
Ethnic Disparities in Lipid Metabolism and Clinical Outcomes between Dutch South Asians and Dutch White Caucasians with Type 2 Diabetes Mellitus

 , ,
, , 
 and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Lipidomics Profiling Using the SLA Platform
2.3. 1H Nuclear Magnetic Resonance (NMR) Spectroscopy Measurement and Processing
2.4. Statistical Analyses
3. Results
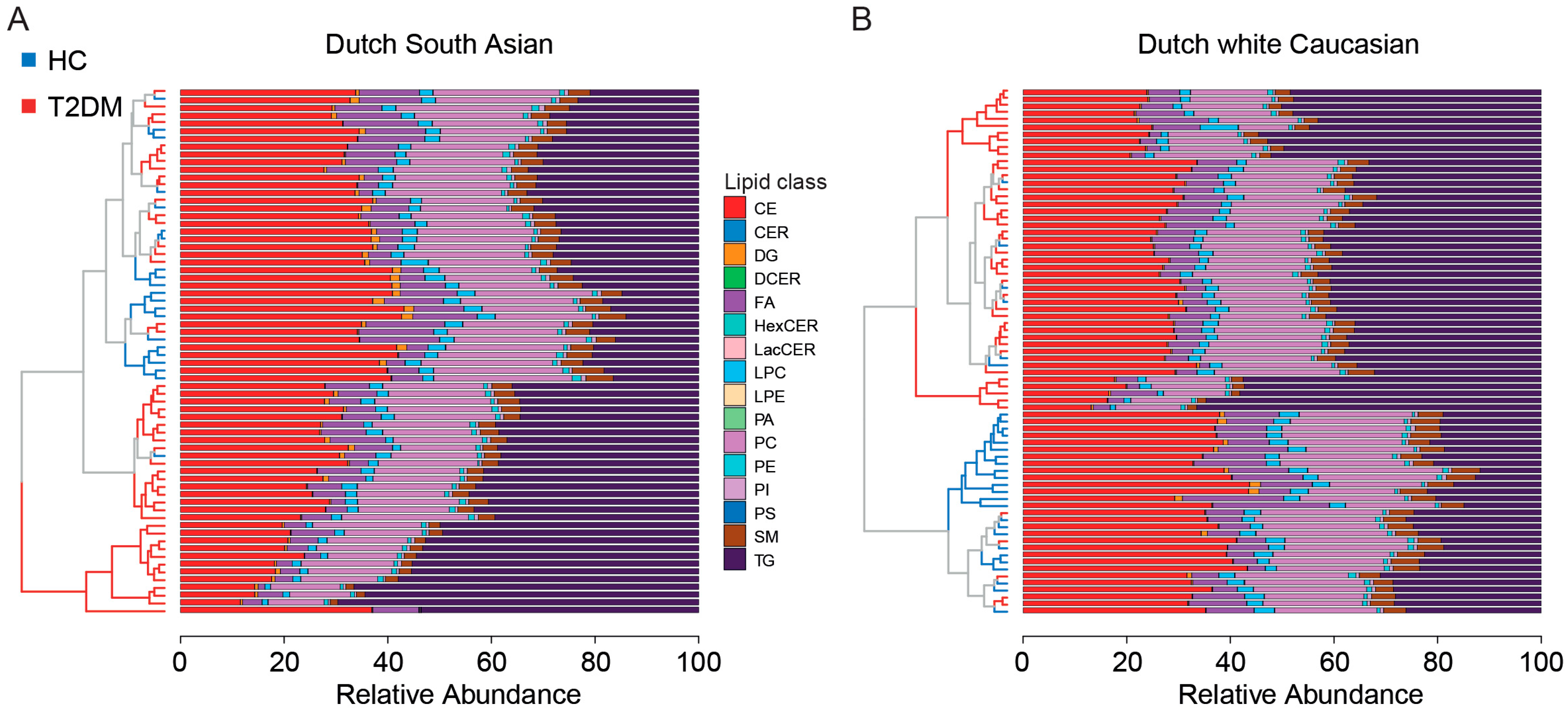
3.1. Pre-Processing of Plasma Lipidome Profiles of Individuals with T2DM vs. Healthy Participants
3.2. Healthy Individuals of Dutch South Asian Ethnicity Reveal a pre-Diabetes Lipid Class Profile
3.3. Comparison of Differential Lipids between Patients with T2DM and Healthy Controls in Two Ethnicities
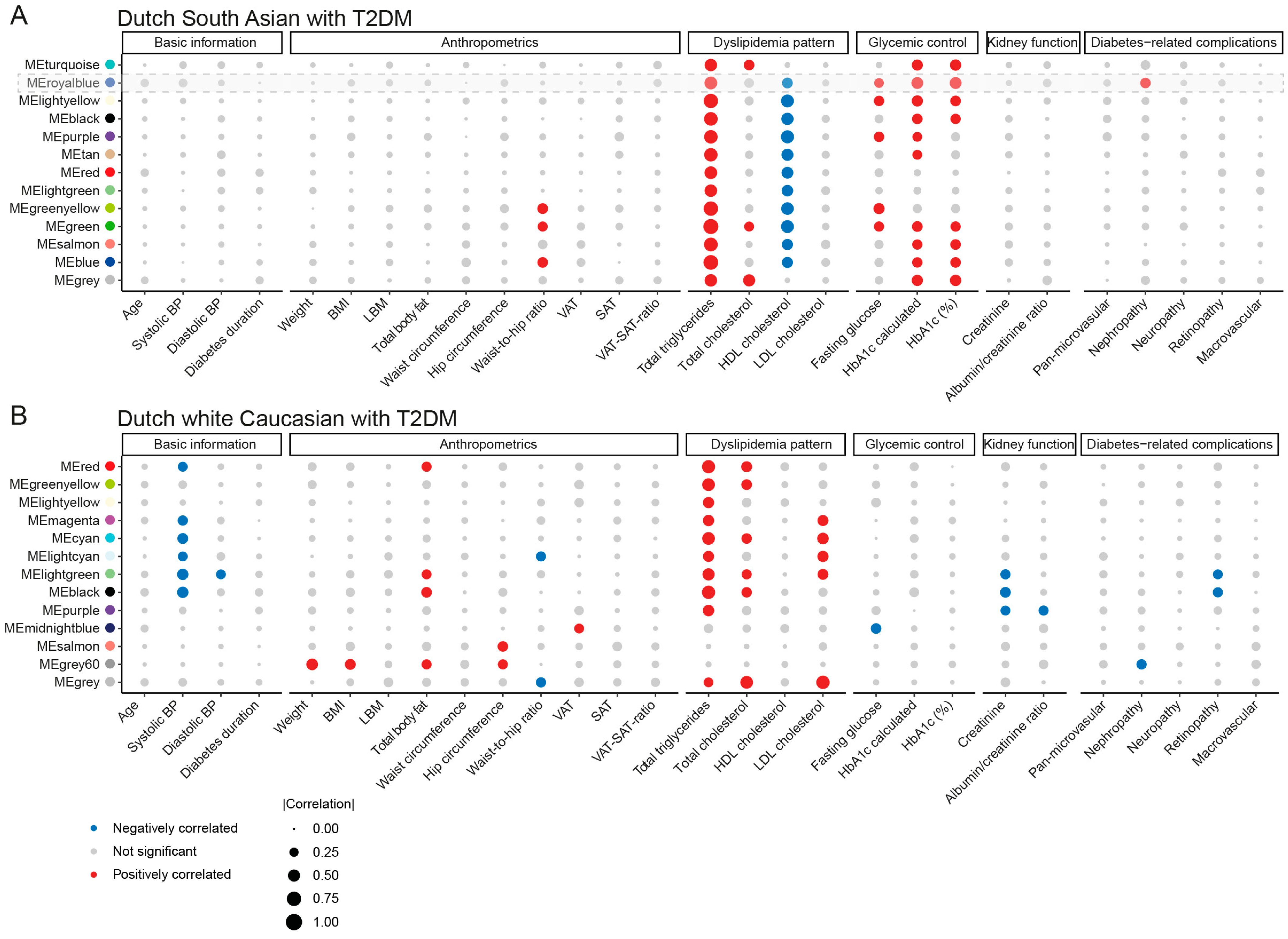
3.4. Ethnic Distinction in Associations of Lipid Correlation Network Modules with Clinical Features
3.5. Clinical Relevance Screening for Key Mediatory Lipids from Two Ethnicities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Unnikrishnan, R.; Pradeepa, R.; Joshi, S.R.; Mohan, V. Type 2 Diabetes: Demystifying the Global Epidemic. Diabetes 2017, 66, 1432–1442. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; Gill, J.M. Type 2 diabetes in migrant south Asians: Mechanisms, mitigation, and management. Lancet Diabetes Endocrinol. 2015, 3, 1004–1016. [Google Scholar] [CrossRef] [PubMed]
- Bakker, L.E.; Sleddering, M.A.; Schoones, J.W.; Meinders, A.E.; Jazet, I.M. Pathogenesis of type 2 diabetes in South Asians. Eur. J. Endocrinol. 2013, 169, R99–R114. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Autieri, M.V.; Scalia, R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am. J. Physiol. Cell Physiol. 2021, 320, C375–C391. [Google Scholar] [CrossRef] [PubMed]
- Chait, A.; den Hartigh, L.J. Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease. Front. Cardiovasc. Med. 2020, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Chandie Shaw, P.K.; Vandenbroucke, J.P.; Tjandra, Y.I.; Rosendaal, F.R.; Rosman, J.B.; Geerlings, W.; de Charro, F.T.; van Es, L.A. Increased end-stage diabetic nephropathy in Indo-Asian immigrants living in The Netherlands. Diabetologia 2002, 45, 337–341. [Google Scholar] [CrossRef]
- Chandie Shaw, P.K.; Baboe, F.; van Es, L.A.; van der Vijver, J.C.; van de Ree, M.A.; de Jonge, N.; Rabelink, T.J. South-Asian type 2 diabetic patients have higher incidence and faster progression of renal disease compared with Dutch-European diabetic patients. Diabetes Care 2006, 29, 1383–1385. [Google Scholar] [CrossRef]
