
Comparison of Metabolites and Gut Microbes between Patients with Parkinson’s Disease and Healthy Individuals—A Pilot Clinical Observational Study (STROBE Compliant)

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
Study Design
3. Subjects
3.1. Sample Size Calculation
3.2. Inclusion and Exclusion Criteria for the PD Group
3.3. Inclusion and Exclusion Criteria for the HC Group
4. Variables
4.1. Metabolite Analysis
4.1.1. Blood Collection Method
4.1.2. Metabolite Analysis Method
4.1.3. Metabolite Pattern Analysis
4.2. Gut Microbe Analysis
4.2.1. Meal Adjustment Guide
4.2.2. Stool Collection and Specimen Delivery
4.2.3. Gut Microbe Analysis
5. Statistical Analysis
6. Results
6.1. Subject Characteristics
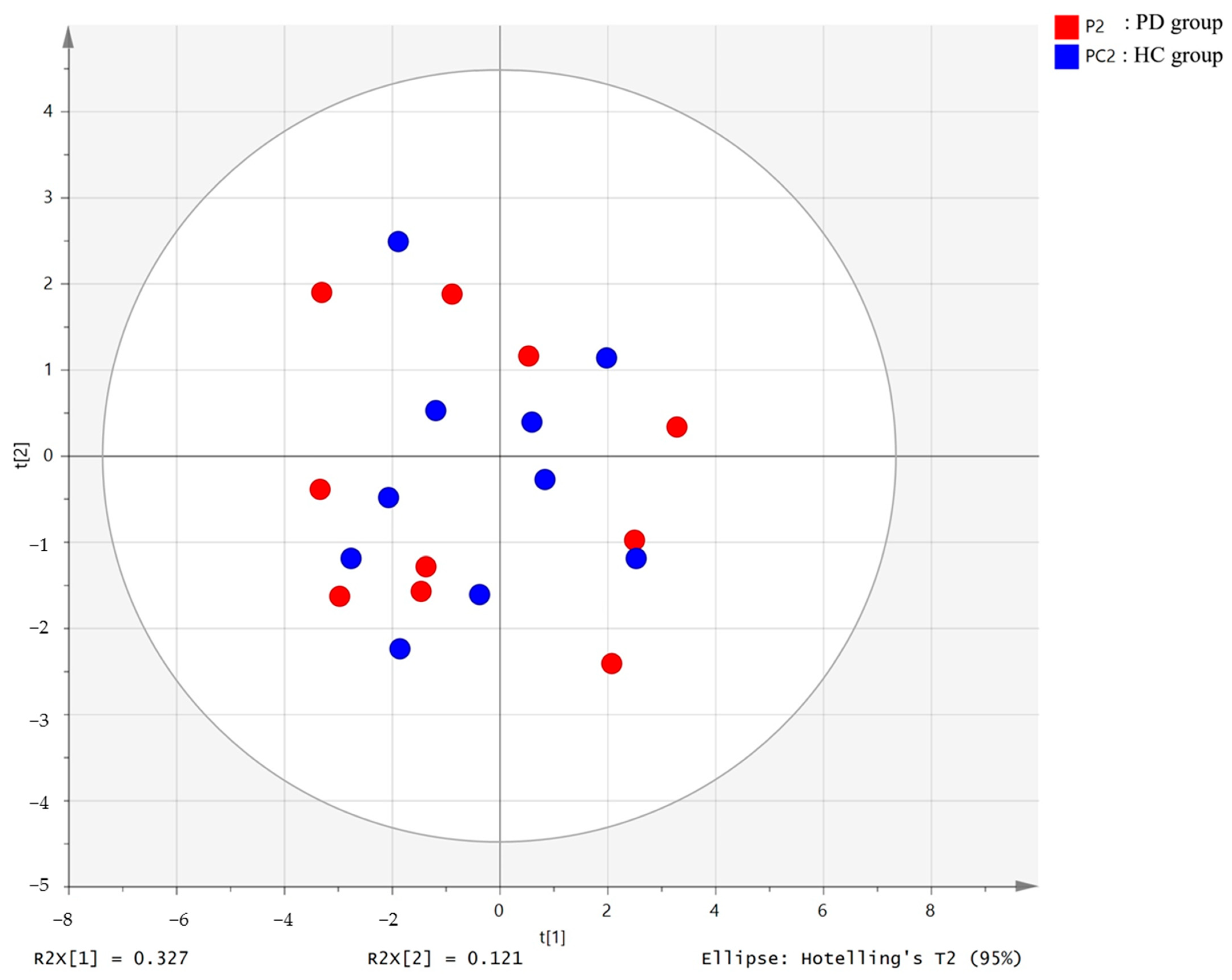
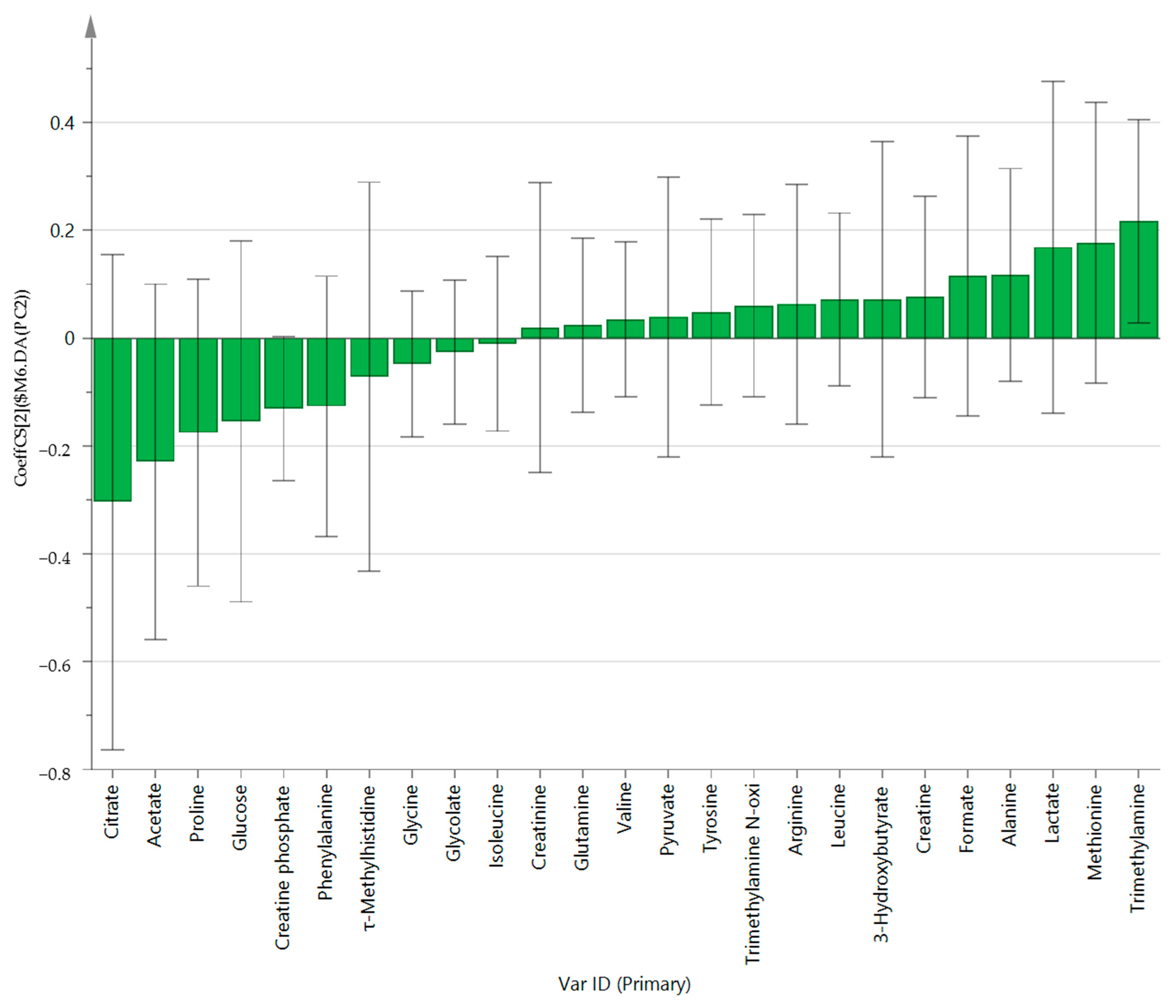
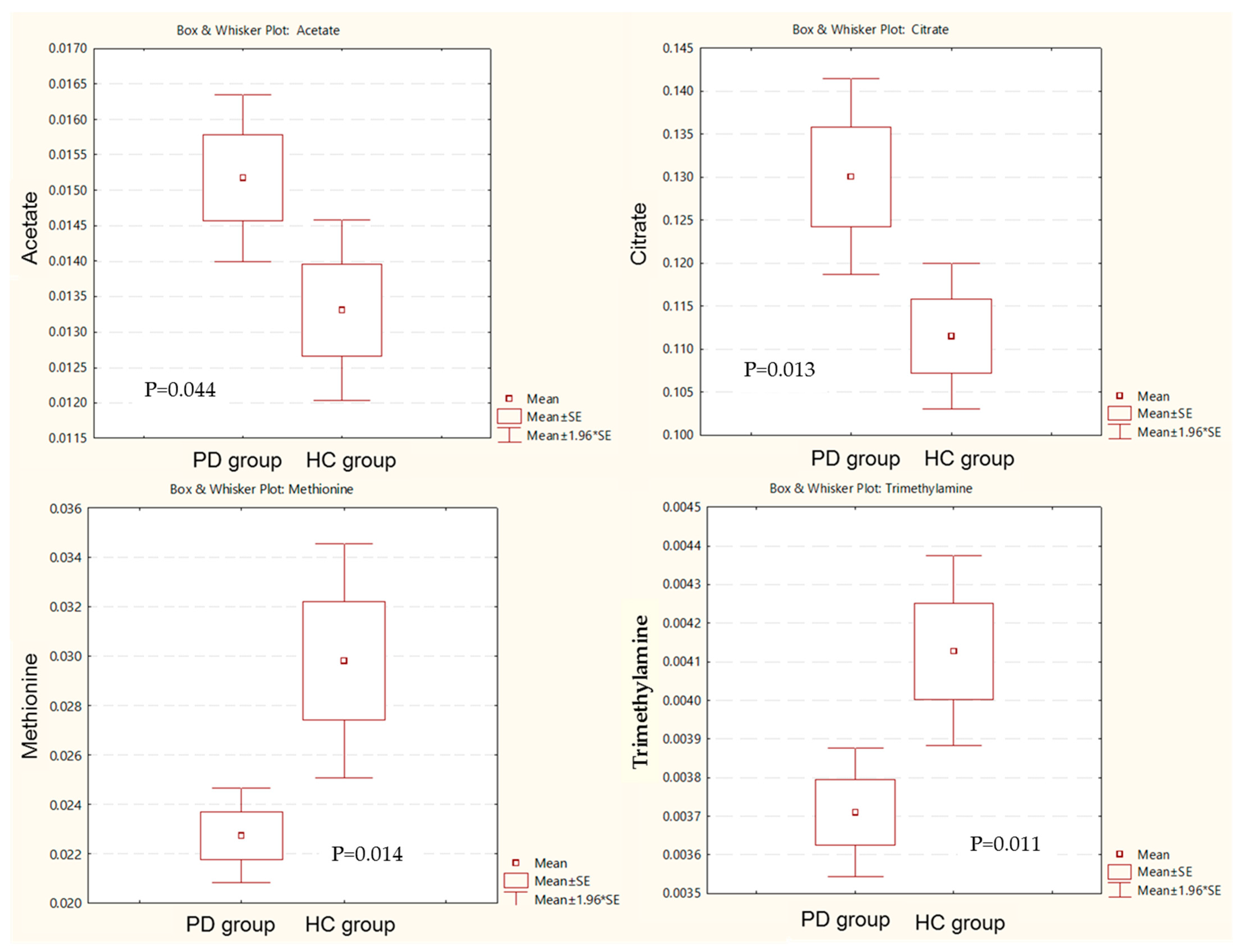
6.2. Metabolite Analysis
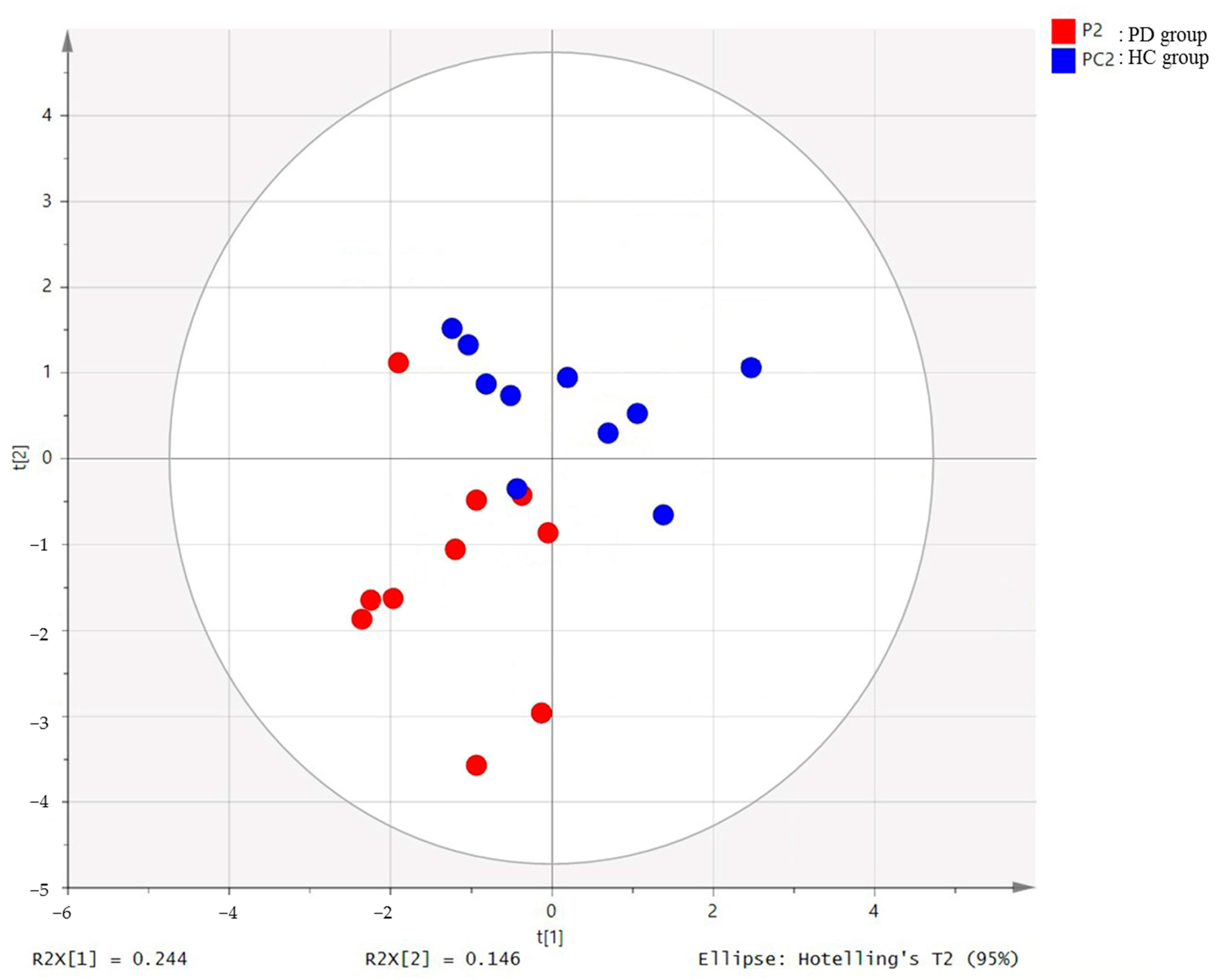
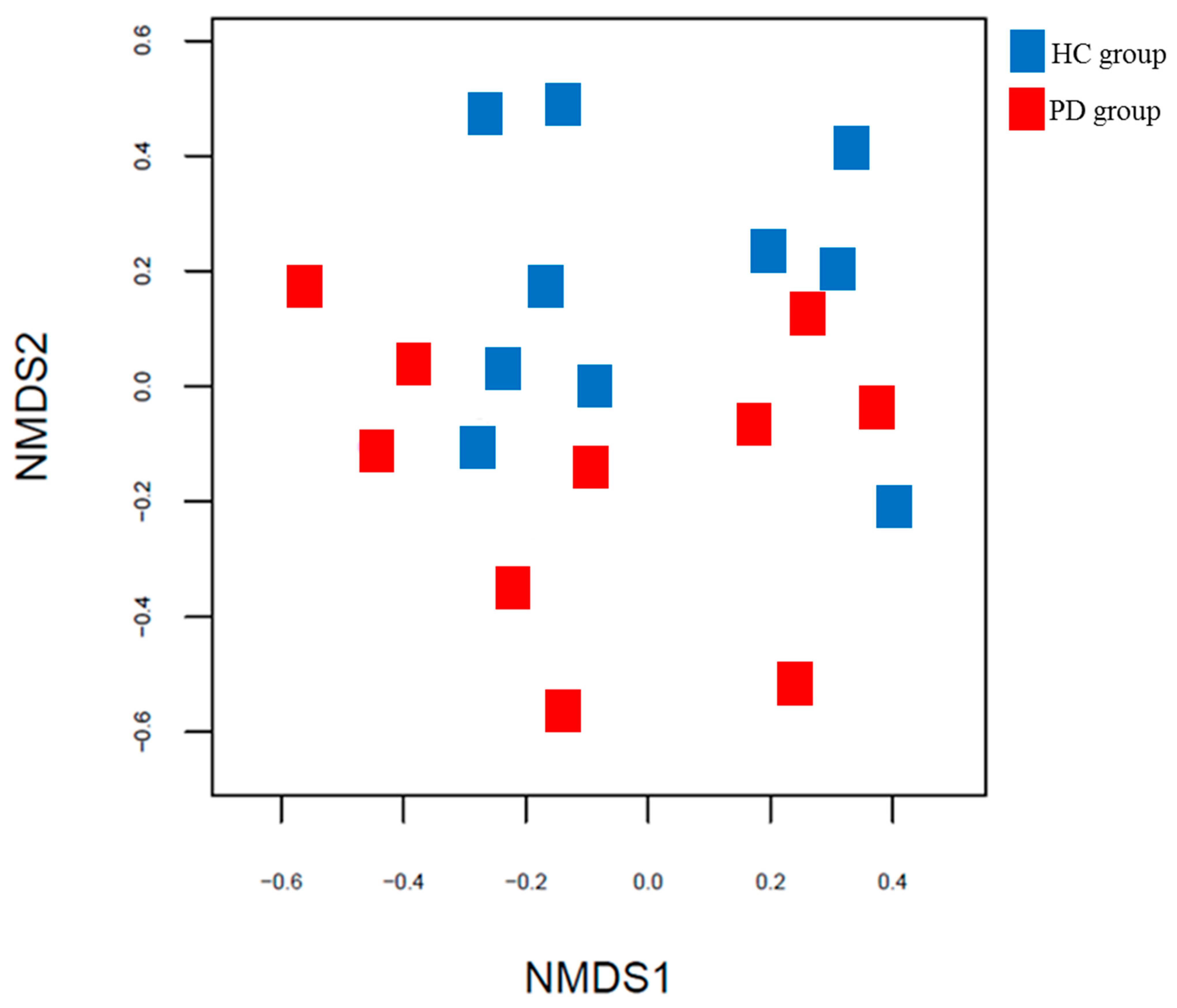
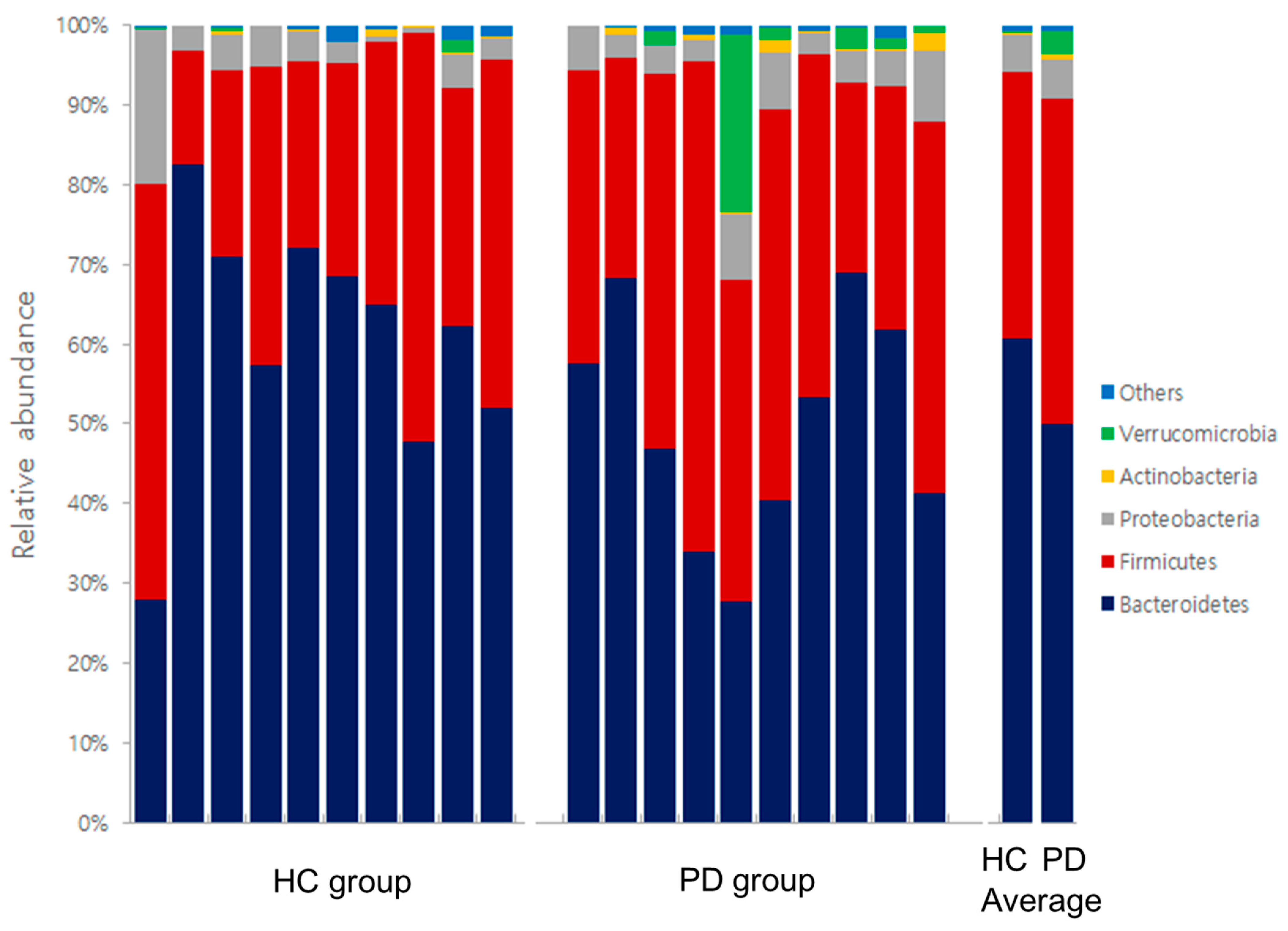
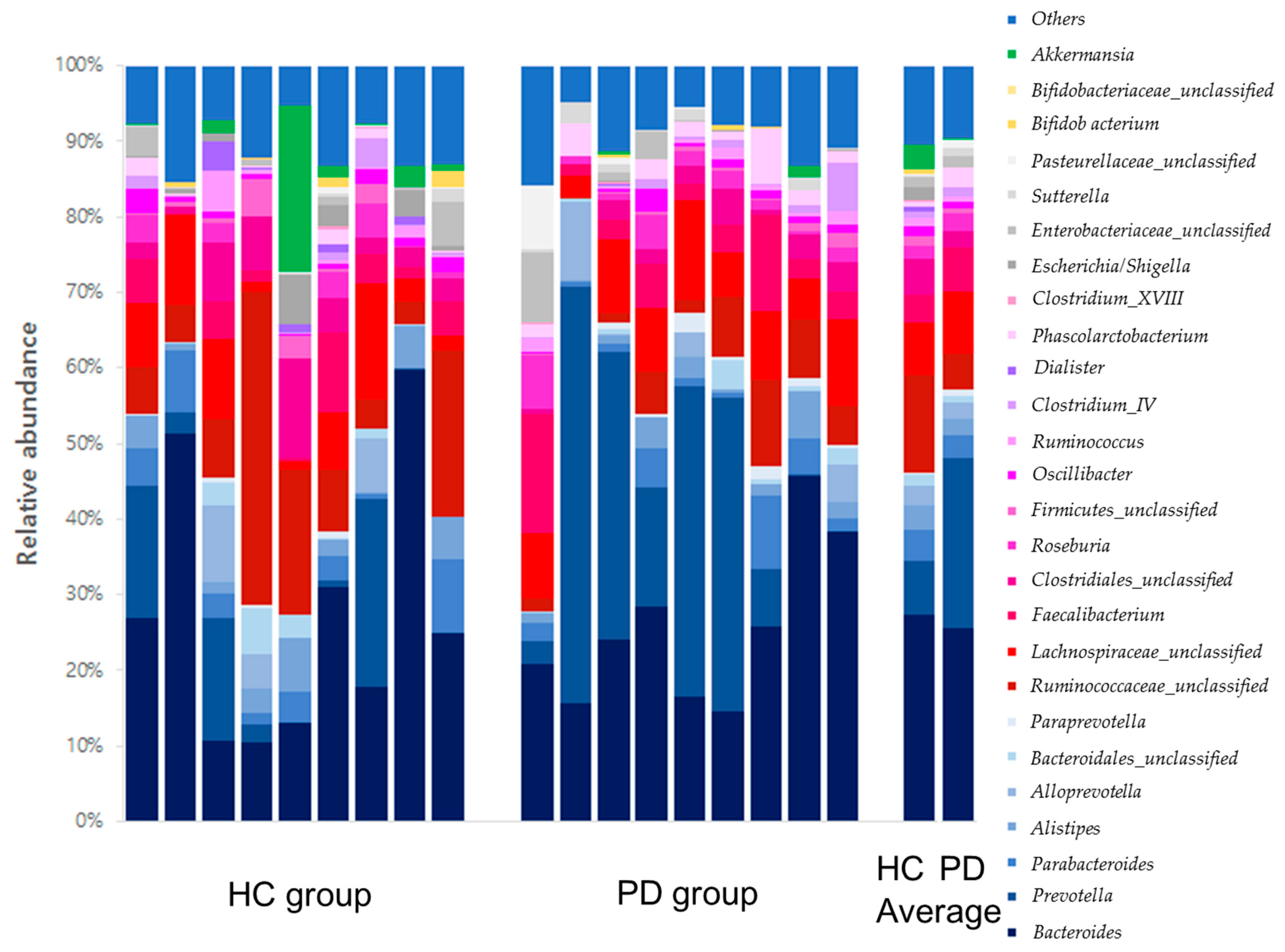
6.3. Gut Microbe Analysis
7. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Pringsheim, T.; Jette, N.; Frolkis, A.; Steeves, T.D. The prevalence of Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2014, 29, 1583–1590. [Google Scholar] [CrossRef] [PubMed]
- Tysnes, O.B.; Storstein, A. Epidemiology of Parkinson’s disease. J. Neural Transm. 2017, 124, 901–905. [Google Scholar] [CrossRef] [PubMed]
