
Disposal Practices of Unused and Leftover Medicines in the Households of Dhaka Metropolis

 ,
,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. In-Depth Interviews
2.4. Data Analysis
2.5. Questionnaire Item Development, Samples, and Population
3. Results
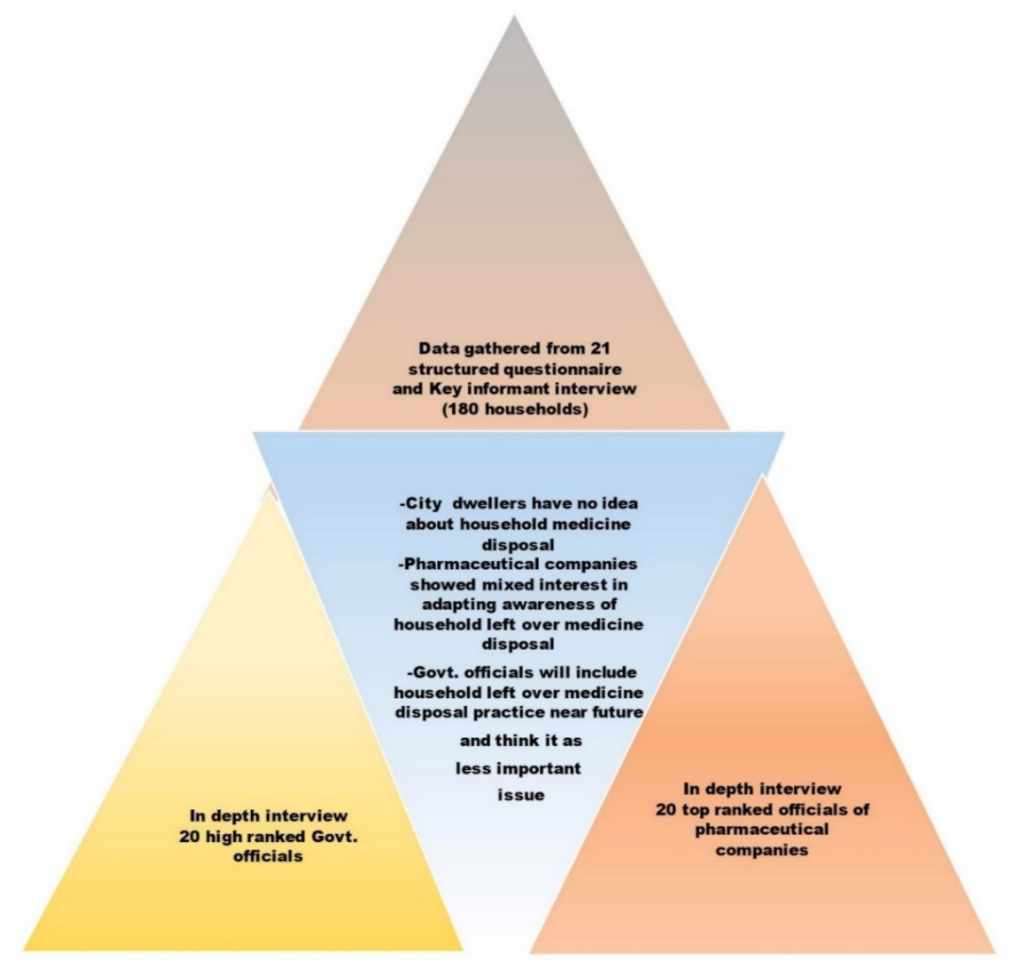
3.1. Feedback from Key Informant Interview
3.2. Feedback from an In-Depth Interview of Top-Ranked Officials of Pharmaceutical Companies
3.3. Feedback from the In-Depth Interview of Top-Ranked Officials of Government Officials
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Al-Naggar, R.A.; Alareefi, A. Patientsû opinion and practice toward unused medication disposal in malaysia: A qualitative study. Thai J. Pharm. Sci. 2010, 34, 117–123. [Google Scholar] [CrossRef]
- Siler, S.; Duda, S.; Brown, R.; Gbemudu, J.; Weier, S.; Glaudemans, J. Safe Disposal of Unused Controlled Substances/Current Challenges and Opportunities for Reform; King Pharmaceuticals, Inc.: Washington, DC, USA, 2008. [Google Scholar]
- Musson, S.E.; Townsend, T.; Seaburg, K.; Mousa, J. A continuous collection system for household pharmaceutical wastes: A pilot project. J. Air Waste Manag. Assoc. 2007, 57, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Ligon, A.P.; Zuehlke, S.; Spiteller, M. GC-MS analysis of organic compounds in wastewater and sewage sludge. J. Sep. Sci. 2008, 31, 143–150. [Google Scholar] [CrossRef]
- Vellinga, A.; Cormican, S.; Driscoll, J.; Furey, M.; O’Sullivan, M.; Cormican, M. Public practice regarding disposal of unused medicines in Ireland. Sci. Total Environ. 2014, 478, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Hignite, C.; Azarnoff, D.L. Drugs and drug metabolites as environmental contaminants: Chlorophenoxyisobutyrate and salicylic acid in sewage water effluent. Life Sci. 1977, 20, 337–341. [Google Scholar] [CrossRef]
- Burke, T.J.; Segrin, C. Examining Diet- and Exercise-Related Communication in Romantic Relationships: Associations with Health Behaviors. Health Commun. 2014, 29, 877–887. [Google Scholar] [CrossRef]
- Kolpin, D.W.; Furlong, E.T.; Meyer, M.T.; Thurman, E.M.; Zaugg, S.D.; Barber, L.B.; Buxton, H.T. Pharmaceuticals, Hormones, and Other Organic Wastewater Contaminants in U.S. Streams, 1999−2000: A National Reconnaissance. Environ. Sci. Technol. 2002, 36, 1202–1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamba, P.F.; Kaggwa, B.; Munanura, E.I.; Okurut, T.; Kitutu, F.E. Why regulatory indifference towards pharmaceutical pollution of the environment could be a missed opportunity in public health protection. A holistic view. Pan Afr. Med. J. 2017, 27, 77. [Google Scholar]
