
Caregiver Burden among Caregivers of Patients with Mental Illness: A Systematic Review and Meta-Analysis

 , , , , and
, , , , and
Abstract
:1. Introduction
- What is the prevalence of caregiver burden among caregivers of individuals with mental illness?
- Does the prevalence of caregiver burden differ according to study setting, measurements used, and type of disorder?
2. Materials and Methods
2.1. Protocol
2.2. Design
2.3. Literature Search
2.4. Study Selection
2.5. Inclusion Criteria
2.6. Exclusion Criteria
2.7. Data Extraction
2.8. Quality Assessment
2.9. Statistical Analysis
2.10. Subgroup Analyses
2.11. Sensitivity Analysis
3. Results
3.1. Description of Included Studies
3.2. Pooled Prevalence of Caregiver Burden among Caregivers of Patients with Mental Illness
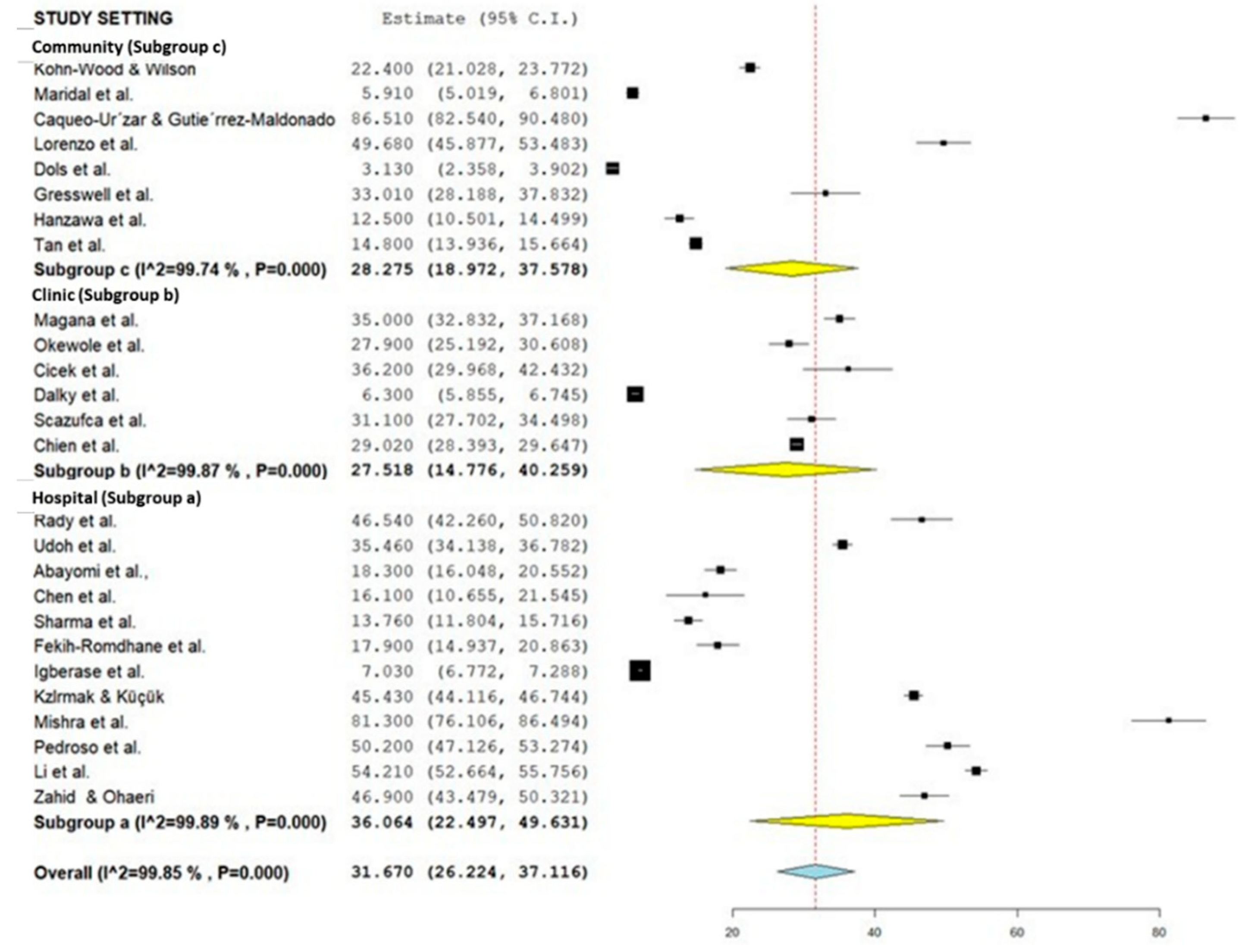
3.3. Subgroup Analysis for the Prevalence of Caregiver Burden among Caregivers of Patients with Mental Illness According to Study Setting, Instruments, and Type of Mental Illness
4. Discussion
5. Implications
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mosley, P.E.; Moodie, R.; Dissanayaka, N. Caregiver Burden in Parkinson Disease: A Critical Review of Recent Literature. J. Geriatr. Psychiatry Neurol. 2017, 30, 235–252. [Google Scholar] [CrossRef] [PubMed]
- Tamizi, Z.; Fallahi-Khoshknab, M.; Dalvandi, A.; Mohammadi-Shahboulaghi, F.; Mohammadi, E.; Bakhshi, E. Caregiving Burden in Family Caregivers of Patients with Schizophrenia: A Qualitative Study. J. Educ. Health Promot. 2020, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Chadda, R.K. Caring for the Family Caregivers of Persons with Mental Illness. Indian J. Psychiatry 2014, 56, 221. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, C.Y.; Lu, H.L.; Tsai, Y.F. Caregiver Burden and Health-Related Quality of Life among Primary Family Caregivers of Individuals with Schizophrenia: A Cross-Sectional Study. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2020, 29, 2745–2757. [Google Scholar] [CrossRef] [PubMed]
- Adelman, R.D.; Tmanova, L.L.; Delgado, D.; Dion, S.; Lachs, M.S. Caregiver Burden: A Clinical Review. JAMA 2014, 311, 1052–1059. [Google Scholar] [CrossRef]
- Alves, L.C.D.S.; Monteiro, D.Q.; Bento, S.R.; Hayashi, V.D.; Pelegrini, L.N.D.C.; Vale, F.A.C. Burnout Syndrome in Informal Caregivers of Older Adults with Dementia: A Systematic Review. Dement. Neuropsychol. 2019, 13, 415–421. [Google Scholar] [CrossRef]
- Cheah, Y.K.; Azahadi, M.; Phang, S.N.; Abd Manaf, N.H. Sociodemographic, Lifestyle, and Health Factors Associated With Depression and Generalized Anxiety Disorder among Malaysian Adults. J. Prim. Care Community Health 2020, 11, 2. [Google Scholar] [CrossRef]
- Walke, S.C.; Chandrasekaran, V.; Mayya, S.S. Caregiver Burden among Caregivers of Mentally Ill Individuals and Their Coping Mechanisms. J. Neurosci. Rural Pract. 2018, 9, 180–185. [Google Scholar] [CrossRef]
