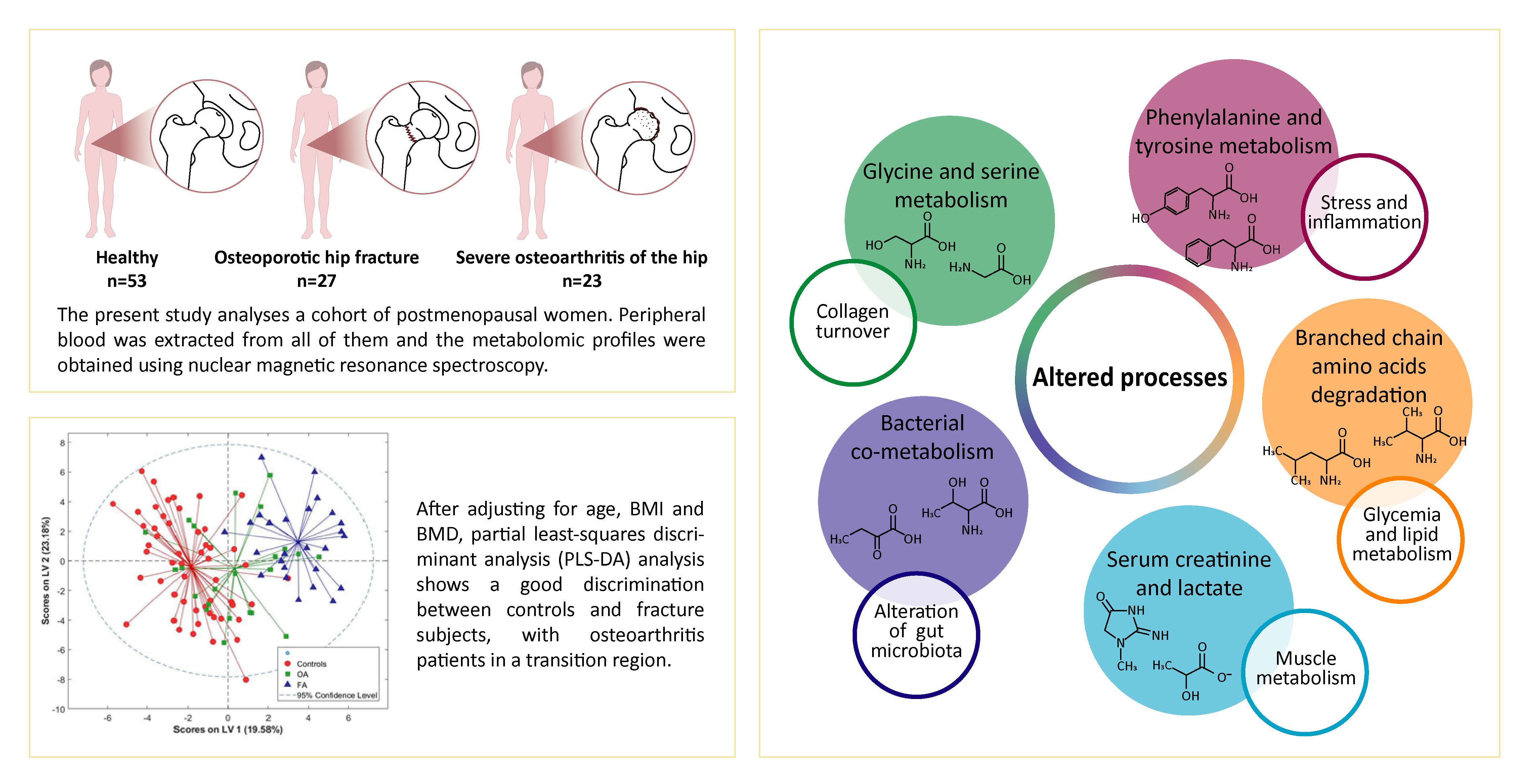
2.1. General Characteristics of the Population
2.2. Metabolic Profiles
3. Discussion
4. Experimental Design
4.1. Study Subjects
4.2. Anthropometric, Biochemical and Bone Density Measurements
4.3. NMR Metabolomics
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Briggs, A.M.; Cross, M.J.; Hoy, D.G.; Sànchez-Riera, L.; Blyth, F.M.; Woolf, A.D.; March, L. Musculoskeletal Health Conditions Represent a Global Threat to Healthy Aging: A Report for the 2015 World Health Organization World Report on Ageing and Health. Gerontologist 2016, 56, S243–S255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dequeker, J.; Aerssens, J.; Luyten, F.P. Osteoarthritis and Osteoporosis: Clinical and Research Evidence of Inverse Relationship. Aging Clin. Exp. Res. 2003, 15, 426–439. [Google Scholar] [CrossRef] [PubMed]
- Geusens, P.P.; Van Den Bergh, J.P. Osteoporosis and Osteoarthritis: Shared Mechanisms and Epidemiology. Curr. Opin. Rheumatol. 2016, 28, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Khosla, S.; Melton, L.J.; Riggs, B.L. The Unitary Model for Estrogen Deficiency and the Pathogenesis of Osteoporosis: Is a Revision Needed? J. Bone Miner. Res. 2011, 26, 441–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bliuc, D.; Nguyen, N.D.; Milch, V.E.; Nguyen, T.V.; Eisman, J.A.; Center, J.R. Mortality Risk Associated with Low-Trauma Osteoporotic Fracture and Subsequent Fracture in Men and Women. JAMA 2009, 301, 513–521. [Google Scholar] [CrossRef] [Green Version]
- Kanis, J.A.; McCloskey, E.V.; Johansson, H.; Cooper, C.; Rizzoli, R.; Reginster, J.-Y. European Guidance for the Diagnosis and Management of Osteoporosis in Postmenopausal Women. Osteoporos. Int. 2013, 24, 23–57. [Google Scholar] [CrossRef] [Green Version]
- Kanis, J.A.; Oden, A.; Johnell, O.; De Laet, C.; Jonsson, B.; Oglesby, A.K.; Parker, M.; Payne, B.; Rushton, N.; Hoszowski, K.; et al. The Components of Excess Mortality after Hip Fracture. Bone 2003, 32, 468–473. [Google Scholar] [CrossRef]
- Martel-Pelletier, J.; Barr, A.J.; Cicuttini, F.M.; Conaghan, P.G.; Cooper, C.; Goldring, M.B.; Goldring, S.R.; Jones, G.; Teichtahl, A.J.; Pelletier, J.P. Osteoarthritis. Nat. Rev. Dis. Primers 2016, 2, 16072. [Google Scholar] [CrossRef] [Green Version]
