
Assessment of Psychometric Properties of the Malay Version of the Brief Resilience Scale (BRS-M) among Non-Academic Staff Working from Home during COVID-19 in Malaysia

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
- 18 years old and above;
- Consented to participate in the study;
- Non-academic staff (defined as non-teaching or administrative staff appointed by the university);
- Able to understand Malay language, as all the questionnaires were in Malay.
2.2. Instruments
2.2.1. Sociodemographic Questionnaire
2.2.2. Brief Resilience Scale (BRS) and the Malay Version of the Brief Resilience Scale (BRS-M)
2.2.3. Malay Version of Copenhagen Burnout Inventory (CBI-M)
2.2.4. Malay Version of Depression, Anxiety, Stress Scale-21 (M-DASS-21)
2.3. Statistical Analyses
3. Results
3.1. Exploratory Factor Analysis (EFA)
3.2. Concurrent (Criterion) Validity of BRS-M
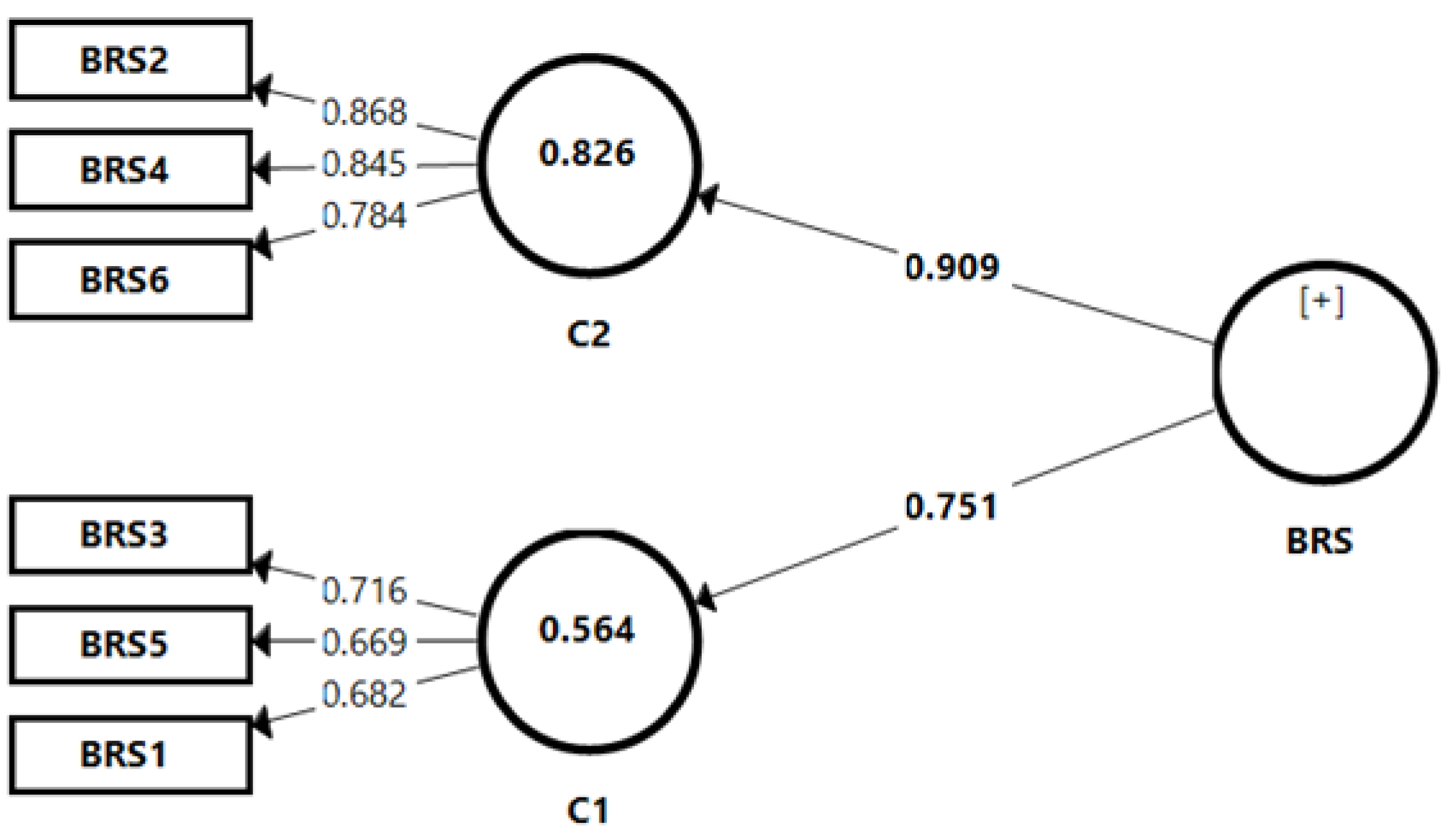
3.3. Confirmatory Factor Analysis (CFA)
3.4. Resilience Level among Non-Academic Staff
3.5. Univariable and Multivariable Analysis on Factors Associated with BRS-M
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suárez, V.J.; Martínez-González, M.B.; Benitez-Agudelo, J.C.; Navarro-Jiménez, E.; Beltran-Velasco, A.I.; Ruisoto, P.; Diaz Arroyo, E.; Laborde-Cárdenas, C.C.; Tornero-Aguilera, J.F. The Impact of the COVID-19 Pandemic on Mental Disorders. A Critical Review. Int. J. Environ. Res. Public Health 2021, 18, 10041. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.H.D. Movement control as an effective measure against Covid-19 spread in Malaysia: An overview. J. Public Health 2022, 30, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Bick, A.; Blandin, A.; Mertens, K. Work from Home after the COVID-19 Outbreak; Federal Reserve Bank of Dallas, Research Department: Dallas, TX, USA, 2020. [Google Scholar]
- Lucey, C.R.; Johnston, S.C. The transformational effects of COVID-19 on medical education. JAMA 2020, 324, 1033–1034. [Google Scholar] [CrossRef]
- Alwi, N.H.; Osman, Z.; Ismail, Z.; Khan, B.N.A. Higher Educations Employees Work From Home Productivity during The COVID-19 Outbreak: The Role Of Motivation As Mediator. Asian J. Manag. Entrep. Soc. Sci. 2022, 2, 17–35. [Google Scholar]
- Shockley, K.M.; Allen, T.D. Motives for flexible work arrangement use. Community Work. Fam. 2012, 15, 217–231. [Google Scholar] [CrossRef]
- Salim, N.; Chan, W.H.; Mansor, S.; Nazira Bazin, N.E.; Amaran, S.; Mohd Faudzi, A.A.; Zainal, A.; Huspi, S.H.; Jiun Hooi, E.K.; Shithil, S.M. COVID-19 epidemic in Malaysia: Impact of lockdown on infection dynamics. medrxiv 2020. [Google Scholar] [CrossRef]
- Tull, M.T.; Edmonds, K.A.; Scamaldo, K.M.; Richmond, J.R.; Rose, J.P.; Gratz, K.L. Psychological outcomes associated with stay-at-home orders and the perceived impact of COVID-19 on daily life. Psychiatry Res. 2020, 289, 113098. [Google Scholar] [CrossRef]