- Ahmad, N.A.; Muhd Yusoff, F.; Ratnasingam, S.; Mohamed, F.; Nasir, N.H.; Mohd Sallehuddin, S.; Mahadir Naidu, B.; Ismail, R.; Aris, T. Trends and Factors Associated with Mental Health Problems among Children and Adolescents in Malaysia. Int. J. Cult. Ment. Health 2015, 8, 125–136. [Google Scholar] [CrossRef]
- Azman, A.; Jamir Singh, P.S.; Sulaiman, J. The Mentally Ill and Their Impact on Family Caregivers: A Qualitative Case Study. Int. Soc. Work 2017, 62, 461–471. [Google Scholar] [CrossRef]
- Lian, C.W.; Shui, I.V.J.; Hazmi, H. Mental Health Status and Its Associated Factors among Caregivers of Psychiatric Patients in Kuching, Sarawak. Malays. Fam. Physician Off. J. Acad. Fam. Physicians Malays. 2019, 14, 18. [Google Scholar]
- Gharavi, Y.; Stringer, B.; Hoogendoorn, A.; Boogaarts, J.; van Raaij, B.; van Meijel, B. Evaluation of an Interaction-Skills Training for Reducing the Burden of Family Caregivers of Patients with Severe Mental Illness: A Pre-Posttest Design. BMC Psychiatry 2018, 18, 84. [Google Scholar] [CrossRef] [PubMed]
- Akbari, M.; Alavi, M.; Irajpour, A.; Maghsoudi, J. Challenges of Family Caregivers of Patients with Mental Disorders in Iran: A Narrative Review. Iran. J. Nurs. Midwifery Res. 2018, 23, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Stanley, S.; Balakrishnan, S.; Ilangovan, S. Psychological Distress, Perceived Burden and Quality of Life in Caregivers of Persons with Schizophrenia. J. Ment. Health Abingdon Engl. 2017, 26, 134–141. [Google Scholar] [CrossRef]
- Neong, S.C.; Rashid, A. Quality of Life of Caregivers of Patients with Psychiatric Illness in Penang. J. Clin. Psychiatry Cogn. Psychol. 2018, 2, 12–13. [Google Scholar] [CrossRef]
- Siddiqui, S.; Khalid, J. Determining the Caregivers’ Burden in Caregivers of Patients with Mental Illness. Pak. J. Med. Sci. 2019, 35, 1329. [Google Scholar] [CrossRef]
- Maeng, S.-R.; Kim, W.-H.; Kim, J.-H.; Bae, J.-N.; Lee, J.-S.; Kim, C.-E. Factors Affecting Quality of Life and Family Burden among the Families of Patients with Schizophrenia. Korean J. Schizophr. Res. 2016, 19, 78. [Google Scholar] [CrossRef]
- Udoh, E.E.; Omorere, D.E.; Sunday, O.; Osasu, O.S.; Amoo, B.A. Psychological Distress and Burden of Care among Family Caregivers of Patients with Mental Illness in a Neuropsychiatric Outpatient Clinic in Nigeria. PLoS ONE 2021, 16, e0250309. [Google Scholar] [CrossRef]
- Aledeh, M.; Adam, P.H. Caring for Dementia Caregivers in Times of the COVID-19 Crisis: A Systematic Review. Am. J. Nurs. Res. 2020, 8, 552–561. [Google Scholar] [CrossRef]
- Collins, R.N.; Kishita, N. Prevalence of Depression and Burden among Informal Care-Givers of People with Dementia: A Meta-Analysis. Ageing Soc. 2020, 40, 2355–2392. [Google Scholar] [CrossRef]
- Leng, M.; Zhao, Y.; Xiao, H.; Li, C.; Wang, Z. Internet-Based Supportive Interventions for Family Caregivers of People with Dementia: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2020, 22, e19468. [Google Scholar] [CrossRef] [PubMed]