- Emrani, S.; McGuirk, A.; Xiao, W. Prognosis and Diagnosis of Parkinson’s Disease Using Multi-Task Learning. In Proceedings of the 23rd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, Halifax, NS, Canada, 13–17 August 2017; Association for Computing Machinery (ACM): New York, NY, USA, 2017; pp. 1457–1466. [Google Scholar]
- Cho, S.Y.; Lee, Y.E.; Doo, K.H.; Lee, J.H.; Jung, W.S.; Moon, S.K.; Park, J.M.; Ko, C.N.; Kim, H.; Rhee, H.Y.; et al. Efficacy of combined treatment with acupuncture and bee venom acupuncture as an adjunctive treatment for Parkinson’s disease. J. Altern. Complement. Med. 2018, 24, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Jameson, J.L. Harrison’s Principles of Internal Medicine; McGraw-Hill Education: New York, NY, USA, 2018. [Google Scholar]
- Seidl, S.E.; Potashkin, J.A. The Promise of Neuroprotective Agents in Parkinson’s Disease. Front. Neurol. 2011, 2, 68. [Google Scholar] [CrossRef] [Green Version]
- Awad, K.; Abushouk, A.I.; Abdelkarim, A.; Mohammed, M.; Negida, A.; Shalash, A. Bee venom for the treatment of Parkinson’s disease: How far is it possible? Biomed. Pharmacother. 2017, 91, 295–302. [Google Scholar] [CrossRef]
- Van Kessel, S.P.; El Aidy, S. Bacterial metabolites mirror altered gut microbiota composition in patients with Parkinson’s disease. J. Parkinsons Dis. 2019, 9, S359–S370. [Google Scholar] [CrossRef] [Green Version]
- Wargo, J.A. Modulating gut microbes. Science 2020, 369, 1302–1303. [Google Scholar] [CrossRef]
- Franzosa, E.A.; Sirota-Madi, A.; Avila-Pacheco, J.; Fornelos, N.; Haiser, H.J.; Reinker, S.; Vatanen, T.; Hall, A.B.; Mallick, H.; McIver, L.J.; et al. Gut microbiome structure and metabolic activity in inflammatory bowel disease. Nat. Microbiol. 2018, 4, 293–305. [Google Scholar] [CrossRef]
