
Maternal and Fetal Effects of Gestational Vitamin D Concentration

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Vitamin D Level Analysis of the Mother
2.3. Maternal Hematological and Serological Analyses
2.4. Maternal Testing for Sexually Transmitted Diseases
2.5. Maternal BMD Measurement
2.6. Precise Fetal Ultrasound Analysis
2.7. Statistical Analysis
3. Results
3.1. Vitamin D Distribution Stratified According to Maternal Age
3.2. Hematologic Correlation Stratified According to Serum Vitamin D Concentration
3.3. Correlation of Serological Factors with the Serum Vitamin D Concentrations
3.4. Correlation between Serum Vitamin D Concentration and Sexually Transmitted Pathogens
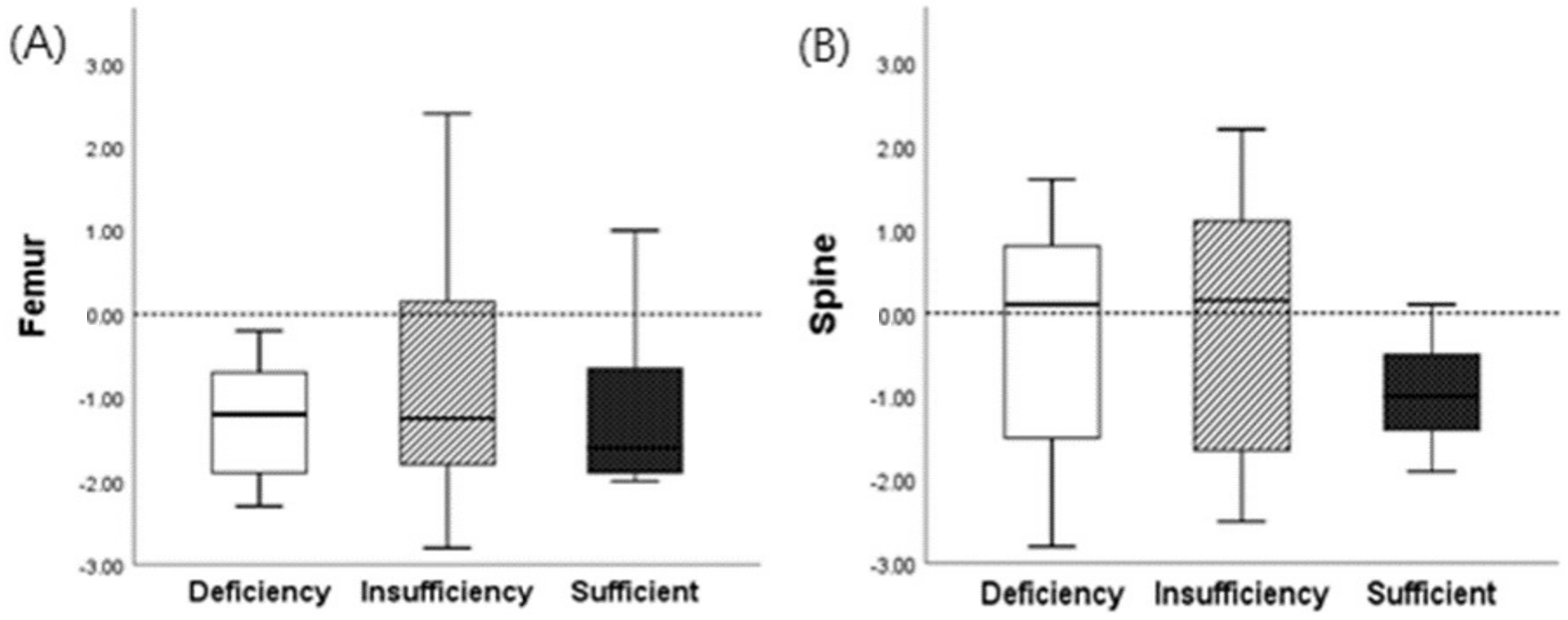
3.5. Correlation between BMD and Serum Vitamin D Concentration in Reproductive Age Women
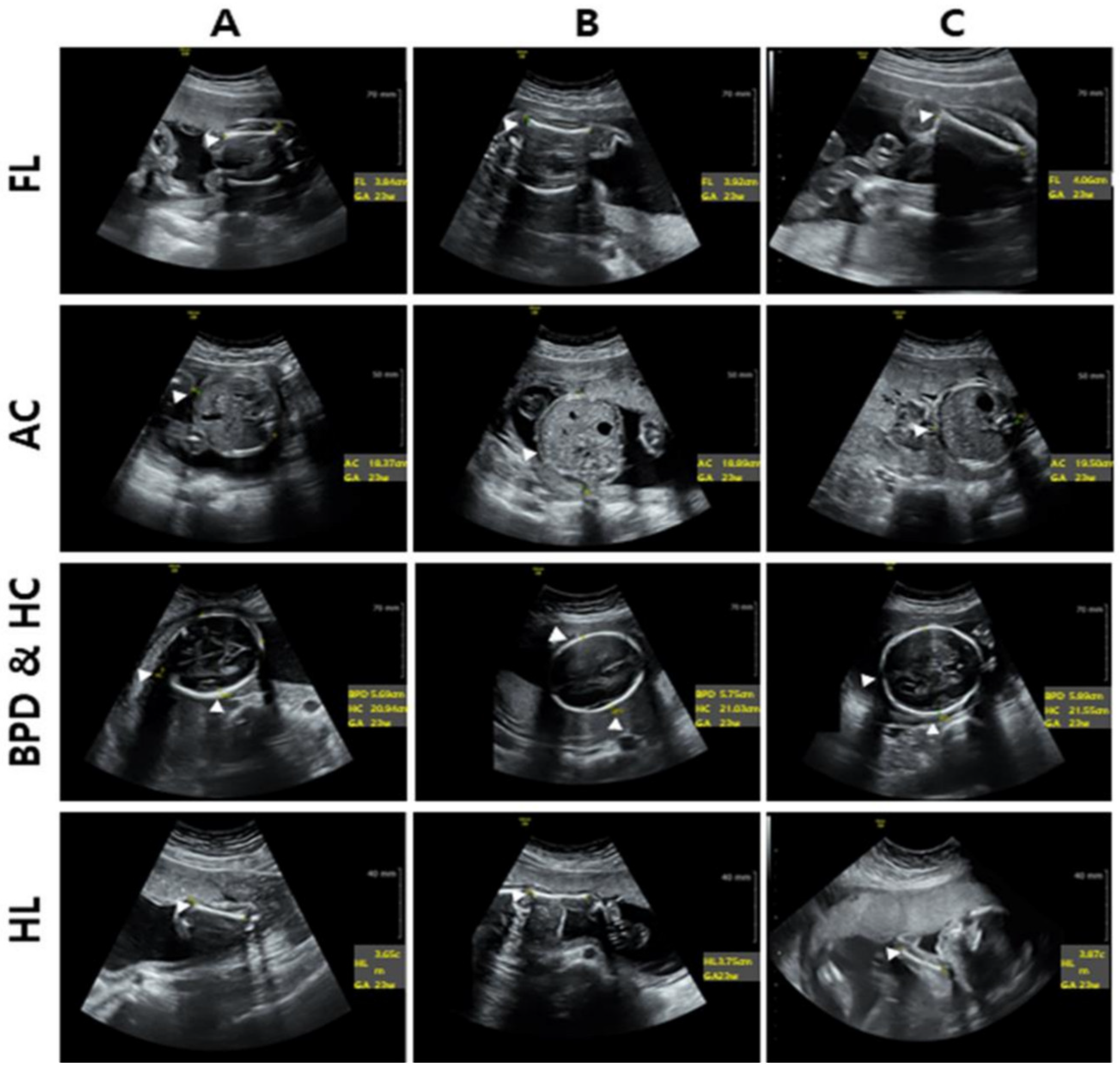
3.6. Results of Prenatal Ultrasonographic Analysis Stratified by Maternal Serum Vitamin D Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shin, C.S.; Choi, H.J.; Kim, M.J.; Kim, J.T.; Yu, S.H.; Koo, B.K.; Cho, H.Y.; Cho, S.W.; Kim, S.W.; Park, Y.J.; et al. Prevalence and risk factors of osteoporosis in Korea: A community-based cohort study with lumbar spine and hip bone mineral density. Bone 2010, 47, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Giovannucci, E.; Willett, W.C.; Dietrich, T.; Dawson-Hughes, B. Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am. J. Clin. Nutr. 2006, 84, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Van Gerwen, O.T.; Muzny, C.A.; Marrazzo, J.M. Sexually transmitted infections and female reproductive health. Nat. Microbiol. 2022, 7, 1116–1126. [Google Scholar] [CrossRef]
- Chung, Y.S.; Yoo, B.W.; Oh, J.E.; Lee, D.C.; Lee, H.S.; Cho, C.Y. The relationship between vitamin D levels and chronic diseases. Korean J. Clin. Geriatr. 2010, 11, 154–169. [Google Scholar]
- Kunz, C.; Rodriguez-Palmero, M.; Koletzko, B.; Jensen, R. Nutritional and biochemical properties of human milk, Part I: General aspects, proteins, and carbohydrates. Clin. Perinatol. 1999, 26, 307–333. [Google Scholar] [CrossRef]
