
Analgesic Efficacy of Acupuncture on Chronic Pelvic Pain: A Systemic Review and Meta-Analysis Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Types of Studies
2.1.2. Types of Participants
2.1.3. Types of Interventions
2.1.4. Outcome
2.2. Data Sources and Study Selection
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Data Synthesis
3. Results
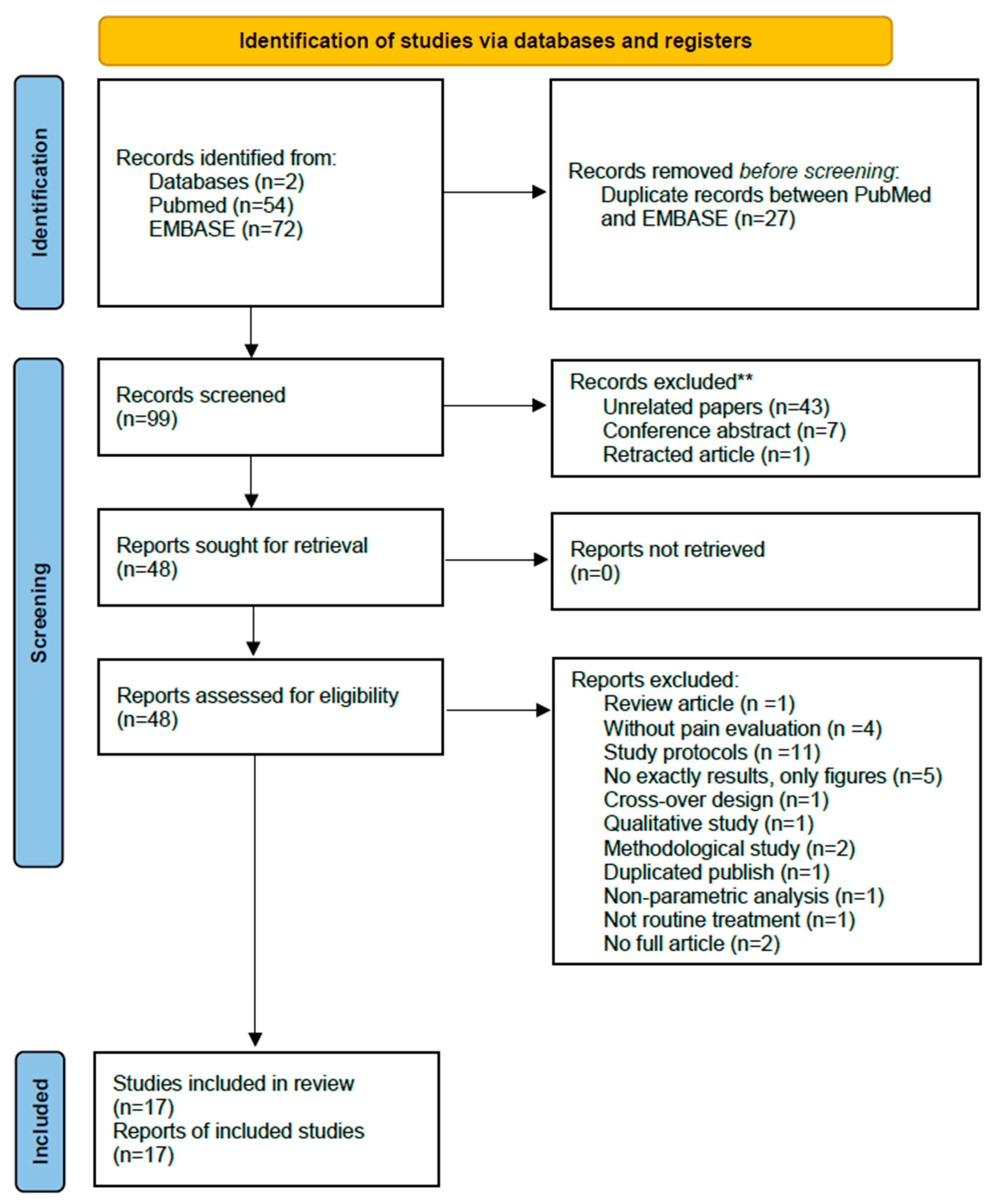
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Patients
3.2.2. Acupuncture Interventions
3.2.3. Controls
3.2.4. Outcome Measures
3.3. Risk of Bias
3.4. Pain Management
3.4.1. Overall Effect
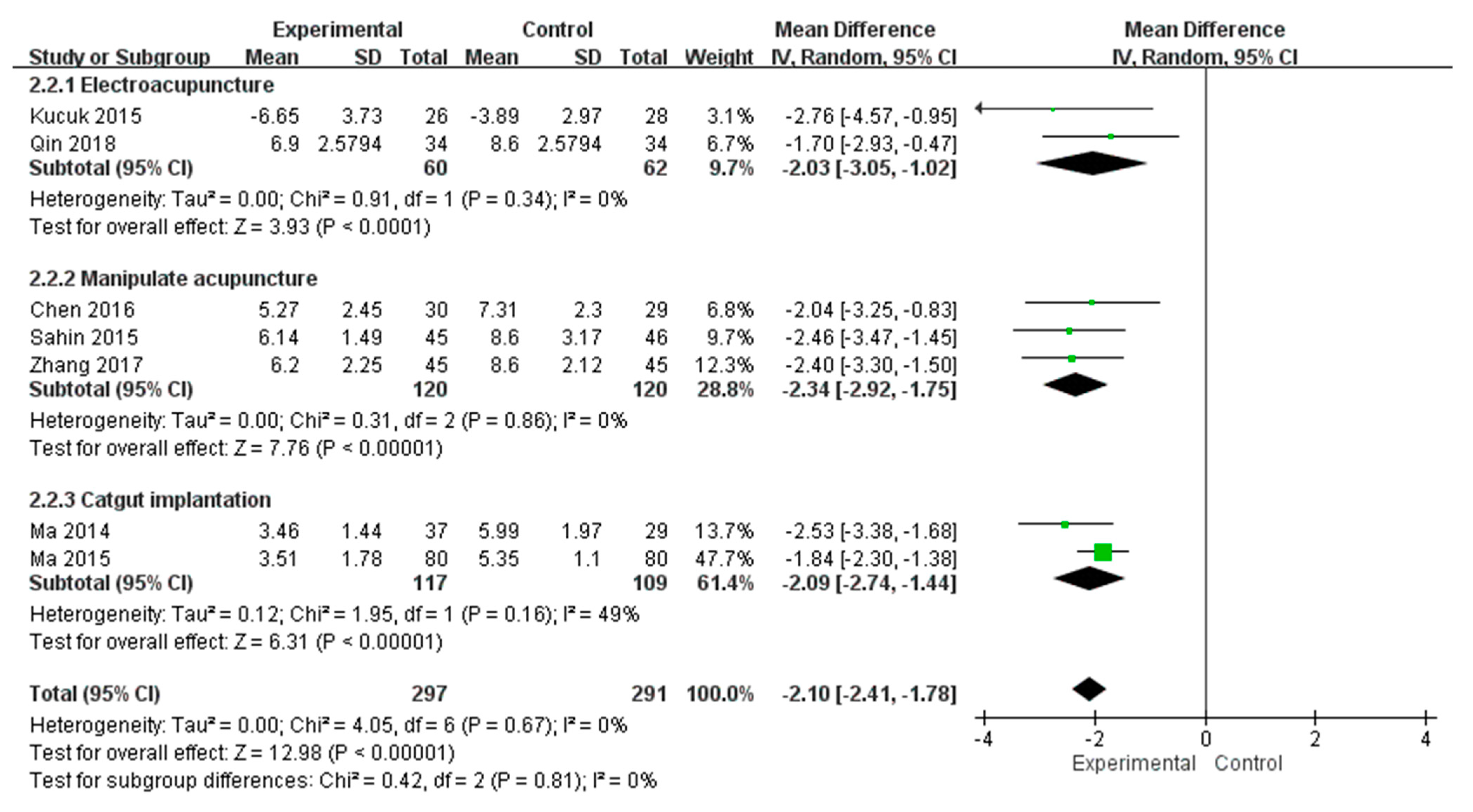
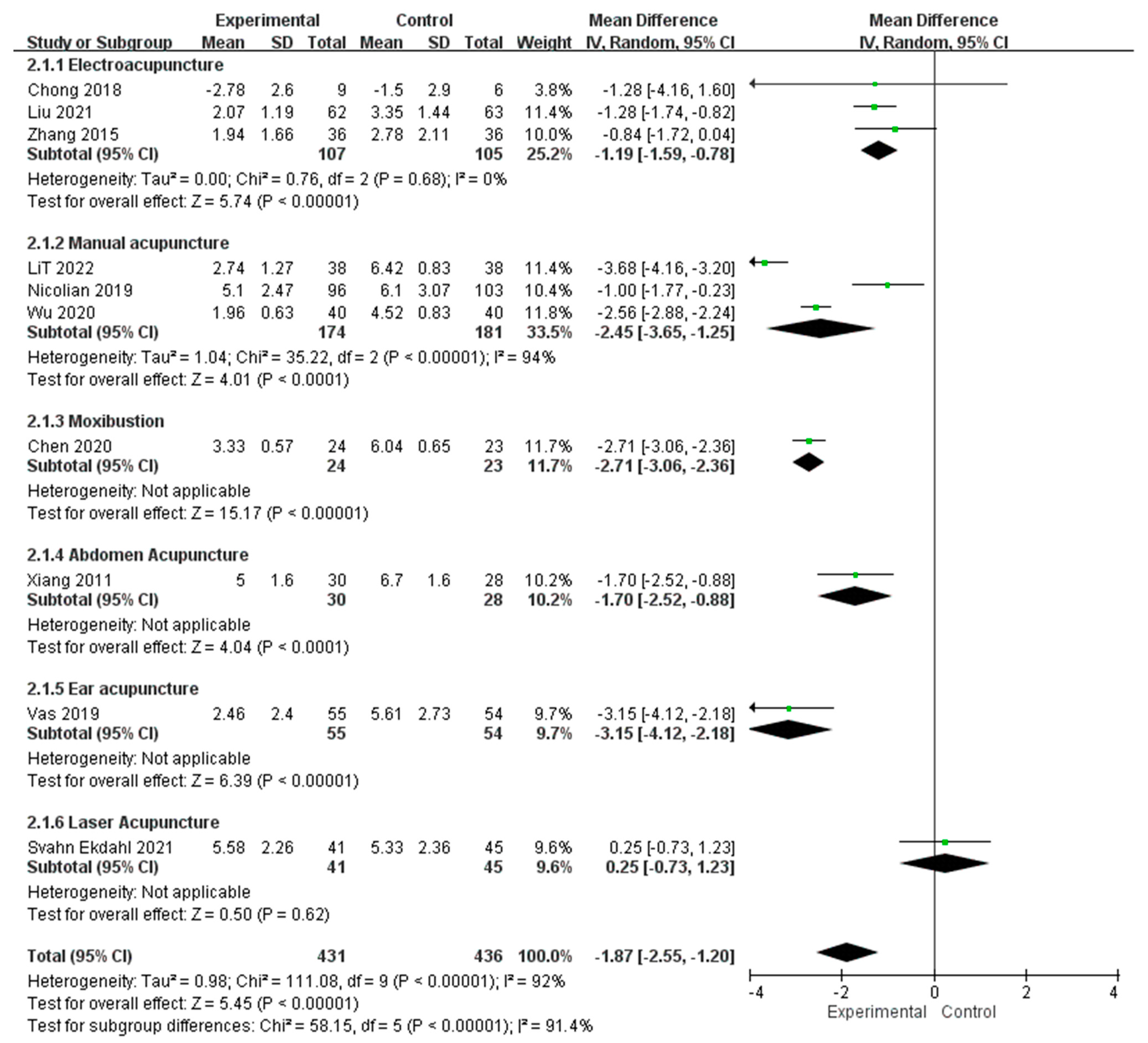
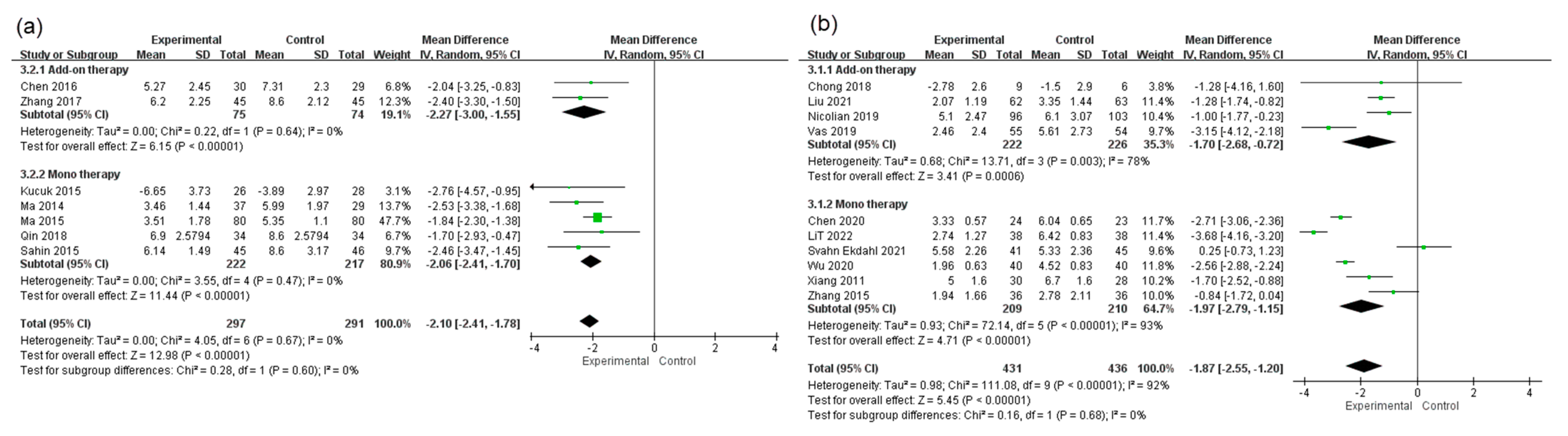
3.4.2. Subgroup Analysis of Acupuncture Interventions
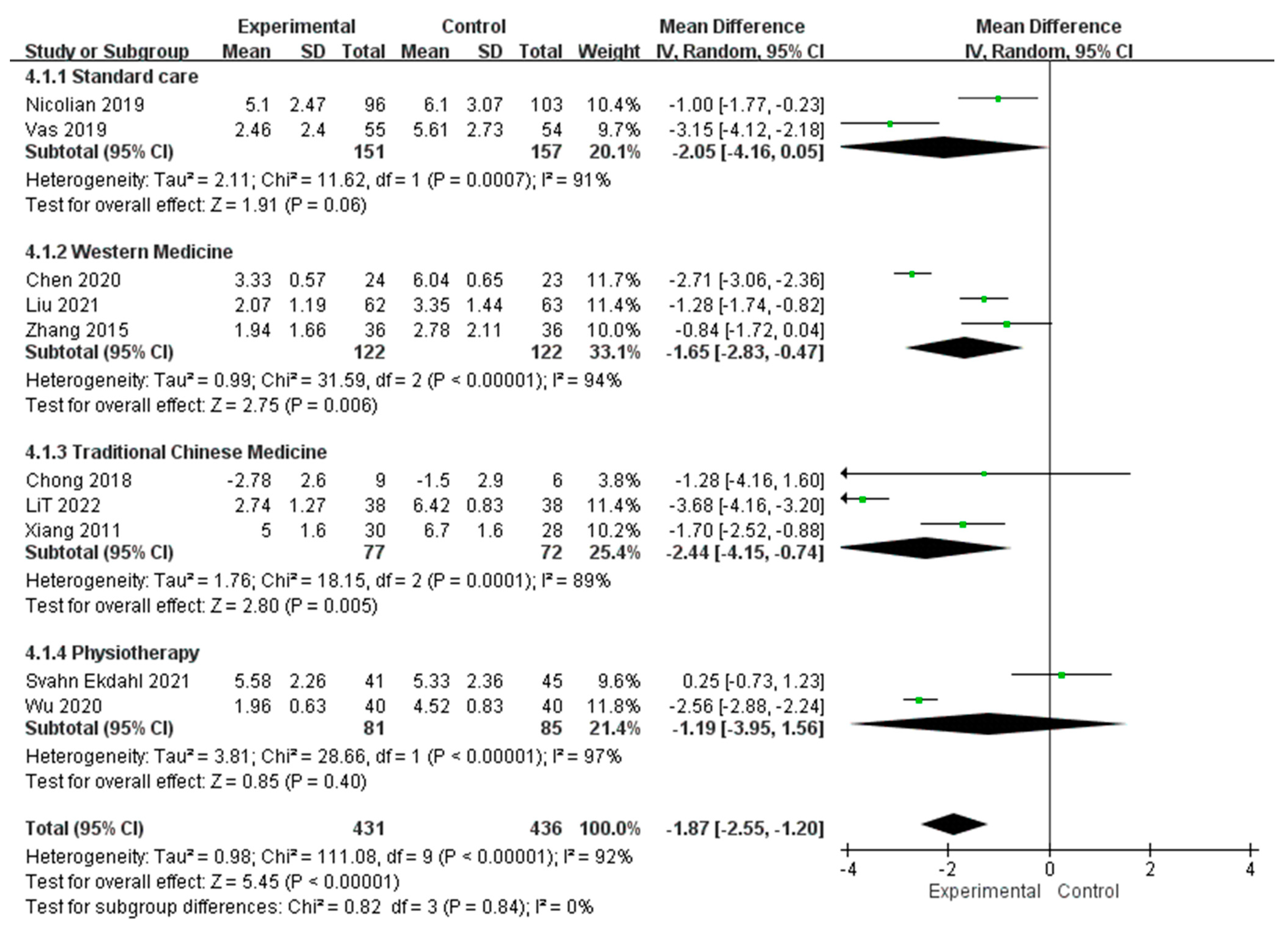
3.4.3. Subgroup Analysis of Control Interventions
3.4.4. Subgroup Analysis of Therapeutic Strategy
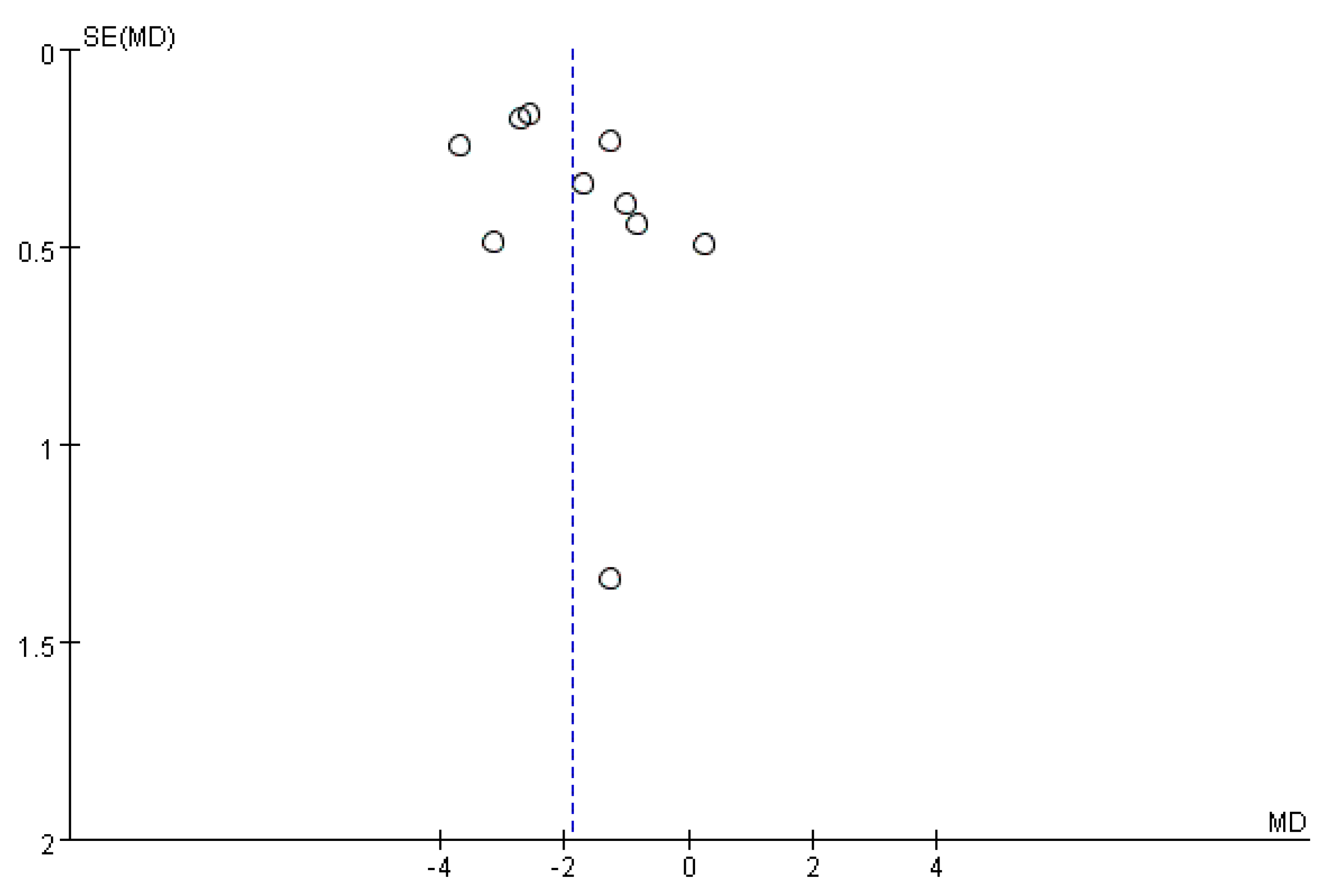
3.4.5. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chronic Pelvic Pain. ACOG Practice Bulletin, Number 218. Obstet. Gynecol. 2020, 135, e98–e109. [CrossRef]
- Latthe, P.; Latthe, M.; Say, L.; Gulmezoglu, M.; Khan, K.S. WHO systematic review of prevalence of chronic pelvic pain: A neglected reproductive health morbidity. BMC Public Health 2006, 6, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sibert, L.; Rigaud, J.; Delavierre, D.; Labat, J.J. Chronic pelvic pain: Epidemiology and economic impact. Prog. Urol. 2010, 20, 872–885. [Google Scholar] [CrossRef] [PubMed]
- Zondervan, K.T.; Yudkin, P.L.; Vessey, M.P.; Dawes, M.G.; Barlow, D.H.; Kennedy, S.H. Prevalence and incidence of chronic pelvic pain in primary care: Evidence from a national general practice database. Br. J. Obstet. Gynaecol. 1999, 106, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Mathias, S.D.; Kuppermann, M.; Liberman, R.F.; Lipschutz, R.C.; Steege, J.F. Chronic pelvic pain: Prevalence, health-related quality of life, and economic correlates. Obstet. Gynecol. 1996, 87, 321–327. [Google Scholar] [CrossRef]
- Leow, H.W.; Szubert, W.; Horne, A.W. 45% of UK gynaecologists think chronic pelvic pain is managed badly. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 224, 200–202. [Google Scholar] [CrossRef]
- Cheong, Y.C.; Smotra, G.; Williams, A.C. Non-surgical interventions for the management of chronic pelvic pain. Cochrane Database Syst. Rev. 2014, 3, CD008797. [Google Scholar] [CrossRef]