- Biomarkers Definitions Working Group. Biomarkers and Surrogate Endpoints: Preferred Definitions and Conceptual Framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar] [CrossRef]
- Munjal, A.; Bapat, S.; Hubbard, D.; Hunter, M.; Kolhe, R.; Fulzele, S. Advances in Molecular Biomarker for Early Diagnosis of Osteoarthritis. Biomol. Concepts 2019, 10, 111–119. [Google Scholar] [CrossRef]
- Johnson, C.H.; Ivanisevic, J.; Siuzdak, G. Metabolomics: Beyond Biomarkers and towards Mechanisms. Nat. Rev. Mol. Cell Biol. 2016, 17, 451–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pontes, T.A.; Barbosa, A.D.; Silva, R.D.; Melo-Junior, M.R.; Silva, R.O. Osteopenia-Osteoporosis Discrimination in Postmenopausal Women by 1H NMR-Based Metabonomics. PLoS ONE 2019, 14, e0217348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaggard, M.K.J.; Boulangé, C.L.; Akhbari, P.; Vaghela, U.; Bhattacharya, R.; Williams, H.R.T.; Lindon, J.C.; Gupte, C.M. A Systematic Review of the Small Molecule Studies of Osteoarthritis Using Nuclear Magnetic Resonance and Mass Spectroscopy. Osteoarthr. Cartil. 2019, 27, 560–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Testa, G.; Giardina, S.M.C.; Culmone, A.; Vescio, A.; Turchetta, M.; Cannavò, S.; Pavone, V. Intra-Articular Injections in Knee Osteoarthritis: A Review of Literature. J. Funct. Morphol. Kinesiol. 2021, 6, 15. [Google Scholar] [CrossRef]
- Bello, A.E.; Oesser, S. Collagen Hydrolysate for the Treatment of Osteoarthritis and Other Joint Disorders:A Review of the Literature. Curr. Med. Res. Opin. 2006, 22, 2221–2232. [Google Scholar] [CrossRef]
- Showiheen, S.A.A.; Sun, A.R.; Wu, X.; Crawford, R.; Xiao, Y.; Wellard, R.M.; Prasadam, I. Application of Metabolomics to Osteoarthritis: From Basic Science to the Clinical Approach. Curr. Rheumatol. Rep. 2019, 21, 26. [Google Scholar] [CrossRef]
- Duarte, J.M.N.; Do, K.Q.; Gruetter, R. Longitudinal Neurochemical Modifications in the Aging Mouse Brain Measured in Vivo by 1H Magnetic Resonance Spectroscopy. Neurobiol. Aging 2014, 35, 1660–1668. [Google Scholar] [CrossRef]