- Jeong, Y.W.; Song, J.H.; Min, J.W.; Park, G.H.; Min, K.S. Correlation and measurement between stress of mother and fetus using heart rate variability. Korean J. Obstet. Gynecol. 2006, 49, 823–830. [Google Scholar]
- Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Willett, W.C.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Changes in dietary intake from the first to the second trimester of pregnancy. Paediatr. Perinat. Epidemiol. 2006, 20, 35–42. [Google Scholar] [CrossRef]
- Dawson-Hughes, B.; Heaney, R.P.; Holick, M.F.; Lips, P.; Meunier, P.J.; Vieth, R. Estimates of optimal vitamin D status. Osteoporos. Int. 2005, 16, 713–716. [Google Scholar] [CrossRef]
- Innes, A.M.; Seshia, M.M.; Prasad, C.; Al Saif, S.; Friesen, F.R.; Chudley, A.E.; Reed, M.; Dilling, L.A.; Haworth, J.C.; Greenberg, C.R. Congenital rickets caused by maternal vitamin D deficiency. Paediatr. Child Health 2002, 7, 455–458. [Google Scholar] [CrossRef]
- Anatoliotaki, M.; Tsilimigaki, A.; Tsekoura, T.; Schinaki, A.; Stefanaki, S.; Nicolaidou, P. Congenital rickets due to maternal vitamin D deficiency in a sunny island of Greece. Acta Paediatr. 2003, 92, 389–391. [Google Scholar] [CrossRef]
- Orbak, Z.; Karacan, M.; Doneray, H.; Karakelleoglu, C. Congenital rickets presenting with hypocalcaemic seizures. West Indian Med. J. 2007, 56, 364–367. [Google Scholar] [PubMed]
- Park, Y.K. Estimation of gestational age from ultrasonic measurement of fetal growth parameter in Korean normal pregnancy: A prospective evaluation. Obstet. Gynecol. Sci. 1995, 38, 2230–2241. [Google Scholar]
- Choi, J.S.; Yang, J.H.; Ryu, H.M.; Kim, M.Y.; Han, J.Y.; Ahn, H.K.; Jung, S.H.; Choi, K.H.; Lee, J.Y.; Lee, S.Y.; et al. Estimation of mean fetal biometry by using ultrasonography in normal pregnancy. Korean J. Obstet. Gynecol. 2002, 45, 1497–1504. [Google Scholar]
- Nah, E.H.; Kim, S.; Cho, H.I. Vitamin D levels and prevalence of vitamin D deficiency associated with sex, age, region, and season in Koreans. Lab. Med. Online 2015, 5, 84–91. [Google Scholar] [CrossRef]
- Harvey, N.C.; Holroyd, C.; Ntani, G.; Javaid, K.; Cooper, P.; Moon, R.; Cole, Z.; Tinati, T.; Godfrey, K.; Dennison, E.; et al. Vitamin D supplementation in pregnancy: A systematic review. Health Technol. Assess. 2014, 18, 1–190. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.; Park, S.; Park, K. Association between vitamin D deficiency and anemia among Korean adolescent girls and young women. J. Nutr. Health 2019, 52, 552–558. [Google Scholar] [CrossRef]