- Van der Lee, J.; Bakker, T.J.E.M.; Duivenvoorden, H.J.; Dröes, R.M. Multivariate Models of Subjective Caregiver Burden in Dementia: A Systematic Review. Ageing Res. Rev. 2014, 15, 76–93. [Google Scholar] [CrossRef] [PubMed]
- Xiong, C.; Biscardi, M.; Nalder, E.; Colantonio, A. Sex and Gender Differences in Caregiving Burden Experienced by Family Caregivers of Persons with Dementia: A Systematic Review Protocol. BMJ Open 2018, 8, e022779. [Google Scholar] [CrossRef] [PubMed]
- Domingues, N.S.; Verreault, P.; Hudon, C. Reducing Burden for Caregivers of Older Adults With Mild Cognitive Impairment: A Systematic Review. Am. J. Alzheimers Dis. Other Dement. 2018, 33, 401–414. [Google Scholar] [CrossRef] [PubMed]
- Wing, W.; Lam, Y.; Nielsen, K.; Sprigg, C.A.; Kelly, C.M. The Demands and Resources of Working Informal Caregivers of Older People: A Systematic Review. Work Stress 2022, 36, 105–127. [Google Scholar] [CrossRef]
- Namasivayam-MacDonald, A.M.; Shune, S.E. The Burden of Dysphagia on Family Caregivers of the Elderly: A Systematic Review. Geriatrics 2018, 3, 30. [Google Scholar] [CrossRef]
- Geng, H.M.; Chuang, D.M.; Yang, F.; Yang, Y.; Liu, W.M.; Liu, L.H.; Tian, H.M. Prevalence and Determinants of Depression in Caregivers of Cancer Patients: A Systematic Review and Meta-Analysis. Medicine 2018, 97, 2–4. [Google Scholar] [CrossRef]
- Jadalla, A.; Page, M.; Ginex, P.A.; Coleman, M.; Vrabel, M.; Bevans, M. Family Caregiver Strain and Burden: A Systematic Review of Evidence-Based Interventions When Caring for Patients with Cancer. Clin. J. Oncol. Nurs. 2020, 24, 31–50. [Google Scholar] [CrossRef]
- Del-Pino-Casado, R.; Priego-Cubero, E.; López-Martínez, C.; Orgeta, V. Subjective Caregiver Burden and Anxiety in Informal Caregivers: A Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0247143. [Google Scholar] [CrossRef]
- Del-Pino-Casado, R.; Cardosa, M.R.; López-Martínez, C.; Orgeta, V. The Association between Subjective Caregiver Burden and Depressive Symptoms in Carers of Older Relatives: A Systematic Review and Meta-Analysis. PLoS ONE 2019, 14, e0217648. [Google Scholar] [CrossRef]
- Park, S.; Park, M. Effects of Family Support Programs for Caregivers of People with Dementia—Caregiving Burden, Depression, and Stress: Systematic Review and Meta-Analysis. J. Korean Acad. Nurs. 2015, 45, 627–640. [Google Scholar] [CrossRef]
- Li, Y.; Li, J.; Zhang, Y.; Ding, Y.; Hu, X. The Effectiveness of E-Health Interventions on Caregiver Burden, Depression, and Quality of Life in Informal Caregivers of Patients with Cancer: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Nurs. Stud. 2022, 127, 104179. [Google Scholar] [CrossRef]
- Williams, F.; Moghaddam, N.; Ramsden, S.; de Boos, D. Interventions for Reducing Levels of Burden amongst Informal Carers of Persons with Dementia in the Community. A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Aging Ment. Health 2019, 23, 1629–1642. [Google Scholar] [CrossRef] [PubMed]
- Psychiatry. Org—DSM. Available online: https://www.psychiatry.org/psychiatrists/practice/dsm (accessed on 20 September 2022).
