Decision-Making Process in Comprehensive Medication Management Services: From the Understanding to the Development of a Theoretical Model


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Data Collection
2.2. Data Analysis
3. Results and Discussion
3.1. Understanding the Rational Method of Decision-Making: The Foundation of the Patient Care Process
“I can provide the same care, the same quality of care to any patient regardless of the number of medications, or the number of health problems he/she has. Nowadays, I feel calmer… because it doesn’t matter which person is in front of me, I know what I am going to do with him/her. After a year of practice, I am already reaching 200 patients, and I can be relaxed because, with just a piece of paper in hand, I know what I have to do. That thanks to the method.”P10
“At all times, the patient arrives, shows me the prescription, and I am thinking like that. I look at each medication, is it indicated, effective, safe, convenient? It is the process in my head all the time. I cannot evaluate medications if it is not this way.”P2
“When I am with the patient, with the medical record, with the literature, with the health team, I always have that sequence in my head, looking for ways to find all the answers.”P1
“Before I was surer about the decisions [the interviewee makes a sign of quotation marks] that I took, not a decision, but the follow-ups I made. For me that was good, and I looked at a patient’s prescription and already knew if it was good or not, but based on what? On posology, on drug interactions. Sometimes I saw a problem with the prescription, which was not a real problem for the patient, but I saw a problem. Or I did not see a problem in the prescription when the patient had a lot of real problems with his medications. However, I was sure at that time! I thought I was a good pharmacist. I knew the reasons all the medications were used… Then I started working with CMM, and I started to understand, to execute the reasoning [rational thought-process] more naturally, without having to be focusing only on the prescription. I overcame the phase of insecurity. I returned to certainty, but a more reasoned certainty. CMM became an architectural project in which my knowledge came back to fit into certain places, places that I could access in a more useful way.”P7
3.2. Balancing the Care Equation: The Objective and the Subjective
“I say CMM is beautiful, it is an art, you take the technical piece and combine it with that wonderful thing that is the person, what he/she has, his/her beliefs, and experiences. Doing this is an art. I think it is incredible because it is not easy… When you get it, it is wonderful because the person realizes that you are taking that into account.”P10
3.2.1. Adding Pharmacotherapy Knowledge
“That is why I say that it is important to train the professional because he/she needs to know about pharmacotherapy to ask questions that are directed, to try to identify problems of effectiveness or safety.… the patient uses a calcium channel blocker, so I ask, ‘Do you feel anything?’ ‘No.’ ‘And edema? Does your foot swell? And then he/she says, ‘Look, my foot swells.’ ‘Oh, do you use diuretics? Do you have a cramp?’ All the time, I will ask questions to help me with this reasoning.”P2
