The Effect of Preoperative Education on Psychological, Clinical and Economic Outcomes in Elective Spinal Surgery: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
Quality Assessment
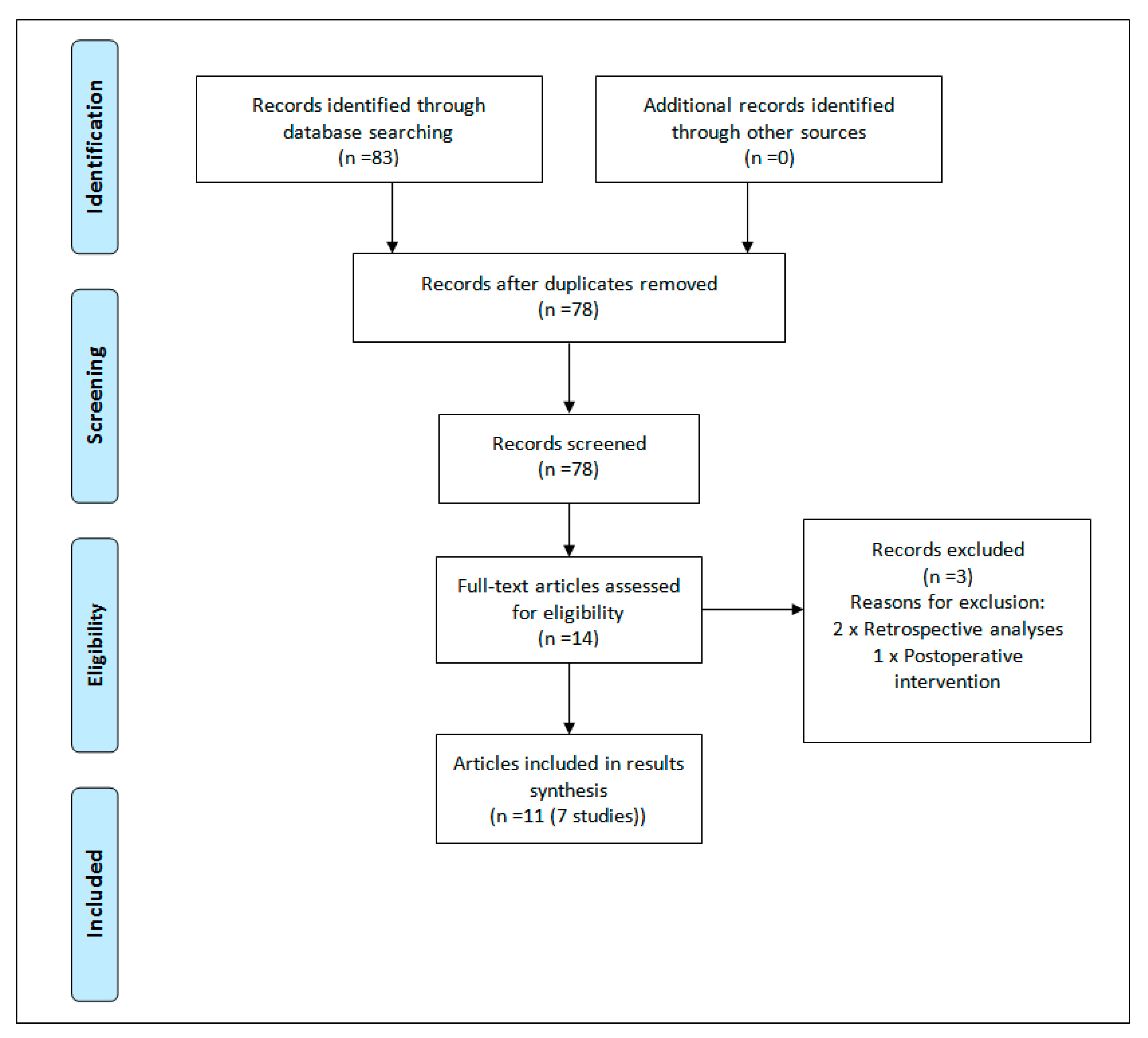
3. Results
3.1. Methodological Quality
3.2. Clinical Outcomes
3.3. Psychological Outcomes
3.4. Fear-Avoidance Beliefs
3.5. Economic Outcomes
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gometz, A.; Maislen, D.; Youtz, C.; Kary, E.; Gometz, E.L.; Sobotka, S.; Choudhri, T.F. The effectiveness of prehabilitation (prehab) in both functional and economic outcomes following spinal surgery: A systematic review. Cureus 2018, 10, e2675. [Google Scholar] [CrossRef] [PubMed]
- Ljungqvist, O.; Scott, M.; Fearon, K.C. Enhanced recovery after surgery: A review. JAMA Surg. 2017, 152, 292–298. [Google Scholar] [CrossRef]
- Wainwright, T.W.; Immins, T.; Middleton, R.G. Enhanced recovery after surgery (ERAS) and its applicability for major spine surgery. Best Pract. Res. Clin. Anaesthesiol. 2016, 30, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Fleege, C.; Arabmotlagh, M.; Almajali, A.; Rauschmann, M. Pra- und postoperative Fast-track-Behandlungskonzepte in der Wirbelsaulenchirurgie: Patienteninformation und Patientenkooperation [Pre- and postoperative fast-track treatment concepts in spinal surgery: Patient information and patient cooperation]. Orthopade 2014, 43, 1062–1064. [Google Scholar] [CrossRef]
- Amaral, V.; Marchi, L.; Martim, H.; Amaral, R.; Nogueira-Neto, J.; Pierro, E.; Oliveira, L.; Coutinho, E.; Marcelino, F.; Faulhaber, N.; et al. Influence of psychosocial distress in the results of elective lumbar spine surgery. J. Spine Surg. 2017, 3, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Mannion, A.F.; Elfering, A.; Staerkle, R.; Junge, A.; Grob, D.; Dvorak, J.; Jacobshagen, N.; Semmer, N.K.; Boos, N. Predictors of multidimensional outcome after spinal surgery. Eur. Spine J. 2007, 16, 777–786. [Google Scholar] [CrossRef]
- Celestin, J.; Edwards, R.R.; Jamison, R.N. Pretreatment psychosocial variables as predictors of outcomes following lumbar surgery and spinal cord stimulation: A systematic review and literature synthesis. Pain Med. 2009, 10, 639–653. [Google Scholar] [CrossRef]
- Strom, J.; Bjerrum, M.B.; Nielsen, C.V.; Thisted, C.N.; Nielsen, T.L.; Laursen, M.; Jorgensen, L.B. Anxiety and depression in spine surgery—A systematic integrative review. Spine J 2018, 18, 1272–1285. [Google Scholar] [CrossRef] [PubMed]
- Redman, B. Advances in Patient Education; Springer Publishing: New York, NY, USA, 2004. [Google Scholar]
- Devine, E.C.; Cook, T.D. Clinical and cost-saving effects of psychoeducational interventions with surgical patients: A meta-analysis. Res. Nurs. Health 1986, 9, 89–105. [Google Scholar] [CrossRef]
- Monticone, M.; Ferrante, S.; Teli, M.; Rocca, B.; Foti, C.; Lovi, A.; Brayda Bruno, M. Management of catastrophising and kinesiophobia improves rehabilitation after fusion for lumbar spondylolisthesis and stenosis. A randomised controlled trial. Eur. Spine J. 2014, 23, 87–95. [Google Scholar] [CrossRef]
- Skolasky, R.L.; Mackenzie, E.J.; Wegener, S.T.; Riley, L.H., 3rd. Patient activation and functional recovery in persons undergoing spine surgery. J. Bone Jt. Surg. Am. 2011, 93, 1665–1671. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, W264–W269. [Google Scholar] [CrossRef]