- Chen, Z. Influence of Working From Home During the COVID-19 Crisis and HR Practitioner Response. Front. Psychol. 2021, 12, 710517. [Google Scholar] [CrossRef] [PubMed]
- Dockery, M.; Bawa, S. Working from Home in the COVID-19 Lockdown; Bankwest Curtin Economics Centre: Bentley, WA, USA, 2020. [Google Scholar]
- Windle, G.; Bennett, K.M.; Noyes, J. A methodological review of resilience measurement scales. Health Qual. Life Outcomes 2011, 9, 8. [Google Scholar] [CrossRef]
- Zabaniotou, A. A systemic approach to resilience and ecological sustainability during the COVID-19 pandemic: Human, societal, and ecological health as a system-wide emergent property in the Anthropocene. Glob. Transit. 2020, 2, 116–126. [Google Scholar] [CrossRef]
- Manning, L.; Ferris, M.; Rosario, C.N.; Prues, M.; Bouchard, L. Spiritual resilience: Understanding the protection and promotion of well-being in the later life. J. Relig. Spirit. Aging 2019, 31, 168–186. [Google Scholar] [CrossRef]
- Pietrzak, R.H.; Southwick, S.M. Psychological resilience in OEF–OIF Veterans: Application of a novel classification approach and examination of demographic and psychosocial correlates. J. Affect. Disord. 2011, 133, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Salata, K.-D.; Yiannakou, A. The Quest for Adaptation through Spatial Planning and Ecosystem-Based Tools in Resilience Strategies. Sustainability 2020, 12, 5548. [Google Scholar] [CrossRef]
- Friedli, L.; WHO Regional Office for Europe. Mental Health, Resilience and Inequalities; WHO Regional Office for Europe: Copenhagen, Denmark, 2009. [Google Scholar]
- Holling, C.S. Resilience and Stability of Ecological Systems. Annu. Rev. Ecol. Syst. 1973, 4, 1–23. [Google Scholar] [CrossRef]
- Wake, L. Neurolinguistic Psychotherapy: A Postmodern Perspective, 1st ed.; Routledge: London, UK, 2008. [Google Scholar]
- Werner, E.E.; Smith, R.S. Overcoming the Odds: High Risk Children from Birth to Adulthood; Cornell University Press: Ithaca, NY, USA, 1992. [Google Scholar]
- Namok, C.; Stephen, M.L.; Hart, J.M.; Hongryun, W. Further Validation of the Brief Resilience Scale from a Korean College Sample. J. Asia Pac. Couns. 2019, 9, 39–56. [Google Scholar]
- Fung, S.-f. Validity of the Brief Resilience Scale and Brief Resilient Coping Scale in a Chinese Sample. Int. J. Environ. Res. Public Health 2020, 17, 1265. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rey, R.; Alonso-Tapia, J.; Hernansaiz-Garrido, H. Reliability and validity of the Brief Resilience Scale (BRS) Spanish Version. Psychol. Assess. 2016, 28, e101–e110. [Google Scholar] [CrossRef] [PubMed]
- Haktanir, A.; Lenz, A.; Can, N.; Watson, J. Development and Evaluation of Turkish Language Versions of three Positive Psychology Assessments. Int. J. Adv. Couns. 2016, 38, 286–297. [Google Scholar] [CrossRef]