- Barnes, K.K.; Kolpin, D.W.; Furlong, E.T.; Zaugg, S.D.; Meyer, M.T.; Barber, L.B. A national reconnaissance of pharmaceuticals and other organic wastewater contaminants in the United States—I) Groundwater. Sci. Total Environ. 2008, 402, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Loos, R.; Locoro, G.; Comero, S.; Contini, S.; Schwesig, D.; Werres, F.; Balsaa, P.; Gans, O.; Weiss, S.; Blaha, L.; et al. Pan-European survey on the occurrence of selected polar organic persistent pollutants in ground water. Water Res. 2010, 44, 4115–4126. [Google Scholar] [CrossRef] [PubMed]
- Ashton, D.; Hilton, M.; Thomas, K.V. Investigating the environmental transport of human pharmaceuticals to streams in the United Kingdom. Sci. Total Environ. 2004, 333, 167–184. [Google Scholar] [CrossRef]
- Granger, A.J.; Nicoll, R.A. Expression mechanisms underlying long-term potentiation: A postsynaptic view, 10 years on. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369. [Google Scholar] [CrossRef] [Green Version]
- Huber, S.; Remberger, M.; Kaj, L.; Schlabach, M.; Jörundsdóttir, H.T.; Vester, J.; Arnórsson, M.; Mortensen, I.; Schwartson, R.; Dam, M. A first screening and risk assessment of pharmaceuticals and additives in personal care products in waste water, sludge, recipient water and sediment from Faroe Islands, Iceland and Greenland. Sci. Total Environ. 2016, 562, 13–25. [Google Scholar] [CrossRef]
- Hughes, S.R.; Kay, P.; Brown, L.E. Global synthesis and critical evaluation of pharmaceutical data sets collected from river systems. Environ. Sci. Technol. 2013, 47, 661–677. [Google Scholar] [CrossRef]
- Humphreys, E.H.; Janssen, S.; Heil, A.; Hiatt, P.; Solomon, G.; Miller, M.D. Outcomes of the California ban on pharmaceutical lindane: Clinical and ecologic impacts. Environ. Health Perspect. 2008, 116, 297–302. [Google Scholar] [CrossRef]
- Verlicchi, P.; Al Aukidy, M.; Zambello, E. Occurrence of pharmaceutical compounds in urban wastewater: Removal, mass load and environmental risk after a secondary treatment-A review. Sci. Total Environ. 2012, 429, 123–155. [Google Scholar] [CrossRef] [PubMed]
- Jones, O.A.H.; Voulvoulis, N.; Lester, J.N. Human pharmaceuticals in wastewater treatment processes. Crit. Rev. Environ. Sci. Technol. 2005, 35, 401–427. [Google Scholar] [CrossRef]
- Stackelberg, P.E.; Gibs, J.; Furlong, E.T.; Meyer, M.T.; Zaugg, S.D.; Lippincott, R.L. Efficiency of conventional drinking-water-treatment processes in removal of pharmaceuticals and other organic compounds. Sci. Total Environ. 2007, 377, 255–272. [Google Scholar] [CrossRef] [PubMed]
- Watkinson, A.J.; Murby, E.J.; Kolpin, D.W.; Costanzo, S.D. The occurrence of antibiotics in an urban watershed: From wastewater to drinking water. Sci. Total Environ. 2009, 407, 2711–2723. [Google Scholar] [CrossRef]