- Mertsalmi, T.H.; Pekkonen, E.; Scheperjans, F. Antibiotic Exposure and Risk of Parkinson’s Disease in Finland: A Nationwide Case-Control Study. Mov. Disord. 2019, 35, 431–442. [Google Scholar] [CrossRef]
- Houser, M.; Tansey, M.G. The gut-brain axis: Is intestinal inflammation a silent driver of Parkinson’s disease pathogenesis? NPJ Park. Dis. 2017, 3, 3. [Google Scholar] [CrossRef]
- Sun, M.-F.; Shen, Y.-Q. Dysbiosis of gut microbiota and microbial metabolites in Parkinson’s Disease. Ageing Res. Rev. 2018, 45, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Kieser, M.; Wassmer, G. On the use of the upper confidence limit for the variance from a pilot sample for sample size deter-mination. Biom. J. 1996, 38, 941–949. [Google Scholar] [CrossRef]
- Beynen, A.C.; Buechler, K.F.; Van der Molen, A.J.; Geelen, M.J. The effects of lactate and acetate on fatty acid and cholesterol biosynthesis by isolated rat hepatocytes. Int. J. Biochem. 1982, 14, 165–169. [Google Scholar] [CrossRef]
- Gao, X.; Lin, S.-H.; Ren, F.; Li, J.-T.; Chen, J.-J.; Yao, C.-B.; Yang, H.-B.; Jiang, S.-X.; Yan, G.-Q.; Wang, D.; et al. Acetate functions as an epigenetic metabolite to promote lipid synthesis under hypoxia. Nat. Commun. 2016, 7, 11960. [Google Scholar] [CrossRef] [Green Version]
- Potashkin, J.; Huang, X.; Becker, C.; Chen, H.; Foltynie, T.; Marras, C. Understanding the Links Between Cardiovascular Disease and Parkinson’s Disease. Mov. Disord. 2020, 35, 55–74. [Google Scholar] [CrossRef]