- Beaufrère, B.; Morio, B. Fat and Protein Redistribution with Aging: Metabolic Considerations. Eur. J. Clin. Nutr. 2000, 54, S48–S53. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.-H.; Tseng, Y.J.; Wang, S.-Y.; Tsai, Y.-S.; Chang, C.-S.; Kuo, T.-C.; Yao, W.-J.; Shieh, C.-C.; Wu, C.-H.; Kuo, P.-H. The Metabolome Profiling and Pathway Analysis in Metabolic Healthy and Abnormal Obesity. Int. J. Obes. 2015, 39, 1241–1248. [Google Scholar] [CrossRef]
- Capellino, S.; Cosentino, M.; Wolff, C.; Schmidt, M.; Grifka, J.; Straub, R.H. Catecholamine-Producing Cells in the Synovial Tissue during Arthritis: Modulation of Sympathetic Neurotransmitters as New Therapeutic Target. Ann. Rheum. Dis. 2010, 69, 1853–1860. [Google Scholar] [CrossRef]
- Pallares-Méndez, R.; Aguilar-Salinas, C.A.; Cruz-Bautista, I.; del Bosque-Plata, L. Metabolomics in Diabetes, a Review. Ann. Med. 2016, 48, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Zhai, G.; Wang-Sattler, R.; Hart, D.J.; Arden, N.K.; Hakim, A.J.; Illig, T.; Spector, T.D. Serum Branched-Chain Amino Acid to Histidine Ratio: A Novel Metabolomic Biomarker of Knee Osteoarthritis. Ann. Rheum. Dis. 2010, 69, 1227–1231. [Google Scholar] [CrossRef] [PubMed]
- Piva, S.R.; Susko, A.M.; Khoja, S.S.; Josbeno, D.A.; Fitzgerald, G.K.; Toledo, F.G.S. Links Between Osteoarthritis and Diabetes: Implications for Management from a Physical Activity Perspective. Clin. Geriatr. Med. 2015, 31, 67–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhury, T.; Bellamkonda, A.; Gousy, N.; Roy, P.D. The Association Between Diabetes Mellitus and Osteoarthritis: Does Diabetes Mellitus Play a Role in the Severity of Pain in Osteoarthritis? Cureus 2022, 14, e21449. [Google Scholar] [CrossRef]
- Adak, A.; Khan, M.R. An Insight into Gut Microbiota and Its Functionalities. Cell. Mol. Life Sci. 2019, 76, 473–493. [Google Scholar] [CrossRef]
- Biver, E.; Berenbaum, F.; Valdes, A.M.; Araujo de Carvalho, I.; Bindels, L.B.; Brandi, M.L.; Calder, P.C.; Castronovo, V.; Cavalier, E.; Cherubini, A.; et al. Gut Microbiota and Osteoarthritis Management: An Expert Consensus of the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Ageing Res. Rev. 2019, 55, 100946. [Google Scholar] [CrossRef]