- Amat, S.; Subhan, M.; Jaafar, W.M.W.; Mahmud, Z.; Johari, K.S.K. Evaluation and Psychometric Status of the Brief Resilience Scale in a Sample of Malaysian International Students. Asian Soc. Sci. 2014, 10, 240–245. [Google Scholar] [CrossRef]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best practices for developing and validating scales for health, social, and behavioral research: A primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef]
- Zou, G.; Shen, X.; Tian, X.; Liu, C.; Li, G.; Kong, L.; Li, P. Correlates of psychological distress, burnout, and resilience among Chinese female nurses. Ind. Health 2016, 54, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Campbell-Sills, L.; Forde, D.R.; Stein, M.B. Demographic and childhood environmental predictors of resilience in a community sample. J. Psychiatr. Res. 2009, 43, 1007–1012. [Google Scholar] [CrossRef] [PubMed]
- Beutel, M.E.; Glaesmer, H.; Decker, O.; Fischbeck, S.; Brähler, E. Life satisfaction, distress, and resiliency across the life span of women. Menopause 2009, 16, 1132–1138. [Google Scholar] [CrossRef]
- Tsang, S.; Royse, C.F.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J. Anaesth. 2017, 11 (Suppl. S1), S80–S89. [Google Scholar] [CrossRef]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- Nunnally, J.; Bernstein, I. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- DOSM. Pendapatan Dan Perbelanjaan Isi Rumah M40 Dan B40 Mengikut NegerI; Department of Statistics: Putrajaya, Malaysia, 2020. [Google Scholar]
- Smith, B.W.; Epstein, E.M.; Ortiz, J.A.; Christopher, P.J.; Tooley, E.M. The foundations of resilience: What are the critical resources for bouncing back from stress? Resil. Child. Adolesc. Adults Transl. Res. Pract. 2013, 167–187. [Google Scholar] [CrossRef]
- Kristensen, T.; Borritz, M.; Villadsen, E.; Christensen, K. The Copenhagen Burnout Inventory: A new tool for the assessment of burnout. Work. Stress 2005, 19, 192–207. [Google Scholar] [CrossRef]
- Andrew Chin, R.W.; Chua, Y.Y.; Chu, M.N.; Mahadi, N.F.; Wong, M.S.; Yusoff, M.S.B.; Lee, Y.Y. Investigating validity evidence of the Malay translation of the Copenhagen Burnout Inventory. J. Taibah Univ. Med. Sci. 2017, 13, 1–9. [Google Scholar] [CrossRef]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychol. Assess. 1998, 10, 176–181. [Google Scholar] [CrossRef]
- Musa, R.; Fadzil, M.A.; Zain, Z. Translation, validation and psychometric properties of Bahasa Malaysia version of the Depression, Anxiety and Stress Scale (DASS). ASEAN J. Psychiatry 2007, 8, 82–89. [Google Scholar]
- Kim, H.Y. Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo-Seva, U.; Ferrando, P.J. FACTOR: A computer program to fit the exploratory factor analysis model. Behav. Res. Methods 2006, 38, 88–91. [Google Scholar] [CrossRef]
- Horn, J.L. A Rationale and Test for the Number of Factors in Factor Analysis. Psychometrika 1965, 30, 179–185. [Google Scholar] [CrossRef]
