

Molecular Biomarkers in Ocular Graft-versus-Host Disease: A Systematic Review
 ,
,
Abstract
:1. Introduction
2. Methods
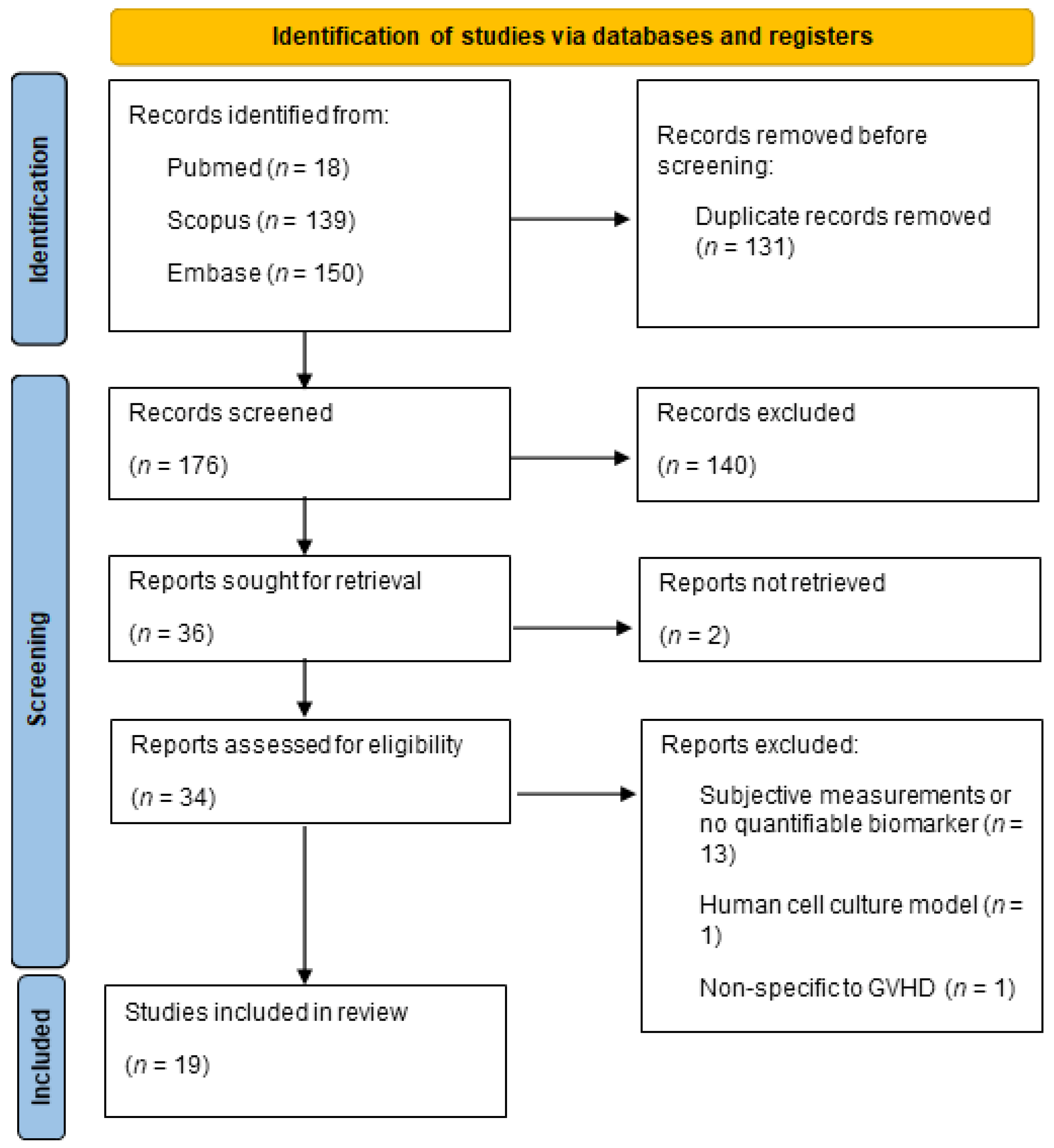
2.1. Search Strategy
- (“ocular graft-versus-host disease” OR “ocular chronic graft-versus-host disease” OR “ocular cGVHD” OR “oGVHD” OR “ocular GVHD” OR “ocular graft versus host disease”) AND (biomark* OR cytokin* OR chemok* OR proteom* OR genom* OR transcriptom* OR metabolom* OR lipidom* OR “immune response” OR “immune profile” OR inflamm* OR “tear film” OR “ocular surface” OR “conjunctiva” OR “cornea” OR “lacrimal gland” OR “meibomian gland” OR “dry eye” OR “macula*” OR “fundus” OR “imaging modalit*” OR “optical coherence tomograph*” OR “OCT” OR “in vivo confocal microscop*” OR “corneal topograph*” OR “fluorescein angiograph*” OR “indocyanine green angiograph*” OR “fundus photograph*” OR “ultrasound biomicroscop*” OR “scanning laser ophthalmoscop*” OR “multimodal imag*” OR “imaging technique*”).