- Kang, S.W. Vitamin D and Immune Responses. J. Rheum. Dis. 2010, 17, 16–22. [Google Scholar] [CrossRef]
- Kranioti, E.F.; Bonicelli, A.; García-Donas, J.G. Bone-mineral density: Clinical significance, methods of quantification and forensic applications. Res. Rep. Forensic. Med. Sci. 2019, 9, 9–21. [Google Scholar] [CrossRef]
- Sadat-Ali, M.; Al Elq, A.H.; Al-Turki, H.A.; Al-Mulhim, F.A.; Al-Ali, A.K. Influence of vitamin D levels on bone mineral density and osteoporosis. Ann. Saudi Med. 2011, 31, 602–608. [Google Scholar] [CrossRef]
- Bolland, M.J.; Grey, A.; Avenell, A. Effects of vitamin D supplementation on musculoskeletal health: A systematic review, meta-analysis, and trial sequential analysis. Lancet Diabetes Endocrinol. 2018, 6, 847–858. [Google Scholar] [CrossRef]
- Reid, I.R.; Bolland, M.J.; Grey, A. Effects of vitamin D supplements on bone mineral density: A systematic review and meta-analysis. Lancet 2014, 383, 146–155. [Google Scholar] [CrossRef]
- Myung, S.K.; Cho, H. Effects of intermittent or single high-dose vitamin D supplementation on risk of falls and fractures: A systematic review and meta-analysis. Osteoporos. Int. 2023, 34, 1355–1367. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, L.M.; Krohn, M.A.; Simhan, H.N. Maternal vitamin D deficiency is associated with bacterial vaginosis in the first trimester of pregnancy. J. Nutr. 2009, 139, 1157–1161. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, C.; Isakova, T.; Collerone, G.; Olbina, G.; Wolf, M.; Westerman, M.; Gutiérrez, O.M. Hepcidin and disordered mineral metabolism in chronic kidney disease. Clin. Nephrol. 2011, 76, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Workowski, K.A.; Bolan, G.A.; Workowski, K.A.; Akinyemi, D.; Bachmann, L.; Burstein, G.; Cohen, S.; Gardella, C.; Geisler, W.M.; Ghanem, K.; et al. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm. Rep. 2015, 64, 1–137. [Google Scholar] [PubMed]
- Hewison, M. An update on vitamin D and human immunity. Clin. Endocrinol. 2012, 76, 315–325. [Google Scholar] [CrossRef]