- Wang, Y.L.; Koh, W.P.; Talaei, M.; Yuan, J.M.; Pan, A. Association between the ratio of triglyceride to high-density lipoprotein cholesterol and incident type 2 diabetes in Singapore Chinese men and women. J. Diabetes 2017, 9, 689–698. [Google Scholar] [CrossRef]
- Peng, J.; Zhao, F.; Yang, X.; Pan, X.; Xin, J.; Wu, M.; Peng, Y.G. Association between dyslipidemia and risk of type 2 diabetes mellitus in middle-aged and older Chinese adults: A secondary analysis of a nationwide cohort. BMJ Open 2021, 11, e042821. [Google Scholar] [CrossRef]
- Rao, H.; Jalali, J.A.; Johnston, T.P.; Koulen, P. Emerging Roles of Dyslipidemia and Hyperglycemia in Diabetic Retinopathy: Molecular Mechanisms and Clinical Perspectives. Front. Endocrinol. 2021, 12, 620045. [Google Scholar] [CrossRef]
- Hukportie, D.N.; Li, F.R.; Zhou, R.; Zheng, J.Z.; Wu, X.X.; Zou, M.C.; Wu, X.B. Lipid variability and risk of microvascular complications in Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial: A post hoc analysis. J. Diabetes 2022, 14, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Narindrarangkura, P.; Bosl, W.; Rangsin, R.; Hatthachote, P. Prevalence of dyslipidemia associated with complications in diabetic patients: A nationwide study in Thailand. Lipids Health Dis. 2019, 18, 90. [Google Scholar] [CrossRef]
- Frank, A.T.; Zhao, B.; Jose, P.O.; Azar, K.M.; Fortmann, S.P.; Palaniappan, L.P. Racial/ethnic differences in dyslipidemia patterns. Circulation 2014, 129, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Zakai, N.A.; Minnier, J.; Safford, M.M.; Koh, I.; Irvin, M.R.; Fazio, S.; Cushman, M.; Howard, V.J.; Pamir, N. Race-Dependent Association of High-Density Lipoprotein Cholesterol Levels With Incident Coronary Artery Disease. J. Am. Coll. Cardiol. 2022, 80, 2104–2115. [Google Scholar] [CrossRef]
- Su, B.; Bettcher, L.F.; Hsieh, W.Y.; Hornburg, D.; Pearson, M.J.; Blomberg, N.; Giera, M.; Snyder, M.P.; Raftery, D.; Bensinger, S.J.; et al. A DMS Shotgun Lipidomics Workflow Application to Facilitate High-Throughput, Comprehensive Lipidomics. J. Am. Soc. Mass. Spectrom. 2021, 32, 2655–2663. [Google Scholar] [CrossRef] [PubMed]
- Bizino, M.B.; Jazet, I.M.; Westenberg, J.J.M.; van Eyk, H.J.; Paiman, E.H.M.; Smit, J.W.A.; Lamb, H.J. Effect of liraglutide on cardiac function in patients with type 2 diabetes mellitus: Randomized placebo-controlled trial. Cardiovasc. Diabetol. 2019, 18, 55. [Google Scholar] [CrossRef] [PubMed]