- Lu, Y.; Fuerst, T.; Hui, S.; Genant, H.K. Standardization of Bone Mineral Density at Femoral Neck, Trochanter and Ward’s Triangle. Osteoporos. Int. 2001, 12, 438–444. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Subject Characteristics | Control (N = 53) | Osteoarthritis (N = 23) | Fracture (N = 27) | ANOVA p-Value |
|---|---|---|---|---|
| Age (years) | 70.02 ± 7.13 | 76.00 ± 9.49 (a) | 83.22 ± 7.73 (b, c) | <0.000 |
| Weight (Kg) | 69.50 ± 11.51 | 69.50 ± 15.13 | 68.62 ± 11.77 | 0.955 |
| Height (cm) | 157.67 ± 6.47 | 158.35 ± 6.25 | 157.00 ± 4.92 | 0.795 |
| BMI (kg/m2) | 28.04 ± 4.83 | 27.66 ± 5.53 | 27.81 ± 4.42 | 0.957 |
| FN-BMD (g/cm2) | 0.79 ± 0.16 | 0.87 ± 0.12 | 0.62 ± 0.11 (b, d) | <0.000 |
| FN T-score | −1.10 ± 1.43 | −0.22 ± 1.11 | −2.50 ± 0.97 (b, d) | <0.000 |
| FN Z-score | 0.23 ± 1.43 | 0.99 ± 1.15 | −0.80 ± 0.71 (b, d) | <0.000 |
| LS-BMD (g/cm2) | 1.01 ± 0.16 | 1.05 ± 0.18 | 0.95 ± 0.20 | 0.226 |
| LS T-score | −1.15 ± 1.44 | −0.78 ± 1.56 | −1.66 ± 1.70 | 0.240 |
| LS Z-score | 0.45 ± 1.58 | 0.75 ± 1.59 | 0.41 ± 1.70 | 0.803 |
| Metabolites | Control (N = 53) | Osteoarthritis (N = 23) | Fracture (N = 27) | ANOVA p-Value |
|---|---|---|---|---|
| CTx (ng/mL) | 0.347 ± 0.147 | 0.457 ± 0.156 (a) | 0.709 ± 0.306 (b, c) | <0.000 |
| Total ALP (U/L) | 88.4 ± 32.3 | 145.0 ± 81.1 (a) | 176.8 ± 96.4 (b) | <0.000 |
| 25(OH)D3 (ng/mL) | 35.3 ± 52.4 | 15.2 ± 9.1 | 14.8 ± 14.0 | 0.043 |
| Cholesterol (mg/dL) | 205.4 ± 32.8 | 158.4 ± 38.8 (b) | 141.9 ± 36.1 (b) | <0.000 |
| Triglycerides (mg/dL) | 105.1 ± 43.5 | 113.8 ± 43.3 | 115.2 ± 48.9 | 0.585 |
| HDL (mg/dL) | 62.8 ± 14.6 | 47.3 ± 13.9 (b) | 39.6 ± 9.1 (b) | <0.000 |
| LDL (mg/dL) | 124.8 ± 30.5 | 97.0 ± 25.1 (a) | 88.8 ± 27.8 (b) | <0.000 |
| Glucose (mg/dL) | 112.4 ± 31.4 | 109.3 ± 27.6 | 127.4 ± 30.4 | 0.100 |
| - | Metabolites- | Control | OA | FA | 3 Way | Control vs. OA | FA vs. OA | Control vs. FA | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (N = 53) | (N = 23) | (N = 27) | p-Value | p-Value | p-Value | p-Value | ||||||
| Amino acids | Mean ± SD | Mean ± SD | Mean ± SD | No Adj. | Adj. | No Adj. | Adj. | No Adj. | Adj | No Adj. | Adj. | |