- Weaver, C.M. Vitamin D, calcium homeostasis, and skeleton accretion in children. J. Bone Miner. Res. 2007, 22, V45–V49. [Google Scholar] [CrossRef]
- Markestad, T.; Aksnes, L.; Ulstein, M.; Aarskog, D. 25-Hydroxyvitamin D and 1,25-dihydroxyvitamin D of D2 and D3 origin in maternal and umbilical cord serum after vitamin D2 supplementation in human pregnancy. Am. J. Clin. Nutr. 1984, 40, 1057–1063. [Google Scholar] [CrossRef]
- Na, B.; No, S.; Kim, M.J.; Han, H.S.; Jeong, E.H.; Han, Y.; Hyeun, T. Nutritional status of vitamin D in Korean mothers and their newborn infants. Korean J. Perinatol. 2007, 18, 399–406. [Google Scholar]
- Greer, F.R. 25-Hydroxyvitamin D: Functional outcomes in infants and young children. Am. J. Clin. Nutr. 2008, 88, 529S–533S. [Google Scholar] [CrossRef]
- Namgung, R.; Tsang, R.C. Factors affecting newborn bone mineral content: In utero effects on newborn bone mineralization. Proc. Nutr. Soc. 2000, 59, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Kim, E.A.; Park, M.N. Effects of calcium supplementations on mineral metabolism during pregnancy with calcium-deficient young adult rats. Korean J. Nutr. 2003, 36, 459–469. [Google Scholar]
- Morley, R.; Carlin, J.B.; Pasco, J.A.; Wark, J.D. Maternal 25-hydroxyvitamin D and parathyroid hormone concentrations and offspring birth size. J. Clin. Endocrinol. Metab. 2006, 91, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Young, B.E.; McNanley, T.J.; Cooper, E.M.; McIntyre, A.W.; Witter, F.; Harris, Z.L.; O’Brien, K.O. Maternal vitamin D status and calcium intake interact to affect fetal skeletal growth in utero in pregnant adolescents. Am. J. Clin. Nutr. 2012, 95, 1103–1112. [Google Scholar] [CrossRef] [PubMed]
- Curtis, E.M.; Moon, R.J.; Dennison, E.M.; Harvey, N.C. Prenatal calcium and vitamin D intake, and bone mass in later life. Curr. Osteoporos. Rep. 2014, 12, 194–204. [Google Scholar] [CrossRef]
- Javaid, M.K.; Crozier, S.R.; Harvey, N.C.; Gale, C.R.; Dennison, E.M.; Boucher, B.J.; Arden, N.K.; Godfrey, K.M.; Cooper, C. Maternal vitamin D status during pregnancy and childhood bone mass at age 9 years: A longitudinal study. Lancet 2006, 367, 36–43. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Women of Childbearing Age (n = 40) | Pregnant Women (n = 48) | |||