- van Eyk, H.J.; Paiman, E.H.M.; Bizino, M.B.; de Heer, P.; Geelhoed-Duijvestijn, P.H.; Kharagjitsingh, A.V.; Smit, J.W.A.; Lamb, H.J.; Rensen, P.C.N.; Jazet, I.M. A double-blind, placebo-controlled, randomised trial to assess the effect of liraglutide on ectopic fat accumulation in South Asian type 2 diabetes patients. Cardiovasc. Diabetol. 2019, 18, 87. [Google Scholar] [CrossRef]
- Paiman, E.H.M.; van Eyk, H.J.; Bizino, M.B.; Dekkers, I.A.; de Heer, P.; Smit, J.W.A.; Jazet, I.M.; Lamb, H.J. Phenotyping diabetic cardiomyopathy in Europeans and South Asians. Cardiovasc. Diabetol. 2019, 18, 133. [Google Scholar] [CrossRef]
- Ghorasaini, M.; Mohammed, Y.; Adamski, J.; Bettcher, L.; Bowden, J.A.; Cabruja, M.; Contrepois, K.; Ellenberger, M.; Gajera, B.; Haid, M.; et al. Cross-Laboratory Standardization of Preclinical Lipidomics Using Differential Mobility Spectrometry and Multiple Reaction Monitoring. Anal. Chem. 2021, 93, 16369–16378. [Google Scholar] [CrossRef]
- Yuan, L.; Li-Gao, R.; Verhoeven, A.; van Eyk, H.J.; Bizino, M.B.; Rensen, P.C.N.; Giera, M.; Jazet, I.M.; Lamb, H.J.; Rabelink, T.J.; et al. Altered high-density lipoprotein composition is associated with risk for complications in type 2 diabetes mellitus in South Asian descendants: A cross-sectional, case-control study on lipoprotein subclass profiling. Diabetes Obes. Metab. 2023, 25, 2374–2387. [Google Scholar] [CrossRef]
- Lounila, J.; Ala-Korpela, M.; Jokisaari, J.; Savolainen, M.J.; Kesaniemi, Y.A. Effects of orientational order and particle size on the NMR line positions of lipoproteins. Phys. Rev. Lett. 1994, 72, 4049–4052. [Google Scholar] [CrossRef] [PubMed]
- Jeyarajah, E.J.; Cromwell, W.C.; Otvos, J.D. Lipoprotein particle analysis by nuclear magnetic resonance spectroscopy. Clin. Lab. Med. 2006, 26, 847–870. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Peng, J.; Zhou, Z.Y.; Duan, Y.; Chen, W.; Cai, B.; Yang, H.; Zhang, W. Establishing 1H nuclear magnetic resonance based metabonomics fingerprinting profile for spinal cord injury: A pilot study. Chin. Med. J. 2010, 123, 2315–2319. [Google Scholar] [PubMed]
- Straat, M.E.; Martinez-Tellez, B.; Nahon, K.J.; Janssen, L.G.M.; Verhoeven, A.; van der Zee, L.; Mulder, M.T.; Kooijman, S.; Boon, M.R.; van Lennep, J.E.R.; et al. Comprehensive (apo)lipoprotein profiling in patients with genetic hypertriglyceridemia using LC-MS and NMR spectroscopy. J. Clin. Lipidol. 2022, 16, 472–482. [Google Scholar] [CrossRef]
