
Borderline Personality Symptoms: What Not to Be Overlooked When Approaching Suicidal Ideation among University Students


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
- Participants
- Instruments
- Screening Instrument for Borderline Personality Disorder (SI-Bord)
- 2.
- Revised Thai Multidimensional Scales of Perceived Social Support (r-MSPSS)
- 3.
- Thai Version of Perceived Stress Scales (T-PSS-10)
- 4.
- Patient-Health Questionaire-8 (PHQ-8)
- 5.
- Suicidality Ideation
- Statistical Analysis
3. Results
4. Discussion
- Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maser, B.; Danilewitz, M.; Guérin, E.; Findlay, L.; Frank, E. Medical Student Psychological Distress and Mental Illness Relative to the General Population: A Canadian Cross-Sectional Survey. Acad. Med. 2019, 94, 1781–1791. [Google Scholar] [CrossRef]
- Sathirapanya, C. Hhempan W: Stress among Students in UniversityStress among Students in UniversityStress among students in university. J. Lib. Arts Maejo U. 2013, 1, 42–58. [Google Scholar]
- Kunanitthaworn, N.; Wongpakaran, T.; Wongpakaran, N.; Paiboonsithiwong, S.; Songtrijuck, N.; Kuntawong, P.; Wedding, D. Factors associated with motivation in medical education: A path analysis. BMC Med. Educ. 2018, 18, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wongpakaran, T.; Wongpakaran, N.; Sirithepthawee, U.; Pratoomsri, W.; Burapakajornpong, N.; Rangseekajee, P.; Bookkamana, P.; Temboonkiat, A. Interpersonal problems among psychiatric outpatients and non-clinical samples. Singap. Med. J. 2012, 53, 481–487. [Google Scholar]
- Liu, C.H.; Stevens, C.; Wong, S.H.M.; Yasui, M.; Chen, J.A. The prevalence and predictors of mental health diagnoses and suicide among U.S. college students: Implications for addressing disparities in service use. Depress Anxiety 2019, 36, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Desalegn, G.T.; Wondie, M.; Dereje, S.; Addisu, A. Suicide ideation, attempt, and determinants among medical students Northwest Ethiopia: An institution-based cross-sectional study. Ann. Gen. Psychiatry 2020, 19, 44. [Google Scholar] [CrossRef]
- Ibrahim, A.K.; Kelly, S.J.; Adams, C.E.; Glazebrook, C. A systematic review of studies of depression prevalence in university students. J. Psychiatr. Res. 2013, 47, 391–400. [Google Scholar] [CrossRef]
- Berman, A.L. Risk factors observed in the last 30 days of life among student suicides: Distinguishing characteristics of college and university student suicides. J. Am. Coll Health 2020, 1–5. [Google Scholar] [CrossRef]
- Nock, M.K.; Borges, G.; Bromet, E.J.; Alonso, J.; Angermeyer, M.; Beautrais, A.; Bruffaerts, R.; Chiu, W.T.; de Girolamo, G.; Gluzman, S.; et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br. J. Psychiatry 2008, 192, 98–105. [Google Scholar] [CrossRef]
- Eskin, M.; AlBuhairan, F.; Rezaeian, M.; Abdel-Khalek, A.M.; Harlak, H.; El-Nayal, M.; Asad, N.; Khan, A.; Mechri, A.; Noor, I.M.; et al. Suicidal Thoughts, Attempts and Motives Among University Students in 12 Muslim-Majority Countries. Psychiatr Q 2019, 90, 229–248. [Google Scholar] [CrossRef]
- Asfaw, H.; Yigzaw, N.; Yohannis, Z.; Fekadu, G.; Alemayehu, Y. Prevalence and associated factors of suicidal ideation and attempt among undergraduate medical students of Haramaya University, Ethiopia. A cross sectional study. PLoS ONE 2020, 15, e0236398. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S. Suicidal ideation and associated factors among school-going adolescents in Thailand. Int. J. Environ. Res. Public Health 2012, 9, 462–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breet, E.; Matooane, M.; Tomlinson, M.; Bantjes, J. Systematic review and narrative synthesis of suicide prevention in high-schools and universities: A research agenda for evidence-based practice. BMC Public Health 2021, 21, 1116. [Google Scholar] [CrossRef] [PubMed]