- Speer, L.M.; Mushkbar, S.; Erbele, T. Chronic Pelvic Pain in Women. Am. Fam. Physician 2016, 93, 380–387. [Google Scholar]
- Vincent, K.; Evans, E. An update on the management of chronic pelvic pain in women. Anaesthesia 2021, 76 (Suppl. 4), 96–107. [Google Scholar] [CrossRef]
- Lamvu, G.; Carrillo, J.; Ouyang, C.; Rapkin, A. Chronic Pelvic Pain in Women: A Review. JAMA 2021, 325, 2381–2391. [Google Scholar] [CrossRef]
- Grinberg, K.; Sela, Y.; Nissanholtz-Gannot, R. New Insights about Chronic Pelvic Pain Syndrome (CPPS). Int. J. Environ. Res. Public Health 2020, 17, 3005. [Google Scholar] [CrossRef]
- Vickers, A.J.; Cronin, A.M.; Maschino, A.C.; Lewith, G.; MacPherson, H.; Foster, N.E.; Sherman, K.J.; Witt, C.M.; Linde, K.; Acupuncture Trialists, C. Acupuncture for chronic pain: Individual patient data meta-analysis. Arch. Intern. Med. 2012, 172, 1444–1453. [Google Scholar] [CrossRef]
- Vickers, A.J.; Vertosick, E.A.; Lewith, G.; MacPherson, H.; Foster, N.E.; Sherman, K.J.; Irnich, D.; Witt, C.M.; Linde, K.; Acupuncture Trialists, C. Acupuncture for Chronic Pain: Update of an Individual Patient Data Meta-Analysis. J. Pain 2018, 19, 455–474. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Gan, T.J.; Dubose, J.W.; Habib, A.S. Acupuncture and related techniques for postoperative pain: A systematic review of randomized controlled trials. Br. J. Anaesth. 2008, 101, 151–160. [Google Scholar] [CrossRef] [Green Version]
- Yuan, Q.L.; Wang, P.; Liu, L.; Sun, F.; Cai, Y.S.; Wu, W.T.; Ye, M.L.; Ma, J.T.; Xu, B.B.; Zhang, Y.G. Acupuncture for musculoskeletal pain: A meta-analysis and meta-regression of sham-controlled randomized clinical trials. Sci. Rep. 2016, 6, 30675. [Google Scholar] [CrossRef] [Green Version]
- Chiu, H.Y.; Hsieh, Y.J.; Tsai, P.S. Systematic review and meta-analysis of acupuncture to reduce cancer-related pain. Eur. J. Cancer Care 2017, 26, e12457. [Google Scholar] [CrossRef] [PubMed]
- Woo, H.L.; Ji, H.R.; Pak, Y.K.; Lee, H.; Heo, S.J.; Lee, J.M.; Park, K.S. The efficacy and safety of acupuncture in women with primary dysmenorrhea: A systematic review and meta-analysis. Medicine 2018, 97, e11007. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Zhao, W.; Li, T.; Zhao, Y.; Bu, H.; Song, S. Effects of acupuncture for the treatment of endometriosis-related pain: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0186616. [Google Scholar] [CrossRef]
