


Older Adults’ Use of a Research-Based Web Platform for Social Interaction

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Setting, Participants and Recruitment
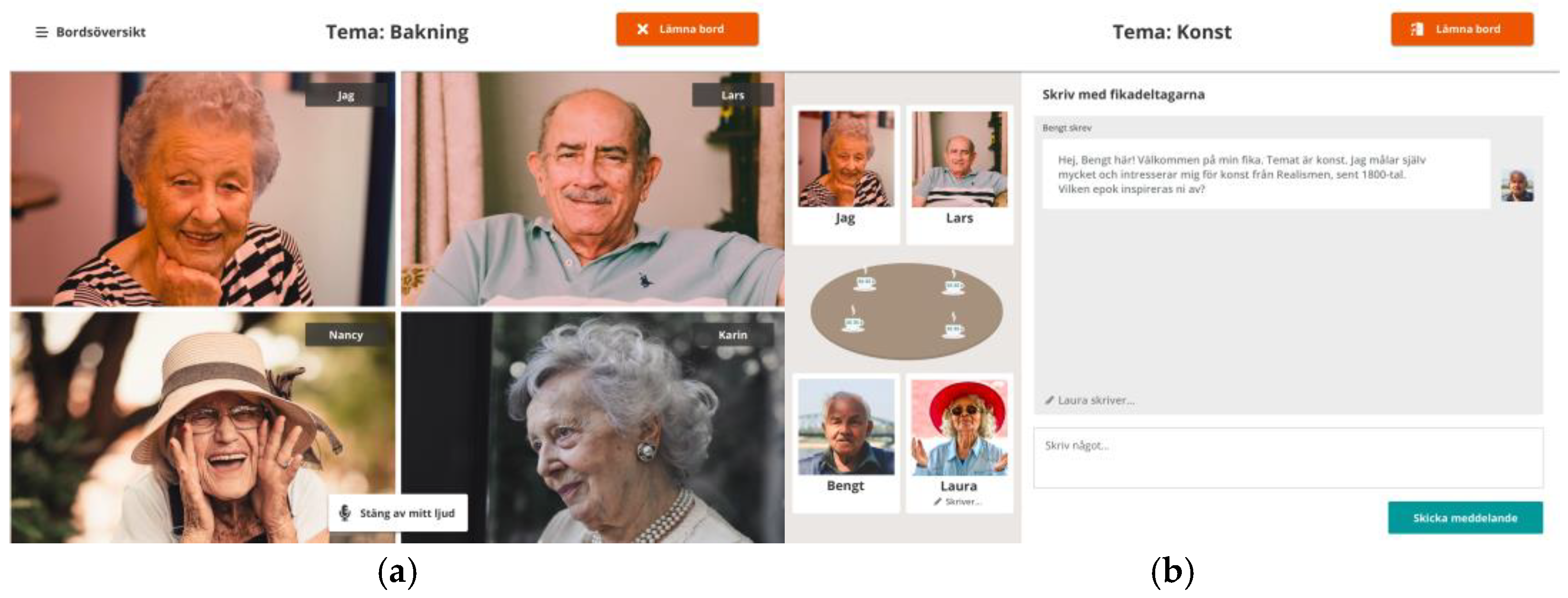
2.3. The Research-Based Web Platform—The Fik@ Room

2.4. The Intervention
2.5. Data Collection
2.5.1. Data Collected from Older Adults
2.5.2. Data Collected from Researchers and Social Services Personnel
2.6. Data Analysis
2.6.1. Quantitative Data
2.6.2. Qualitative Data
3. Results
3.1. Participants
3.2. Older Adults’ Experienced Loneliness and Social Network
3.3. Older Adults’ Patterns of Use of the Fik@ Room
3.4. Support and Information, Navigationand Use of the Functions from the Perspectives of Older Adults, Researchers, and Social Services Personnel
3.5. Older Adults’ Expectations of the Fik@ Room and Its Importance in Relation to the Pandemic
3.6. Older Adults’ Incentives to Participate or Not Participate in the Fik@ Room—From the Perspective of the Social Services Personnel
4. Discussion
Strengths and Limitations
5. Conclusions and Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Courtin, E.; Knapp, M. Social Isolation, Loneliness and Health in Old Age: A Scoping Review. Health Soc. Care Community 2015, 25, 799–812. [Google Scholar] [CrossRef] [PubMed]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and Social Isolation as Risk Factors for Mortality. Perspect. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An Overview of Systematic Reviews on the Public Health Consequences of Social Isolation and Loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, C.; Majeed, A.; Gill, H.; Tamura, J.; Ho, R.C.; Mansur, R.B.; Nasri, F.; Lee, Y.; Rosenblat, J.D.; Wong, E.; et al. The Effect of Loneliness on Distinct Health Outcomes: A Comprehensive Review and Meta-Analysis. Psychiatry Res. 2020, 294, 113514. [Google Scholar] [CrossRef]
- Böger, A.; Huxhold, O. Age-Related Changes in Emotional Qualities of the Social Network from Middle Adulthood into Old Age: How Do They Relate to the Experience of Loneliness? Psychol. Aging 2018, 33, 482–496. [Google Scholar] [CrossRef]
- Wrzus, C.; Hänel, M.; Wagner, J.; Neyer, F.J. Social Network Changes and Life Events across the Life Span: A Meta-Analysis. Psychol. Bull. 2013, 139, 53–80. [Google Scholar] [CrossRef] [Green Version]
- Dahlberg, L. Loneliness during the COVID-19 Pandemic. Aging Ment. Health 2021, 25, 1–4. [Google Scholar] [CrossRef]
- Elran-Barak, R.; Mozeikov, M. One Month into the Reinforcement of Social Distancing due to the COVID-19 Outbreak: Subjective Health, Health Behaviors, and Loneliness among People with Chronic Medical Conditions. Int. J. Environ. Res. Public Health 2020, 17, 5403. [Google Scholar] [CrossRef]