- Ringle, C.M. SmartPLS 2.0 (M3). 2005. Available online: http://www.smartpls.de (accessed on 25 October 2021).
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Werts, C.E.; Linn, R.L.; Jöreskog, K.G. Intraclass Reliability Estimates: Testing Structural Assumptions. Educ. Psychol. Meas. 1974, 34, 25–33. [Google Scholar] [CrossRef]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); SAGE Publications, Incorporated: Thousand Oaks, CA, USA, 2021. [Google Scholar]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238. [Google Scholar] [CrossRef]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Streiner, D.L. Figuring out factors: The use and misuse of factor analysis. Can. J. Psychiatry 1994, 39, 135–140. [Google Scholar] [CrossRef]
- Hu, L.-t.; Bentler, P.M. Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychol. Methods 1998, 3, 424. [Google Scholar] [CrossRef]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; Guilford Publications: London, UK, 2015. [Google Scholar]
- Kyriazos, T.; Stalikas, A.; Prassa, K.; Galanakis, M.; Yotsidi, V.; Lakioti, A. Psychometric Evidence of the Brief Resilience Scale (BRS) and Modeling Distinctiveness of Resilience from Depression and Stress. Psychology 2018, 9, 1828–1857. [Google Scholar] [CrossRef]
- Konaszewski, K.; Niesiobędzka, M.; Surzykiewicz, J. Validation of the Polish version of the Brief Resilience Scale (BRS). PLoS ONE 2020, 15, e0237038. [Google Scholar] [CrossRef] [PubMed]
- Macovei, C.M. The Brief Resilience Scale—A Romanian-Language Adaptation; Land Forces Academy: Sibiu, Roman, 2015. [Google Scholar]
- Dunn, T.J.; Baguley, T.; Brunsden, V. From alpha to omega: A practical solution to the pervasive problem of internal consistency estimation. Br. J. Psychol. 2014, 105, 399–412. [Google Scholar] [CrossRef] [PubMed]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Brunner, M.; Süβ, H.-M. Analyzing the reliability of multidimensional measures: An example from intelligence research. Educ. Psychol. Meas. 2005, 65, 227–240. [Google Scholar] [CrossRef]
- Clark, L.A.; Watson, D. Constructing Validity: Basic Issues in Objective Scale Development. In Methodological Issues and Strategies in Clinical Research; Kazdin, A.E., Ed.; American Psychological Association: Washington, DC, USA; pp. 187–203. [CrossRef]
- MacCallum, R.; Browne, M.; Sugawara, H.; Modeling, P. Power Analysis and Determination of Sample Size for Covariance Structure Modeling. Psychol. Methods 1996, 1, 130–149. [Google Scholar] [CrossRef]


{kind=link}
| Items | Factors | |
|---|---|---|
| 1 Succumbing | 2 Resilience | |
| Item 2 I have a hard time making it through stressful events. Saya mempunyai kesukaran untuk mengharungi peristiwa yang menekankan. | 0.954 | |
| Item 4 It is hard for me to snap back when something bad happens. Sukar untuk saya kembali kepada keadaan sediakala apabila sesuatu yang buruk berlaku. | 0.842 | |