- Yang, Y.; Rao, K.; Zhan, K.; Shen, M.; Zheng, H.; Qin, S.; Wu, H.; Bian, Z.; Huang, S. Clinical evidence of acupuncture and moxibustion for irritable bowel syndrome: A systematic review and meta-analysis of randomized controlled trials. Front. Public Health 2022, 10, 1022145. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.C.; Hsu, C.H.; Hsu, C.K.; Yang, S.S.; Chang, S.J. The efficacy of acupuncture in managing patients with chronic prostatitis/chronic pelvic pain syndrome: A systemic review and meta-analysis. Neurourol. Urodyn. 2017, 36, 474–481. [Google Scholar] [CrossRef]
- MacPherson, H.; Altman, D.G.; Hammerschlag, R.; Youping, L.; Taixiang, W.; White, A.; Moher, D.; Group, S.R. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT statement. PLoS Med. 2010, 7, e1000261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, G.; Xiang, J.; Ouyang, L.; Wang, X.; Zhang, S.; Chen, H.; Chen, J.; Li, T. Acupuncture combined with western medicine for CP/CPPS:a randomized controlled trial. Zhongguo Zhen Jiu = Chin. Acupunct. Moxibustion 2016, 36, 1247–1251. [Google Scholar] [CrossRef]
- Chen, L.F.; Jin, X.F.; Li, B.W.; Zhan, M.J.; Hu, H.T. Herb-separated moxibustion on dysmenorrhea in ovarian endometriosis: A randomized controlled trial. Zhongguo Zhen Jiu = Chin. Acupunct. Moxibustion 2020, 40, 717–720. [Google Scholar] [CrossRef]
- Li, T.; Wang, S.Y.; Huang, Z.Q.; Cai, Q.H.; Zhang, S.; Wang, S.; Tian, T. CO2 laser moxibustion for endometriosis related pelvic pain of cold coagulation and blood stasis: A randomized controlled trial. Zhongguo Zhen Jiu = Chin. Acupunct. Moxibustion 2022, 42, 397–401. [Google Scholar] [CrossRef]
- Liu, Y.H.; Wang, X.; Liang, Z.; Li, H.; Zhang, D.M.; Shi, L. Acupuncture combined with western medication on chronic pelvic pain after pelvic inflammatory disease: A multi-center randomized controlled trial. Zhongguo Zhen Jiu = Chin. Acupunct. Moxibustion 2021, 41, 31–35. [Google Scholar] [CrossRef]
- Ma, Y.; Li, X.; Li, F.; Yu, W.; Wang, Z. Clinical research of chronic pelvic cavity pain syndrome treated with acupoint catgut embedding therapy. Zhongguo Zhen Jiu = Chin. Acupunct. Moxibustion 2015, 35, 561–566. [Google Scholar]
- Ma, Y.; Wang, Z.L.; Sun, Z.X.; Men, B.; Shen, B.Q. Efficacy observation on chronic pelvic pain syndrome of damp-heat stagnation pattern treated with acupoint catgut embedding therapy. Zhongguo Zhen Jiu = Chin. Acupunct. Moxibustion 2014, 34, 351–354. [Google Scholar]