- (“chronic graft-versus-host disease” OR “acute graft-versus-host disease”) AND (“conjunctiva” OR “cornea” OR “lacrimal gland” OR “meibomian gland” OR “dry eye” OR “macula*” OR “fundus”) AND (biomark* OR cytokin* OR chemok* OR proteom* OR genom* OR transcriptom* OR metabolom* OR lipidom* OR “immune response*” OR “immune profile*” OR inflamm* OR “tear film” OR “ocular surface” OR “imaging modalit*” OR “optical coherence tomograph*” OR “OCT” OR “in vivo confocal microscop*” OR “corneal topograph*” OR “fluorescein angiograph*” OR “indocyanine green angiograph*” OR “fundus photograph*” OR “ultrasound biomicroscop*” OR “scanning laser ophthalmoscop*” OR “multimodal imag*” OR “imaging technique*”).
2.2. Selection Criteria
2.3. Data Extraction and Quality Assessment
3. Results
Quality Assessment
4. Discussion
4.1. Tears as a Valuable Resource for Biomarker Analysis
4.2. Cytokine Profile in Tears
4.3. Proteomic Profile in Tears
4.4. Lipid Profile in Tears
4.5. Leukocyte Profile in Tears
4.6. Microflora Profile on the Ocular Surface
4.7. Clinical Findings as Biomarkers
4.8. Limitations and Future Implications
Funding
Data Availability Statement
Conflicts of Interest
References
- Strimbu, K.; Tavel, J.A. What are biomarkers? Curr. Opin. HIV AIDS 2010, 5, 463–466. [Google Scholar] [CrossRef]
- Justiz Vaillant, A.A.; Modi, P.; Mohammadi, O. Graft-Versus-Host Disease. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK538235/ (accessed on 10 October 2022).
- Ogawa, Y.; Kim, S.K.; Dana, R.; Clayton, J.; Jain, S.; Rosenblatt, M.I.; Perez, V.L.; Shikari, H.; Riemens, A.; Tsubota, K. International Chronic Ocular Graft-vs-Host-Disease (GVHD) Consensus Group: Proposed diagnostic criteria for chronic GVHD (Part I). Sci. Rep. 2013, 3, 3419. [Google Scholar] [CrossRef]
- Jagasia, M.H.; Greinix, H.T.; Arora, M.; Williams, K.M.; Wolff, D.; Cowen, E.W.; Palmer, J.; Weisdorf, D.; Treister, N.S.; Cheng, G.-S.; et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group Report. Biol. Blood Marrow Transplant. 2015, 21, 389–401.e1. [Google Scholar] [CrossRef]
- Soleimani, M.; Sharif, P.M.; Cheraqpour, K.; Koganti, R.; Masoumi, A.; Baharnoori, S.M.; Salabati, M.; Djalilian, A.R. Ocular graft-versus-host disease (oGVHD): From A to Z. Surv. Ophthalmol. 2023, 68, 697–712. [Google Scholar] [CrossRef]
- Choi, W.; Ha, J.Y.; Li, Y.; Choi, J.H.; Ji, Y.S.; Yoon, K.C. Comparison of the meibomian gland dysfunction in patients with chronic ocular graft-versus-host disease and Sjögren’s syndrome. Int. J. Ophthalmol. 2019, 12, 393–400. [Google Scholar] [CrossRef]
- Bernabei, F.; Versura, P.B.; Pellegrini, M.; Moscardelli, F.C.; Bonifazi, F.; Sessa, M.; Arpinati, M.; Scorcia, V.; Giannaccare, G.M. Longitudinal Analysis of Infrared Meibography in Patients Undergoing Hematopoietic Stem Cell Transplantation. Cornea 2020, 39, 812–817. [Google Scholar] [CrossRef]
- Dikmetas, O.; Kocabeyoglu, S.; Mocan, M.C. The Association between Meibomian Gland Atrophy and Corneal Subbasal Nerve Loss in Patients with Chronic Ocular Graft-versus-host Disease. Curr. Eye Res. 2021, 46, 796–801. [Google Scholar] [CrossRef]
- Zhao, W.; Yang, J.; Liao, Y.; Lao, H.Y.; Huang, Q.; Jin, L.; Sun, J.; Huang, F.; Liang, L. Comparable meibomian gland changes in patients with and without ocular graft-versus-host disease after hematopoietic stem cell transplantation. Ocul. Surf. 2022, 25, 1–7. [Google Scholar] [CrossRef]
- Hwang, H.S.; Ha, M.; Kim, H.-S.; Na, K.-S. Longitudinal analysis of meibomian gland dropout in patients with ocular graft-versus-host disease. Ocul. Surf. 2019, 17, 464–469. [Google Scholar] [CrossRef]