| Isoleucine | 0.278 ± 0.90 | −0.032 ± 0.91 | −0.518 ± 1.08 | 0.003 | 0.087 | 0.174 | 0.164 | 0.096 | 0.639 | 0.001 | 0.105 | |
| Alanine | 0.367 ± 0.86 | −0.009 ± 0.95 | −0.713 ± 0.92 | 0.000 | 0.000 | 0.096 | 0.020 | 0.011 | 0.743 | 0.000 | 0.000 | |
| Leucine | 0.295 ± 0.93 | 0.039 ± 0.98 | −0.613 ± 0.90 | 0.000 | 0.001 | 0.280 | 0.062 | 0.018 | 0.594 | 0.000 | 0.000 | |
| Glutamate | 0.172 ± 1.05 | 0.101 ± 0.93 | −0.423 ± 0.86 | 0.035 | 0.045 | 0.783 | 0.443 | 0.043 | 0.716 | 0.013 | 0.012 | |
| Glutamine | 0.195 ± 1.03 | 0.080 ± 0.99 | −0.450 ± 0.82 | 0.021 | 0.018 | 0.652 | 0.306 | 0.044 | 0.782 | 0.006 | 0.005 | |
| Aspartate | 0.126 ± 1.02 | 0.027 ± 0.98 | −0.270 ± 0.96 | 0.246 | 0.360 | 0.698 | 0.419 | 0.284 | 0.289 | 0.099 | 0.129 | |
| Glycine | 0.241 ± 0.86 | −0.179 ± 1.23 | −0.320 ± 0.94 | 0.036 | 0.049 | 0.093 | 0.047 | 0.650 | 0.403 | 0.009 | 0.073 | |
| Threonine | 0.387 ± 0.83 | 0.003 ± 1.08 | −0.761 ± 0.80 | 0.000 | 0.000 | 0.097 | 0.057 | 0.006 | 0.838 | 0.000 | 0.000 | |
| Valine | 0.302 ± 0.87 | −0.064 ± 0.94 | −0.539 ± 1.08 | 0.001 | 0.042 | 0.104 | 0.081 | 0.107 | 0.648 | 0.000 | 0.067 | |
| Total creatine | −0.319 ± 0.80 | 0.124 ± 1.23 | 0.522 ± 0.92 | 0.001 | 0.026 | 0.066 | 0.054 | 0.198 | 0.543 | 0.000 | 0.023 | |
| Phenylalanine | 0.266 ± 0.68 | 0.229 ± 1.50 | −0.717 ± 0.60 | 0.000 | 0.000 | 0.883 | 0.015 | 0.004 | 0.694 | 0.000 | 0.000 | |
| Tyrosine | 0.433 ± 0.85 | −0.043 ± 0.97 | −0.813 ± 0.78 | 0.000 | 0.000 | 0.035 | 0.030 | 0.003 | 0.807 | 0.000 | 0.000 | |
| Cholesterol and lipoproteins | Cholesterol | 0.208 ± 1.09 | −0.034 ± 0.90 | −0.380 ± 0.80 | 0.043 | 0.549 | 0.352 | 0.507 | 0.156 | 0.981 | 0.015 | 0.557 |
| HDL apolipopr | 0.410 ± 0.87 | −0.023 ± 0.99 | −0.786 ± 0.77 | 0.000 | 0.001 | 0.060 | 0.057 | 0.004 | 0.780 | 0.000 | 0.001 | |
| Fatty acids | FA -CH3 | 0.255 ± 1.04 | −0.043 ± 0.86 | −0.464 ± 0.87 | 0.008 | 0.336 | 0.234 | 0.417 | 0.093 | 0.877 | 0.003 | 0.360 |
| FA BCH2 | 0.291 ± 0.90 | −0.026 ± 0.97 | −0.548 ± 1.01 | 0.001 | 0.014 | 0.173 | 0.082 | 0.070 | 0.672 | 0.000 | 0.012 | |
| FA =CH-CH2-CH2- | 0.341 ± 0.93 | −0.126 ± 0.94 | −0.562 ± 0.93 | 0.000 | 0.022 | 0.048 | 0.066 | 0.108 | 0.597 | 0.000 | 0.038 | |