- Ahmed, S.S.; Santosh, W.; Kumar, S.; Christlet, H.T.T. Metabolic profiling of Parkinson’s disease: Evidence of biomarker from gene expression analysis and rapid neural network detection. J. Biomed. Sci. 2009, 16, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glaser, C.B.; Yamin, G.; Uversky, V.N.; Fink, A.L. Methionine oxidation, α-synuclein and Parkinson’s disease. Biochim. Biophys. Acta Proteins Proteom. 2005, 1703, 157–169. [Google Scholar] [CrossRef]
- Andréasson, M.; Brodin, L.; Laffita-Mesa, J.M.; Svenningsson, P. Correlations Between Methionine Cycle Metabolism, COMT Genotype, and Polyneuropathy in L-Dopa Treated Parkinson’s Disease: A Preliminary Cross-Sectional Study. J. Park. Dis. 2017, 7, 619–628. [Google Scholar] [CrossRef]
- Chung, S.J.; Rim, J.H.; Ji, D.; Lee, S.; Yoo, H.S.; Jung, J.H.; Baik, K.; Choi, Y.; Ye, B.S.; Sohn, Y.H.; et al. The gut microbiota-derived metabolite trimethylamine N-oxide as a biomarker in early Par-kinson’s disease. Nutrition 2020, 83, 111090. [Google Scholar] [CrossRef]
- Trompette, A.; Gollwitzer, E.S.; Yadava, K.; Sichelstiel, A.K.; Sprenger, N.; Ngom-Bru, C.; Blanchard, C.; Junt, T.; Nicod, L.P.; Harris, N.L.; et al. Gut microbiota metabolism of dietary fiber influences allergic airway disease and hematopoiesis. Nat. Med. 2014, 20, 159–166. [Google Scholar] [CrossRef]