- Shamloo, K.; Mistry, P.; Barbarino, A.; Ross, C.; Jhanji, V.; Sharma, A. Differential Effect of Proinflammatory Cytokines on Corneal and Conjunctival Epithelial Cell Mucins and Glycocalyx. Transl. Vis. Sci. Technol. 2021, 10, 17. [Google Scholar] [CrossRef]
- Tong, L.; Lim, E.W.L.; Yeo, S.W.J.; Hou, A.; Linn, Y.C.; Ho, A.; Than, H.; Quek, J.K.S.; Hwang, W.Y.K.; Lim, F.L.W.I.; et al. Conjunctival T Cell Profile in Allogeneic Hematopoietic Stem Cell Transplant Patients after Instilling Topical Cyclosporine-A 0.1% Cationic Emulsion. Ophthalmol. Ther. 2023, 12, 1547–1567. [Google Scholar] [CrossRef]
- Gerber-Hollbach, N.; Plattner, K.; O’Leary, O.E.; Jenoe, P.; Moes, S.; Drexler, B.; Schoetzau, A.; Halter, J.P.; Goldblum, D. Tear Film Proteomics Reveal Important Differences Between Patients with and Without Ocular GvHD After Allogeneic Hematopoietic Cell Transplantation. Investig. Ophthalmol. Vis. Sci. 2018, 59, 3521–3530. [Google Scholar] [CrossRef]
- Hu, B.; Qiu, Y.; Hong, J. Tear cytokine levels in the diagnosis and severity assessment of ocular chronic graft-versus-host disease (GVHD). Ocul. Surf. 2020, 18, 298–304. [Google Scholar] [CrossRef]
- Pietraszkiewicz, A.A.; Payne, D.; Abraham, M.; Garced, A.; Devarasetty, K.C.; Wall, M.; Menezes, S.M.; Ugarte, S.; Pirsl, F.; Goklemez, S.; et al. Ocular surface indicators and biomarkers in chronic ocular graft-versus-host disease: A prospective cohort study. Bone Marrow Transplant. 2021, 56, 1850–1858, Erratum in Bone Marrow Transplant. 2021, 56, 2040–2041. [Google Scholar] [CrossRef]
- An, S.; Raju, I.; Surenkhuu, B.; Kwon, J.-E.; Gulati, S.; Karaman, M.; Pradeep, A.; Sinha, S.; Mun, C.; Jain, S. Neutrophil extracellular traps (NETs) contribute to pathological changes of ocular graft-vs.-host disease (oGVHD) dry eye: Implications for novel biomarkers and therapeutic strategies. Ocul. Surf. 2019, 17, 589–614. [Google Scholar] [CrossRef]
- Ciavarella, C.; Astolfi, G.; Valsecchi, N.; Barbato, F.; Arpinati, M.; Bonifazi, F.; Versura, P. Longitudinal Tear Protein Changes Correlate with Ocular Chronic GVHD Development in Allogeneic Hematopoietic Stem Cell Transplant Patients. Appl. Sci. 2021, 11, 8221. [Google Scholar] [CrossRef]
- Liu, S.; Peng, R.; Ma, J.; Shen, Z.; Hu, B.; Zhao, Y.; Hong, J. Assessment of Corneal Epithelial Changes and Related Factors in Ocular Chronic Graft-Versus-Host Disease (GVHD) by in Vivo Confocal Microscopy. Ocul. Immunol. Inflamm. 2023; online ahead of print. [Google Scholar] [CrossRef]
- Berchicci, L.; Aragona, E.; Arrigo, A.; Marchese, A.; Miserocchi, E.; Bandello, F.; Modorati, G. Conjunctival Matrix Metalloproteinase-9 Clinical Assessment in Early Ocular Graft versus Host Disease. J. Ophthalmol. 2021, 2021, 9958713. [Google Scholar] [CrossRef]
- Alba-Linero, C.; de Mora, M.R.C.; Valenzuela, R.L.; Cascón, M.J.P.; Cerezo, A.R.M.; Pérez, M.; Recio, L.V.; Aragonés, J.M.J.; Campos, J.M.G. Ocular surface characterization after allogeneic stem cell transplantation: A prospective study in a referral center. Indian J. Ophthalmol. 2020, 68, 1556–1562. [Google Scholar] [CrossRef]
- Ma, J.; Shen, Z.; Peng, R.; Li, C.; Hu, B.; Hong, J. Tear Lipid Metabolites As Potential Diagnostic Biomarkers for Ocular Chronic Graft-Versus-Host Disease. Biol. Blood Marrow Transplant. 2021, 27, 232.e1–232.e6. [Google Scholar] [CrossRef]
- Pellegrini, M.; Bernabei, F.; Moscardelli, F.; Vagge, A.; Scotto, R.; Bovone, C.; Scorcia, V.; Giannaccare, G. Assessment of Corneal Fluorescein Staining in Different Dry Eye Subtypes Using Digital Image Analysis. Transl. Vis. Sci. Technol. 2019, 8, 34. [Google Scholar] [CrossRef]