- Wahl, H.-W.; Gerstorf, D. A Conceptual Framework for Studying COntext Dynamics in Aging (CODA). Dev. Rev. 2018, 50, 155–176. [Google Scholar] [CrossRef]
- Schlomann, A.; Seifert, A.; Zank, S.; Woopen, C.; Rietz, C. Use of Information and Communication Technology (ICT) Devices among the Oldest-Old: Loneliness, Anomie, and Autonomy. Innov. Aging 2020, 4, igz050. [Google Scholar] [CrossRef]
- Baker, S.; Warburton, J.; Waycott, J.; Batchelor, F.; Hoang, T.; Dow, B.; Ozanne, E.; Vetere, F. Combatting Social Isolation and Increasing Social Participation of Older Adults through the Use of Technology: A Systematic Review of Existing Evidence. Australas. J. Ageing 2018, 37, 184–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.-R.R.; Schulz, P.J. The Effect of Information Communication Technology Interventions on Reducing Social Isolation in the Elderly: A Systematic Review. J. Med. Internet Res. 2016, 18, e18. [Google Scholar] [CrossRef]
- Chen, E.; Wood, D.; Ysseldyk, R. Online Social Networking and Mental Health among Older Adults: A Scoping Review. Can. J. Aging La Rev. Can. Du Vieil. 2021, 41, 26–39. [Google Scholar] [CrossRef]
- Czaja, S.J.; Boot, W.R.; Charness, N.; Rogers, W.A.; Sharit, J. Improving Social Support for Older Adults through Technology: Findings from the PRISM Randomized Controlled Trial. Gerontologist 2017, 58, 467–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibarra, F.; Baez, M.; Cernuzzi, L.; Casati, F. A Systematic Review on Technology-Supported Interventions to Improve Old-Age Social Wellbeing: Loneliness, Social Isolation, and Connectedness. J. Healthc. Eng. 2020, 2020, 1–14. [Google Scholar] [CrossRef]
- Beller, J.; Wagner, A. Loneliness, Social Isolation, Their Synergistic Interaction, and Mortality. Health Psychol. 2018, 37, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Newall, N.E.G.; Menec, V.H. Loneliness and Social Isolation of Older Adults. J. Soc. Pers. Relatsh. 2017, 36, 026540751774904. [Google Scholar] [CrossRef] [Green Version]
- Casanova, G.; Zaccaria, D.; Rolandi, E.; Guaita, A. The Effect of Information and Communication Technology and Social Networking Site Use on Older People’s Well-Being in Relation to Loneliness: Review of Experimental Studies. J. Med. Internet Res. 2021, 23, e23588. [Google Scholar] [CrossRef]
- Khosravi, P.; Rezvani, A.; Wiewiora, A. The Impact of Technology on Older Adults’ Social Isolation. Comput. Hum. Behav. 2016, 63, 594–603. [Google Scholar] [CrossRef]