“Understanding treatment protocols to know the indication, understand the disease, the parameters to monitor the effectiveness of the medication, and the safety profile of each medication to evaluate the safety. It is what will guide you. You have to think about the unique contribution you bring to care. It is your gaze. You have to combine the information to find specific problems there.”P1
“The patient had a request for a lab to evaluate the serum concentration of phenytoin and phenobarbital. Both student and pharmacist decided to wait for the test result to decide if it would be possible to increase the dose or to change to a more effective medication for that patient.”(Excerpt from the field diary)
“Looking for scientific studies, I was at this stage… there are good signs that atenolol can be a good option for the elderly. I said well, so that will be it, she needs another antihypertensive since she is in the maximum dose of losartan and hydrochlorothiazide… She used them correctly. I could not increase the dose of losartan nor hydrochlorothiazide. She needed another antihypertensive, and the natural thing was to add a beta-blocker that could also treat the migraine.”P7
3.2.2. Exploring the Patient’s Medication Experience
“The doubt was regarding a patient with a prescription of nortriptyline for depression, but who reported not taking it, as she claims to have no depression. For the student, who participated in the discussion, the patient had a problem with adherence to the treatment. However, it was argued the need to investigate whether the patient had depression to determine if there was an indication for the medication.”(Excerpt from the field diary)
“Regarding the patient’s concerns, he [patient] will tell me a lot about adverse reactions that are already happening or that he is afraid of because he heard about it or because he is not sure that it has a relationship with his medication, but it seems to have it, so it is a concern. The understanding is very much related to the behavior of the patient… So I think that it will inform much of the question of convenience.”P11
“I try to understand his experience, and I try to see where he is wrong or right.”P3
“We clarify if those concerns are real or if they are unfounded. If they are real, how we will monitor them during the process… If the expectation is not correct, we work on it.”P5
“A hypertensive patient was taking an ACE inhibitor [angiotensin-converting enzyme]. It was indicated, effective, safe, and convenient medication in my evaluation. However, her mother had died from drug hepatitis… and the doctor said the suspected drug was an ACE inhibitor. The ACE inhibitor controlled the patient’s blood pressure… it was indicated, effective, apparently safe, but there was this concern. I could not tell her that she was not going to have drug-induced hepatitis, do you understand? The fact that her mother had hepatitis did not mean she would have it, but I also could not affirm that she would not have it. Thus, that fear interfered with the process of adherence of this patient. She was taking it, but it would come a moment, in my evaluation, that she would stop taking it. So why can’t we suggest the change this medication, get in touch with her doctor and ask for the change? I could have said, ‘Keep taking it, it will not happen to you, this medicine is great, you are not even sure if it was, in fact, the ACE inhibitor that caused your mom’s hepatitis.’ However, out of respect for the patient, we have constructed another therapeutic plan. We made a letter proposing the class change of the antihypertensive drug.”P5