- Wu, J.M.; Zhuo, Y.Y.; Qin, X.L.; Yu, X.Y.; Hu, S.; Ning, Y. Pelvic-sacral tendon-regulation needling technique of acupuncture combined with manipulative reduction in treatment of postpartum pelvic girdle pain: A randomized controlled trial. Zhongguo Zhen Jiu = Chin. Acupunct. Moxibustion 2020, 40, 262–266. [Google Scholar] [CrossRef]
- Xiang, D.F.; Sun, Q.Z.; Liang, X.F. Effect of abdominal acupuncture on pain of pelvic cavity in patients with endometriosis. Zhongguo Zhen Jiu = Chin. Acupunct. Moxibustion 2011, 31, 113–116. [Google Scholar]
- Zhang, X.; Li, W. Efficacy on endometriosis treated with electroacupuncture. Zhongguo Zhen Jiu = Chin. Acupunct. Moxibustion 2015, 35, 323–326. [Google Scholar]
- Zhang, X.Y.; Luo, S.B.; Zhang, J.Y.; Meng, Z.C. Triple acupuncture at the Qugu acupoint as an adjunctive therapy for type-Ⅲ chronic prostatitis: Analysis of short- and long-term clinical effects. Zhonghua Nan Ke Xue = Natl. J. Androl. 2017, 23, 464–467. [Google Scholar]
- Chong, O.T.; Critchley, H.O.D.; Williams, L.J.; Haraldsdottir, E.; Horne, A.W.; Fallon, M. The impact of meridian balance method electro-acupuncture treatment on chronic pelvic pain in women: A three-armed randomised controlled feasibility study using a mixed-methods approach. Br. J. Pain 2018, 12, 238–249. [Google Scholar] [CrossRef] [PubMed]
- Küçük, E.V.; Suçeken, F.Y.; Bindayı, A.; Boylu, U.; Onol, F.F.; Gümüş, E. Effectiveness of acupuncture on chronic prostatitis-chronic pelvic pain syndrome category IIIB patients: A prospective, randomized, nonblinded, clinical trial. Urology 2015, 85, 636–640. [Google Scholar] [CrossRef]
- Nicolian, S.; Butel, T.; Gambotti, L.; Durand, M.; Filipovic-Pierucci, A.; Mallet, A.; Kone, M.; Durand-Zaleski, I.; Dommergues, M. Cost-effectiveness of acupuncture versus standard care for pelvic and low back pain in pregnancy: A randomized controlled trial. PLoS ONE 2019, 14, e0214195. [Google Scholar] [CrossRef] [PubMed]
- Qin, Z.; Zang, Z.; Zhou, K.; Wu, J.; Zhou, J.; Kwong, J.S.W.; Liu, Z. Acupuncture for Chronic Prostatitis/Chronic Pelvic Pain Syndrome: A Randomized, Sham Acupuncture Controlled Trial. J. Urol. 2018, 200, 815–822. [Google Scholar] [CrossRef]
- Sahin, S.; Bicer, M.; Eren, G.A.; Tas, S.; Tugcu, V.; Tasci, A.I.; Cek, M. Acupuncture relieves symptoms in chronic prostatitis/chronic pelvic pain syndrome: A randomized, sham-controlled trial. Prostate Cancer Prostatic Dis. 2015, 18, 249–254. [Google Scholar] [CrossRef]