- Bakker, L.E.; Boon, M.R.; Annema, W.; Dikkers, A.; van Eyk, H.J.; Verhoeven, A.; Mayboroda, O.A.; Jukema, J.W.; Havekes, L.M.; Meinders, A.E.; et al. HDL functionality in South Asians as compared to white Caucasians. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Nodeland, M.; Klevjer, M.; Saether, J.; Giskeodegard, G.; Bathen, T.F.; Wisloff, U.; Bye, A. Atherogenic lipidomics profile in healthy individuals with low cardiorespiratory fitness: The HUNT3 fitness study. Atherosclerosis 2022, 343, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Langfelder, P.; Horvath, S. WGCNA: An R package for weighted correlation network analysis. BMC Bioinform. 2008, 9, 559. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Wu, Q.; Chen, W.; Zhu, L.; Liu, W.; Xia, F.; Sun, L.; Lin, X.; Zeng, R. Lipidomics reveals association of circulating lipids with body mass index and outcomes in IgA nephropathy patients. J. Mol. Cell Biol. 2021, 13, 565–575. [Google Scholar] [CrossRef]
- Narayan, K.M.V.; Kanaya, A.M. Why are South Asians prone to type 2 diabetes? A hypothesis based on underexplored pathways. Diabetologia 2020, 63, 1103–1109. [Google Scholar] [CrossRef]
- Razquin, C.; Toledo, E.; Clish, C.B.; Ruiz-Canela, M.; Dennis, C.; Corella, D.; Papandreou, C.; Ros, E.; Estruch, R.; Guasch-Ferre, M.; et al. Plasma Lipidomic Profiling and Risk of Type 2 Diabetes in the PREDIMED Trial. Diabetes Care 2018, 41, 2617–2624. [Google Scholar] [CrossRef]
- Suvitaival, T.; Bondia-Pons, I.; Yetukuri, L.; Poho, P.; Nolan, J.J.; Hyotylainen, T.; Kuusisto, J.; Oresic, M. Lipidome as a predictive tool in progression to type 2 diabetes in Finnish men. Metabolism 2018, 78, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Xuan, Q.; Hu, C.; Zhang, Y.; Wang, Q.; Zhao, X.; Liu, X.; Wang, C.; Jia, W.; Xu, G. Serum lipidomics profiles reveal potential lipid markers for prediabetes and type 2 diabetes in patients from multiple communities. Front. Endocrinol. 2022, 13, 966823. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Hu, Y.; An, Y.; Wang, Q.; Liu, J.; Wang, G. The Changes of Lipidomic Profiles Reveal Therapeutic Effects of Exenatide in Patients With Type 2 Diabetes. Front. Endocrinol. 2022, 13, 677202. [Google Scholar] [CrossRef] [PubMed]
- Taskinen, M.R. Insulin resistance and lipoprotein metabolism. Curr. Opin. Lipidol. 1995, 6, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Ginsberg, H.N. Increased very low density lipoprotein (VLDL) secretion, hepatic steatosis, and insulin resistance. Trends Endocrinol. Metab. 2011, 22, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Norton, L.; Shannon, C.; Gastaldelli, A.; DeFronzo, R.A. Insulin: The master regulator of glucose metabolism. Metabolism 2022, 129, 155142. [Google Scholar] [CrossRef]