- Carli, F.; Scheede-Bergdahl, C. Prehabilitation to enhance perioperative care. Anesthesiol. Clin. 2015, 33, 17–33. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, 5.1.0 ed; The Cochrane Collaboration: Oxford, UK, 2011. [Google Scholar]
- Papanastassiou, I.; Anderson, R.; Barber, N.; Conover, C.; Castellvi, A.E. Effects of preoperative education on spinal surgery patients. SAS J. 2011, 5, 120–124. [Google Scholar] [CrossRef]
- Eastwood, D.; Manson, N.; Bigney, E.; Darling, M.; Richardson, E.; Paixao, R.; Underwood, T.; Ellis, K.; Abraham, E. Improving postoperative patient reported benefits and satisfaction following spinal fusion with a single preoperative education session. Spine J. 2018. [Google Scholar] [CrossRef] [PubMed]
- Archer, K.R.; Devin, C.J.; Vanston, S.W.; Koyama, T.; Phillips, S.E.; Mathis, S.L.; George, S.Z.; McGirt, M.J.; Spengler, D.M.; Aaronson, O.S.; et al. Cognitive-behavioral-based physical therapy for patients with chronic pain undergoing lumbar spine surgery: A randomized controlled trial. J. Pain 2016, 17, 76–89. [Google Scholar] [CrossRef]
- Rolving, N.; Nielsen, C.V.; Christensen, F.B.; Holm, R.; Bunger, C.E.; Oestergaard, L.G. Does a preoperative cognitive-behavioral intervention affect disability, pain behavior, pain, and return to work the first year after lumbar spinal fusion surgery? Spine (Phila PA 1976) 2015, 40, 593–600. [Google Scholar] [CrossRef]
- Rolving, N.; Nielsen, C.V.; Christensen, F.B.; Holm, R.; Bunger, C.E.; Oestergaard, L.G. Preoperative cognitive-behavioural intervention improves in-hospital mobilisation and analgesic use for lumbar spinal fusion patients. BMC Musculoskelet. Disord. 2016, 17, 217. [Google Scholar] [CrossRef]
- Rolving, N.; Sogaard, R.; Nielsen, C.V.; Christensen, F.B.; Bunger, C.; Oestergaard, L.G. Preoperative cognitive-behavioral patient education versus standard care for lumbar spinal fusion patients: Economic evaluation alongside a randomized controlled trial. Spine 2016, 41, 18–25. [Google Scholar] [CrossRef]
- Louw, A.; Diener, I.; Landers, M.R.; Puentedura, E.J. Preoperative pain neuroscience education for lumbar radiculopathy: A multicenter randomized controlled trial with 1-year follow-up. Spine (Phila PA 1976) 2014, 39, 1449–1457. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, P.R.; Andreasen, J.; Asmussen, M.; Tonnesen, H. Costs and quality of life for prehabilitation and early rehabilitation after surgery of the lumbar spine. BMC Health Serv. Res. 2008, 8, 209. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, P.R.; Jorgensen, L.D.; Dahl, B.; Pedersen, T.; Tonnesen, H. Prehabilitation and early rehabilitation after spinal surgery: Randomized clinical trial. Clin. Rehabil. 2010, 24, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Lindback, Y.; Tropp, H.; Enthoven, P.; Abbott, A.; Oberg, B. PREPARE: Presurgery physiotherapy for patients with degenerative lumbar spine disorder: A randomized controlled trial. Spine J. 2018, 18, 1347–1355. [Google Scholar] [CrossRef] [PubMed]