- Vandenbrouckel, J.P.; von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. PLoS Med. 2007, 4, 1628–1655. [Google Scholar]
- Samara, M.T.; Spineli, L.M.; Furukawa, T.A.; Engel, R.R.; Davis, J.M.; Salanti, G.; Leucht, S. Imputation of Response Rates from Means and Standard Deviations in Schizophrenia. Schizophr. Res. 2013, 151, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the Mean and Variance from the Median, Range, and the Size of a Sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- Wallace, B.C.; Dahabreh, I.J.; Trikalinos, T.A.; Lau, J.; Trow, P.; Schmid, C.H. Closing the Gap between Methodologists and End-Users: R as a Computational Back-End. J. Stat. Softw. 2012, 49, 1–15. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Okewole, A.O.; Dada, M.U.; Bello-Mojeed, M.; Ogun, O.C. A Comparison of Clinician and Caregiver Assessment of Functioning in Patients Attending a Child and Adolescent Mental Health Clinic in Nigeria. SAJCH S. Afr. J. Child Health 2016, 10, 8–11. [Google Scholar] [CrossRef]
- Abayomi, O.; Akinhanmi, A.O.; Adelufosi, A.O. Psychiatric Morbidity and Subjective Burden Among Carers of Outpatients of a Psychogeriatric Clinic in Southwestern Nigeria. J. Cross Cult. Gerontol. 2015, 30, 439–450. [Google Scholar] [CrossRef]
- Dada, M.U.; Okewole, N.O.; Ogun, O.C.; Bello-Mojeed, M.A. Factors Associated with Caregiver Burden in a Child and Adolescent Psychiatric Facility in Lagos, Nigeria: A Descriptive Cross Sectional Study. BMC Pediatr. 2011, 11, 110. [Google Scholar] [CrossRef] [PubMed]
- Inogbo, C.F.; Olotu, S.O.; James, B.O.; Nna, E.O. Burden of Care amongst Caregivers Who Are First Degree Relatives of Patients with Schizophrenia. Pan Afr. Med. J. 2017, 28, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Igberase, O.O.; Morakinyo, O.; Lawani, A.O.; James, B.O.; Omoaregba, J.O. Burden of Care among Relatives of Patients with Schizophrenia in Midwestern Nigeria. Int. J. Soc. Psychiatry 2012, 58, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Penteado, C.T.; Loureiro, J.C.; Pais, M.V.; Carvalho, C.L.; Sant’Ana, L.F.G.; Valiengo, L.C.L.; Stella, F.; Forlenza, O.V. Mental Health Status of Psychogeriatric Patients During the 2019 New Coronavirus Disease (COVID-19) Pandemic and Effects on Caregiver Burden. Front. Psychiatry 2020, 11, 578672. [Google Scholar] [CrossRef]
- Andrade, J.J.d.C.; Silva, A.C.O.; Frazão, I.d.S.; Perrelli, J.G.A.; Silva, T.T.d.M.; Cavalcanti, A.M.T.S. Family Functionality and Burden of Family Caregivers of Users with Mental Disorders. Rev. Bras. Enferm. 2021, 74, e20201061. [Google Scholar] [CrossRef]
- Dos Santos, C.A.; Jardim, V.M.d.; Tomasi, E.; Kantorski, L.P.; de Oliveira, M.M.; Coimbra, V.C.C. Minor Psychiatric Disorders among Family Caregivers of Users of Psychosocial Care Centers: Prevalence and Associated Factors. Cienc. E Saude Coletiva 2020, 25, 461–472. [Google Scholar] [CrossRef]
- Pedroso, T.G.; Araújo, A.d.S.; Santos, M.T.S.; Galera, S.A.F.; Cardoso, L. Caregiver Burden and Stress in Psychiatric Hospital Admission. Rev. Bras. Enferm. 2019, 72, 1699–1706. [Google Scholar] [CrossRef]
- Scazufca, M.; Menezes, P.R.; Almeida, O.P. Caregiver Burden in an Elderly Population with Depression in São Paulo, Brazil. Soc. Psychiatry Psychiatr. Epidemiol. 2002, 37, 416–422. [Google Scholar] [CrossRef]
- Maridal, H.K.; Bjørgaas, H.M.; Hagen, K.; Jonsbu, E.; Mahat, P.; Malakar, S.; Dørheim, S. Psychological Distress among Caregivers of Children with Neurodevelopmental Disorders in Nepal. Int. J. Environ. Res. Public. Health 2021, 18, 2460. [Google Scholar] [CrossRef]
- Sharma, R.; Sharma, S.C.; Pradhan, S.N. Assessing Caregiver Burden in Caregivers of Patients with Schizophrenia and Bipolar Affective Disorder in Kathmandu Medical College. J. Nepal Health Res. Counc. 2018, 15, 258–263. [Google Scholar] [CrossRef]