- Aho, V.T.E.; Houser, M.C.; Pereira, P.A.B.; Chang, J.; Rudi, K.; Paulin, L.; Hertzberg, V.; Auvinen, P.; Tansey, M.G.; Scheperjans, F. Relationships of gut microbiota, short-chain fatty acids, inflammation, and the gut barrier in Parkinson’s disease. Mol. Neurodegener. 2021, 16, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Sobhonslidsuk, A.; Chanprasertyothin, S.; Pongrujikorn, T.; Kaewduang, P.; Promson, K.; Petraksa, S.; Ongphiphadhanakul, B. The association of gut microbiota with nonalcoholic steato-hepatitis in Thais. BioMed Res. Int. 2018, 2018, 9340316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vural, S.; Ayvaz, M.A.; Kesicioğlu, T.; Turfan, S.; Ayraler, A. Prevalence of Non Alcoholic Fatty Liver Disease in patients with Parkinson Disease. Anatol. J. Fam. Med. 2019, 2, 38–40. [Google Scholar] [CrossRef]
- Wang, Y.; Ouyang, M.; Gao, X.; Wang, S.; Fu, C.; Zeng, J.; He, X. Phocea, Pseudoflavonifractor and Lactobacillus intestinalis: Three Potential Biomarkers of Gut Microbiota That Affect Progression and Complications of Obesity-Induced Type 2 Diabetes Mellitus. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 835–850. [Google Scholar] [CrossRef] [Green Version]
- Hassan, A.; Kandel, R.S.; Mishra, R.; Gautam, J.; Alaref, A.; Jahan, N. Diabetes Mellitus and Parkinson’s Disease: Shared Pathophysiological Links and Possible Therapeutic Implications. Cureus 2020, 12, e9853. [Google Scholar] [CrossRef] [PubMed]
- Fontana, A.; Manchia, M.; Panebianco, C.; Paribello, P.; Arzedi, C.; Cossu, E.; Garzilli, M.; Montis, M.A.; Mura, A.; Pisanu, C.; et al. Exploring the Role of Gut Microbiota in Major Depressive Disorder and in Treatment Resistance to Antidepressants. Biomedicines 2020, 8, 311. [Google Scholar] [CrossRef]