- Kesanen, J.; Leino-Kilpi, H.; Lund, T.; Montin, L.; Puukka, P.; Valkeapaa, K. The Knowledge Test Feedback Intervention (KTFI) increases knowledge level of spinal stenosis patients before operation-A randomized controlled follow-up trial. Patient Educ. Couns. 2016, 99, 1984–1991. [Google Scholar] [CrossRef] [PubMed]
- Kesanen, J.; Leino-Kilpi, H.; Lund, T.; Montin, L.; Puukka, P.; Valkeapaa, K. Increased preoperative knowledge reduces surgery-related anxiety: A randomised clinical trial in 100 spinal stenosis patients. Eur. Spine J. 2017, 26, 2520–2528. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Liu, J.T.; Lin, S.C.; Hsu, T.Y.; Lin, C.Y.; Lin, L.Y. Effects of educational intervention on state anxiety and pain in people undergoing spinal surgery: A randomized controlled trial. Pain Manag. Nurs. 2018, 19, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Chuang, M.-F.; Tung, H.-H.; Clinciu, D.L.; Huang, J.-S.; Iqbal, U.; Chang, C.-J.; Su, I.C.; Lai, F.-C.; Li, Y.-C. The effect of an integrated education model on anxiety and uncertainty in patients undergoing cervical disc herniation surgery. Comput. Methods Prog. Biomed. 2016, 133, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Ronnberg, K.; Lind, B.; Zoega, B.; Halldin, K.; Gellerstedt, M.; Brisby, H. Patients’ satisfaction with provided care/information and expectations on clinical outcome after lumbar disc herniation surgery. Spine (Phila PA 1976) 2007, 32, 256–261. [Google Scholar] [CrossRef]
- den Hartog, Y.M.; Mathijssen, N.M.C.; Vehmeijer, S.B.W. Reduced length of hospital stay after the introduction of a rapid recovery protocol for primary THA procedures. Acta Orthop. 2013, 84, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H. Fast-track hip and knee arthroplasty. Lancet (London) 2013, 381, 1600–1602. [Google Scholar] [CrossRef]
- Khan, S.K.; Malviya, A.; Muller, S.D.; Carluke, I.; Partington, P.F.; Emmerson, K.P.; Reed, M.R. Reduced short-term complications and mortality following Enhanced Recovery primary hip and knee arthroplasty: Results from 6,000 consecutive procedures. Acta Orthop. 2014, 85, 26–31. [Google Scholar] [CrossRef]
- Aasvang, E.K.; Luna, I.E.; Kehlet, H. Challenges in postdischarge function and recovery: The case of fast-track hip and knee arthroplasty. Br. J. Anaesth. 2015, 115, 861–866. [Google Scholar] [CrossRef]
- Gromov, K.; Kjarsgaard-Andersen, P.; Revald, P.; Kehlet, H.; Husted, H. Feasibility of outpatient total hip and knee arthroplasty in unselected patients. Acta Orthop. 2017, 88, 516–521. [Google Scholar] [CrossRef]
- McDonald, S.; Page, M.J.; Beringer, K.; Wasiak, J.; Sprowson, A. Preoperative education for hip or knee replacement. Cochrane Database Syst. Rev. 2014, CD003526. [Google Scholar] [CrossRef]
- Daltroy, L.H.; Morlino, C.I.; Eaton, H.M.; Poss, R.; Liang, M.H. Preoperative education for total hip and knee replacement patients. Arthritis Care Res. 1998, 11, 469–478. [Google Scholar] [CrossRef]
- Gammon, J.; Mulholland, C.W. Effect of preparatory information prior to elective total hip replacement on post-operative physical coping outcomes. Int. J. Nurs. Stud. 1996, 33, 589–604. [Google Scholar] [CrossRef]
- Rampersaud, Y.R.; Tso, P.; Walker, K.R.; Lewis, S.J.; Davey, J.R.; Mahomed, N.N.; Coyte, P.C. Comparative outcomes and cost-utility following surgical treatment of focal lumbar spinal stenosis compared with osteoarthritis of the hip or knee: Part 2—Estimated lifetime incremental cost-utility ratios. Spine J. Off. J. N. Am. Spine Soc. 2014, 14, 244–254. [Google Scholar] [CrossRef]