- Mishra, S.K.; Pandey, A.K.; Adhikari, B.R.; Nepal, S. Caregiver Burden and Coping Strategies in Schizophrenia: A Hospital Based Study. J. Psychiatr. Assoc. Nepal 2017, 5, 26–31. [Google Scholar] [CrossRef]
- Baykal, S.; Karakurt, M.N.; Çakır, M.; Karabekiroğlu, K. An Examination of the Relations Between Symptom Distributions in Children Diagnosed with Autism and Caregiver Burden, Anxiety and Depression Levels. Community Ment. Health J. 2019, 55, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Cicek, E.; Cicek, I.E.; Kayhan, F.; Uguz, F.; Kaya, N. Quality of Life, Family Burden and Associated Factors in Relatives with Obsessive-Compulsive Disorder. Gen. Hosp. Psychiatry 2013, 35, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Kizilirmak, B.; Küçük, L. Care Burden Level and Mental Health Condition of the Families of Individuals with Mental Disorders. Arch. Psychiatr. Nurs. 2016, 30, 47–54. [Google Scholar] [CrossRef]
- Chien, W.T.; Chan, S.W.C.; Morrissey, J. The Perceived Burden among Chinese Family Caregivers of People with Schizophrenia. J. Clin. Nurs. 2007, 16, 1151–1161. [Google Scholar] [CrossRef]
- Wong, D.F.K.; Lam, A.Y.K.; Chan, S.K.; Chan, S.F. Quality of Life of Caregivers with Relatives Suffering from Mental Illness in Hong Kong: Roles of Caregiver Characteristics, Caregiving Burdens, and Satisfaction with Psychiatric Services. Health Qual. Life Outcomes 2012, 10, 15. [Google Scholar] [CrossRef]
- Kohn-Wood, L.P.; Wilson, M.N. The Context of Caretaking in Rural Areas: Family Factors Influencing the Level of Functioning of Seriously Mentally Ill Patients Living at Home. Am. J. Community Psychol. 2005, 36, 1–13. [Google Scholar] [CrossRef]
- Magaña, S.M.; Ramírez García, J.I.; Hernández, M.G.; Cortez, R. Psychological Distress among Latino Family Caregivers of Adults with Schizophrenia: The Roles of Burden and Stigma. Psychiatr. Serv. 2007, 58, 378–384. [Google Scholar] [CrossRef]
- Chen, H.M.; Hou, S.Y.; Yeh, Y.C.; Chang, C.Y.; Yen, J.Y.; Ko, C.H.; Yen, C.F.; Chen, C.S. Frontal Function, Disability and Caregiver Burden in Elderly Patients with Major Depressive Disorder. Kaohsiung J. Med. Sci. 2010, 26, 548–554. [Google Scholar] [CrossRef]
- Fan, C.C.; Chen, Y.Y. Factors Associated with Care Burden and Quality of Life among Caregivers of the Mentally Ill in Chinese Society. Int. J. Soc. Psychiatry 2011, 57, 195–206. [Google Scholar] [CrossRef]
- Fekih-Romdhane, F.; Ben Ali, S.; Ghazouani, N.; Tira, S.; Cheour, M. Burden in Tunisian Family Caregivers of Older Patients with Schizophrenia Spectrum and Bipolar Disorders; Associations with Depression, Anxiety, Stress, and Quality of Life. Clin. Gerontol. 2020, 43, 545–557. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Lambert, C.E.; Lambert, V.A. Predictors of Family Caregivers’ Burden and Quality of Life When Providing Care for a Family Member with Schizophrenia in the People’s Republic of China. Nurs. Health Sci. 2007, 9, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Caqueo-Urízar, A.; Gutiérrez-Maldonado, J. Burden of Care in Families of Patients with Schizophrenia. Qual. Life Res. 2006, 15, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Rady, A.; Mouloukheya, T.; Gamal, E. Posttraumatic Stress Symptoms, Quality of Life, and Stress Burden in Caregivers of Patients With Severe Mental Illness: An Underestimated Health Concern. Front. Psychiatry 2021, 12, 623499. [Google Scholar] [CrossRef] [PubMed]
- Koutra, K.; Simos, P.; Triliva, S.; Lionis, C.; Vgontzas, A.N. Linking Family Cohesion and Flexibility with Expressed Emotion, Family Burden and Psychological Distress in Caregivers of Patients with Psychosis: A Path Analytic Model. Psychiatry Res. 2016, 240, 66–75. [Google Scholar] [CrossRef]