|---|---|---|---|---|
| Deficiency | Insufficiency | Sufficient | ||
| Number of women | 40 (100%) | 20 (41.67%) | 11 (22.97%) | 17 (35.42%) |
| 25(OH)D3 (ng/mL) | 20.20 (±10.16) | 15.87 (±2.68) ** | 25.79 (±3.59) | 39.58 (±5.80) ** |
| Hematology | Control | Vitamin D Group | p-Value | |||
|---|---|---|---|---|---|---|
| Deficiency | Insufficiency | Sufficient | ||||
| WBC | 103/µL | 7.21 (±1.41) | 7.80 (±1.21) | 7.88 (±1.47) | 8.49 (±1.15) | 0.776 |
| RBC | 106/µL | 4.39 (±0.43) | 4.23 (±0.43) | 4.21 (±0.22)) | 4.10 (±0.37) | 0.801 |
| Hb | g/dL | 12.96 (±0.73) | 12.80 (±0.77) | 12.62 (±0.82) | 12.40 (±1.13) | 0.713 |
| Ht | % | 37.11 (±2.23) | 36.80 (±2.20) | 36.74 (±1.84) | 36.13 (±2.95) | 0.936 |
| PLT | 103/µL | 262.80 (±92.89) | 271.00 (±107.17) | 286.29 (±69.51) | 279.71 (±48.30) | 0.711 |
| Clinical Chemistry Test | Control | Vitamin D Group | p-Value | |||
|---|---|---|---|---|---|---|
| Deficiency | Insufficiency | Sufficient | ||||
| AST | U/L | 18.82 (±3.26) | 17.00 (±3.22) | 17.04 (±2.84) | 19.57 (±3.44) | 0.475 |
| ALT | U/L | 12.90 (±6.92) | 12.00 (±5.89) | 12.19 (±5.68) | 16.21 (±11.17) | 0.707 |
| BUN | mg/dL | 8.93 (±3.36) | 8.70 (±2.89) | 7.95 (±2.25) | 7.46 (±1.21) | 0.245 |
| CRE | mg/dL | 0.63 (±0.11) | 0.60 (±0.09) | 0.58 (±0.12) | 0.66 (±0.12) | 0.528 |
| TP | g/dL | 7.39 (±0.37) | 7.00 (±0.27) | 7.10 (±0.45) | 7.06 (±0.54) | 0.808 |
| Alb | g/dL | 4.45 (±0.28) | 4.20 (±0.29) | 4.34 (±0.23) | 4.19 (±0.21) | 0.298 |
| Globulin | g/dL | 2.82 (±0.27) | 2.70 (±0.24) | 2.75 (±0.24) | 2.85 (±0.43) | 0.979 |
| GFR | mL/min/1.73 m2 | 128.39 (±22.19) | 127.0 (±20.87) | 127.35 (±23.97) | 108.81 (±24.36) | 0.841 |
| STD | Vitamin D Group | ||
|---|---|---|---|
| Deficiency | Insufficiency | Sufficient | |
| Negative | 5 (25.0%) | 6 (54.5%) | 11 (64.7%) |
| Positive | 15 (75.0%) | 5 (45.5%) | 6 (35.3%) |
| Total | 20 (100%) | 11 (100%) | 17 (100%) |
| Microorganism Infection | Vitamin D Group | ||
|---|---|---|---|
| Deficiency | Insufficiency | Sufficient | |
| Single | 7 (46.6%) | 2 (40.0%) | 3 (50.0%) |
| 2 Cross | 5 (33.4%) | 3 (60.0%) | 3 (50.0%) |
| 3 Cross | 3 (20.0%) | 0 (0%) | 0 (0%) |