“I have already seen a patient like this: ‘What do you think about insulin?’ ‘Horrible, those who use insulin die. My brother died because he started using insulin. Then I go to explore the story of his brother. ‘But did your brother control diabetes?’ ‘No, he ate sweets.’ Then I say, ‘So did he die because he used insulin or because his diabetes was out of control? Then the patient says, ‘Oh, it is because he did not control it, right?’ ‘Probably.’ Then when I see that he understood it, I start saying that insulin is the best option.”P3
3.2.3. Discussing Versus Sharing the Decision with the Patient: What Are We Really Doing?
“The order I follow is: I identify the DTP, I share my choice to resolve the DTP with the patient because all my interventions are agreed upon with him. I always ask, ‘Can we do it? Can it be this way?’ He says, ‘It may be this way,’ and then I go to the prescriber and talk to him.”P2
3.2.4. Factors That Can Modify the Decision-Making Process
“I feel like an octopus with multiple arms. So it turns out that I make a decision about pharmacotherapy, I make a decision about non-pharmacological measures, I make a decision about other areas… because the patient is not just the medication he takes; he is a whole. Thus, to meet this need of the whole, of the complex being that he is, I must make other decisions…”P2
“So many times I came across situations where everything was ready, and the doctor just did not agree, and the patient needed it.”P3
“… I have no habit of talking to the patient before discussing with the doctor, or if I depend on any other professional because I think this will further stress our relationship.”P3
“If you do not have a solid foundation in pharmacology, first you do not identify the problem, and second you cannot draw up different solutions… when you have a more solid knowledge of pharmacotherapy, you can even think of different solutions to present them to the individual.”P11
“There is a case that happened recently, a patient who is an alcoholic and already has ascites due to his cirrhosis and I went to discuss with the doctor the treatment. He was using propranolol, which… worsens the survival of a patient who has ascites. When I went to discuss the case, she said, ‘no, propranolol is a choice,’ and I said, ‘It is not, let us open the algorithm, let us look.’ Then, the moment we opened it, she saw that any beta-blocker, any that decreases peripheral vascular resistance, could increase ascites, and then she changed it. If it were a letter, I would not have the chance to argue, and that happened too much.”P2
“In many situations, it is more difficult because, sometimes, I do not have a patient history. I have what the patient tells me. I often have tests that can corroborate what the patient told me, but I only have the story told by the patient. I do not know the patient’s health team.”P4
“… He [the doctor] chooses a patient that he cannot adjust his dose of warfarin and directs him to me, that’s fantastic.”P3
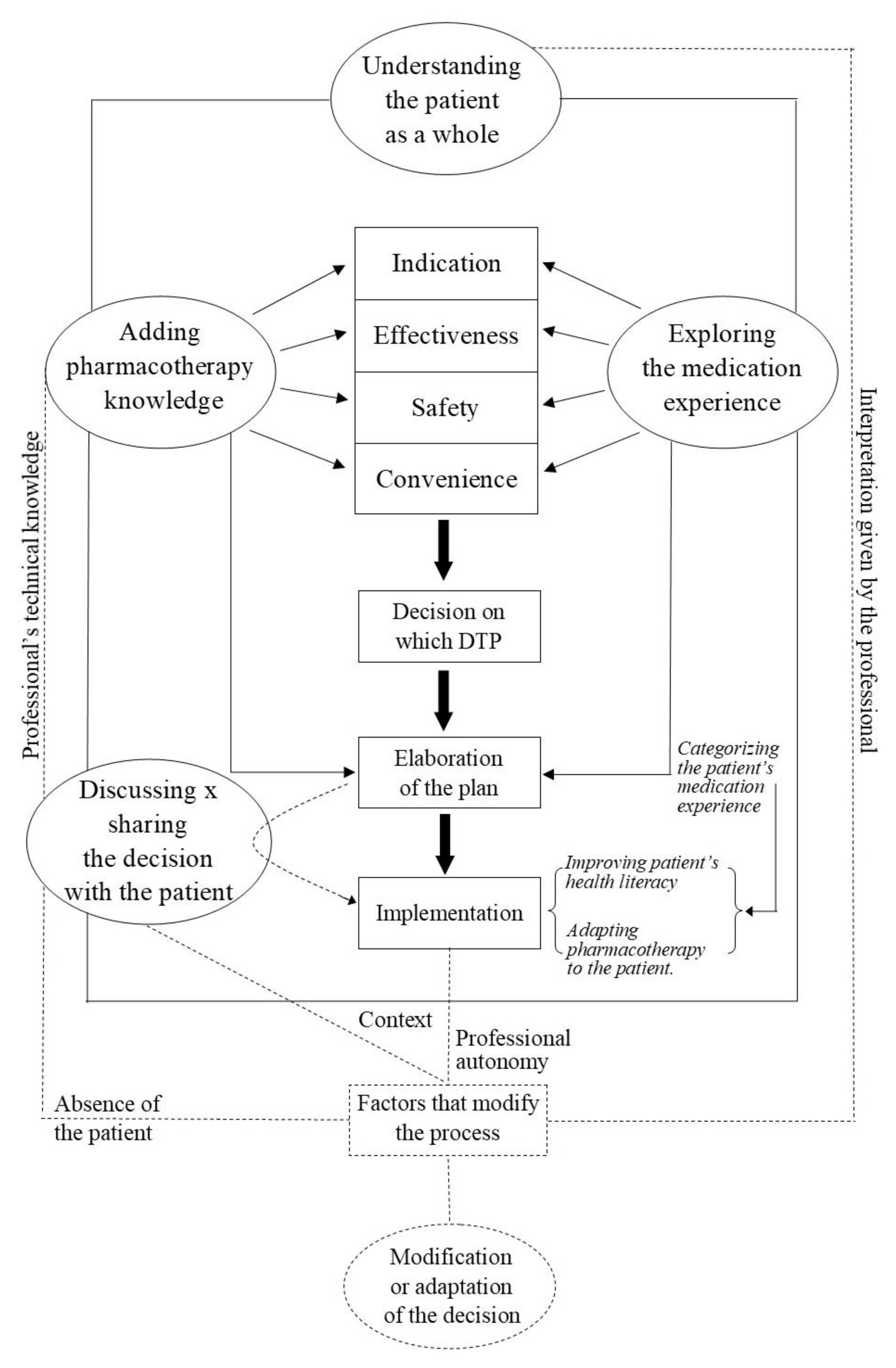
3.3. The Proposed Theoretical Model
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Interview Guide
References
- Patient-Centered Primary Care Collaborative. The Patient-Centered Medical Home: Integrating Comprehensive Medication Management to Optimize Patient Outcomes. June 2012. Available online: https://www.pcpcc.org/sites/default/files/media/medmanagement.pdf (accessed on 2 October 2020).