- Grover, S.; Chakrabarti, S.; Ghormode, D.; Dutt, A. A Comparative Study of Caregivers Perceptions of Health-Care Needs and Burden of Patients with Bipolar Affective Disorder and Schizophrenia. Nord. J. Psychiatry 2015, 69, 629–636. [Google Scholar] [CrossRef]
- Gresswell, I.; Lally, L.; Adamis, D.; McCarthy, G.M. Widening the Net: Exploring Social Determinants of Burden of Informal Carers. Ir. J. Psychol. Med. 2018, 35, 43–51. [Google Scholar] [CrossRef]
- Di Lorenzo, R.; Girone, A.; Panzera, N.; Fiore, G.; Pinelli, M.; Venturi, G.; Magarini, F.; Ferri, P. Empathy and Perceived Burden in Caregivers of Patients with Schizophrenia Spectrum Disorders. BMC Health Serv. Res. 2021, 21, 250. [Google Scholar] [CrossRef]
- Hanzawa, S.; Tanaka, G.; Inadomi, H.; Urata, M.; Ohta, Y. Burden and Coping Strategies in Mothers of Patients with Schizophrenia in Japan. Psychiatry Clin. Neurosci. 2008, 62, 256–263. [Google Scholar] [CrossRef]
- Dalky, H.F.; Qandil, A.M.; Natour, A.S.; Janet, M.C. Quality of Life, Stigma and Burden Perception Among Family Caregivers and Patients with Psychiatric Illnesses in Jordan. Community Ment. Health J. 2017, 53, 266–274. [Google Scholar] [CrossRef]
- Zahid, M.A.; Ohaeri, J.U. Relationship of Family Caregiver Burden with Quality of Care and Psychopathology in a Sample of Arab Subjects with Schizophrenia. BMC Psychiatry 2010, 10, 71. [Google Scholar] [CrossRef]
- Hadryś, T.; Adamowski, T.; Kiejna, A. Mental Disorder in Polish Families: Is Diagnosis a Predictor of Caregiver’s Burden? Soc. Psychiatry Psychiatr. Epidemiol. 2011, 46, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves-Pereira, M.; Xavier, M.; van Wijngaarden, B.; Papoila, A.L.; Schene, A.H.; Caldas-De-Almeida, J.M. Impact of Psychosis on Portuguese Caregivers: A Cross-Cultural Exploration of Burden, Distress, Positive Aspects and Clinical-Functional Correlates. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.C.; Yeoh, A.L.; Choo, I.B.; Huang, A.P.; Ong, S.H.; Ismail, H.; Ang, P.P.; Chan, Y.H. Burden and Coping Strategies Experienced by Caregivers of Persons with Schizophrenia in the Community. J. Clin. Nurs. 2012, 21, 2410–2418. [Google Scholar] [CrossRef]
- Reinares, M.; Vieta, E.; Colom, F.; Martínez-Arán, A.; Torrent, C.; Comes, M.; Goikolea, J.M.; Benabarre, A.; Daban, C.; Sánchez-Moreno, J. What Really Matters to Bipolar Patients’ Caregivers: Sources of Family Burden. J. Affect. Disord. 2006, 94, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Dols, A.; Thesing, C.; Wouters, M.; Theunissen, J.; Sonnenberg, C.; Comijs, H.; Stek, M.L. Burden on Caregivers of Older Patients with Bipolar Disorder. Aging Ment. Health 2018, 22, 686–691. [Google Scholar] [CrossRef]
- Zarit, S.H.; Reever, K.E.; Bach-Peterson, J. Relatives of the Impaired Elderly: Correlates of Feelings of Burden. Gerontologist 1980, 20, 649–655. [Google Scholar] [CrossRef]
- Pai, S.; Kapur, R.L. The Burden on the Family of a Psychiatric Patient: Development of an Interview Schedule. Br. J. Psychiatry J. Ment. Sci. 1981, 138, 332–334. [Google Scholar] [CrossRef]
- Van Wijngaarden, B.; Schene, A.H.; Koeter, M.; Vázquez-Barquero, J.L.; Knudsen, H.C.; Lasalvia, A.; McCrone, P. Caregiving in Schizophrenia: Development, Internal Consistency and Reliability of the Involvement Evaluation Questionnaire—European Version: EPSILON Study 4. Br. J. Psychiatry 2000, 177, s21–s27. [Google Scholar] [CrossRef]
- Robinson, B.C. Validation of a Caregiver Strain Index. J. Gerontol. 1983, 38, 344–348. [Google Scholar] [CrossRef]
- Reinhard, S.C.; Gubman, G.D.; Horwitz, A.V.; Minsky, S. Burden Assessment Scale for Families of the Seriously Mentally Ill. Eval. Program Plan. 1994, 17, 261–269. [Google Scholar] [CrossRef]