- Marsh, L. Depression and Parkinson’s Disease: Current Knowledge. Curr. Neurol. Neurosci. Rep. 2013, 13, 1–9. [Google Scholar] [CrossRef]
- Vogt, N.M.; Kerby, R.L.; Dill-McFarland, K.A.; Harding, S.J.; Merluzzi, A.P.; Johnson, S.C.; Carlsson, C.M.; Asthana, S.; Zetterberg, H.; Blennow, K.; et al. Gut microbiome alterations in Alzheimer’s disease. Sci. Rep. 2017, 7, 1–11. [Google Scholar] [CrossRef]
- Goetz, C.G.; Emre, M.; Dubois, B. Parkinson’s disease dementia: Definitions, guidelines, and research perspectives in diagnosis. Ann. Neurol. Off. J. Am. Neurol. Assoc. Child Neurol. Soc. 2008, 64 (Suppl. 2), S81–S92. [Google Scholar] [CrossRef]
- Gibiino, G.; Lopetuso, L.R.; Scaldaferri, F.; Rizzatti, G.; Binda, C.; Gasbarrini, A. Exploring Bacteroidetes: Metabolic key points and immunological tricks of our gut commensals. Dig. Liver Dis. 2018, 50, 635–639. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classification | PD Group | HC Group | Total | |
|---|---|---|---|---|
| Total | 10 | 10 | 20 | |
| Sex (number) | Male | 5 | 4 | 9 |
| Female | 5 | 6 | 11 | |
| Age (years) | Minimum | 50 | 51 | 50 |
| Maximum | 74 | 68 | 74 | |
| Average | 66.6 | 58.7 | 62.65 | |
| Disease duration (years) | Minimum | 0.17 | - | 0.17 |
| Maximum | 12 | - | 12 | |
| Average | 5.02 | - | 5.02 | |
| Classification | Gut Microbes | PD Group vs. HC Group | ||
|---|---|---|---|---|
| ↑/↓ § | Significance (p < 0.05) | |||