- Benotti, M.J.; Trenholm, R.A.; Vanderford, B.J.; Holady, J.C.; Stanford, B.D.; Snyder, S.A. Pharmaceuticals and endocrine disrupting compounds in U.S. drinking water. Environ. Sci. Technol. 2009, 43, 597–603. [Google Scholar] [CrossRef] [Green Version]
- Kookana, R.S.; Williams, M.; Boxall, A.B.A.; Larsson, D.G.J.; Gaw, S.; Choi, K.; Yamamoto, H.; Thatikonda, S.; Zhu, Y.G.; Carriquiriborde, P. Potential ecological footprints of active pharmaceutical ingredients: An examination of risk factors in low-, middle- and high-income countries. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369. [Google Scholar] [CrossRef] [PubMed]
- Kusturica, M.P.; Tomić, Z.; Bukumirić, Z.; Horvat, O.; Pavlović, N.; Mikov, M.; Sabo, A. Antibiotics in Serbian Households: A Source of Potential Health and Environmental Threats? Cent. Eur. J. Public Health 2015, 23, 90–94. [Google Scholar] [CrossRef] [Green Version]
- Heberer, T. Occurrence, fate, and removal of pharmaceutical residues in the aquatic environment: A review of recent research data. Toxicol. Lett. 2002, 131, 5–17. [Google Scholar] [CrossRef]
- McEneff, G.; Barron, L.; Kelleher, B.; Paull, B.; Quinn, B. The determination of pharmaceutical residues in cooked and uncooked marine bivalves using pressurised liquid extraction, solid-phase extraction and liquid chromatography-tandem mass spectrometry. Anal. Bioanal. Chem. 2013, 405, 9509–9521. [Google Scholar] [CrossRef] [PubMed]
- Uno, K. Oxytetracycline and oxolinic acid residues in kuruma prawn (Penaeus japonicus) and the effect of cooking procedures on the residues. J. Food Hyg. Soc. Jpn 2002, 43, 62–67. [Google Scholar] [CrossRef] [Green Version]
- Uno, K.; Aoki, T.; Kleechaya, W.; Ruangpan, L.; Tanasomwang, V. Pharmacokinetics of oxolinic acid in black tiger shrimp, Penaeus monodon Fabricius, and the effect of cooking on residues. Aquac. Res. 2006, 37, 826–833. [Google Scholar] [CrossRef]
- Wang, Y.; Yuen, K.H.; Ng, W.K. Deposition of tocotrienols and tocopherols in the tissues of red hybrid tilapia, Oreochromis sp., fed a tocotrienol-rich fraction extracted from crude palm oil and its effect on lipid peroxidation. Aquaculture 2006, 253, 583–591. [Google Scholar] [CrossRef]
- Uno, K.; Chaweepack, T.; Ruangpan, L. Pharmacokinetics and bioavailability of oxytetracycline in vannamei shrimp (Penaeus vannamei) and the effect of processing on the residues in muscle and shell. Aquac. Int. 2010, 18, 1003–1015. [Google Scholar] [CrossRef]
- Pharmaceutical Waste Compliance For Healthcare Facilities. Available online: https://www.state.nj.us/dep/enforcement/1%20RCRA%20Pharmaceutical%20Waste%20-%20Best%20Management%20Practices%20-Vona%205-17-12.pdf (accessed on 20 March 2021).