- Noone, C.; McSharry, J.; Smalle, M.; Burns, A.; Dwan, K.; Devane, D.; Morrissey, E.C. Video Calls for Reducing Social Isolation and Loneliness in Older People: A Rapid Review. Cochrane Database Syst. Rev. 2020, 5, 5. [Google Scholar] [CrossRef]
- Jiménez, F.N.; Brazier, J.F.; Davoodi, N.M.; Florence, L.C.; Thomas, K.S.; Gadbois, E.A. A Technology Training Program to Alleviate Social Isolation and Loneliness among Homebound Older Adults: A Community Case Study. Front. Public Health 2021, 9, 1753. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Coughlin, J.F. PERSPECTIVE: Older Adults’ Adoption of Technology: An Integrated Approach to Identifying Determinants and Barriers. J. Prod. Innov. Manag. 2014, 32, 747–759. [Google Scholar] [CrossRef]
- Nef, T.; Ganea, R.L.; Müri, R.M.; Mosimann, U.P. Social Networking Sites and Older Users—A Systematic Review. Int. Psychogeriatr. 2013, 25, 1041–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poscia, A.; Stojanovic, J.; La Milia, D.I.; Duplaga, M.; Grysztar, M.; Moscato, U.; Onder, G.; Collamati, A.; Ricciardi, W.; Magnavita, N. Interventions Targeting Loneliness and Social Isolation among the Older People: An Update Systematic Review. Exp. Gerontol. 2018, 102, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Thangavel, G.; Memedi, M.; Hedström, K. Customised Information and Communication Technology for Reducing Social Isolation and Loneliness among Older Adults: A Scoping Review (Preprint). JMIR Ment. Health 2021, 9, e34221. [Google Scholar] [CrossRef] [PubMed]
- Hunter, A.; Brewer, J.D. Designing Multimethod Research; Hesse-Biber, S.N., Johnson, R.B., Eds.; Oxford University Press: Oxford, UK, 2015. [Google Scholar] [CrossRef]
- Florin, U. On design dialogues: Their roots, features, and usage. In Different Perspectives in Design Thinking; Eriksson, Y., Ed.; CRC Press: Boca Raton, FL, USA, 2021. [Google Scholar] [CrossRef]
- Sanders, E.B.-N.; Stappers, P.J. Co-Creation and the New Landscapes of Design. CoDesign 2008, 4, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Johansson-Pajala, R.-M.; Gusdal, A.K.; Eklund, C.; Florin, U.; Wågert, P.V.H. A Codesigned Web Platform for Reducing Social Isolation and Loneliness in Older People: A Feasibility Study. Inform. Health Soc. Care 2022, 5, 1–16. [Google Scholar] [CrossRef]
- Russell, D.W. UCLA Loneliness Scale (Version 3): Reliability, Validity, and Factor Structure. J. Personal. Assess. 1996, 66, 20–40. [Google Scholar] [CrossRef]
- UCLA Loneliness Scale. Available online: https://www.studocu.com/en-au/document/queensland-university-of-technology/forensic-digital-analysis/self-measures-for-loneliness-and-interpersonal-problems-ucla-loneliness/15668682 (accessed on 15 May 2021).