- Cipolle, R.J.; Strand, L.M.; Morley, P.C. Pharmaceutical Care Practice: The Patient-Centered Approach to Medication, 3rd ed.; McGraw-Hill: New York, NY, USA, 2012. [Google Scholar]
- Neves, C.M.; Nascimento, M.M.G.D.; Silva, D.Á.M.; Ramalho-De-Oliveira, D. Clinical Results of Comprehensive Medication Management Services in Primary Care in Belo Horizonte. Pharmacy 2019, 7, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budlong, H.; Brummel, A.; Rhodes, A.; Nici, H. Impact of Comprehensive Medication Management on Hospital Readmission Rates. Popul. Health Manag. 2018, 21, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, S.A.M.; Melo, A.C.; Pereira, G.C.C.; Santos, D.M.D.S.D.; Grossi, E.B.; Sousa, M.D.C.V.B.; Ramalho-De Oliveira, D.; Soares, A.C. Clinical outcomes of medication therapy management services in primary health care. Braz. J. Pharm. Sci. 2016, 52, 365–373. [Google Scholar] [CrossRef]
- Detoni, K.B.; Oliveira, I.V.; Nascimento, M.M.; Caux, T.R.; Alves, M.R.; Ramalho-De-Oliveira, D. Impact of a medication therapy management service on the clinical status of patients with chronic obstructive pulmonary disease. Int. J. Clin. Pharm. 2016, 39, 95–103. [Google Scholar] [CrossRef]
- Ramalho-De Oliveira, D.; Brummel, A.R.; Miller, D.B. Medication Therapy Management: 10 Years of Experience in a Large Integrated Health Care System. J. Manag. Care Pharm. 2010, 16, 185–195. [Google Scholar] [CrossRef] [Green Version]
- Obreli-neto, P.R.; Marusic, S.; Guidoni, C.M.; Baldoni, A.O.; Renovato, R.D.; Pilger, D.; Cuman, R.K.; Pereira, L.R. Economic evaluation of a pharmaceutical care program for elderly diabetic and hypertensive patients in primary health care: A 36-moa 36-month randomized controlled clinical trial. J. Manag. Care Spec. Pharm. 2005, 21, 66–75. [Google Scholar] [CrossRef]
- Patient Care Process for Delivering Comprehensive Medication Management (CMM): Optimizing Medication Use in Patient-Centered, Team-Based Care Settings. CMM in Primary Care Research Team. July 2018. Available online: http://www.accp.com/cmm_care_process (accessed on 2 October 2020).