- Jaseem, M.; Kumar, P.; Mariam John, R.; Muhammed Jaseem, C. An overview of waste management in pharmaceutical industry. Pharma Innov. J. 2017, 6, 158–161. [Google Scholar]
- Askarian, M.; Heidarpoor, P.; Assadian, O. A total quality management approach to healthcare waste management in Namazi Hospital, Iran. Waste Manag. 2010, 30, 2321–2326. [Google Scholar] [CrossRef] [PubMed]
- Ruhoy, I.S.; Daughton, C.G. Types and quantities of leftover drugs entering the environment via disposal to sewage—Revealed by coroner records. Sci. Total Environ. 2007, 388, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Easy Steps for Getting Rid of Unused Medication. Available online: https://www.winknews.com/2017/04/11/easy-steps-for-getting-rid-of-unused-medication/ (accessed on 20 March 2021).
- The Problem With Expired Medication—Consumer Reports. Available online: https://www.consumerreports.org/drug-safety/the-problem-with-expired-medication/ (accessed on 25 March 2021).
- Bronstein, A.C.; Spyker, D.A.; Cantilena, L.R.; Green, J.L.; Rumack, B.H.; Dart, R.C. 2010 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 28th Annual Report. Proc. Clin. Toxicol. 2011, 49, 910–941. [Google Scholar] [CrossRef]
- Guidelines for Safe Disposal of Unwanted Pharmaceuticals in and after Emergencies; World Health Organization: Geneva, Switzerland, 1999.
- Tischler, L.; Buzby, M.; Finan, D.S.; Cunningham, V.L. Landfill disposal of unused medicines reduces surface water releases. Integr. Environ. Assess. Manag. 2013, 9, 142–154. [Google Scholar] [CrossRef]
- National Association of Boards of Pharmacy. Available online: https://nabp.pharmacy/ (accessed on 29 March 2021).
- How to Dispose of Medication|BeMedWise. Available online: https://www.bemedwise.org/your-medicines-self-care/drug-storage-and-disposal/ (accessed on 15 March 2021).
- Safe Medication Disposal | Walgreens. Available online: https://www.walgreens.com/topic/pharmacy/safe-medication-disposal.jsp (accessed on 20 March 2021).
- AMA Medical Student Section Education Guide Election Manual Convention Committees GC Actions Items. Available online: https://www.ama-assn.org/system/files/2019-05/mss-election-manual_0.pdf (accessed on 20 March 2021).
- Pharmaceutical Waste & Medication Disposal—Stericycle. Available online: https://www.stericycle.com/en-us/our-solutions/medical-waste-disposal/pharmaceutical-waste (accessed on 20 March 2021).
- The National Health Service (Pharmaceutical and Local Pharmaceutical Services) Regulations 2013. Available online: https://www.legislation.gov.uk/uksi/2013/349/contents/made (accessed on 25 March 2021).
- Mashiane, M. Disposal Practices for Unwanted Medicines from Households in Johannesburg, 1st ed.; LAP LAMBERT Academic Publishing: Saarbrücken, Germany, 2017. [Google Scholar]
- Pharmaceutical Disposal Programs for the Public: A Canadian Perspective. Available online: https://cdn.ymaws.com/www.productstewardship.us/resource/resmgr/imported/Takeback%20%282%29.pdf (accessed on 20 March 2021).
- Safe disposal of prescription drugs—Canada.ca. Available online: https://www.canada.ca/en/health-canada/services/safe-disposal-prescription-drugs.html (accessed on 25 March 2021).
- EUR-Lex—32001L0083—EN—EUR-Lex. Available online: https://eur-lex.europa.eu/legal-content/en/ALL/?uri=CELEX%3A32001L0083 (accessed on 20 March 2021).