| Total | 15 (100%) | 5 (100%) | 6 (100%) |
| Infection | Microorganism | ||||||
|---|---|---|---|---|---|---|---|
| GV | CA | UP | UU | MH | HSV 1 | ||
| Single Infection | A | 3 | 0 | 2 | 0 | 0 | 0 |
| B | 3 | 0 | 0 | 0 | 0 | 0 | |
| C | 1 | 0 | 3 | 0 | 0 | 0 | |
| 2 Cross infection | A | 5 | 0 | 5 | 1 | 0 | 0 |
| B | 1 | 0 | 1 | 0 | 1 | 0 | |
| C | 0 | 0 | 1 | 1 | 0 | 0 | |
| 3 Cross infection | A | 3 | 2 | 2 | 0 | 2 | 0 |
| B | 0 | 0 | 0 | 0 | 0 | 0 | |
| C | 0 | 0 | 0 | 0 | 0 | 0 | |
| Total | 16 | 2 | 14 | 2 | 3 | 0 | |
| Bone Mineral Density | Vitamin D Group | p-Value | ||
|---|---|---|---|---|
| Deficiency | Insufficiency | Sufficient | ||
| Spine (L1) | 0.15 (±1.37) | 0.20 (±1.52) | −0.95 (±0.73) | 0.296 |
| Femur (neck) | −1.20 (±1.08) | −1.10 (±1.45) | −1.70 (±1.05) | 0.824 |
| Fetus Ultra-Sound Imaging | Vitamin D Group | p-Value | ||
|---|---|---|---|---|
| Deficiency | Insufficiency | Sufficient | ||
| HC | 21.04 (±0.82) | 20.44 (±0.71) | 21.58 (±0.72) | 0.011 |
| AC | 18.56 (±0.92) | 18.37 (±0.76) | 19.08 (±0.70) | 0.11 |
| HL | 3.71 (±0.16) | 3.64 (±0.17) | 3.86 (±0.09) | 0.002 |
| BPD | 5.70 (±0.34) | 5.40 (±0.37) | 5.71 (±0.33) | 0.638 |
| FL | 3.92 (±0.82) | 3.84 (±0.15) | 4.01 (±0.33) | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, K.-W.; Lee, Y.-H.; Yeo, M.-H.; Park, S.-H.; Kim, H.-R.; Kim, H.-S.; Chang, K.-S. Maternal and Fetal Effects of Gestational Vitamin D Concentration. Healthcare 2023, 11, 2325. https://doi.org/10.3390/healthcare11162325
Kwon K-W, Lee Y-H, Yeo M-H, Park S-H, Kim H-R, Kim H-S, Chang K-S. Maternal and Fetal Effects of Gestational Vitamin D Concentration. Healthcare. 2023; 11(16):2325. https://doi.org/10.3390/healthcare11162325
Chicago/Turabian StyleKwon, Ki-Wook, Young-Hyeon Lee, Min-Ho Yeo, Sang-Hyun Park, Hye-Ran Kim, Hye-Sook Kim, and Kyung-Soo Chang. 2023. "Maternal and Fetal Effects of Gestational Vitamin D Concentration" Healthcare 11, no. 16: 2325. https://doi.org/10.3390/healthcare11162325
APA StyleKwon, K. -W., Lee, Y. -H., Yeo, M. -H., Park, S. -H., Kim, H. -R., Kim, H. -S., & Chang, K. -S. (2023). Maternal and Fetal Effects of Gestational Vitamin D Concentration. Healthcare, 11(16), 2325. https://doi.org/10.3390/healthcare11162325