Community Pharmacists’ Motivation and Barriers to Providing and Billing Patient Care Services


Abstract
:1. Introduction
- Independently furnish self-administered hormonal contraceptives, nicotine replacement therapy medications, and medications for symptoms not requiring a diagnosis that are recommended for international travelers (Senate Bill (SB) 493)
- Furnish naloxone hydrochloride in accordance with standardized procedures or protocols (SB 1535)
- Furnish HIV preexposure and postexposure (PrEP/PEP) medications (SB 159)
- Earn certification in a relevant area of practice, including, but not limited to, ambulatory care, critical care, geriatric pharmacy, nuclear pharmacy, nutrition support pharmacy, oncology pharmacy, pediatric pharmacy, pharmacotherapy, or psychiatric pharmacy, from an organization recognized by Accreditation Council for Pharmacy Education (ACPE) or another entity recognized by the board.
- Complete a postgraduate residency through an accredited postgraduate institution where at least 50 percent of the experience includes the provision of direct patient care services with interdisciplinary teams.
- Have provided clinical services to patients for at least one year under a collaborative practice agreement or protocol with a physician, advanced practice pharmacist, pharmacist practicing collaborative drug therapy management, or health system.
2. Materials and Methods
2.1. Study Design
2.2. Web-Based Survey Development
2.3. Electronic Survey Distribution
2.4. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Knowledge of Patient Care Services
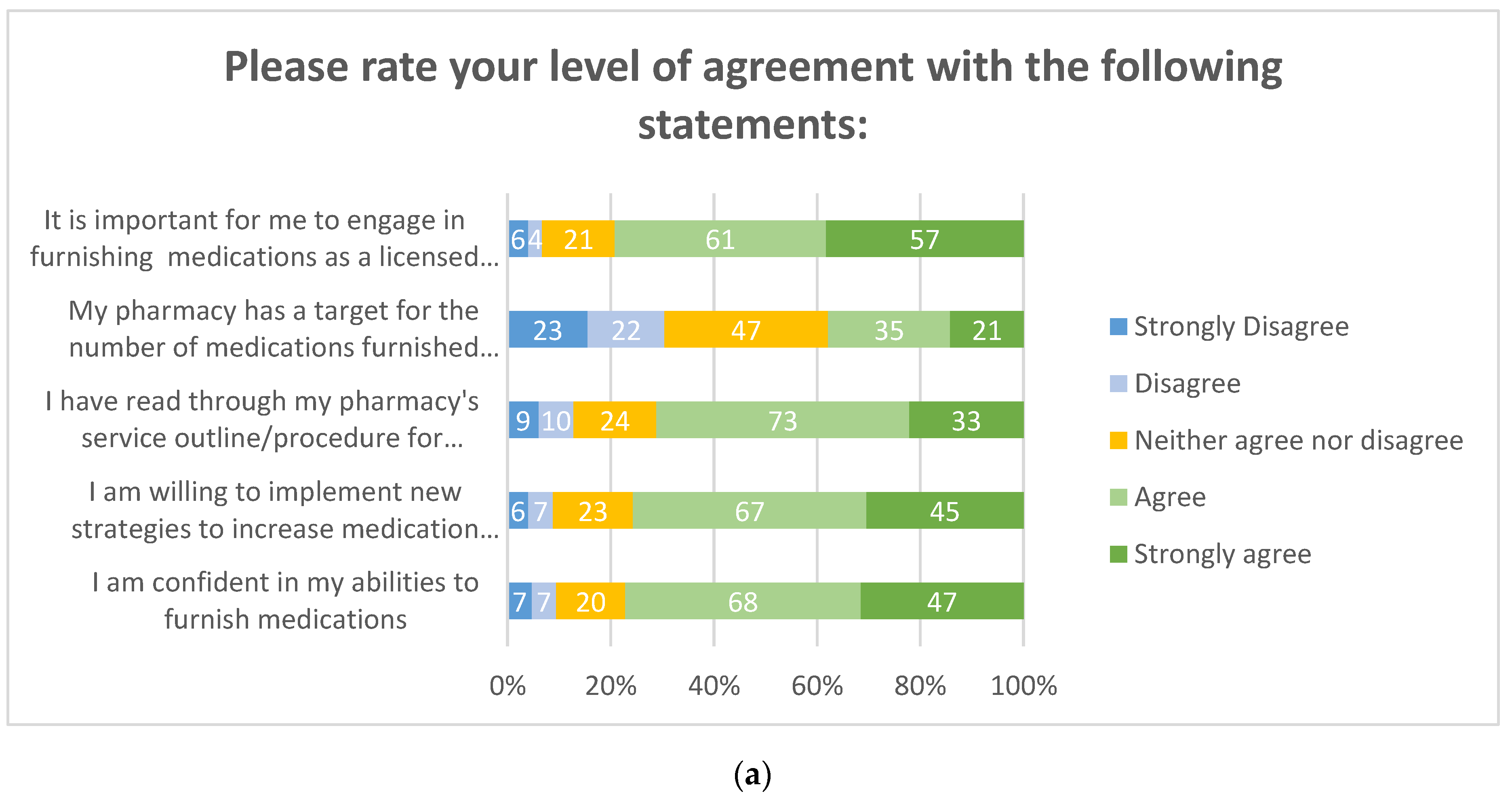
3.3. Motivation to Provide Patient Care Services
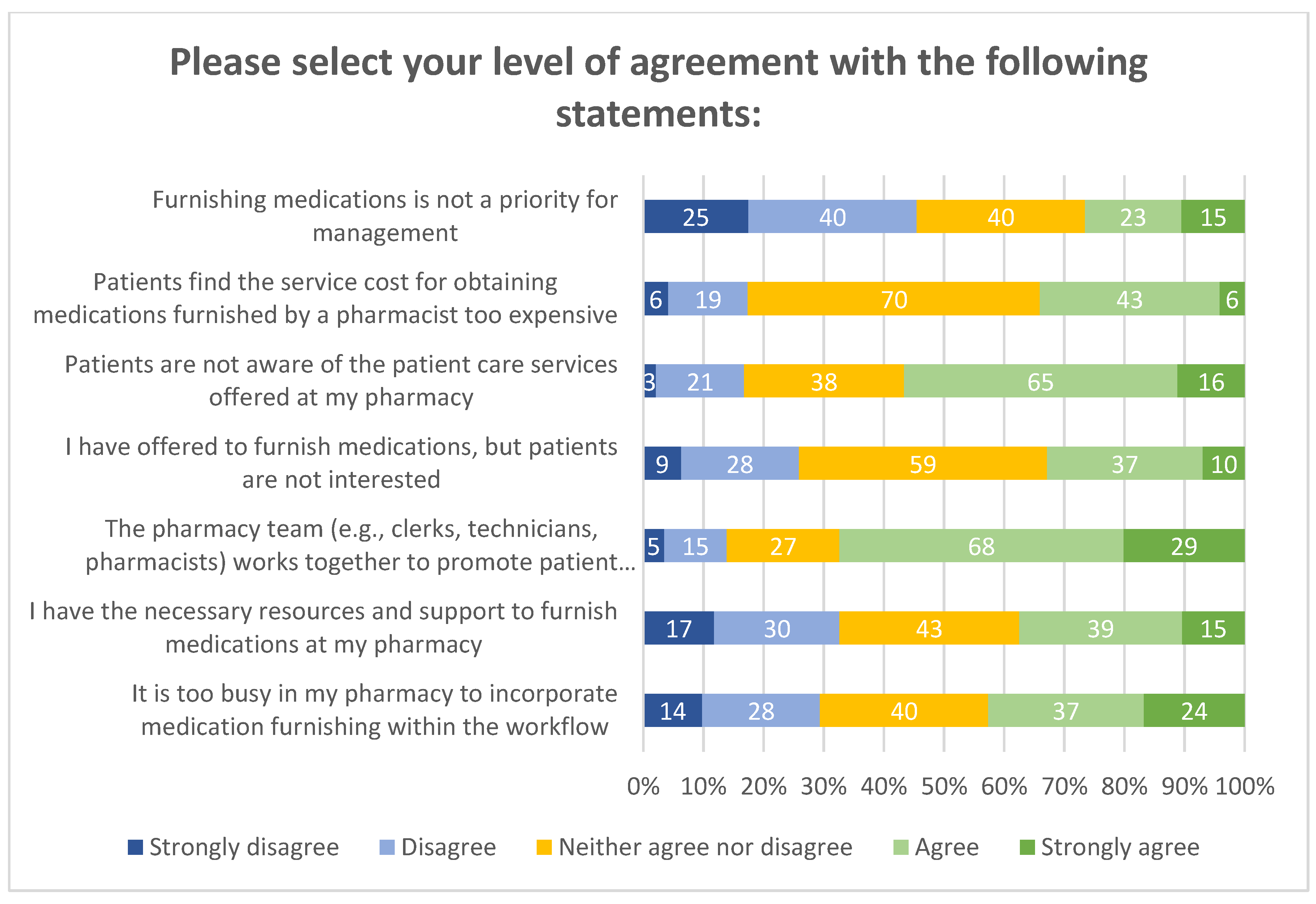
3.4. Barriers to Providing Patient Care Services
4. Discussion
4.1. Findings
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- California Legislative Information: Senate Bill No. 493. Available online: https://leginfo.legislature.ca.gov/faces/billTextClient.xhtml?bill_id=201320140SB493 (accessed on 15 April 2020).