- Montserrat Moliner, A.; Waligora, J. The European Union policy in the field of rare diseases. In Advances in Experimental Medicine and Biology; Springer: New York, NY, USA, 2017; Volume 1031, pp. 561–587. [Google Scholar]
- Kristina, S.A.; Wiedyaningsih, C.; Cahyadi, A.; Ridwan, B.A. A Survey on Medicine Disposal Practice among Households in Yogyakarta. Asian J. Pharm. 2018, 12, 955. [Google Scholar]
- Bashatah, A.; Wajid, S. Knowledge and disposal practice of leftover and expired medicine: A cross-sectional study from nursing and pharmacy students’ perspectives. Int. J. Environ. Res. Public Health 2020, 17, 2068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogler, S.; de Rooij, R.H.P.F. Medication wasted—Contents and costs of medicines ending up in household garbage. Res. Soc. Adm. Pharm. 2018, 14, 1140–1146. [Google Scholar] [CrossRef]
- Osei-Djarbeng, S.N.; Larbi, G.O.; Abdul-Rahman, R.; Osei-Asante, S.; Owusu-Antwi, R.; Samuel Osei-Djarbeng, C.N. The Pharma Innovation Journal 2015; 4(8): 85-88 Household acquisition of medicines and disposal of expired and unused medicines at two suburbs (Bohyen and Kaase) in Kumasi-Ghana. Pharma Innov. J. 2015, 4, 85–88. [Google Scholar]
- Barnett-Itzhaki, Z.; Berman, T.; Grotto, I.; Schwartzberg, E. Household medical waste disposal policy in Israel. Isr. J. Health Policy Res. 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Banwat, S.B.; Auta, A.; Dayom, D.W.; Buba, Z. Assessment of the storage and disposal of medicines in some homes in Jos north local government area of Plateau state, Nigeria. Trop. J. Pharm. Res. 2016, 15, 989–993. [Google Scholar] [CrossRef] [Green Version]
- Maharana, S.; Paul, B.; Dasgupta, A.; Garg, S. Storage, reuse, and disposal of unused medications: A cross-sectional study among rural households of Singur, West Bengal. Int. J. Med. Sci. Public Health 2017, 1. [Google Scholar] [CrossRef] [Green Version]
- Chung, S.; Brooks, B.W. Identifying household pharmaceutical waste characteristics and population behaviors in one of the most densely populated global cities. Resour. Conserv. Recycl. 2019, 140, 267–277. [Google Scholar] [CrossRef]
- The Multi-billion Dollar Industry Pharmaceutical Industry of Bangladesh Industry Overview Ratings of Listed Pharmaceutical Companies View of Industry Expert Financials of listed Pharmaceutical Companies Industry Size Industry Growth Expected Growth. Available online: https://www.arx.cfa/~/media/2A85F9B2CEAB43CFAF325AB54F3EF404 (accessed on 30 March 2021).
- Bangladesh Pharmaceutical Market Future Opportunity Outlook 2025. Available online: https://www.researchandmarkets.com/reports/5125539/bangladesh-pharmaceutical-market-future (accessed on 5 April 2021).
- Shailendra Mudgal, A.; De Toni, A.; Shailendra Mudgal, O.; Wiberg, O. Study on the environmental risks of medicinal products, Final Report prepared for Executive Agency for Health and Consumers; 2013. Available online: https://ec.europa.eu/health/sites/health/files/files/environment/study_environment.pdf (accessed on 20 March 2021).
- Van der Geest, S. Part 1: The Illegal Distribution of Western Medicines in Developing Countries: Pharmacists, Drug Pedlars, Injection Doctors and Others. A Bibliographic Exploration. Med. Anthropol. 1982, 6, 197–219. [Google Scholar] [CrossRef]
- Glassmeyer, S.T.; Hinchey, E.K.; Boehme, S.E.; Daughton, C.G.; Ruhoy, I.S.; Conerly, O.; Daniels, R.L.; Lauer, L.; McCarthy, M.; Nettesheim, T.G.; et al. Disposal practices for unwanted residential medications in the United States. Environ. Int. 2009, 35, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Aschenbrenner, D.S. Disposal of Unused Drugs in the Community. Am. J. Nurs. 2015, 115, 20. [Google Scholar] [CrossRef]