- Andersson, J.; Vogt, J.K.; Dalgaard, M.D.; Pedersen, O.; Holmgaard, K.; Heegaard, S. Ocular surface microbiota in patients with aqueous tear-deficient dry eye. Ocul. Surf. 2021, 19, 210–217. [Google Scholar] [CrossRef]
- O’Leary, O.E.; Schoetzau, A.; Amruthalingam, L.; Geber-Hollbach, N.; Plattner, K.; Jenoe, P.; Schmidt, A.; Ullmer, C.; Drawnel, F.M.; Fauser, S.; et al. Tear Proteomic Predictive Biomarker Model for Ocular Graft Versus Host Disease Classification. Transl. Vis. Sci. Technol. 2020, 9, 3. [Google Scholar] [CrossRef]
- Nair, S.; Vanathi, M.; Mahapatra, M.; Seth, T.; Kaur, J.; Velpandian, T.; Ravi, A.; Titiyal, J.S.; Tandon, R. Tear inflammatory mediators and protein in eyes of post allogenic hematopoeitic stem cell transplant patients. Ocul. Surf. 2018, 16, 352–367. [Google Scholar] [CrossRef]
- Li, J.; Liang, Q.; Huang, F.; Liao, Y.; Zhao, W.; Yang, J.; Wen, X.; Li, X.; Chen, T.; Guo, S.; et al. Metagenomic Profiling of the Ocular Surface Microbiome in Patients After Allogeneic Hematopoietic Stem Cell Transplantation. Arch. Ophthalmol. 2022, 242, 144–155. [Google Scholar] [CrossRef]
- Shimizu, E.; Ogawa, Y.; Saijo, Y.; Yamane, M.; Uchino, M.; Kamoi, M.; Fukui, M.; Yang, F.; He, J.; Mukai, S.; et al. Commensal microflora in human conjunctiva; characteristics of microflora in the patients with chronic ocular graft-versus-host disease. Ocul. Surf. 2019, 17, 265–271. [Google Scholar] [CrossRef]
- Zilliox, M.J.; Gange, W.S.; Kuffel, G.; Mores, C.R.; Joyce, C.; de Bustros, P.; Bouchard, C.S. Assessing the ocular surface microbiome in severe ocular surface diseases. Ocul. Surf. 2020, 18, 706–712. [Google Scholar] [CrossRef]
- Ma, J.; Li, C.; Zhao, Y.; Shen, Z.; Hu, B.; Peng, R.; Hong, J. Ophthalmic manifestations are associated with reduced tear lymphotoxin-α levels in chronic ocular graft-versus-host disease. BMC Ophthalmol. 2022, 22, 18. [Google Scholar] [CrossRef]
- Shen, Z.; Ma, J.; Peng, R.; Hu, B.; Zhao, Y.; Liu, S.; Hong, J. Biomarkers in Ocular Graft-Versus-Host Disease: Implications for the Involvement of B Cells. Biol. Blood Marrow Transplant. 2022, 28, 749.e1–749.e7. [Google Scholar] [CrossRef]
- Qiu, Y.; Hu, B.M.; Peng, R.-M.; Huang, J.-F.; Hong, J. Tear Cytokines as Biomarkers for Acute Ocular Graft-Versus-Host Disease. Cornea 2022, 41, 1405–1411. [Google Scholar] [CrossRef]
- Shaikh, R.B.; Santee, S.; Granger, S.W.; Butrovich, K.; Cheung, T.; Kronenberg, M.; Cheroutre, H.; Ware, C.F. Constitutive Expression of LIGHT on T Cells Leads to Lymphocyte Activation, Inflammation, and Tissue Destruction. J. Immunol. 2001, 167, 6330–6337. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lo, J.C.; Foster, A.; Yu, P.; Chen, H.M.; Wang, Y.; Tamada, K.; Chen, L.; Fu, Y.-X. The regulation of T cell homeostasis and autoimmunity by T cell–derived LIGHT. J. Clin. Investig. 2001, 108, 1771–1780. [Google Scholar] [CrossRef]
- Bron, A.; Tiffany, J.; Gouveia, S.; Yokoi, N.; Voon, L. Functional aspects of the tear film lipid layer. Exp. Eye Res. 2004, 78, 347–360. [Google Scholar] [CrossRef] [PubMed]
- Miguel, L.; Owen, D.M.; Lim, C.; Liebig, C.; Evans, J.; Magee, A.I.; Jury, E.C. Primary human CD4+ T cells have diverse levels of membrane lipid order that correlate with their function. J. Immunol. 2011, 186, 3505–3516. [Google Scholar] [CrossRef] [PubMed]
- Raha, S.; Raud, B.; Oberdörfer, L.; Castro, C.N.; Schreder, A.; Freitag, J.; Longerich, T.; Lochner, M.; Sparwasser, T.; Berod, L.; et al. Disruption of de novo fatty acid synthesis via acetyl-CoA carboxylase 1 inhibition prevents acute graft-versus-host disease. Eur. J. Immunol. 2016, 46, 2233–2238. [Google Scholar] [CrossRef]