- Rampersaud, Y.R.; Lewis, S.J.; Davey, J.R.; Gandhi, R.; Mahomed, N.N. Comparative outcomes and cost-utility after surgical treatment of focal lumbar spinal stenosis compared with osteoarthritis of the hip or knee—Part 1: Long-term change in health-related quality of life. Spine J. Off. J. N. Am. Spine Soc. 2014, 14, 234–243. [Google Scholar] [CrossRef]
- Landers, M.R.; Puentedura, E.; Louw, A.; McCauley, A.; Rasmussen, Z.; Bungum, T. A population-based survey of lumbar surgery beliefs in the United States. Orthop. Nurs. 2014, 33, 207–216. [Google Scholar] [CrossRef]
- Pritchard, M.J. Managing anxiety in the elective surgical patient. Br. J. Nurs. 2009, 18, 416–419. [Google Scholar]
- Grupe, D.W.; Nitschke, J.B. Uncertainty and anticipation in anxiety: An integrated neurobiological and psychological perspective. Nat. Rev. Neurosci. 2013, 14, 488–501. [Google Scholar] [CrossRef]
- Hanton, S.; Connaughton, D. Perceived control of anxiety and its relationship to self-confidence and performance. Res. Q. Exerc. Sport 2002, 73, 87–97. [Google Scholar] [CrossRef]
- Block, A.R.; Gatchel, R.J.; Deardroff, W.W.; Guyer, R.D. Chapter 9: Preparing for spine surgery: Cognitive behavioural interventions. In The Psychology of Spine Surgery; American Psychological Association: Washington, DC, USA, 2003. [Google Scholar]
- Shuldham, C. A review of the impact of pre-operative education on recovery from surgery. Int. J. Nurs. Stud. 1999, 36, 171–177. [Google Scholar] [CrossRef]
- Leino-Kilpi, H.; Luoto, E.; Katajisto, J. Elements of empowerment and MS patients. J. Neurosci. Nurs. 1998, 30, 116–123. [Google Scholar] [CrossRef]
- Gillis, C.; Gill, M.; Marlett, N.; MacKean, G.; GermAnn, K.; Gilmour, L.; Nelson, G.; Wasylak, T.; Nguyen, S.; Araujo, E.; et al. Patients as partners in Enhanced Recovery After Surgery: A qualitative patient-led study. BMJ Open 2017, 7, e017002. [Google Scholar] [CrossRef]
- Vermeire, E.; Hearnshaw, H.; Van Royen, P.; Denekens, J. Patient adherence to treatment: Three decades of research. A comprehensive review. J. Clin. Pharm. Ther. 2001, 26, 331–342. [Google Scholar] [CrossRef]
- de Mik, S.M.L.; Stubenrouch, F.E.; Balm, R.; Ubbink, D.T. Systematic review of shared decision-making in surgery. Br. J. Surg. 2018, 105, 1721–1730. [Google Scholar] [CrossRef]
- Kelley, J.M.; Kraft-Todd, G.; Schapira, L.; Kossowsky, J.; Riess, H. The influence of the patient-clinician relationship on healthcare outcomes: A systematic review and meta-analysis of randomized controlled trials. PLoS ONE 2014, 9, e94207. [Google Scholar] [CrossRef]
- Stewart, M.A. Effective physician-patient communication and health outcomes: A review. CMAJ 1995, 152, 1423–1433. [Google Scholar]
- Ingadottir, B.; Zoega, S. Role of patient education in postoperative pain management. Nurs. Stand. 2017, 32, 50–63. [Google Scholar] [CrossRef]
- Meichenbaum, D. A cognititive-behaviour modification approach to assessment. In Cognititve Behaviour Modification, The Springer Behavior Therapy Series; Springer: Boston, MA, USA, 1977. [Google Scholar]