- Freitas, E.L.; Ramalho-De-Oliveira, D. Critical thinking in the context of clinical practice: The need to reinvent pharmacy education. Rev. Port. Educ. 2015, 28, 231–250. [Google Scholar] [CrossRef]
- Bartels, C.E. Analysis of Experienced Pharmacist Clinical Decision-Making for Drug Therapy Management in the Ambulatory Care Setting. Ph.D. Thesis, University of Minnesota, Minneapolis, MN, USA, 2013. [Google Scholar]
- LaDuca, A.; Engel, J.D.; Chovan, J.D. An Exploratory Study of Physicians’ Clinical Judgment. Eval. Health Prof. 1988, 11, 178–200. [Google Scholar] [CrossRef]
- Burman, M.E.; Stepans, M.B.; Jansa, N.; Steiner, S. How do NPs make clinical decisions? Nurse Pract. 2002, 27, 57–64. [Google Scholar] [CrossRef]
- Hedberg, B.; Larsson, U.S. Observations, confirmations and strategies—Useful tools in decision-making process for nurses in practice? J. Clin. Nurs. 2003, 12, 215–222. [Google Scholar] [CrossRef]
- Hoffman, K.; Donoghue, J.; Duffield, C. Decision-making in clinical nursing: Investigating contributing factors. J. Adv. Nurs. 2003, 45, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Mamede, S.; Schmidt, H.G.; Rikers, R.M.; Penaforte, J.C.; Coelho-Filho, J.M. Breaking down automaticity: Case ambiguity and the shift to reflective approaches in clinical reasoning. Med. Educ. 2007, 41, 1185–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traynor, M.; Boland, M.; Buus, N. Autonomy, evidence and intuition: Nurses and decision-making. J. Adv. Nurs. 2010, 66, 1584–1591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickson, G.L.; Flynn, L. Nurses’ Clinical Reasoning: Processes and practices of medication safety. Qual. Health Res. 2011, 22, 3–16. [Google Scholar] [CrossRef]
- Marcum, J.A. The Role of Emotions in Clinical Reasoning and Decision Making. J. Med. Philos. 2013, 38, 501–519. [Google Scholar] [CrossRef]
- Wainwright, S.F.; Shepard, K.F.; Harman, L.B.; Stephens, J. Factors That Influence the Clinical Decision Making of Novice and Experienced Physical Therapists. Phys. Ther. 2011, 91, 87–101. [Google Scholar] [CrossRef] [Green Version]
- Simmons, B. Clinical reasoning: Concept analysis. J. Adv. Nurs. 2010, 66, 1151–1158. [Google Scholar] [CrossRef]
- Simmons, B.; Lanuza, D.; Fonteyn, M.; Hicks, F.; Holm, K. Clinical Reasoning in Experienced Nurses. West. J. Nurs. Res. 2003, 25, 701–719. [Google Scholar] [CrossRef]
- American College of Clinical Pharmacy; McBane, S.E.; Dopp, A.L.; Abe, A.; Benavides, S.; Chester, E.A.; Dixon, D.L.; Dunn, M.; Johnson, M.D.; Nigro, S.J.; et al. Collaborative Drug Therapy Management and Comprehensive Medication Management―2015. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2015, 35, e39–e50. [Google Scholar] [CrossRef]
- Butler, A.; Dehner, M.; Gates, R.J.; Shane, P.A.; Chu, M.; DeMartini, L.; Stebbins, M.; De Ybarra, J.N.; Peck, C.; McInnis, T.; et al. Comprehensive Medication Management programs: 2015 status in Southern California. Res. Soc. Adm. Pharm. 2017, 13, 63–87. [Google Scholar] [CrossRef]
- DiPiro, J.T.; Talbert, R.L.; Yee, G.C.; Matzke, G.R.; Wells, G.B.; Posey, M. Pharmacotherapy: A Pathophysiologic Approach, 10th ed.; McGraw-Hill Education: New York, NY, USA, 2016. [Google Scholar]
- Mendonça, S.A.M.; Meireles, B.L.; Freitas, E.L.; Ramalho-De Oliveira, D. Pharmacy Practice Experiential Programs in the Context of Clinical Education. Int. J. Pharm. Pharm. Sci. 2017, 9, 35. [Google Scholar] [CrossRef] [Green Version]