- Lynch, S.V.; Pedersen, O. The Human Intestinal Microbiome in Health and Disease. N. Engl. J. Med. 2016, 375, 2369–2379. [Google Scholar] [CrossRef]
- Poruk, K.E.; Gay, D.Z.; Brown, K.; Mulvihill, J.D.; Boucher, K.M.; Scaife, C.L.; Firpo, M.A.; Mulvihill, S.J. The clinical utility of CA 19-9 in pancreatic adenocarcinoma: Diagnostic and prognostic updates. Curr. Mol. Med. 2013, 13, 340–351. [Google Scholar] [CrossRef]
- Sternhagen, E.; Bettendorf, B.; Lenert, A.; Lenert, P.S. The Role of Clinical Features and Serum Biomarkers in Identifying Patients with Incomplete Lupus Erythematosus at Higher Risk of Transitioning to Systemic Lupus Erythematosus: Current Perspectives. J. Inflamm. Res. 2022, 15, 1133–1145. [Google Scholar] [CrossRef]


{kind=link}
| Score | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| OSDI Score | <13 | 13–22 | 23–32 | ≥33 |
| Schirmer’s Test (in mm) | >15 | 11–15 | 6–10 | ≤5 |
| Corneal Staining | No staining | Minimal staining | Mild/moderate staining | Severe staining |
| Conjunctival Injection | No injection | Mild/moderate injection | Severe injection |
| Potential Biomarker(s) | Sample Type | Patient Groups | Technique | Comparison vs. Control | Correlations with Clinical Parameters | References |
|---|---|---|---|---|---|---|
| Cytokines: ICAM-1, IFN-β, IFN-γ, IL-1β, IL-1Ra, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-13, IL-12/23p40, IL-17A, IL-18, IL-21, IL33, LTA, TNFa, GM-CSF, BAFF, EGF | Tears | oGVHD, DED | Microsphere-based immunoassay analysis | oGVHD: ICAM-1, IL1β, IL-6, IL-8 higher than DED; IL-7 and EGF lower than DED. | Schirmer’s test: Neg correlations w/ ICAM-1, IL-6, IL-1β, and IL-8; pos correlations w/ EGF and IL-7. CFS: Pos correlations w/ ICAM-1, IL-6, IL-1β, and IL-8 (sig for IL-6 and IL-8). TBUT: Neg correlations w/ ICAM-1, IL-6, IL-1β, and IL-8 (sig for ICAM-1 and IL-8); pos correlations w/ EGF and IL-7. OSDI score: Pos correlations w/ ICAM-1, IL-6, IL-1β, and IL-8; neg correlations w/ EGF and IL-7. Elevated ICAM-1, IL-6, and IL-8 levels may signal disease severity. | Hu et al. [14] |
| Cytokines: IFN-γ, IL-10, MMP-9, IL-12, IL-13, IL17α, IL-1β, IL-2, IL-4, IL-6, IL-8, CXCL10, MCP-1, MIP-1α, RANTES, TNF-α; tear osmolarity | Tears and serum | oGVHD HSCT, healthy controls | Tearlab osmolarity system; serum sent to Allergen, Inc., Dublin, Ireland, for biomarker analysis | oGVHD had a higher median Oxford corneal staining score, lower RANTES, and higher IL-8 and TNF-α compared to non-oGVHD. | Elevated tear TNF-α positively correlated with higher corneal staining scores. Reduced tear RANTES levels associated with decreased Schirmer’s test and TBUT. | Pietraszkiewicz et al. [15] |
| Innate inflammatory cells, DNA products, cytokines, proteins | Ocular surface washing, peripheral blood (mice in vivo) | oGVHD HSCT, non-oGVHD HSCT, healthy controls | IHC, qPCR, Western blot | Elevated neutrophils and NET presence/activity correlates with oGVHD severity. | NET-related proteins, neutrophil elastase, MPO, OSM, NGAL, LIGHT/TNFSF14 cause corneal issues, conjunctival cicatrization, inflammation, and meibomian gland disease. | An et al. [16] |
| Proteins: TP, LYS-C, LACTO, LIPOC-1, TRANSF, ALB, ZAG-2 levels | Tears | oGVHD HSCT, pre-HSCT (same patients) | 2100 BioAnalyzer (Agilent Technology, Santa Clara, CA, USA) | TP, LACTO, TRANSF, and ZAG-2 decreased in late-onset oGVHD patients. | No statistically significant differences were found in the clinical parameters between the oGVHD and pre-HSCT groups, and as such no correlational analyses between biomarkers and clinical parameters were made in this study. | Ciavarella et al. [17] |