- Luna, I.E.; Kehlet, H.; Peterson, B.; Wede, H.R.; Hoevsgaard, S.J.; Aasvang, E.K. Early patient-reported outcomes versus objective function after total hip and knee arthroplasty: A prospective cohort study. Bone Jt. J. 2017, 99-B, 1167–1175. [Google Scholar] [CrossRef]


{kind=link}
| PICOS Item | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population |
|
|
| Intervention |
|
|
| Comparison |
| |
| Outcome Measures |
| |
| Study Design |
|
|
| Publication |
|
|
| Population | Intervention | Timing | Publication Type |
|---|---|---|---|
| “Spine surgery” OR “back surgery” OR “spine fusion” OR “spine stenosis” OR Spondylodesis OR “spine disease” OR “disc surgery” OR “lumbar surgery” OR “thoracic surgery” OR “cervical surgery” OR “kyphosis” OR “lordosis” OR “thoracolumbar surgery” OR “degenerative scoliosis” | (“Education”) OR (“Counseling”) OR Counselling OR Education OR “Cognitive based therapy” OR CBT OR “Psychological support” OR “Neuroscience education” OR “Prehabilitation” OR “Goal setting” OR “Goal achievement” | “Preoperative education” OR “Preoperative conditioning” OR “Preoperative interventions” OR Preoperative OR Perioperative OR “Preoperative” OR “Peri operative” OR “Pre-operative” OR Before OR Prior to OR (MM “Preoperative Period”) | “Randomized controlled trial” OR “Randomised controlled trial” OR “randomized clinical trial” OR “randomised clinical trial” OR “Controlled clinical trial” OR “clinical study” |
| Study | Population | Intervention | Control Group | Outcomes | Main Findings |
|---|---|---|---|---|---|
| Louw et al., 2014 [23] (n = 67) | Decompressive lumbar surgery. IG: n = 32 CG: n = 35 | Preoperative pain-specific neuroscience education programme in addition to usual care one week prior to lumbar surgery. Topics included the following:
| Usual care regarding preoperative education. | Pain (NPRS), function (ODI), postoperative thoughts/beliefs and health care utilization post-lumbar surgery. | At 1-year follow up, there were no statistical differences between groups with regard to primary outcome measure of low back pain (p = 0.183), leg pain (p = 0.075), and function (p = 0.365). The IG group scored significantly better in the following categories: better prepared for lumbar surgery (p = 0.001); preoperative session preparing them for lumbar surgery (p < 0.001) and lumbar surgery meeting their expectations (p = 0.021). Healthcare utilization post-lumbar surgery also favored the IG (p = 0.007). |
| Rolving et al., 2015, 2016a,b [20,21,22] (n = 90) | Lumbar spinal fusion. At baseline: IG: n = 59 CG: n = 31 | Six 3-h cognitive-behavioral therapy group sessions (4 sessions preoperatively and 2 sessions postoperatively). Topics included the following:
| Usual care regarding preoperative education. | (1) Disability (ODI), psychological variables, return to work and pain (low back pain rating scale); (2) Back pain (NPRS), mobility on day-3, analgesic use, hospitalization; (3) QALY, disability (ODI). | At 1-year follow up, there was no statistically significant difference between the IG and the CG in ODI score (p = 0.082). However, the IG had achieved a significant reduction of −15 points (−26, −4) already at 3 months (between group difference (p = 0.003), and this reduction was maintained throughout the