| Item 6 I tend to take a long time to get over setbacks in my life. Saya cenderung untuk mengambil masa yang lama untuk mengatasi halangan-halangan di dalam hidup saya. | 0.795 | |
| Item 1 I tend to bounce back quickly after hard times. Saya cenderung untuk bangkit kembali dengan kadar segera setelah melalui sesuatu tempoh yang sukar. | 0.975 | |
| Item 3 It does not take me long to recover from a stressful event. Ianya tidak memerlukan saya masa yang lama untuk pulih daripada peristiwa yang menekankan. | 0.525 | |
| Item 5 I usually come through difficult times with little trouble. Saya hampir tiada masalah apabila menghadapi situasi yang sukar. | 0.622 | |
| Eigenvalues | 3.113 | 1.166 |
| % of Variance | 51.88 | 19.43 |
| Cronbach’s α | 0.911 | 0.878 |
| Scales | BRS-M | |
|---|---|---|
| CBI-M | Personal | −0.449 ** |
| Work-related | −0.462 ** | |
| Client-related | −0.373 ** | |
| M-DASS 21 | Depression | −0.530 ** |
| Anxiety | −0.416 ** | |
| Stress | −0.492 ** | |
| Constructs | Item | Outer Loading | Cronbach’s Alpha | Composite Reliability | Average Variance Extracted |
|---|---|---|---|---|---|
| Resilience C1 | BRS3 BRS5 BRS1 | 0.716 0.669 0.682 | 0.448 | 0.731 | 0.475 |
| Succumbing C2 | BRS2 BRS4 BRS6 | 0.868 0.845 0.784 | 0.778 | 0.872 | 0.694 |
| Variables | N (%) | Succumbing | Resilience | BRS-M Total Score | |||
|---|---|---|---|---|---|---|---|
| Mean (SD) | F/t Statistics (p-Value) | Mean (SD) | F/t Statistics (p-Value) | Mean (SD) | F/t Statistics (p-Value) | ||
| Age group | |||||||
| 18–35 36–45 46–60 | 110 (36.9) 123 (41.3) 65 (21.8) | 3.25 (0.89) 3.45 (0.85) 3.37 (0.77) | F = 1.644 (0.195) | 3.39 (0.70) 3.43 (0.67) 3.57 (0.65) | F = 1.500 (0.225) | 3.32 (0.70) 3.44 (0.67) 3.47 (0.51) | F = 1.481 (0.230) |
| Gender | |||||||
| Male Female | 44 (14.8) 254 (85.2) | 3.28 (0.86) 3.37 (0.85) | t = −0.658 (0.511) | 3.48 (0.63) 3.44 (0.69) | t = 0.323 (0.747) | 3.38 (0.63) 3.41 (0.65) | t = −0.261 (0.794) |
| Race | |||||||
| Malay Chinese/Indian/ Others | 268 (89.9) 30 (10.1) | 3.36 (0.85) 3.36 (0.88) | t = 0.016 (0.987) | 3.45 (0.66) 3.42 (0.81) | t = 0.233 (0.816) | 3.41 (0.64) 3.39 (0.71) | t = 0.133 (0.895) |
| Marital status | |||||||
| Single Married | 68 (22.8) 230 (77.2) | 3.15 (0.87) 3.42 (0.84) | t = −2.294 (0.023) * | 3.30 (0.80) 3.49 (0.63) | t = −1.843 (0.068) | 3.22 (0.74) 3.46 (0.61) | t = −2.604 (0.010) * |
| Education level | |||||||
| Secondary school Diploma Degree | 78 (26.2) 97 (32.6) 123 (41.3) | 3.24 (0.85) 3.47 (0.85) 3.35 (0.85) | F = 1.699 (0.185) | 3.50 (0.59) 3.36 (0.63) 3.49 (0.76) | F = 1.212 (0.299) | 3.37 (0.56) 3.42 (0.63) 3.42 (0.72) | F = 0.207 (0.813) |
| Household income # | |||||||
| B40 M40 T20 | 131 (44.0) 140 (47.0) 27 (9.1) | 3.27 (0.80) 3.39 (0.89) 3.63 (0.80) | F = 2.142 (0.119) | 3.35 (0.67) 3.49 (0.66) 3.70 (0.75) | F = 3.588 (0.029) * | 3.31 (0.59) 3.44 (0.67) 3.67 (0.73) | F = 3.801 (0.023) * |