| Cytokines: IL-6, IL-10, TNF-a, EGF, MMP-2, MMP-3, MMP-7, BAFF, and APRIL. | Tears and imaging (cornea) | oGVHD HSCT, non-oGVHD HSCT | Microsphere-based immunoassay analysis; confocal laser scanning microscopy | oGVHD: EGF, MMP-7, and APRIL significantly decreased compared to non-oGVHD HSCT. | Corneal epithelial scores significantly correlated with tear EGF and APRIL. | Liu et al. [18] |
| Protein: MMP-9 | Tears | oGVHD, non-Sjogren DED | TearLabTM Osmolarity System (TearLabTM Corp., San Diego, CA, USA) | MMP-9 expression elevated in oGVHD patients. | Positive correlations between MMP-9 and conjunctival staining, OSDI, and Schirmer test. | Berchicci et al. [19] |
| T-Cells: CD8 | Conjunctival impression cytology | oGVHD HSCT, non-oGVHD HSCT, healthy controls | Immunofluorescence | Significant difference in controls vs. pre- and post-HSCT w/ and w/o GVHD; no significant difference between oGVHD HSCT and non-oGVHD HSCT. | Association between CD8 T-cell levels and Schirmer’s test, TBUT, and OSDI. | Alba-Linero et al. [20] |
| Lipids: phosphatidylcholine, sphingomyelin, lactosylceramide, DHA | Tears | oGVHD HSCT, healthy controls | Mass spectroscopy | Phosphatidylcholine, sphingomyelin, and lactosylceramide correlate with clinical findings. | Phosphatidylcholine, sphingomyelin, and lactosylceramide: strong correlations with NIH eye score, TBUT, CFS, and Schirmer’s test. | Ma et al. [21] |
| Fluorescein uptake | Split lamp photography of corneal staining | Sjogren Syndrome, oGVHD HSCT | Corneal staining index via ImageJ 1.51s (National Institutes of Health, Bethesda, MD, USA) | Circularity and roundness of corneal staining index were higher in oGVHD vs. SS. | The corneal staining index was significantly correlated with Oxford and NEI scales. | Pellegrini et al. [22] |
| Microbiota | Swab samples from conjunctival fornix | Dry eye w/ and w/o GVHD, healthy controls | 16S rRNA gene sequencing | Pseudomonas identified as a bacterial biomarker for controls and Bacilli for aqueous tear-deficient dry eye. | Three genera correlated with OSDI or Schirmer’s test: Staphylococcus in the OGVHD group and Chryseobacterium and Micrococcus in the dry eye group | Andersson et al. [23] |
| 79 proteins (nucleic acid binding proteins, cytoskeletal proteins, transfer and receptor proteins, enzyme modulators, and hydrolases) | Tears | oGVHD HSCT, healthy controls | Liquid chromatography, mass spectrometry | 54 out of 79 proteins were upregulated, encompassing nucleic acid binding and cytoskeletal proteins. Downregulated proteins included transfer and receptor proteins, enzyme modulators, and hydrolases. 36 newly identified proteins displayed altered expressions. | No direct correlations were made between clinical parameters and potential biomarkers. The study focused on following changes in protein levels between both groups. However, OSDI, TBUT, Oxford score, and Schirmers test are strongly associated with progression to ocular GVHD in this study. | Gerber-Hollbach et al. [13] |
| Proteins, untargeted proteomic methods | Tears | oGVHD HSCT, non-oGVHD HSCT | Liquid chromatography, mass spectrometry | Lactotransferrin, lysozyme, polymeric immunoglobulin receptor, immunoglobulin J chain, prolactin-inducible protein, and immunoglobulin heavy constant alpha downregulated with increased severity. | Reduced LYZ and PIGR linked to higher OSDI and Oxford staining scores. These proteins also had strong inverse relationships with overall NIH scores. Regarding PGAM1, weaker correlations were observed with clinical measures. PGAM1 levels were positively associated with Oxford score and OSDI but negatively correlated with the Schirmer test and TBUT scores. | O’Leary et al. [24] |