- Svahn Ekdahl, A.; Fagevik Olsén, M.; Jendman, T.; Gutke, A. Maintenance of physical activity level, functioning and health after non-pharmacological treatment of pelvic girdle pain with either transcutaneous electrical nerve stimulation or acupuncture: A randomised controlled trial. BMJ Open 2021, 11, e046314. [Google Scholar] [CrossRef]
- Vas, J.; Cintado, M.C.; Aranda-Regules, J.M.; Aguilar, I.; Rivas Ruiz, F. Effect of ear acupuncture on pregnancy-related pain in the lower back and posterior pelvic girdle: A multicenter randomized clinical trial. Acta Obstet. Et Gynecol. Scand. 2019, 98, 1307–1317. [Google Scholar] [CrossRef]
- Chen, T.; Zhang, W.W.; Chu, Y.X.; Wang, Y.Q. Acupuncture for Pain Management: Molecular Mechanisms of Action. Am. J. Chin. Med. 2020, 48, 793–811. [Google Scholar] [CrossRef]
- Lee, I.S.; Cheon, S.; Park, J.Y. Central and Peripheral Mechanism of Acupuncture Analgesia on Visceral Pain: A Systematic Review. Evid. Based Complement. Alternat. Med. 2019, 2019, 1304152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.G.; Chen, W.L. Acupuncture analgesia: A review of its mechanisms of actions. Am. J. Chin. Med. 2008, 36, 635–645. [Google Scholar] [CrossRef] [PubMed]
- Witt, C.M.; Pach, D.; Brinkhaus, B.; Wruck, K.; Tag, B.; Mank, S.; Willich, S.N. Safety of acupuncture: Results of a prospective observational study with 229,230 patients and introduction of a medical information and consent form. Forsch. Komplementmed. 2009, 16, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies | Population Type | Sample Size Intervention/Control | Age (Mean) Intervention/Control | Outcomes | Course of Treatment | Follow-Up Visit |
|---|---|---|---|---|---|---|
| Xiang 2011 [30] | Patients with endometriosis | 30/28 | 34.6/34.6 | VAS 4 (0–10) McGill pain questionnaire | 3 months (3 MC 7 cycle) | NA 8 |
| Zhang 2015 [31] | Patients with endometriosis | 36/36 | 33/35 | VAS 4 (0–10) | 6 months | NA 8 |
| Chong 2018 [33] | Women with CPP 1 over 6 months | 9/6 | 34.7/31.4 | NRS 5 (0–10) | 4 weeks | 12th week |
| Nicolian 2019 [35] | Pregnant women with pelvic girdle and low back pain | 96/103 | 31/30.7 | NRS 5 (0–10) | 4 weeks | NA 8 |
| Vas 2019 [39] | Pregnant women at 24–36 weeks of gestation with pregnancy-related lower back and/or posterior pelvic girdle pain | 55/54 | 31.4/31.7 | VAS 4 (0–100) | 2 weeks | 3 months postpartum, and 1 year after randomization |
| Chen 2020 [24] | Patients with ovarian endometriosis dysmenorrhea | 24/23 | 33/32 | VAS 4 (0–10) | 3 months | NA 8 |