- Charmaz, K. A Construção da Teoria Fundamentada: Guia Prático para Análise Qualitative; Artmed Editora: Porto Alegre, Brazil, 2009. [Google Scholar]
- Daly, K.J. Qualitative Methods for Family Studies and Human Development; SAGE: Los Angeles, CA, USA, 2007. [Google Scholar]
- Strauss, A.; Corbin, J. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; SAGE: Thousand Oaks, CA, USA, 2008. [Google Scholar]
- Ramalho-de-Oliveira, D. The Reality of Pharmaceutical Care Based Medication Therapy Management: Patients’, Pharmacists’ and Students’ Perspectives; Academic Publishing: Köln, Germany, 2010. [Google Scholar]
- Freitas, E.L. Why Do I Think the Way I do? Troubling the Concept of Critical Thinking in Pharmacy Classrooms. Ph.D. Thesis, University of Minnesota, Minneapolis, MN, USA, 2014. [Google Scholar]
- Facione, N.C.; Facione, P.A. Critical thinking and clinical judgment. In Critical Thinking and Clinical Reasoning in the Health Sciences: A Teaching Anthology; The California Academic Press: Millbrae, CA, USA, 2008; pp. 1–13. [Google Scholar]
- Sorensen, T.D.; Hager, K.D.; Schlichte, A.; Janke, K. A Dentist, Pilot, and Pastry Chef Walk into a Bar… Why Teaching PPCP is Not Enough. Am. J. Pharm. Educ. 2020, 84, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Losinski, V. Educating for Action: Understanding the Development of Pharmaceutical Care Practitioners. Ph.D. Thesis, University of Minnesota, Minneapolis, MN, USA, 2011. [Google Scholar]
- Aleluia, I.M.B.; Carvalho, P.M., Jr.; Menezes, M.S. A way to assess students’ clinical reasoning. Med. Educ. 2010, 44, 1145–1146. [Google Scholar] [CrossRef] [PubMed]
- Etminan, M.; Wright, J.M.; Carleton, B. Evidence-based pharmacotherapy: Review of basic concepts and applications in clinical practice. Ann. Pharmacother. 1998, 32, 1193–1200. [Google Scholar] [CrossRef]
- Adams, R. Health literacy—A new concept for general practice? Aust. Fam. Phys. 2009, 38, 144–147. [Google Scholar]
- Elwyn, G.; Frosch, D.L.; Thomson, R.; Joseph-Williams, N.; Lloyd, A.; Kinnersley, P.; Cording, E.; Tomson, D.; Dodd, C.; Rollnick, S.; et al. Shared Decision Making: A Model for Clinical Practice. J. Gen. Intern. Med. 2012, 27, 1361–1367. [Google Scholar] [CrossRef] [Green Version]
- Elwyn, G.; Dehlendorf, C.; Epstein, R.M.; Marrin, K.; White, J.; Frosch, D.L. Shared Decision Making and Motivational Interviewing: Achieving Patient-Centered Care across the Spectrum of Health Care Problems. Ann. Fam. Med. 2014, 12, 270–275. [Google Scholar] [CrossRef] [Green Version]
- Freitas, E.L. Revelando a Experiência do Paciente com a Prática da Atenção Farmacêutica: Uma Abordagem Qualitativa. Master’s Thesis, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil, 2005. [Google Scholar]
- De Caux, T.R. Meus Filhos me Perguntam, ‘por que Consulta com a Farmacêutica?’ Experiência de Pacientes com um Serviço de Gerenciamento da Terapia Medicamentosa. Undergraduate Thesis, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil, 2015. [Google Scholar]
- Towle, A.; Godolphin, W.; Grams, G.; Lamarre, A. Putting informed and shared decision making into practice. Health Expect. 2006, 9, 321–332. [Google Scholar] [CrossRef] [Green Version]
- Gwyn, R.; Elwyn, G. When is a shared decision not (quite) a shared decision? Negotiating preferences in a general practice encounter. Soc. Sci. Med. 1999, 49, 437–447. [Google Scholar] [CrossRef]