- Guirguis, K. Medications collected for disposal by outreach pharmacists in Australia. Pharm. World Sci. 2010, 32, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Jonjić, D.; Vitale, K. Issues around household pharmaceutical waste disposal through community pharmacies in Croatia. Int. J. Clin. Pharm. 2014, 36, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.Y.C.; Peake, B.M.; Braund, R. Disposal practices for unused medications in New Zealand community pharmacies. J. Prim. Health Care 2011, 3, 197–203. [Google Scholar]
- Atinafu, T.; Takele, A.; Kassie, A.; Yehualaw, A.; Tesfaw, G.; Desseno, T.; Mekonnen, T.; Fentie, M. Unused Medications Disposal Practice: The case of Patients Visiting University of Gondar Specialized Teaching Hospital, Gondar, Ethiopia. IJPSR 2014, 5, 999–1005. [Google Scholar]
- Ayele, Y.; Mamu, M. Assessment of knowledge, attitude and practice towards disposal of unused and expired pharmaceuticals among community in Harar city, Eastern Ethiopia. J. Pharm. Policy Pract. 2018, 11. [Google Scholar] [CrossRef]
- Stoddard, K.I.; Hodge, V.; Maxey, G.; Tiwari, C.; Cready, C.; Huggett, D.B. Investigating Research Gaps of Pharmaceutical take back Events: An Analysis of take back Program Participants’ Socioeconomic, Demographic, and Geographic Characteristics and the Public Health Benefits of take back Programs. Environ. Manag. 2017, 59, 871–884. [Google Scholar] [CrossRef]
- Manocha, S.; Suranagi, U.D.; Sah, R.K.; Chandane, R.D.; Kulhare, S.; Goyal, N.; Tanwar, K. Disposal Practices of Unused and Expired Medicines among General Public in Delhi & National Capital Region, India. Curr. Drug Saf. 2019, 14. [Google Scholar] [CrossRef]
- Kelly, F.; McMillan, S.; Spinks, J.; Bettington, E.; Wheeler, A.J. ‘You don’t throw these things out:’ an exploration of medicines retention and disposal practices in Australian homes. BMC Public Health 2018, 18, 1026. [Google Scholar] [CrossRef]
- Teni, F.S.; Birru, E.M.; Surur, A.S.; Belay, A.; Wondimsigegn, D.; Gelayee, D.A.; Shewamene, Z. Pattern and predictors of medicine use among households in Gondar Town, northwestern Ethiopia: A community-based medicine utilization study. BMC Res. Notes 2017, 10. [Google Scholar] [CrossRef] [Green Version]
- Ariffin, M.; Zakili, T.S.T. Household Pharmaceutical Waste Disposal in Selangor, Malaysia—Policy, Public Perception, and Current Practices. Environ. Manag. 2019, 64, 509–519. [Google Scholar] [CrossRef]
- Rogowska, J.; Zimmermann, A.; Muszyńska, A.; Ratajczyk, W.; Wolska, L. Pharmaceutical Household Waste Practices: Preliminary Findings from a Case Study in Poland. Environ. Manag. 2019, 64, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Massoud, M.A.; Chami, G.; Al-Hindi, M.; Alameddine, I. Assessment of Household Disposal of Pharmaceuticals in Lebanon: Management Options to Protect Water Quality and Public Health. Environ. Manag. 2016, 57, 1125–1137. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.; Chan, S.S.; Conway, F.D.L.; Phd, D.S. Environmental stewardship practices of veterinary professionals and educators related to use and disposal of pharmaceuticals and personal care products. J. Am. Vet. Med. Assoc. 2018, 252, 596–604. [Google Scholar] [CrossRef]