| Wu 2020 [29] | Patients with postpartum pelvic girdle pain | 40/40 | 28/28 | VAS 4 (0–10) | 3 weeks | NA 8 |
| Liu 2021 [26] | CPP 1 patients with sequelae of pelvic inflammatory disease | 62/63 | 35/36 | VAS 4 (0–10) Lower abdomen | 3 months (3 MC cycles) | NA 8 |
| Svahn Ekdahl 2021 [38] | Patients with pelvic girdle pain 12–48 weeks | 41/45 | 30.5/31.1 | VAS 4 (0–10) | 5 weeks | NA 8 |
| Li 2022 [25] | Endometriosis related pelvic pain of cold coagulation and blood stasis. | 38/38 | 33/37 | VAS 4 (0–10) | 4 weeks | 3-month after treatment |
| Ma 2014 [28] | Patients with CP/CPPS 2 (NIH 3 category IIIB) | 37/29 | 31/33 | NIH-CPSI 6 score Pain (0–21) | 8 weeks | NA 8 |
| Kucuk 2015 [34] | Patients with CP/CPPS 2 | 26/28 | All subjects’ mean: 33.3 | NIH-CPSI 6 pain total score (0–21) | 7 weeks | NA 8 |
| Ma 2015 [27] | Patients with CP/CPPS 2 (NIH 3 category IIIB) | 80/80 | 35/33 | NIH-CPSI 6 score Pain (0–21) | 8 weeks | NA 8 |
| Sahin 2015 [37] | Patients with CP/CPPS 2 (NIH 3 category IIIB) | 45/46 | 32.1/32.8 | NIH-CPSI 6 pain score (0–21) | 6 weeks | At 8th, 16th, and 24th week |
| Chen 2016 [23] | Patients with CP/CPPS 2 | 30/29 | 34/34 | NIH-CPSI 6 Pain total score (0–21) | 24 days | NA 8 |
| Zhang 2017 [32] | Patients with CP/CPPS 2 (NIH 3 category IIIB) | 45/45 | All subjects’ mean: 30.6 | NIH-CPSI 6 Pain total score (0–21) | 4 weeks | NA 8 |
| Qin 2018 [36] | Patients with CP/CPPS | 34/34 | 33.8/35.1 | NIH-CPSI 6 Pain total score (0–21) | 8 weeks | 32 weeks |
| Studies | Intervention | Treatment Schedule | |
|---|---|---|---|
| Acupuncture Group | Control Group | ||
| Xiang 2011 [30] | Abdominal acupuncture Acupoint: CV12, CV10, CV6…etc. | Chinese Medicine: Tianqi Tongjing Capsule | For 3 MC cycle, once each 1~2 days, at least 3 time each MC cycle |
| Zhang 2015 [31] | Electro-acupuncture Acupoints: CV6, CV4, CV3, EXCA1, SP8, SP6, LI4, LR3. EA on CV4 and CV3 | Mifeprisone tablet 12.5 mg once a day for 6 months | once every 2 days for 6 months, suspend treatment during menstruation |
| Chong 2018 [33] | BMEA treatment (BMEA + TCM HC) Acupoints: the most painful Ashi points (tight and tender points) with electrical stimulation | TCM HC interventions twice a week for 4 weeks | Twice a week for 4 weeks |
| Nicolian 2019 [35] | Acupuncture plus standard care Acupoints: Bilateral BL40 and Ashi points | Standard care: pregnancy belt, lifestyle recommendations, and exercises | Twice in first week, then once per week in next 3 weeks. 5 sessions. |