| Working from home (WFH) | |||||||
| No Yes | 5 (1.7) 293 (98.3) | 3.40 (0.89) 3.36 (0.85) | t = 0.112 (0.911) | 2.87 (1.04) 3.46 (0.67) | t = −1.946 (0.053) | 3.13 (0.94) 3.41 (0.64) | t = −0.940 (0.348) |
| Factors | Crude B (95% CI) | p-Value | Adjusted B (95% CI) | p-Value |
|---|---|---|---|---|
| Marital status | ||||
| Single | −0.231 (−0.406, −0.056) | 0.010 * | −0.095 (−0.250, 0.059) | 0.227 |
| Married | ||||
| Household income | ||||
| B40 | −0.355 (−0.623, −0.088) | 0.009 * | −0.299(−0.529, −0.070) | 0.011 * |
| M40 | −0.228 (−0.494,0.038) | 0.092 | −0.179 (−0.402, 0.044) | 0.115 |
| T20 | ||||
| Personal burnout | −0.016 (−0.020, −0.012) | <0.001 * | −0.002 (−0.008, 0.003) | 0.405 |
| Work-related burnout | −0.017 (−0.021, −0.013) | <0.001 * | −0.004 (−0.010,0.002) | 0.214 |
| Client-related burnout | −0.016 (−0.020, −0.011) | <0.001 * | −0.004 (−0.009, 0.001) | 0.105 |
| Depression | −0.100 (−0.118, −0.082) | <0.001 * | −0.047 (−0.077, −0.016) | 0.003 * |
| Anxiety | −0.089 (−0.111, −0.067) | <0.001 * | 0.005 (−0.027, 0.037) | 0.758 |
| Stress | −0.092 (−0.110, −0.073) | <0.001 * | −0.029 (−0.062, 0.004) | 0.082 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmad Sabki, Z.; Kim, L.H.; Danaee, M.; Sulaiman, A.H.; Razali, K.A.; Koh, O.H.; Kanagasundram, S.; Kaur, M.; Azhar, F.L.; Francis, B. Assessment of Psychometric Properties of the Malay Version of the Brief Resilience Scale (BRS-M) among Non-Academic Staff Working from Home during COVID-19 in Malaysia. Healthcare 2023, 11, 1146. https://doi.org/10.3390/healthcare11081146
Ahmad Sabki Z, Kim LH, Danaee M, Sulaiman AH, Razali KA, Koh OH, Kanagasundram S, Kaur M, Azhar FL, Francis B. Assessment of Psychometric Properties of the Malay Version of the Brief Resilience Scale (BRS-M) among Non-Academic Staff Working from Home during COVID-19 in Malaysia. Healthcare. 2023; 11(8):1146. https://doi.org/10.3390/healthcare11081146
Chicago/Turabian StyleAhmad Sabki, Zuraida, Lee Hui Kim, Mahmoud Danaee, Ahmad Hatim Sulaiman, Khairul Arif Razali, Ong Hui Koh, Sharmilla Kanagasundram, Manveen Kaur, Fatin Liyana Azhar, and Benedict Francis. 2023. "Assessment of Psychometric Properties of the Malay Version of the Brief Resilience Scale (BRS-M) among Non-Academic Staff Working from Home during COVID-19 in Malaysia" Healthcare 11, no. 8: 1146. https://doi.org/10.3390/healthcare11081146
APA StyleAhmad Sabki, Z., Kim, L. H., Danaee, M., Sulaiman, A. H., Razali, K. A., Koh, O. H., Kanagasundram, S., Kaur, M., Azhar, F. L., & Francis, B. (2023). Assessment of Psychometric Properties of the Malay Version of the Brief Resilience Scale (BRS-M) among Non-Academic Staff Working from Home during COVID-19 in Malaysia. Healthcare, 11(8), 1146. https://doi.org/10.3390/healthcare11081146