- Larsson, E.; Nilsson, I.; Larsson Lund, M. Participation in Social Internet-Based Activities: Five Seniors’ Intervention Processes. Scand. J. Occup. Ther. 2013, 20, 471–480. [Google Scholar] [CrossRef]
- Rudman, A.; Hutell, D.; Gustavsson, P. Sjuksköterskors Karriärvägar Och Hälsoutveckling de Första Åren Efter Utbildning. Enkät Använd Vid LUST-Projektets Datainsamling för X2004-Kohorten Fem år Efter Examen [In Swedish: Nurses’ Career Paths and Health Development in the First Years after Education. Questionnaire Used in the LUST Project’s Data Collection for the X2004 Cohort Five Years after Graduation]; Karolinska Institutet: Stockholm, Sweden, 2010. [Google Scholar]
- Edwards, K.; Winkel, J. A Method for Effect Modifier Assessment (EMA) in Ergonomic Intervention Research. Appl. Ergon. 2018, 72, 113–120. [Google Scholar] [CrossRef]
- Krueger, R.A.; Casey, M.A. Focus Groups: A Practical Guide for Applied Research, 5th ed.; Sage: Thousand Oaks, CA, USA, 2015. [Google Scholar]
- Neves, B.B.; Franz, R.L.; Munteanu, C.; Baecker, R. Adoption and Feasibility of a Communication App to Enhance Social Connectedness amongst Frail Institutionalized Oldest Old: An Embedded Case Study. Inf. Commun. Soc. 2017, 21, 1681–1699. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- NVivo Software Program, NVivo 1.5.2; QSR International (UK) Limited: London, UK, 2021.
- Dahlberg, L.; McKee, K.J.; Frank, A.; Naseer, M. A Systematic Review of Longitudinal Risk Factors for Loneliness in Older Adults. Aging Ment. Health 2021, 26, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Barreto, M.; Victor, C.; Hammond, C.; Eccles, A.; Richins, M.T.; Qualter, P. Loneliness around the World: Age, Gender, and Cultural Differences in Loneliness. Personal. Individ. Differ. 2020, 169, 110066. [Google Scholar] [CrossRef]
- Marcelino, I.; Laza, R.; Pereira, A. SSN: Senior Social Network for Improving Quality of Life. Int. J. Distrib. Sens. Netw. 2016, 12, 2150734. [Google Scholar] [CrossRef] [Green Version]
- An Overview of Reviews of the Effectiveness of Interventions Affecting Loneliness in People at All Stages of the Life-Course. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42018097293 (accessed on 15 November 2022).
- Morton, T.A.; Wilson, N.; Haslam, C.; Birney, M.; Kingston, R.; McCloskey, L.-G. Activating and Guiding the Engagement of Seniors with Online Social Networking: Experimental Findings from the AGES 2.0 Project. J. Aging Health 2016, 30, 27–51. [Google Scholar] [CrossRef] [PubMed]
- Dahlberg, L.; Agahi, N.; Lennartsson, C. Lonelier than Ever? Loneliness of Older People over Two Decades. Arch. Gerontol. Geriatr. 2018, 75, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Dahlberg, L.; Andersson, L.; McKee, K.J.; Lennartsson, C. Predictors of Loneliness among Older Women and Men in Sweden: A National Longitudinal Study. Aging Ment. Health 2014, 19, 409–417. [Google Scholar] [CrossRef]
- World Medical Association. WMA—The World Medical Association-WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 15 May 2021).