| Stool | Phylum level | Bacteroidetes | ↓ | 0.012 |
| Genus level | Prevotella | ↓ | 0.030 | |
| Phascolarctobacterium | ↓ | 0.047 | ||
| Pseudoflavonifractor | ↓ | 0.037 | ||
| Eisenbergiella | ↑ | 0.037 | ||
| Gemella | ↓ | 0.014 | ||
| Classification | Function | |
|---|---|---|
| Metabolites | Acetate | Acetate is involved in lipid metabolism. It enhances de novo lipid synthesis by activating lipogenic genes [16]. |
| Citrate | Citrate is involved in glucose metabolism. As an intermediate of the Kreb’s cycle, it regulates the activity of PDH, an enzyme that converts pyruvate to acetyl-coA [18]. | |
| Methionine | Methionine is involved in the accumulation of α-synuclein. The accumulation of α-synuclein in the dopaminergic neurons of substantia nigra is a crucial step in the pathogenesis of PD [19]. | |
| Trimethylamine | Trimethylamine is oxidized to produce TMAO. TMAO is related to the severity and the progression of motor symptoms of PD [21]. | |
| Gut microbes | Bacteroidetes | Bacteroidetes produces favorable metabolites such as SCFAs that reduce inflammation [22]. |
| Prevotella | Prevotella produces H2S, which is a gasotransmitter closely related to neuroprotection [8]. | |
| Phascolarctobacterium | Phascolarctobacterium has beneficial effects by producing SCFAs. It is known to be associated with the occurrence of NAFLD [24]. | |
| Pseudoflavonifractor | Pseudoflavonifractor is associated with energy metabolism and insulin sensitivity [26]. | |
| Eisenbergiella | Eisenbergiella is reported to be associated with major depressive disorder [28]. | |