| Proteins: IL-6, IFN Gamma, IL-8, IL 10, IL-15, IL-4, IL-2, IL-12P70, IL-17A, VEGF, TNF-alpha, MMPs | Tears | oGVHD HSCT, non-oGVHD HSCT, healthy controls | Bio-Plex assay | oGVHD: elevated levels of interferon γ, IL-6, IL-8, IL-10, IL-12P70, IL-17A, MMP-9, and VEGF compared to controls. Tear MMP-7 and MMP-9 are higher in non-oGVHD, suggesting potential indicators for oGVHD in post-allo-HSCT individuals. | A negative correlation was found between Schirmer’s test values and IL-2, IL-4, IL-6, IL-12P70, MMP9, and VEGF. Tear proteins were significantly decreased in oGVHD eyes, while levels appeared similar in non-GVHD and control eyes. Notably, tear levels of MMP7 and MMP9 were significantly elevated in non-oGVHD patients compared to healthy controls. | Nair et al. [25] |
| Microbiota | Conjunctival sample | oGVHD HSCT, non-oGVHD HSCT, healthy controls | Metagenomic shotgun sequencing, sequencing libraries qPCR | Reduction in ocular surface microbiota diversity in both allo-HSCT w/ and w/o oGVHD, indicating microbial dysbiosis post-allo-HSCT, irrespective of oGVHD development. | Paracoccus sp. was negatively associated with corneal fluorescein staining score, while Acidovorax sp. had a positive association. | Li et al. [26] |
| Microbiota | Samples from the lower conjunctiva via a sterile cotton swab (without anesthesia) | oGVHD HSCT, non-oGVHD HSCT, healthy controls | Microbes were cultured | More species were detected in severe chronic ocular GVHD, implying diversified conjunctival microbial communities in GVHD patients. | Positive correlation between the number of detected species and the ICO score and an inverse correlation between the number of detected species and TBUT. | Shimizu et al. [27] |
| Microbiome | Samples from superior and inferior tarsal conjunctiva and inferior conjunctival fornixes (with anesthesia) | Chronic SJS, oGVHD HSCT, LES, DED, healthy controls | MiSeq (Illumina Inc. San Diego, CA, USA), Mothur software v. 1.31.2 | Positive relationship between the number of detected species and the ICO score. These findings suggest that as the severity of chronic ocular GVHD grading increases, more bacteria can be detected. | Biopsy-confirmed SJS/TEN, ocular oGVHD per the Chronic Ocular Graft-vs-Host-Disease (GVHD) Consensus Group, LES as defined by van den Bosch, and DED diagnosed based on DEWS II criteria. | Zilliox et al. [28] |
| Lymphotoxin-α (LT-α) | Tears | oGVHD HSCT, healthy controls | LT-α concentration test strip, S03A analyzer | LT-α decreased significantly in oGVHD patients with no sex difference. | LT-α significantly correlated with OSDI, NIH eye score, T-BUT, and CFS among all participants. | Ma et al. [29] |
| Proteins: IL-2, IL-6, IL-8, IL-10, IL-12, IL-17, CCL2, GM-CSF, M-CSF, GMCSF, FGF1, FGF2, EGF, VEGF, Fas-L, BAFF, CD40L, CD137, APRIL, ICAM-1, CD62E CD106, MMP-2, MMP-3, MMP-7, neuropilin-1, PDGF-CC, NGF-beta, and TNF-alpha | Tears | oGVHD HSCT, dry eye disease | Microsphere-based immunoassay analysis | oGVHD: Elevated G-CSF, M-CSF, GM-CSF, FGF1, FGF2, BAFF, CD40L, CD137, CD106, CD62E, MMP2, MMP3, and neuropilin-1. Reduced APRIL. | IL-2, IL-6, IL-8, MMP-3, neuropilin-1, CD62E, CD52, and BAFF negatively correlated with TBUT. BAFF positively correlated with OSDI and CFS scores. CD62E and CD52 are positively associated with OSDI and NIH grades. | Shen et al. [30] |