{kind=link}
| Collected Data | Pre-Test | During Test | Post-Test | Data Collection Tools |
|---|---|---|---|---|
| Older adults’ experienced loneliness and social networks. Older adults’ patterns of use, experienced support and information, and navigation and use of the Fik@ room’s functions. Older adults’ expectations of the Fik@ room, its importance in relation to the pandemic, and suggestions for improvement. Researchers’ and social services personnel’s notes on older adults’ need of support. Social services personnel’s experiences of older adults’ use of, and incentives to participate in, the Fik@ room. | X | X | X X X X | UCLA Loneliness Scale Social network questionnaire Evaluation questionnaire Evaluation questionnaire Logbooks Workshops |
| Variables | |
|---|---|
| Older adults (women/men) | 20 (18/2) |
| Age, Md (range) | 77 (63–93) |
| Highest level of education | |
| University/College, n (%) | 9 (45) |
| Vocational school, n (%) | 3 (15) |
| Secondary school, n (%) | 2 (10) |
| Elementary school, n (%) | 6 (30) |
| Household | |
| Living alone, n (%) | 14 (70) |
| Cohabiting with partner, n (%) | 5 (25) |
| Nursing home, n (%) | 1 (5) |
| Experience with digital technology | |
| Computer/Laptop, n (%) | 7 (35) |
| Tablet, n (%) | 7 (35) |
| Smartphone, n (%) | 14 (70) |
| Social media, n (%) | 10 (50) |
| Digital assistant, n (%) | 7 (35) |
| Questionnaire and Variables (Min–Max) | Md (q1–q3) at Pretest | Md (q1–q3) at Posttest | p Value * |
|---|---|---|---|
| UCLA Loneliness Scale (20–80) | 46.5 (32.5–52.25) | 47.5 (37.25–51.75) | 0.352 |
| Evaluation questionnaire | |||
| The Fik@ room contains functions that are valuable in reducing my experience of loneliness. (1–5) | NA | 3 (2.25–4) | NA |
| The Fik@ room contains functions that are valuable in increasing my social network. (1–5) The bulletin board has an important function in the Fik@ room to reduce my experience of loneliness. (1–5) | NA NA | 3 (1–4.75) 3 (1–4.75) | NA NA |
| The bulletin board has an important function in the Fik@ room to increase my social network. (1–5) | NA | 3 (1–3.75) | NA |
| Social network questionnaire (16–89) | 52 (47.75–55.50) | 54 (47–59) | 0.100 |
| 1. How often do you taken part in social activities with others outside the internet? (1–4) | 2 (1–3) | 2 (2–3) | 0.446 |
| 2. How often do you take part in social activities with others on the internet? (1–4) | 3 (1–3) | 2 (1–3) | 0.953 |
| 3. How satisfied are you with your social activities outside the internet? (1–4) | 3 (2–3) | 3 (2–3) | 0.130 |
| 4. How satisfied are you with your social activities on the internet? (1–4) | 3 (2–3) | 3 (3–3) | 0.672 |
| 5. How many acquaintances, friends, or relatives do you have that … (1–5) a. …you meet or speak with in an ordinary week? b. …can come to your home and feel comfortable at any time (even if you are in the middle of a meal, or if your home is untidy)? c. … have the same interests as you? d. … you can speak with openly without unease? e. … you can count on receiving support from if you get into trouble? | 3 (2–3) 3 (2–3.75) 2 (2–3) 2 (2–3) 3 (3–3) | 3 (2–4) 3 (2–3.75) 2 (2–3) 2 (2–3) 3 (2–3) | 0.592 0.193 0.782 1.000 1.000 |
| 6. How satisfied are you (to what extent are your needs met) with the acquaintances, friends, or relatives that … (1–5) a. … you meet or speak with in an ordinary week? b. … can come to your home and feel comfortable at any time (even if you are in the middle of a meal, or if your home is untidy)? c. … have the same interests as you? d. … you can speak with openly without unease? e. … you can count on receiving support from if you get into trouble? | 3 (3–3) 3 (3–3) 3 (2.25–3) 3 (3–3) 3 (3–4) | 3 (3–3.75) 3 (3–3) 3 (3–3) 3 (3–4) 3 (3–4) | 0.132 1.000 0.157 0.020 0.046 |