- California Legislative Information: Assembly Bill No. 1535. 2014. Available online: https://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=201320140AB1535 (accessed on 15 April 2020).
- California Legislative Information: SB-159 HIV: Preexposure and Postexposure Prophylaxis. Available online: http://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=201920200SB159 (accessed on 15 April 2020).
- 2009 California Business and Professions Code—Section 4015–4045: Article 2. Available online: https://law.justia.com/codes/california/2009/bpc/4015-4045.html (accessed on 15 April 2020).
- California Provider Status Law Effective January 1. Available online: https://www.pharmacist.com/article/california-provider-status-law-effective-january-1 (accessed on 15 April 2020).
- California Legislative Information: Assembly Bill No. 1114. 2016. Available online: https://leginfo.legislature.ca.gov/faces/billTextClient.xhtml?bill_id=201520160AB1114 (accessed on 15 April 2020).
- Puzantian, T.; Gasper, J.J. Provision of Naloxone without a Prescription by California Pharmacists 2 Years after Legislation Implementation. JAMA 2018, 320, 1933–1934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kritz, F. Pharmacists Can Now Prescribe Birth Control, But Few Do. California Health Report. Available online: http://www.calhealthreport.org/2019/02/15/pharmacists-can-now-prescribe-birth-control-but-few-do-%EF%BB%BF/ (accessed on 15 April 2020).
- Brame, C. Writing Good Multiple-Choice Test Questions. Vanderbilt University Center for Teaching. Available online: https://cft.vanderbilt.edu/guides-sub-pages/writing-good-multiple-choice-test-questions/ (accessed on 23 June 2020).
- Blalock, S.J.; Roberts, A.W.; Lauffenburger, J.C.; Thompson, T.; O’Connor, S.K. The Effect of Community Pharmacy-based Interventions on Patient Health Outcomes: A Systematic Review. Med. Care Res. Rev. 2013, 70, 235–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makowsky, M.J.; Guirguis, L.M.; Hughes, C.A.; Sadowski, C.A.; Yuksel, N. Factors Influencing Pharmacists’ Adoption of Prescribing: Qualitative Application of the Diffusion of Innovations Theory. Implement Sci. 2013, 8, 109. [Google Scholar] [CrossRef] [Green Version]
- Bakhireva, L.N.; Bautista, A.; Cano, S.; Shrestha, S.; Bachyrycz, A.M.; Cruz, T.H. Barriers and Facilitators to Dispensing of Intranasal Naloxone by Pharmacists. Subst. Abus. 2018, 39, 331–341. [Google Scholar] [CrossRef]
- Newman, T.V.; Hernandez, I.; Keyser, D.; San-Juan-Rodriguez, A.; Swart, E.C.S.; Shrank, W.H.; Parekh, N. Optimizing the Role of Community Pharmacists in Managing the Health of Populations: Barriers, Facilitators, and Policy Recommendations. J. Manag. Care Spec. Pharm. 2019, 25, 995–1000. [Google Scholar] [CrossRef]
- Snyder, M.E.; Zillich, A.J.; Primack, B.A.; Rice, K.R.; McGivney, M.A.S.; Pringle, J.L.; Smith, R.B. Exploring Successful Community Pharmacist-Physician Collaborative Working Relationships Using Mixed Methods. Res. Soc. Adm. Pharm. 2010, 4, 307–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Percentage (No.) |
|---|---|
| Additional training (N = 32) | |
| PGY1 Residency | 44% (14) |
| PGY2 Specialty Residency | 13% (4) |
| Fellowship | 9% (3) |
| Other | 34% (11) |
| Ethnicity (N = 139) | |
| White | 40% (56) |
| Hispanic or Latino | 4% (6) |
| Black or African American | 2% (3) |
| Native American | 2% (3) |
| Asian or Pacific Islander | 37% (52) |
| Other | 5% (7) |
| Prefer not to specify | 9% (12) |
| Gender (N = 140) | |
| Male | 53% (74) |