| FA a-CH2 | 0.183 ± 0.96 | −0.061 ± 0.98 | −0.308 ± 1.04 | 0.108 | 0.142 | 0.316 | 0.189 | 0.394 | 0.504 | 0.039 | 0.087 | |
| FA-CH = CH | 0.180 ± 0.98 | −0.159 ± 1.02 | −0.218 ± 0.99 | 0.168 | 0.735 | 0.176 | 0.421 | 0.836 | 0.153 | 0.092 | 0.890 | |
| Valerate | 0.218 ± 0.99 | −0.035 ± 0.99 | −0.399 ± 0.94 | 0.031 | 0.031 | 0.308 | 0.149 | 0.189 | 0.804 | 0.009 | 0.015 | |
| Energy metabolism—glycolisis | Glucose | 0.188 ± 0.88 | 0.198 ± 1.32 | −0.537 ± 0.70 | 0.004 | 0.128 | 0.969 | 0.515 | 0.015 | 0.861 | 0.000 | 0.107 |
| Lactate | 0.314 ± 0.81 | −0.082 ± 1.10 | −0.546 ± 1.04 | 0.001 | 0.022 | 0.084 | 0.043 | 0.132 | 0.483 | 0.000 | 0.019 | |
| 2-phosphoglycerate | −0.224 ± 0.61 | −0.222 ± 1.26 | 0.628 ± 1.14 | 0.000 | 0.015 | 0.995 | 0.339 | 0.015 | 0.414 | 0.000 | 0.001 | |
| Energy metabolism—ketone bodies | 3-hydroxybutyrate | 0.253 ± 1.07 | −0.109 ± 0.84 | −0.403 ± 0.85 | 0.016 | 0.430 | 0.155 | 0.289 | 0.226 | 0.638 | 0.007 | 0.623 |
| Acetate | 0.409 ± 0.86 | −0.050 ± 0.95 | −0.760 ± 0.87 | 0.000 | 0.000 | 0.041 | 0.021 | 0.008 | 0.924 | 0.000 | 0.000 | |
| Fluid balance | Creatinine | 0.336 ± 0.88 | −0.007 ± 1.09 | −0.654 ± 0.84 | 0.000 | 0.004 | 0.151 | 0.105 | 0.022 | 0.701 | 0.000 | 0.002 |
| Inflammation | Glycoprotein A | 0.091 ± 0.86 | −0.072 ± 1.06 | −0.117 ± 1.21 | 0.634 | 0.783 | 0.480 | 0.458 | 0.892 | 0.196 | 0.378 | 0.975 |
| Bacterial co-metabolism | 4-hydroxybutyrate | 0.325 ± 0.92 | 0.020 ± 0.95 | −0.655 ± 0.90 | 0.000 | 0.001 | 0.192 | 0.064 | 0.013 | 0.690 | 0.000 | 0.000 |
| 2-aminobutyrate | 0.354 ± 0.89 | −0.009 ± 0.97 | −0.687 ± 0.90 | 0.000 | 0.000 | 0.116 | 0.031 | 0.014 | 0.980 | 0.000 | 0.000 | |
| 4-aminobutyrate | 0.406 ± 0.74 | 0.070 ± 1.05 | −0.856 ± 0.89 | 0.000 | 0.000 | 0.116 | 0.008 | 0.001 | 0.494 | 0.000 | 0.000 | |
| 2-oxobutyrate | 0.313 ± 0.93 | −0.040 ± 0.92 | −0.580 ± 0.97 | 0.001 | 0.071 | 0.131 | 0.148 | 0.050 | 0.751 | 0.000 | 0.105 | |
| N(CH3)3 | 0.375 ± 0.93 | −0.089 ± 1.00 | −0.659 ± 0.78 | 0.000 | 0.001 | 0.054 | 0.015 | 0.029 | 0.717 | 0.000 | 0.010 | |
| Dimethylamine | 0.056 ± 0.35 | 0.345 ± 1.97 | −0.404 ± 0.32 | 0.024 | 0.000 | 0.302 | 0.049 | 0.058 | 0.622 | 0.000 | 0.000 | |