- Novak, M.; Guest, C. Application of a Multidimensional Caregiver Burden Inventory. Gerontologist 1989, 29, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Levene, J.E.; Lancee, W.J.; Seeman, M.V. The Perceived Family Burden Scale: Measurement and Validation. Schizophr. Res. 1996, 22, 151–157. [Google Scholar] [CrossRef]
- Morosini, P.I.; Roncone, R.I.; Veltro, F.R.; Palomba, U.; Casacchia, M.A. Routine Assessment Tool in Psychiatry: A Case of Questionnaire of Family Attitudes and Burden. Ital. J. Psychiatry Behav. Sci. 1660, 1, 95–102. [Google Scholar]
- Roberts, C.S.; Feetham, S.L. Assessing Family Functioning across Three Areas of Relationships. Nurs. Res. 1982, 31, 231–235. [Google Scholar] [CrossRef]
- Wong, D.F.K. Stress Factors and Mental Health of Carers with Relatives Suffering from Schizophrenia in Hong Kong: Implications for Culturally Sensitive Practices. Br. J. Soc. Work 2000, 30, 365–382. [Google Scholar] [CrossRef]
- Pot, A.M.; van Dyck, R.; Deeg, D.J.H. Perceived Stress Caused by Informal Caregiving. Construction of a Scale. Tijdschr. Gerontol. Geriatr. 1995, 26, 214–219. [Google Scholar]
- Platt, S.; Weyman, A.; Hirsch, S.; Hewett, S. The Social Behaviour Assessment Schedule (SBAS): Rationale, Contents, Scoring and Reliability of a New Interview Schedule. Soc. Psychiatry 1980, 15, 43–55. [Google Scholar] [CrossRef]
- Thara, R.; Padmavati, R.; Kumar, S.; Srinivasan, L. Burden Assessment Schedule. Indian J. Psychiatry 2022, 40, 21. [Google Scholar]
- Ohaeri, J.U.; Campbell, O.B.; Ilesanmi, A.O.; Omigbodun, A.O. The Psychosocial Burden of Caring for Some Nigerian Women with Breast Cancer and Cervical Cancer. Soc. Sci. Med. 1999, 49, 1541–1549. [Google Scholar] [CrossRef]
- Montgomery, R.J.; Montgomery, R.J.V. Using and Interpreting the Montgomery Borgatta Caregiving Burden Scale. Available online: https://www.researchgate.net/publication/265679222_Using_and_Interpreting_the_Montgomery_Borgatta_Caregiving_Burden_Scale (accessed on 22 September 2022).
- Rezaei, H.; Niksima, S.H.; Ghanei Gheshlagh, R. Burden of Care in Caregivers of Iranian Patients with Chronic Disorders: A Systematic Review and Meta-Analysis. Health Qual. Life Outcomes 2020, 18, 261. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-González, A.M.; Rodríguez-Míguez, E. A Meta-Analysis of the Association between Caregiver Burden and the Dependent’s Illness. J. Women Aging 2019, 32, 220–235. [Google Scholar] [CrossRef] [PubMed]
- Tanna, K.J. Evaluation of Burden Felt by Caregivers of Patients with Schizophrenia and Bipolar Disorder. Ind. Psychiatry J. 2021, 30, 299. [Google Scholar] [CrossRef] [PubMed]
- Cleary, M.; West, S.; Hunt, G.E.; McLean, L.; Kornhaber, R. A Qualitative Systematic Review of Caregivers’ Experiences of Caring for Family Diagnosed with Schizophrenia. Issues Ment. Health Nurs. 2020, 41, 667–683. [Google Scholar] [CrossRef] [PubMed]
- Kate, N.; Grover, S.; Kulhara, P.; Nehra, R. Relationship of Caregiver Burden with Coping Strategies, Social Support, Psychological Morbidity, and Quality of Life in the Caregivers of Schizophrenia. Asian J. Psychiatry 2013, 6, 380–388. [Google Scholar] [CrossRef]
- Van Wijngaarden, B.; Koeter, M.; Knapp, M.; Tansella, M.; Thornicroft, G.; Vázquez-Barquero, J.L.; Schene, A. Caring for People with Depression or with Schizophrenia: Are the Consequences Different? Psychiatry Res. 2009, 169, 62–69. [Google Scholar] [CrossRef]
- Wood, L.; Birtel, M.; Alsawy, S.; Pyle, M.; Morrison, A. Public Perceptions of Stigma towards People with Schizophrenia, Depression, and Anxiety. Psychiatry Res. 2014, 220, 604–608. [Google Scholar] [CrossRef]
- Pescosolido, B.A.; Halpern-Manners, A.; Luo, L.; Perry, B. Trends in Public Stigma of Mental Illness in the US, 1996-2018. JAMA Netw. Open 2021, 4, e2140202. [Google Scholar] [CrossRef]
- Silva, B.; Golay, P.; Morandi, S. Factors Associated with Involuntary Hospitalisation for Psychiatric Patients in Switzerland: A Retrospective Study. BMC Psychiatry 2018, 18, 401. [Google Scholar] [CrossRef]