| Compliment: C2, C3a, C3/C5a; Cytokines: IFN-b, IFN-g, IL-1b, IL-1Ra, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-13, IL-12, IL-17A, IL-18, IL-21, IL-33, TNF-a, GM-CSF, BAFF, EGF, ICAM-1, lipoteichoic acid | Tears | oGVHD HSCT, healthy controls | Microsphere-based immunoassay analysis | oGVHD: Differences were observed in C2, C3a, and C5/C5a. ICAM-1, IL-1b, IL-6, IL-8, BAFF, and GM-CSF exhibited increased levels compared to healthy controls. IL-7 and EGF were lower. | Schirmer: neg. correlated with ICAM-1, IL-6, IL-1b, IL-8, BAFF, GM-CSF, C2, and C3a, while pos. correlating with EGF, IL-7, and C5/C5a, significantly for IL-1b, EGF, GM-CSF, and IL-7. CFS: pos. correlations with IL-6, IL-1b, IL-8, BAFF, GM-CSF, C2, and C3a and neg. correlations with ICAM-1, EGF, IL-7, and C5/C5a. TBUT: neg. correlations with ICAM-1, IL-6, IL-1b, IL-8, BAFF, GM-CSF, C2, C3a, and C5/C5a, while pos. correlations with EGF and IL-7, particularly for IL-1b, GM-CSF, and C3a. OSDI: pos. correlations with IL-6, IL-1b, IL-8, BAFF, GM-CSF, C2, C3a, and C5/C5a and neg. correlations with ICAM-1, EGF, and IL-7, notably for IL-6, IL-1b, GM-CSF, and IL-7 | Qiu et al. [31] |
| Selection | Comparability | Exposure | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Is the Case Definition Adequate | Representativeness of the Cases | Selection of Controls | Definition of Controls | Comparability of Cases and Controls | Ascertainment of Exposure | Same Method of Ascertainment for Cases and Controls | Non-Response Rate | Total | |
| Pietraszkiewicz, et al. [15] | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 6 | ||
| Qiu et al. [31] | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 6 | ||
| Shimizu et al. [27] | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 6 | ||
| Li et al. [26] | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 6 | ||
| O’Leary et al. [24] | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 6 | ||
| Gerber-Hollbach et al. [13] | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 6 | ||
| Liu et al. [18] | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 6 | ||
| Alba-Linero et al. [20] | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 6 | ||
| Hu et al. [14] | ☆ | ☆ | ☆ | ☆ | ☆ | 5 | |||
| Shen et al. [30] | ☆ | ☆ | ☆ | ☆ | ☆ | 5 | |||
| Ma et al. [29] | ☆ | ☆ | ☆ | ☆ | ☆ | 5 | |||
| Ciavarella et al. [17] | ☆ | ☆ | ☆ | ☆ | ☆ | 5 | |||
| Pellegrini et al. [22] | ☆ | ☆ | ☆ | ☆ | ☆ | 5 | |||
| Ma et al. [21] | ☆ | ☆ | ☆ | ☆ | ☆ | 5 | |||
| Andersson et al. [23] | ☆ | ☆ | ☆ | ☆ | ☆ | 5 | |||
| Zilliox et al. [28] | ☆ | ☆ | ☆ | ☆ | 4 | ||||
| Nair et al. [25] | ☆ | ☆ | ☆ | ☆ | 4 | ||||
| An, et al. [16] | ☆ | ☆ | ☆ | ☆ | 4 | ||||
| Berchicci et al. [19] | ☆ | ☆ | ☆ | ☆ | 4 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bohlen, J.; Gomez, C.; Zhou, J.; Martinez Guasch, F.; Wandvik, C.; Sunshine, S.B. Molecular Biomarkers in Ocular Graft-versus-Host Disease: A Systematic Review. Biomolecules 2024, 14, 102. https://doi.org/10.3390/biom14010102
Bohlen J, Gomez C, Zhou J, Martinez Guasch F, Wandvik C, Sunshine SB. Molecular Biomarkers in Ocular Graft-versus-Host Disease: A Systematic Review. Biomolecules. 2024; 14(1):102. https://doi.org/10.3390/biom14010102
Chicago/Turabian StyleBohlen, Jerry, Charlyn Gomez, Jason Zhou, Fernando Martinez Guasch, Caitlyn Wandvik, and Sarah Brem Sunshine. 2024. "Molecular Biomarkers in Ocular Graft-versus-Host Disease: A Systematic Review" Biomolecules 14, no. 1: 102. https://doi.org/10.3390/biom14010102
APA StyleBohlen, J., Gomez, C., Zhou, J., Martinez Guasch, F., Wandvik, C., & Sunshine, S. B. (2024). Molecular Biomarkers in Ocular Graft-versus-Host Disease: A Systematic Review. Biomolecules, 14(1), 102. https://doi.org/10.3390/biom14010102