year. There was no difference between the groups’ self-reported back pain (p = 0.76). Independent mobility was reached by a significantly larger number of patients in the IG than the CG during the first three postoperative days. Analgesic consumption tended to be lower in the IG, whereas length of hospitalization was unaffected by the CBT intervention. One year after the surgery, the estimated QALY was significantly better for the IG. There was no difference in the overall costs of the two groups. |
| Nielsen et al., 2008, 2010 [24,25] (n = 60) | Spinal surgery for degenerative disease with low back pain and radiating pain (decompression and fusion). Received intervention: IG: n = 28 CG: n = 32 | Prehabilitation and early rehabilitation, for 30 min daily for 6 to 8 weeks, including the following:
| Usual care regarding preoperative education. Postoperatively, the patient was mobilized on the day of surgery (if possible) and trained for 30 min daily. | (1) Cost and health-related quality of life; (2) Pain (BPI) function (Roland Morris questionnaire, sit to stand, TUG, milestone achieved under hospitalization, quality of life (HRQOL: 15-D). | No difference in health-related quality of life scores were observed. The IG obtained their postoperative milestones sooner, returned to work and utilized less primary care following discharge. The intervention programme was €1625 (direct costs €494 and indirect costs €1131) less per patient than usual care costs. At operation, the IG had improved function and postoperatively reached recovery milestones faster than the CG (1–6 days versus 3–13 days p = 0.001). Length of stay was shorter for the IG at 5 days (range: 3–9) versus 7 days (range: 5–15) and no differences were recorded in postoperative complications, or adverse events. |
| Kesänen et al., 2016, 2017 [27,28] (n = 100) | Surgery for spinal stenosis. At baseline: IG: n = 50 CG: n = 50 | Patients received an empowering telephone discourse based on scores from the KNOWBACK test. Items in the test included bio-physiological, functional, social, ethical and financial. | Usual care regarding preoperative education. | (1) Patient knowledge; (2) Anxiety (STAI-S), HRQoL (RAND-36), Disability (ODI), Pain (VAS). | At baseline, there was no difference in the knowledge level of the study groups. At admission, the knowledge level was significantly higher in five or six dimensions of empowering knowledge in the IG compared group to the CG. During the 3 and 6-month follow up, the knowledge level within the study groups remained stable. In the IG, a significant reduction in anxiety was noted after the intervention, whereas in the CG, anxiety reduced only after surgery. In both groups, a significant improvement in HRQoL, disability, and pain was noticed at the 6-month follow up, but there were no between-group differences. |
| Lee et al., 2018 [29] (n = 86) | Lumbar spinal surgery (fusion and decompression). IG: n = 43 CG: n = 43 | A patient booklet covering the following topics:
| Usual care regarding preoperative education. | Anxiety (STAI), pain (VAS), patient monitors for physical indicators (cortisol levels through saliva, blood pressure, heart rate and respiration rate). | The adjusted anxiety and pain levels were significantly lower for the IG: mean STAI scores were 52.67 at baseline and 47.54 at 30 min before surgery (p < 0.001); mean pain scores were 6.07 at baseline and 5.28 on day after surgery (p < 0.001). |