| Vas 2019 [39] | Standard obstetric care plus ear acupuncture | Standard obstetric care | 2 weeks |
| Chen 2020 [24] | Herb-separated moxibustion was applied at hypogastrium and lumbosacral area for 30 min | Giving ibuprofen sustained-release capsule when necessary | Once a week for 3 months |
| Wu 2020 [29] | Acupuncture plus manipulative reduction Acupoints: GV4, BL25, GV3, BL32, BL33, GB30, and GB34 | Manipulative reduction | once every two days, three times a week and 3 treatments taken as one course. In total, 3 courses of treatment were required (3 weeks) |
| Liu 2021 [26] | Electro-acupuncture Acupoints: CV4, ST28, ST29, BL23, and BL32 Disperse-dense wave, 2 Hz/15 Hz of frequency for 30 min | Ibuprofen sustained-release capsules 10 days before menstruation, 0.3 g each time, once a day per menstrual cycle for 3 menstrual cycles | once a day, 10 days per menstrual cycle, for 3 menstrual cycles |
| Svahn Ekdahl 2021 [38] | Manual acupuncture Acupoint: GV 20, bil LI 4, bil BL 26, bil BL 32, bil BL 33, bil BL 54, bil KI 11, bil BL 60, bil EX 21, bil GB 30, bil SP 12, bil ST 36 | TENS device at home. Treatment area: unilaterally or bilaterally over the sacroiliac joint and gluteal muscles for dorsal pelvic pain or in the groin area for pubic pain. Intensity: High frequency stimulation (80 Hz) | Acupuncture: 10 acupuncture sessions (two sessions per week) TENS: At least 30 min per day for 5 weeks. |
| Li 2022 [25] | CO2 laser acupuncture (100 mW, area 2 cm, distance to skin 3 cm) Acupoint: bil Zigong (EX-CA 1) | Sham laser acupuncture (0 mW, area 2 cm, distance to skin 3 cm) Acupoint: bil Zigong (EX-CA 1) | Once every other day, 30 min each time, 3 times a week for 4 weeks. |
| Ma 2014 [28] | Catgut embedding acupuncture Acupoints: SP6, CV1, LI11, ST36, CV3, and BL23 | Tamsulosin hydrochloride, 0.2 mg, once daily Indomethacin, 75 mg, once daily | Once each 2-week for 8 weeks |
| Kucuk 2015 [34] | Electro-acupuncture Acupoints: UB28, GB41, LIV3, LI4, SP6, and SP8 | Levofloxacin 500 mg once daily and ibuprofen 200 mg twice daily for 6 weeks | Twice a week for 7 weeks |
| Ma 2015 [27] | Catgut embedding acupuncture Acupoints: SP 6, CV 1, CV 2, BL 54, and BL 23 | Tamsulosin hydrochloride 0.2 mg once daily Indomethacin 75 mg three times daily | Once every two weeks; the treatment of 4 weeks made one session, and two sessions were required. |