| Phospholipids precursors | Phosphocholine | 0.275 ± 0.52 | 0.223 ± 1.63 | −0.730 ± 0.61 | 0.000 | 0.000 | 0.834 | 0.002 | 0.007 | 0.572 | 0.000 | 0.000 |
| Choline | 0.107 ± 0.76 | −0.029 ± 1.26 | −0.186 ± 1.17 | 0.462 | 0.634 | 0.562 | 0.733 | 0.650 | 0.895 | 0.179 | 0.265 | |
| Unknowns | U1 | 0.212 ± 0.93 | 0.223 ± 1.09 | −0.606 ± 0.82 | 0.001 | 0.002 | 0.965 | 0.959 | 0.004 | 0.252 | 0.000 | 0.000 |
| U2 | −0.203 ± 0.36 | 0.342 ± 1.96 | 0.107 ± 0.47 | 0.074 | 0.156 | 0.053 | 0.043 | 0.549 | 0.849 | 0.002 | 0.316 | |
| U3 | −0.091 ± 0.13 | 0.329 ± 2.10 | −0.102 ± 0.20 | 0.203 | 0.484 | 0.148 | 0.254 | 0.293 | 0.929 | 0.752 | 0.653 | |
| U4 | −0.413 ± 0.55 | 0.081 ± 1.03 | 0.742 ± 1.22 | 0.000 | 0.000 | 0.008 | 0.000 | 0.046 | 0.907 | 0.000 | 0.000 | |
| U5 | −0.184 ± 0.85 | 0.067 ± 0.99 | 0.303 ± 1.22 | 0.112 | 0.118 | 0.264 | 0.094 | 0.461 | 0.384 | 0.041 | 0.161 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pertusa, C.; Mifsut, D.; Morales, J.M.; Tarín, J.J.; Cano, A.; Monleón, D.; García-Pérez, M.Á. Metabolomic Analysis of Severe Osteoarthritis in a Spanish Population of Women Compared to Healthy and Osteoporotic Subjects. Metabolites 2022, 12, 677. https://doi.org/10.3390/metabo12080677
Pertusa C, Mifsut D, Morales JM, Tarín JJ, Cano A, Monleón D, García-Pérez MÁ. Metabolomic Analysis of Severe Osteoarthritis in a Spanish Population of Women Compared to Healthy and Osteoporotic Subjects. Metabolites. 2022; 12(8):677. https://doi.org/10.3390/metabo12080677
Chicago/Turabian StylePertusa, Clara, Damián Mifsut, José Manuel Morales, Juan J. Tarín, Antonio Cano, Daniel Monleón, and Miguel Ángel García-Pérez. 2022. "Metabolomic Analysis of Severe Osteoarthritis in a Spanish Population of Women Compared to Healthy and Osteoporotic Subjects" Metabolites 12, no. 8: 677. https://doi.org/10.3390/metabo12080677
APA StylePertusa, C., Mifsut, D., Morales, J. M., Tarín, J. J., Cano, A., Monleón, D., & García-Pérez, M. Á. (2022). Metabolomic Analysis of Severe Osteoarthritis in a Spanish Population of Women Compared to Healthy and Osteoporotic Subjects. Metabolites, 12(8), 677. https://doi.org/10.3390/metabo12080677