- Ma, M.; Liu, H.; Yu, J.; He, S.; Li, P.; Ma, C.; Zhang, H.; Xu, L.; Ping, F.; Li, W.; et al. Triglyceride is independently correlated with insulin resistance and islet beta cell function: A study in population with different glucose and lipid metabolism states. Lipids Health Dis. 2020, 19, 121. [Google Scholar] [CrossRef]
- Yan, Y.Z.; Ma, R.L.; Zhang, J.Y.; He, J.; Ma, J.L.; Pang, H.R.; Mu, L.T.; Ding, Y.S.; Guo, H.; Zhang, M.; et al. Association of Insulin Resistance with Glucose and Lipid Metabolism: Ethnic Heterogeneity in Far Western China. Mediators Inflamm. 2016, 2016, 3825037. [Google Scholar] [CrossRef]
- Baek, J.; He, C.; Afshinnia, F.; Michailidis, G.; Pennathur, S. Lipidomic approaches to dissect dysregulated lipid metabolism in kidney disease. Nat. Rev. Nephrol. 2022, 18, 38–55. [Google Scholar] [CrossRef]
- Chen, H.; Chen, L.; Liu, D.; Chen, D.Q.; Vaziri, N.D.; Yu, X.Y.; Zhang, L.; Su, W.; Bai, X.; Zhao, Y.Y. Combined Clinical Phenotype and Lipidomic Analysis Reveals the Impact of Chronic Kidney Disease on Lipid Metabolism. J. Proteome Res. 2017, 16, 1566–1578. [Google Scholar] [CrossRef]
- Ehtisham, S.; Crabtree, N.; Clark, P.; Shaw, N.; Barrett, T. Ethnic differences in insulin resistance and body composition in United Kingdom adolescents. J. Clin. Endocrinol. Metab. 2005, 90, 3963–3969. [Google Scholar] [CrossRef] [PubMed]
- Gujral, U.P.; Pradeepa, R.; Weber, M.B.; Narayan, K.M.; Mohan, V. Type 2 diabetes in South Asians: Similarities and differences with white Caucasian and other populations. Ann. N. Y Acad. Sci. 2013, 1281, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, Y.; Shirai, K. Clinical determination of the severity of metabolic syndrome: Preheparin lipoprotein lipase mass as a new marker of metabolic syndrome. Curr. Med. Chem. Cardiovasc. Hematol. Agents 2005, 3, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Li, X.; Wang, M.; Ning, H.; A, L.; Li, Y.; Sun, C. Lipoprotein lipase links vitamin D, insulin resistance, and type 2 diabetes: A cross-sectional epidemiological study. Cardiovasc. Diabetol. 2013, 12, 17. [Google Scholar] [CrossRef] [PubMed]
- Camporez, J.P.; Jornayvaz, F.R.; Petersen, M.C.; Pesta, D.; Guigni, B.A.; Serr, J.; Zhang, D.; Kahn, M.; Samuel, V.T.; Jurczak, M.J.; et al. Cellular mechanisms by which FGF21 improves insulin sensitivity in male mice. Endocrinology 2013, 154, 3099–3109. [Google Scholar] [CrossRef] [PubMed]