- Hassan, M.M.; Ahmed, S.A.; Rahman, K.A.; Biswas, T.K. Pattern of medical waste management: Existing scenario in Dhaka City, Bangladesh. BMC Public Health 2008, 8. [Google Scholar] [CrossRef] [Green Version]
- Akici, A.; Aydin, V.; Kiroglu, A. Assessment of the association between drug disposal practices and drug use and storage behaviors. Saudi Pharm. J. 2018, 26, 7–13. [Google Scholar] [CrossRef]
- Bettington, E.; Spinks, J.; Kelly, F.; Gallardo-Godoy, A.; Nghiem, S.; Wheeler, A.J. When is a medicine unwanted, how is it disposed, and how might safe disposal be promoted? insights from the Australian population. Aust. Health Rev. 2018, 42, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Bashaar, M.; Thawani, V.; Hassali, M.A.; Saleem, F. Disposal practices of unused and expired pharmaceuticals among general public in Kabul. BMC Public Health 2017, 17, 45. [Google Scholar] [CrossRef] [Green Version]
- Kusturica, M.P.; Sabo, A.; Tomic, Z.; Horvat, O.; Šolak, Z. Storage and disposal of unused medications: Knowledge, behavior, and attitudes among Serbian people. Int. J. Clin. Pharm. 2012, 34, 604–610. [Google Scholar] [CrossRef]
- Herring, M.E.; Shah, S.K.; Shah, S.K.; Gupta, A.K. Current regulations and modest proposals regarding disposal of unused opioids and other controlled substances. J. Am. Osteopath. Assoc. 2008, 108, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Zorpas, A.A.; Dimitriou, M.; Voukkali, I. Disposal of household pharmaceuticals in insular communities: Social attitude, behaviour evaluation and prevention activities. Environ. Sci. Pollut. Res. 2018, 25, 26725–26735. [Google Scholar] [CrossRef] [PubMed]
- Egan, K.L.; Gregory, E.; Sparks, M.; Wolfson, M. From dispensed to disposed: Evaluating the effectiveness of disposal programs through a comparison with prescription drug monitoring program data. Am. J. Drug Alcohol Abuse 2017, 43, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Wieczorkiewicz, S.M.; Kassamali, Z.; Danziger, L.H. Behind closed doors: Medication storage and disposal in the home. Ann. Pharmacother. 2013, 47, 482–489. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sources of Data Collection | Sample Size |
|---|---|
| Structured questionnaire and key informant interview | 180 participants from households |
| In-depth Interview | 40 top-ranked officials |
| 6 |
| 7 |
| 13 |
| 5 |
| 7 |
| 5 |
| 3 |
| Parameters | Key Informants/Participants Who Responded in Quantitative Questionnaire and Key Informant Interview (180) | Participants Who Responded in the In-Depth Interview (40) | ||
|---|---|---|---|---|
| Male | Female | Male | Female | |
| Gender | 42 (23%) | 138 (77%) | 28 (70%) | 12 (30%) |
| Age range | ||||
| 18–29 | 4 (10%) | 23 (17%) | 3 (11%) | 2 (17%) |
| 30–41 | 9 (21%) | 67 (49%) | 7 (25%) | 4 (33%) |
| 42–53 | 12 (29%) | 26 (19%) | 11 (39%) | 5 (42%) |
| 54–65 | 17 (40%) | 22 (16%) | 7 (25%) | 1 (8%) |
| Educational qualification | ||||
| No general education | 5 (12%) | 17 (12%) | 0 (0%) | 0 (0%) |
| Primary education | 12 (29%) | 43 (31%) | 0 (0%) | 0 (0%) |
| Secondary education | 19 (45%) | 57 (41%) | 0 (0%) | 0 (0%) |
| Graduated | 6 (14%) | 21 (15%) | 28 (100%) | 12 (100%) |
| Marital status | ||||
| Married | 22 (52%) | 85 (62%) | 25 (89%) | 12 (100%) |
| Unmarried | 17 (40%) | 48 (35%) | 2(7%) | 0 (0%) |
| Others(widower/widow) | 3(7%) | 5 (4%) | 1 (4%) | 0 (0%) |
| Financial condition | ||||
| Poor | 7 (17%) | 18 (13%) | 0 (0%) | 0 (%) |
| Lower-middle class | 11 (26%) | 21 (15%) | 0 (0%) | 0 (0%) |
| Middle-middle class | 15 (36%) | 54 (39%) | 0 (0%) | 0 (%) |