| Female | 41% (58) |
| Other | 1% (1) |
| Prefer not to specify | 5% (7) |
| Characteristic | Percentage (No.) | ||||
|---|---|---|---|---|---|
| Patient groups served | 0–25% | 26–50% | 51–75% | >75% | I don’t Know |
| Geriatrics (65 years and older) | 15% (27/183) | 33% (60/183) | 39% (72/183) | 11% (20/183) | 2% (4/183) |
| Middle-age adults (40–64 years old) | 18% (33/179) | 59% (106/179) | 18% (32/179) | 1% (2/179) | 3% (6/179) |
| Young adults (18–39 years old) | 62% (110/177) | 29% (51/177) | 5% (9/177) | 1% (2/177) | 3% (5/177) |
| Pediatrics (under 18 years old) | 84% (139/165) | 12% (20/165) | 1% (2/165) | 0% (0/165) | 2% (4/165) |
| Medicare & Medi-Cal (“Medi-Medi”) beneficiaries | 34% (58/171) | 28% (48/171) | 19% (32/171) | 12% (21/171) | 7% (12/171) |
| Medi-Cal beneficiaries | 32% (54/168) | 25% (42/168) | 23% (38/168) | 15% (26/168) | 5% (8/168) |
| Prescriptions Dispensed per Week | Percentage (No.) |
|---|---|
| <500 | 14% (27) |
| 500–1000 | 39% (73) |
| 1001–1500 | 24% (44) |
| 1501–2000 | 8% (14) |
| 2001–2500 | 6% (11) |
| >2500 | 10% (18) |
| Service Fee Billed | Percentage (SD, Range) |
| Directly to Patient (N = 98) | 16% (25.5, 0–100) |
| Commercial Payor (N = 96) | 35% (27.9, 0–100) |
| Medicare (N = 98) | 29% (23.4, 0–100) |
| Medi-Cal (N = 95) | 22% (23.4, 0–100) |
| No bill or charge (N = 82) | 15% (31.1, 0–100) |
| Survey Question | Number of Individuals That Selected the Correct Answer |
|---|---|
| A pharmacist licensed in California who has completed the training required by the Board of Pharmacy can furnish the following medications (select all that apply): (a) Travel medications (b) Self-administered hormonal contraceptives (c) Routine vaccinations (d) Nicotine replacement therapies (e) Naloxone hydrochloride (f) HIV PrEP/PEP medications * (g) Chantix (varenicline) * (h) Buprenorphine (e.g., Suboxone) * (i) I don’t know | 20% (34/168) |
| AB 1114 requires the rate of reimbursement for pharmacist services to be at ______ percentage of the fee schedule for physician services under the Medi-Cal program. (a) 50% (b) 65% (c) 70% (d) 85% (e) 100% | 56% (25/45) |
| Reimbursement for pharmacist services provided to Medi-Cal beneficiaries is contingent upon (select all that apply): (a) Completion of a 2 h, AB 1114 continuing education session (b) Enrollment as an ordering, referring, and prescribing (ORP) provider with Medi-Cal (c) Payment of a yearly fee to the Department of Health Care Services (d) Completion of a PGY-1 residency (e) California licensure as an Advanced Practice Pharmacist | 62% (51/82) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reyes, L.D.; Hong, J.; Lin, C.; Hamper, J.; Kroon, L. Community Pharmacists’ Motivation and Barriers to Providing and Billing Patient Care Services. Pharmacy 2020, 8, 145. https://doi.org/10.3390/pharmacy8030145
Reyes LD, Hong J, Lin C, Hamper J, Kroon L. Community Pharmacists’ Motivation and Barriers to Providing and Billing Patient Care Services. Pharmacy. 2020; 8(3):145. https://doi.org/10.3390/pharmacy8030145
Chicago/Turabian StyleReyes, Liesl D., Jenny Hong, Christine Lin, Jeffrey Hamper, and Lisa Kroon. 2020. "Community Pharmacists’ Motivation and Barriers to Providing and Billing Patient Care Services" Pharmacy 8, no. 3: 145. https://doi.org/10.3390/pharmacy8030145
APA StyleReyes, L. D., Hong, J., Lin, C., Hamper, J., & Kroon, L. (2020). Community Pharmacists’ Motivation and Barriers to Providing and Billing Patient Care Services. Pharmacy, 8(3), 145. https://doi.org/10.3390/pharmacy8030145