| 7. How satisfied are you with your social networks outside the internet? (0–10) | 3 (2.25–3) | 3 (2–3) | 0.593 |
| 8. How satisfied are you with your social networks on the internet? (0–10) 9. Have your social networks changed due to the pandemic outside the internet? (0–10) 10. Have your social networks changed due to the pandemic on the internet? (0–10) | 3 (3–4) 2 (0–3) 5 (3.5–7) | 3 (3–3) 4 (2.25–5) 6 (4.25–8) | 0.632 0.005 0.528 |
| Variables | n |
|---|---|
| Frequency of use | |
| 2–3 times /week | 8 |
| Once/week | 2 |
| Less than once/week | 9 |
| Missing data | 1 |
| Duration of time spent in the Fik@room on each occasion | |
| More than 60 min | 5 |
| 30–60 min | 6 |
| Less than 30 min | 6 |
| Missing data | 3 |
| Preferred type of conversation | |
| Video | 11 |
| Voice | 0 |
| Chat | 1 |
| No preferences | 2 |
| Missing data | 6 |
| Variables—Evaluation Questionnaire (Min–Max) | Md (q1–q3) at Posttest |
|---|---|
| Support and information | |
| I received enough information to get started with the use of the Fik@ room. (1–5) | 4 (3–5) |
| I needed to contact support to be able to log in to the Fik@ room for the first time. (1–5) | 5 (1.25–5) |
| The written instructions on how to use the Fik@ room are a support for me. (1–5) | 3 (1.25–4) |
| The instructional videos on how to use the Fik@ room are a support for me. (1–5) | 2.5 (1–3.75) |
| I need to contact the support to be able to use the Fik@ room. (1–5) | 2.5 (1.25–4) |
| Navigation and use of the functions | |
| It is easy to log in to the Fik@ room. (1–5) | 4 (3–5) |
| It is easy to navigate in the Fik@ room. (1–5) | 4 (3–5) |
| It is easy to “connect to conversations”. (1–5) | 4 (3.25–5) |
| It is easy to “create a new conversation” (Video). (1–5) | 4 (3–5) |
| It is easy to “create a new conversation” (Voice). (1–5) | 4 (1.25–4.75) |
| It is easy to “create a new conversation” (Chat). (1–5) | 4 (1–4) |
| It is easy to “create a new message” on the bulletin board. (1–5) | 1 (1–4) |
| It is easy to reply to others’ messages on the bulletin board. (1–5) | 1 (1–3.75) |
| I have a problem with the sound level/sound quality. (1–5) | 2.5 (1–3) |
| I have a problem with the image quality. (1–5) | 2 (1–2.75) |
| I have a problem using the keyboard. (1–5) | 1 (1–3) |
| In the conversations, everyone has a friendly and respectful tone towards each other. (1–5) | 5 (3.25–5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gusdal, A.K.; Florin, U.; Johansson-Pajala, R.-M.; Eklund, C.; Fritz, J.; von Heideken Wågert, P. Older Adults’ Use of a Research-Based Web Platform for Social Interaction. Healthcare 2023, 11, 408. https://doi.org/10.3390/healthcare11030408
Gusdal AK, Florin U, Johansson-Pajala R-M, Eklund C, Fritz J, von Heideken Wågert P. Older Adults’ Use of a Research-Based Web Platform for Social Interaction. Healthcare. 2023; 11(3):408. https://doi.org/10.3390/healthcare11030408
Chicago/Turabian StyleGusdal, Annelie K., Ulrika Florin, Rose-Marie Johansson-Pajala, Caroline Eklund, Johanna Fritz, and Petra von Heideken Wågert. 2023. "Older Adults’ Use of a Research-Based Web Platform for Social Interaction" Healthcare 11, no. 3: 408. https://doi.org/10.3390/healthcare11030408
APA StyleGusdal, A. K., Florin, U., Johansson-Pajala, R. -M., Eklund, C., Fritz, J., & von Heideken Wågert, P. (2023). Older Adults’ Use of a Research-Based Web Platform for Social Interaction. Healthcare, 11(3), 408. https://doi.org/10.3390/healthcare11030408