- Camporez, J.P.G.; Kanda, S.; Petersen, M.C.; Jornayvaz, F.R.; Samuel, V.T.; Bhanot, S.; Petersen, K.F.; Jurczak, M.J.; Shulman, G.I. ApoA5 knockdown improves whole-body insulin sensitivity in high-fat-fed mice by reducing ectopic lipid content. J. Lipid Res. 2015, 56, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Kumashiro, N.; Erion, D.M.; Zhang, D.; Kahn, M.; Beddow, S.A.; Chu, X.; Still, C.D.; Gerhard, G.S.; Han, X.; Dziura, J.; et al. Cellular mechanism of insulin resistance in nonalcoholic fatty liver disease. Proc. Natl. Acad. Sci. USA 2011, 108, 16381–16385. [Google Scholar] [CrossRef]
- Jornayvaz, F.R.; Shulman, G.I. Diacylglycerol activation of protein kinase Cepsilon and hepatic insulin resistance. Cell Metab. 2012, 15, 574–584. [Google Scholar] [CrossRef]
- Luukkonen, P.K.; Zhou, Y.; Sadevirta, S.; Leivonen, M.; Arola, J.; Oresic, M.; Hyotylainen, T.; Yki-Jarvinen, H. Hepatic ceramides dissociate steatosis and insulin resistance in patients with non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1167–1175. [Google Scholar] [CrossRef]
- Ter Horst, K.W.; Gilijamse, P.W.; Versteeg, R.I.; Ackermans, M.T.; Nederveen, A.J.; la Fleur, S.E.; Romijn, J.A.; Nieuwdorp, M.; Zhang, D.; Samuel, V.T.; et al. Hepatic Diacylglycerol-Associated Protein Kinase Cepsilon Translocation Links Hepatic Steatosis to Hepatic Insulin Resistance in Humans. Cell Rep. 2017, 19, 1997–2004. [Google Scholar] [CrossRef]
- Wang, Q.J. PKD at the crossroads of DAG and PKC signaling. Trends Pharmacol. Sci. 2006, 27, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Noh, H.; King, G.L. The role of protein kinase C activation in diabetic nephropathy. Kidney Int. 2007, S49–S53. [Google Scholar] [CrossRef] [PubMed]
- Pan, D.; Xu, L.; Guo, M. The role of protein kinase C in diabetic microvascular complications. Front. Endocrinol. 2022, 13, 973058. [Google Scholar] [CrossRef] [PubMed]
- Zethof, M.; Mosterd, C.M.; Collard, D.; Galenkamp, H.; Agyemang, C.; Nieuwdorp, M.; van Raalte, D.H.; van den Born, B.H. Differences in Body Composition Convey a Similar Risk of Type 2 Diabetes Among Different Ethnic Groups With Disparate Cardiometabolic Risk-The HELIUS Study. Diabetes Care 2021, 44, 1692–1698. [Google Scholar] [CrossRef] [PubMed]
- Augustine, J.; Troendle, E.P.; Barabas, P.; McAleese, C.A.; Friedel, T.; Stitt, A.W.; Curtis, T.M. The Role of Lipoxidation in the Pathogenesis of Diabetic Retinopathy. Front. Endocrinol. 2020, 11, 621938. [Google Scholar] [CrossRef] [PubMed]
- Reis, A.; Rocha, S.; Dias, I.H.; Costa, R.; Soares, R.; Sanchez-Quesada, J.L.; Perez, A.; de Freitas, V. Type 2 Diabetes mellitus alters the cargo of (poly)phenol metabolome and the oxidative status in circulating lipoproteins. Redox Biol. 2023, 59, 102572. [Google Scholar] [CrossRef] [PubMed]