- Park, J.M.; Kim, M.J. Epidemiologic Characteristics of Hospitalised Patients after Suicidal Acts from 2005 to 2016 in Korea: Analysis of the Korean National Hospital Discharge Survey. J. Affect. Disord. 2020, 275, 238–246. [Google Scholar] [CrossRef]
- Donnelly, N.A.; Hickey, A.; Burns, A.; Murphy, P.; Doyle, F. Systematic Review and Meta-Analysis of the Impact of Carer Stress on Subsequent Institutionalisation of Community-Dwelling Older People. PLoS ONE 2015, 10, e0128213. [Google Scholar] [CrossRef] [PubMed]
- McManus, B.M.; Carle, A.; Acevedo-Garcia, D.; Ganz, M.; Hauser-Cram, P.; McCormick, M. Modeling the Social Determinants of Caregiver Burden among Families of Children with Developmental Disabilities. Am. J. Intellect. Dev. Disabil. 2011, 116, 246–260. [Google Scholar] [CrossRef] [PubMed]
- Schulze, B.; Rössler, W. Caregiver Burden in Mental Illness: Review of Measurement, Findings and Interventions in 2004–2005. Curr. Opin. Psychiatry 2005, 18, 684–691. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (1) | burden* OR caregiver burden* OR burnout OR exhaustion OR strain OR overload* OR frustrate* OR stress |
| (2) | caregiver* OR informal caregiver OR family caregiver OR carer* |
| (3) | mental* OR mental illness OR mental disorder OR mental issues OR schizophrenia OR psychiatric disorder OR psych* problem OR mental health OR bipolar disorder OR substance abuse OR psychiatric illness OR depression OR anxiety OR psychotic disorder OR obsessive-compulsive disorder OR behaviour disorder OR behavioural disorder |
| Variables | No. of Studies | Prevalence, % | 95% CI | I2, % | p-Value | |
|---|---|---|---|---|---|---|
| Study setting | Community (Subgroup c) | 8 | 28.28 | 18.97–37.58 | 99.74 | <0.001 |
| Clinic (Subgroup b) | 6 | 27.52 | 14.78–40.26 | 99.87 | <0.001 | |
| Hospital (Subgroup a) | 12 | 36.06 | 22.50–49.63 | 99.89 | <0.001 | |
| Subtotal | 26 | 31.67 | 26.22–37.12 | 99.85 | <0.001 | |
| Instruments | The Zarit Burden Interview (Subgroup 0) | 13 | 36.90 | 28.17–45.62 | 99.26 | <0.001 |
| Others (Subgroup 1) | 13 | 26.47 | 19.55–33.40 | 99.90 | <0.001 | |
| Subtotal | 26 | 31.67 | 26.22–37.12 | 99.85 | <0.001 | |
| Disorders | With psychosis (Subgroup 1) | 14 | 35.88 | 27.03–44.72 | 99.88 | <0.001 |
| Without psychosis (Subgroup 0) | 12 | 26.82 | 17.98–35.67 | 99.82 | <0.001 | |
| Subtotal | 26 | 31.67 | 26.22–37.12 | 99.85 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cham, C.Q.; Ibrahim, N.; Siau, C.S.; Kalaman, C.R.; Ho, M.C.; Yahya, A.N.; Visvalingam, U.; Roslan, S.; Abd Rahman, F.N.; Lee, K.W. Caregiver Burden among Caregivers of Patients with Mental Illness: A Systematic Review and Meta-Analysis. Healthcare 2022, 10, 2423. https://doi.org/10.3390/healthcare10122423
Cham CQ, Ibrahim N, Siau CS, Kalaman CR, Ho MC, Yahya AN, Visvalingam U, Roslan S, Abd Rahman FN, Lee KW. Caregiver Burden among Caregivers of Patients with Mental Illness: A Systematic Review and Meta-Analysis. Healthcare. 2022; 10(12):2423. https://doi.org/10.3390/healthcare10122423
Chicago/Turabian StyleCham, Choy Qing, Norhayati Ibrahim, Ching Sin Siau, Clarisse Roswini Kalaman, Meng Chuan Ho, Amira Najiha Yahya, Uma Visvalingam, Samsilah Roslan, Fairuz Nazri Abd Rahman, and Kai Wei Lee. 2022. "Caregiver Burden among Caregivers of Patients with Mental Illness: A Systematic Review and Meta-Analysis" Healthcare 10, no. 12: 2423. https://doi.org/10.3390/healthcare10122423
APA StyleCham, C. Q., Ibrahim, N., Siau, C. S., Kalaman, C. R., Ho, M. C., Yahya, A. N., Visvalingam, U., Roslan, S., Abd Rahman, F. N., & Lee, K. W. (2022). Caregiver Burden among Caregivers of Patients with Mental Illness: A Systematic Review and Meta-Analysis. Healthcare, 10(12), 2423. https://doi.org/10.3390/healthcare10122423