| Sahin 2015 [37] | Acupuncture Acupoints: Bilateral BL33, BL34, BL54, CV1, CV4, SP6, and SP9 | Sham acupuncture Acupoints: 1 cm left of each selected acupoint bilaterally (BL33, BL34, BL54, CV1, CV4, SP6 and SP9) | The acupuncture needles were lasted for 20 min in both groups and half of this period covered by needle stimulation through rotation. The procedure was repeated every week for a period 6 week |
| Chen 2016 [23] | Manual acupuncture plus western medicine Scalp points GV24, GV22, GV21, GV20, BL6, BL7. Body points: CV3, CV4, BL28, and BL32 | Levofloxacin 200 mg twice daily Tamsulosin hydrochloride 0.2 mg once daily | Once a day, 12 days treatments as one session and total 2 session were given. |
| Zhang 2017 [32] | Triple acupuncture at the Qugu (RN2) acupoint 20 min, twice a week plus Levofloxacin Mesylate Tablets 0.5 g three times daily, and Terazosin Hydrochloride Capsules 2 mg once daily for 4 weeks | Levofloxacin Mesylate Tablets 0.5 g three times daily, and Terazosin Hydrochloride Capsules 2 mg once daily for 4 weeks | Twice a week for 4 weeks |
| Qin 2018 [36] | Manual acupuncture Acupoints: Bilateral BL33, BL23, SP6, and BL35 | Sham non-penetration acupuncture Same procedure as Verum acupuncture groups with placebo needles | 3 treatment sessions per week for 8 consecutive weeks for a total of 24 sessions |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, K.Y.-H.; Chang, Y.-C.; Lu, W.-C.; Kotha, P.; Chen, Y.-H.; Tu, C.-H. Analgesic Efficacy of Acupuncture on Chronic Pelvic Pain: A Systemic Review and Meta-Analysis Study. Healthcare 2023, 11, 830. https://doi.org/10.3390/healthcare11060830
Lin KY-H, Chang Y-C, Lu W-C, Kotha P, Chen Y-H, Tu C-H. Analgesic Efficacy of Acupuncture on Chronic Pelvic Pain: A Systemic Review and Meta-Analysis Study. Healthcare. 2023; 11(6):830. https://doi.org/10.3390/healthcare11060830
Chicago/Turabian StyleLin, Kent Yu-Hsien, Yi-Chuan Chang, Wen-Chi Lu, Peddanna Kotha, Yi-Hung Chen, and Cheng-Hao Tu. 2023. "Analgesic Efficacy of Acupuncture on Chronic Pelvic Pain: A Systemic Review and Meta-Analysis Study" Healthcare 11, no. 6: 830. https://doi.org/10.3390/healthcare11060830
APA StyleLin, K. Y. -H., Chang, Y. -C., Lu, W. -C., Kotha, P., Chen, Y. -H., & Tu, C. -H. (2023). Analgesic Efficacy of Acupuncture on Chronic Pelvic Pain: A Systemic Review and Meta-Analysis Study. Healthcare, 11(6), 830. https://doi.org/10.3390/healthcare11060830