- Couët, N.; Desroches, S.; Robitaille, H.; Vaillancourt, H.; Leblanc, A.; Turcotte, S.; Elwyn, G.; Légaré, F. Assessments of the extent to which health-care providers involve patients in decision making: A systematic review of studies using the OPTION instrument. Health Expect. 2015, 18, 542–561. [Google Scholar] [CrossRef]
- Joseph-Williams, N.; Elwyn, G.; Edwards, A. Knowledge is not power for patients: A systematic review and thematic synthesis of patient-reported barriers and facilitators to shared decision making. Patient Educ. Couns. 2014, 94, 291–309. [Google Scholar] [CrossRef] [PubMed]
- Ramalho-de-Oliveira, D. Atenção Farmacêutica: Da Filosofia ao Gerenciamento da Terapia Medicamentosa; RCN Editora: São Paulo, Brazil, 2011. [Google Scholar]
- Weiss, M.C.; Sutton, J. The changing nature of prescribing: Pharmacists as prescribers and challenges to medical dominance. Sociol. Health Illn. 2009, 31, 406–421. [Google Scholar] [CrossRef] [PubMed]
- Schafer, K.M.; Gionfriddo, M.R.; Boehm, D.H. Shared decision making and medication therapy management with the use of an interactive template. J. Am. Pharm. Assoc. 2016, 56, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.M.F.; Amaral, C.F.S. Medicina centrada no paciente e ensino médico: A importância do cuidado com a pessoa e o poder médico. Rev. Bras. Educ. Méd. 2008, 32, 90–97. [Google Scholar] [CrossRef] [Green Version]
- Legault, F.; Humbert, J.; Amos, S.; Hogg, W.; Ward, N.; Dahrouge, S.; Ziebell, L. Difficulties Encountered in Collaborative Care: Logistics Trumps Desire. J. Am. Board Fam. Med. 2012, 25, 168–176. [Google Scholar] [CrossRef]


{kind=link}
| Participating Pharmacists | Setting Providing CMM Services | Period of Time in Practice (Years) * | Number of Patients Assisted * |
|---|---|---|---|
| P1 | Primary care clinic | 10 | More than 150 |
| P2 | Specialty clinic | 8 | More than 400 |
| P3 | Primary care clinic | 2 | 200 |
| P4 | Public Pharmacy | 1 | 50 |
| P5 | Clinic at university | 13 | More than 500 |
| P6 | Primary care clinic | 3 | 69 |
| P7 | Primary care clinic | 1 | 65 |
| P8 | Specialty clinic | 2 | More than 200 |
| P9 | Specialty clinic | 1 | 20 |
| P10 | Primary care clinic | 1 | 200 |
| P11 | Clinic at university | 16 | More than 300 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira, I.V.; Nascimento, Y.d.A.; Ramalho-de-Oliveira, D. Decision-Making Process in Comprehensive Medication Management Services: From the Understanding to the Development of a Theoretical Model. Pharmacy 2020, 8, 180. https://doi.org/10.3390/pharmacy8040180
Oliveira IV, Nascimento YdA, Ramalho-de-Oliveira D. Decision-Making Process in Comprehensive Medication Management Services: From the Understanding to the Development of a Theoretical Model. Pharmacy. 2020; 8(4):180. https://doi.org/10.3390/pharmacy8040180
Chicago/Turabian StyleOliveira, Isabela Viana, Yone de Almeida Nascimento, and Djenane Ramalho-de-Oliveira. 2020. "Decision-Making Process in Comprehensive Medication Management Services: From the Understanding to the Development of a Theoretical Model" Pharmacy 8, no. 4: 180. https://doi.org/10.3390/pharmacy8040180
APA StyleOliveira, I. V., Nascimento, Y. d. A., & Ramalho-de-Oliveira, D. (2020). Decision-Making Process in Comprehensive Medication Management Services: From the Understanding to the Development of a Theoretical Model. Pharmacy, 8(4), 180. https://doi.org/10.3390/pharmacy8040180