| Higher-middle class | 7 (17%) | 33 (24%) | 19 (68%) | 8 (67%) |
| Rich | 2 (5%) | 12 (9%) | 9 (32%) | 4 (33%) |
| Information Obtained from Questionnaires | Percentage (Yes) |
|---|---|
| |
| The patient claimed to be taking medicine after being prescribed by the doctor | 94 |
| Completing the full course of medicine as per the doctor’s prescription | 62 |
| Following the instructions, while taking medicines | 81 |
| Keeping medicines out of reach of children | 79 |
| Reading the insertion/drug literature before taking medicines | 56 |
| Following dosage regimens, while taking medicines | 66 |
| Storing medicines according to the directions for proper storage conditions | 70 |
| Follow the direction of measurable medicine | 85 |
| |
| Borrowing or sharing own medicine with others | 57 |
| Stopping medicine intake once starting to feel better | 58 |
| Consuming the leftover antibiotics | 46 |
| Following the same prescription for taking medicine after facing a recurrence of symptoms | 26 |
| |
| Checking the expiry date of medicines before throwing them out | 91 |
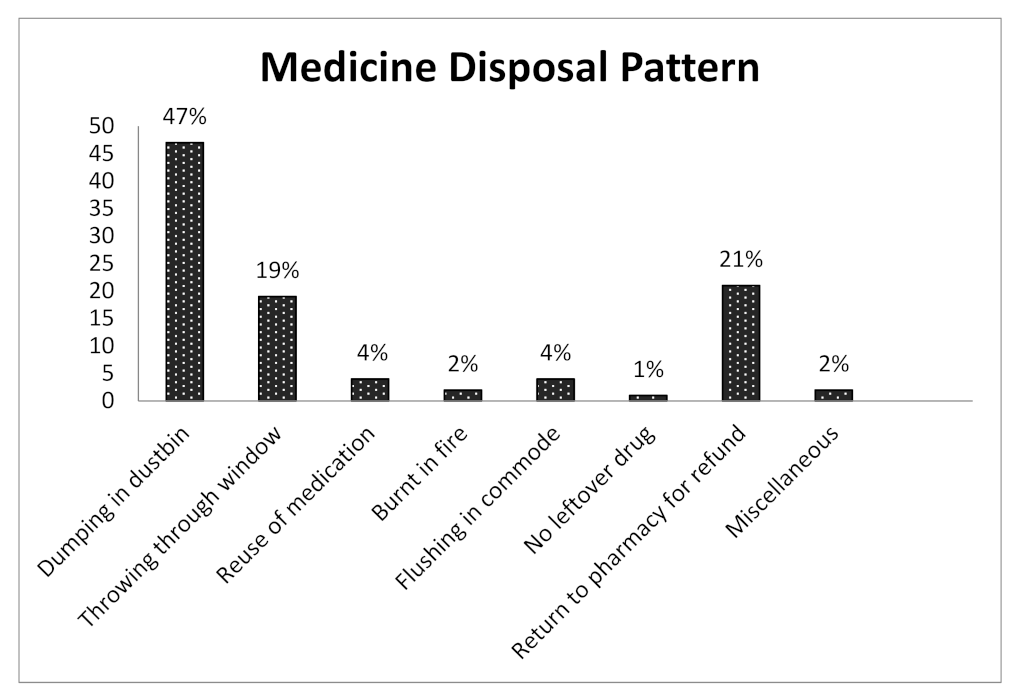
| Throwing out the leftover medicines | 33 |
| Having any idea about drug disposal | 33 |
| Having any idea about drug pollution | 26 |
| Experiencing incidences regarding unsafe drug disposal in own household | 87 |
| Having desire to take part in any medicine take-back program | 72 |
| Having the willingness to pay for that | 34 |
| Public education is required to create awareness | 100 |
| It is the government’s responsibility to dispose of medicines in a safe place | 72 |
| Habits Regarding Buying Medicine Without a Prescription | ||||||
| Buying Antibiotics, sedatives, sex stimulants (including OTC) without prescription | Buying all types of medicine (including OTC) with prescription | |||||
| Number | 58 (32%) | 122 (68%) | ||||
| The Idea about Medication Intake | ||||||
| No ideas about wrong medication intake | Having less idea about wrong medication intake | Have a proper idea about wrong medication intake | Being afraid of death due to wrong medication intake. | Miscellaneous | ||
| Number | 38 (21%) | 67 (37%) | 25 (14%) | 44 (24%) | 6 (4%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Begum, M.M.; Rivu, S.F.; Hasan, M.M.A.; Nova, T.T.; Rahman, M.M.; Alim, M.A.; Uddin, M.S.; Islam, A.; Nurnahar; Tabassum, N.; et al. Disposal Practices of Unused and Leftover Medicines in the Households of Dhaka Metropolis. Pharmacy 2021, 9, 103. https://doi.org/10.3390/pharmacy9020103
Begum MM, Rivu SF, Hasan MMA, Nova TT, Rahman MM, Alim MA, Uddin MS, Islam A, Nurnahar, Tabassum N, et al. Disposal Practices of Unused and Leftover Medicines in the Households of Dhaka Metropolis. Pharmacy. 2021; 9(2):103. https://doi.org/10.3390/pharmacy9020103
Chicago/Turabian StyleBegum, Mst. Marium, Sanzana Fareen Rivu, Md. Mahmud Al Hasan, Tasnova Tasnim Nova, Md. Motiar Rahman, Md. Abdul Alim, Md. Sahab Uddin, Azharul Islam, Nurnahar, Nuzhat Tabassum, and et al. 2021. "Disposal Practices of Unused and Leftover Medicines in the Households of Dhaka Metropolis" Pharmacy 9, no. 2: 103. https://doi.org/10.3390/pharmacy9020103
APA StyleBegum, M. M., Rivu, S. F., Hasan, M. M. A., Nova, T. T., Rahman, M. M., Alim, M. A., Uddin, M. S., Islam, A., Nurnahar, Tabassum, N., Moni, M. M. R., Roselin, R., Das, M., Begum, R., & Rahman, M. S. (2021). Disposal Practices of Unused and Leftover Medicines in the Households of Dhaka Metropolis. Pharmacy, 9(2), 103. https://doi.org/10.3390/pharmacy9020103