- Calzada, C.; Vors, C.; Penhoat, A.; Cheillan, D.; Michalski, M.C. Role of circulating sphingolipids in lipid metabolism: Why dietary lipids matter. Front. Nutr. 2022, 9, 1108098. [Google Scholar] [CrossRef]
- Vesper, H.; Schmelz, E.M.; Nikolova-Karakashian, M.N.; Dillehay, D.L.; Lynch, D.V.; Merrill, A.H., Jr. Sphingolipids in food and the emerging importance of sphingolipids to nutrition. J. Nutr. 1999, 129, 1239–1250. [Google Scholar] [CrossRef]
- Brussaard, J.H.; van Erp-Baart, M.A.; Brants, H.A.; Hulshof, K.F.; Lowik, M.R. Nutrition and health among migrants in The Netherlands. Public. Health Nutr. 2001, 4, 659–664. [Google Scholar] [CrossRef]
- Dekker, L.H.; van Dam, R.M.; Snijder, M.B.; Peters, R.J.; Dekker, J.M.; de Vries, J.H.; de Boer, E.J.; Schulze, M.B.; Stronks, K.; Nicolaou, M. Comparable Dietary Patterns Describe Dietary Behavior across Ethnic Groups in The Netherlands, but Different Elements in the Diet Are Associated with Glycated Hemoglobin and Fasting Glucose Concentrations. J. Nutr. 2015, 145, 1884–1891. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuan, L.; Verhoeven, A.; Blomberg, N.; van Eyk, H.J.; Bizino, M.B.; Rensen, P.C.N.; Jazet, I.M.; Lamb, H.J.; Rabelink, T.J.; Giera, M.; et al. Ethnic Disparities in Lipid Metabolism and Clinical Outcomes between Dutch South Asians and Dutch White Caucasians with Type 2 Diabetes Mellitus. Metabolites 2024, 14, 33. https://doi.org/10.3390/metabo14010033
Yuan L, Verhoeven A, Blomberg N, van Eyk HJ, Bizino MB, Rensen PCN, Jazet IM, Lamb HJ, Rabelink TJ, Giera M, et al. Ethnic Disparities in Lipid Metabolism and Clinical Outcomes between Dutch South Asians and Dutch White Caucasians with Type 2 Diabetes Mellitus. Metabolites. 2024; 14(1):33. https://doi.org/10.3390/metabo14010033
Chicago/Turabian StyleYuan, Lushun, Aswin Verhoeven, Niek Blomberg, Huub J. van Eyk, Maurice B. Bizino, Patrick C. N. Rensen, Ingrid M. Jazet, Hildo J. Lamb, Ton J. Rabelink, Martin Giera, and et al. 2024. "Ethnic Disparities in Lipid Metabolism and Clinical Outcomes between Dutch South Asians and Dutch White Caucasians with Type 2 Diabetes Mellitus" Metabolites 14, no. 1: 33. https://doi.org/10.3390/metabo14010033
APA StyleYuan, L., Verhoeven, A., Blomberg, N., van Eyk, H. J., Bizino, M. B., Rensen, P. C. N., Jazet, I. M., Lamb, H. J., Rabelink, T. J., Giera, M., & van den Berg, B. M. (2024). Ethnic Disparities in Lipid Metabolism and Clinical Outcomes between Dutch South Asians and Dutch White Caucasians with Type 2 Diabetes Mellitus. Metabolites, 14(1), 33. https://doi.org/10.3390/metabo14010033