| Lindback et al., 2017 [26] (n = 197) | Surgery for disc herniation, spinal stenosis, spondylolisthesis, or degenerative disc disease. At randomization: IG: n = 99 CG: n = 91 | Pre-surgery physiotherapy twice a week for 9 weeks, including the following:
| Usual care regarding preoperative education. | Function and activity limitation (ODI), health related quality of life (SF-36 and EQ-5D) pain intensity (VAS), anxiety, depression (HADS), self-efficacy (SES), fear avoidance (FABQ-PA), physical activity and treatment effect (PGIC). | The IG demonstrated small improvements in disability, back pain, EQ-5D, EQ-VAS, dear avoidance belief questionnaire—physical activity, SES, and HADS scores and activity level after the pre-surgery intervention. However, post-surgery, the only differences between groups was a higher activity level in the IG compared to the CG. |
| Chuang et al., 2016 [30] (n = 64) | Anterior cervical discectomy and fusion surgery. IG: n = 32 CG: n = 32 | Twenty minutes of one-to-one education on the day of surgery, provided on an iPad and a booklet. Topics included the following:
| Usual care regarding preoperative education. | Anxiety (STAI), uncertainty (MUIS) and satisfaction with pre-surgery education (5-point Likert scale). | The educational intervention was found to be more effective than conventional care in reducing patient’s anxiety and uncertainty (p < 0.005). Patients were more satisfied in the IG due to a more holistic approach to individual health. |
| Study | Bias | ||||||
|---|---|---|---|---|---|---|---|
| Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Other Bias | |
| Rolving et al. [20] | + | − | − | − | + | + | − |
| Louw et al. [23] | + | + | − | − | + | + | − |
| Nielsen et al. [25] | + | + | − | − | − | + | + |
| Lindbäck et al. [26] | + | + | − | + | − | + | − |
| Kesänen et al. [28] | + | + | + | + | + | + | − |
| Lee et al. [29] | + | + | − | − | + | + | − |
| Chuang et al. [30] | + | − | − | − | + | + | + |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burgess, L.C.; Arundel, J.; Wainwright, T.W. The Effect of Preoperative Education on Psychological, Clinical and Economic Outcomes in Elective Spinal Surgery: A Systematic Review. Healthcare 2019, 7, 48. https://doi.org/10.3390/healthcare7010048
Burgess LC, Arundel J, Wainwright TW. The Effect of Preoperative Education on Psychological, Clinical and Economic Outcomes in Elective Spinal Surgery: A Systematic Review. Healthcare. 2019; 7(1):48. https://doi.org/10.3390/healthcare7010048
Chicago/Turabian StyleBurgess, Louise C., Joe Arundel, and Thomas W. Wainwright. 2019. "The Effect of Preoperative Education on Psychological, Clinical and Economic Outcomes in Elective Spinal Surgery: A Systematic Review" Healthcare 7, no. 1: 48. https://doi.org/10.3390/healthcare7010048
APA StyleBurgess, L. C., Arundel, J., & Wainwright, T. W. (2019). The Effect of Preoperative Education on Psychological, Clinical and Economic Outcomes in Elective Spinal Surgery: A Systematic Review. Healthcare, 7(1), 48. https://doi.org/10.3390/healthcare7010048