| Gemella | Gemella is reported to be associated with Alzheimer’s disease [30]. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, C.-H.; Jung, J.; Lee, Y.-u.; Kim, K.-h.; Kang, S.; Kang, G.-h.; Chu, H.; Kim, S.-Y.; Lee, S. Comparison of Metabolites and Gut Microbes between Patients with Parkinson’s Disease and Healthy Individuals—A Pilot Clinical Observational Study (STROBE Compliant). Healthcare 2022, 10, 302. https://doi.org/10.3390/healthcare10020302
Kim C-H, Jung J, Lee Y-u, Kim K-h, Kang S, Kang G-h, Chu H, Kim S-Y, Lee S. Comparison of Metabolites and Gut Microbes between Patients with Parkinson’s Disease and Healthy Individuals—A Pilot Clinical Observational Study (STROBE Compliant). Healthcare. 2022; 10(2):302. https://doi.org/10.3390/healthcare10020302
Chicago/Turabian StyleKim, Cheol-Hyun, Jeeyoun Jung, Young-ung Lee, Kwang-ho Kim, Sunny Kang, Geon-hui Kang, Hongmin Chu, Se-Young Kim, and Sangkwan Lee. 2022. "Comparison of Metabolites and Gut Microbes between Patients with Parkinson’s Disease and Healthy Individuals—A Pilot Clinical Observational Study (STROBE Compliant)" Healthcare 10, no. 2: 302. https://doi.org/10.3390/healthcare10020302
APA StyleKim, C. -H., Jung, J., Lee, Y. -u., Kim, K. -h., Kang, S., Kang, G. -h., Chu, H., Kim, S. -Y., & Lee, S. (2022). Comparison of Metabolites and Gut Microbes between Patients with Parkinson’s Disease and Healthy Individuals—A Pilot Clinical Observational Study (STROBE Compliant). Healthcare, 10(2), 302. https://doi.org/10.3390/healthcare10020302