- Heinen, I.; Bullinger, M. Kocalevent RD: Perceived stress in first year medical students—associations with personal resources and emotional distress. BMC Med. Educ. 2017, 17, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, N.D.; Chavda, P.; Shah, S. Prevalence and predictors of suicide ideation among undergraduate medical students from a medical college of Western India. Med. J. Armed Forces India 2021, 77 (Suppl. 1), S107–S114. [Google Scholar] [CrossRef]
- Coentre, R. Góis C: Suicidal ideation in medical students: Recent insights. Adv. Med. Educ. Pract. 2018, 9, 873–880. [Google Scholar] [CrossRef] [Green Version]
- Blasco, M.J.; Vilagut, G.; Almenara, J.; Roca, M.; Piqueras, J.A.; Gabilondo, A.; Lagares, C.; Soto-Sanz, V.; Alayo, I.; Forero, C.G.; et al. Suicidal Thoughts and Behaviors: Prevalence and Association with Distal and Proximal Factors in Spanish University Students. Suicide Life Threat Behav. 2019, 49, 881–898. [Google Scholar] [CrossRef]
- Tan, S.T.; Sherina, M.S.; Rampal, L.; Normala, I. Prevalence and predictors of suicidality among medical students in a public university. Med. J. Malays. 2015, 70, 1–5. [Google Scholar]
- Xu, Y.; Wang, C.; Shi, M. Identifying Chinese adolescents with a high suicide attempt risk. Psychiatry Res. 2018, 269, 474–480. [Google Scholar] [CrossRef]
- Mitsui, N.; Asakura, S.; Takanobu, K.; Watanabe, S.; Toyoshima, K.; Kako, Y.; Ito, Y.M.; Kusumi, I. Prediction of major depressive episodes and suicide-related ideation over a 3-year interval among Japanese undergraduates. PLoS ONE 2018, 13, e0201047. [Google Scholar] [CrossRef]
- Patsali, M.E.; Mousa, D.V.; Papadopoulou, E.V.K.; Papadopoulou, K.K.K.; Kaparounaki, C.K.; Diakogiannis, I.; Fountoulakis, K.N. University students’ changes in mental health status and determinants of behavior during the COVID-19 lockdown in Greece. Psychiatry Res. 2020, 292, 113298. [Google Scholar] [CrossRef]
- Gelezelyte, O.; Kazlauskas, E.; Brailovskaia, J.; Margraf, J.; Truskauskaite-Kuneviciene, I. Suicidal ideation in university students in Lithuania amid the COVID-19 pandemic: A prospective study with pre-pandemic measures. Death Stud. 2021, 1–9. [Google Scholar] [CrossRef]
- Findlay, L. Depression and suicidal ideation among Canadians aged 15 to 24. Health Rep. 2017, 28, 3–11. [Google Scholar] [PubMed]
- Casale, M.; Boyes, M.; Pantelic, M.; Toska, E.; Cluver, L. Suicidal thoughts and behaviour among South African adolescents living with HIV: Can social support buffer the impact of stigma? J. Affect Disord 2019, 245, 82–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booniam, S.; Wongpakaran, T.; Lerttrakarnnon, P.; Jiraniramai, S.; Kuntawong, P.; Wongpakaran, N. Predictors of Passive and Active Suicidal Ideation and Suicide Attempt Among Older People: A Study in Tertiary Care Settings in Thailand. Neuropsychiatr. Dis. Treat 2020, 16, 3135–3144. [Google Scholar] [CrossRef] [PubMed]
- Oon-arom, A.; Wongpakaran, T.; Kuntawong, P.; Wongpakaran, N. Attachment anxiety, depression, and perceived social support: A moderated mediation model of suicide ideation among the elderly. Int. Psychogeriatr. 2021, 33, 169–178. [Google Scholar] [CrossRef]
- Kaplan, C.; Tarlow, N.; Stewart, J.G.; Aguirre, B.; Galen, G.; Auerbach, R.P. Borderline personality disorder in youth: The prospective impact of child abuse on non-suicidal self-injury and suicidality. Compr Psychiatry 2016, 71, 86–94. [Google Scholar] [CrossRef] [Green Version]
- Khosravi, M.; Kasaeiyan, R. The relationship between neuroticism and suicidal thoughts among medical students: Moderating role of attachment styles. J. Fam. Med. Prim. Care 2020, 9, 2680–2687. [Google Scholar] [CrossRef]
- Costa, A.C.B.; Mariusso, L.M.; Canassa, T.C.; Previdelli, I.T.S.; Porcu, M. Risk factors for suicidal behavior in a university population in Brazil: A retrospective study. Psychiatry Res. 2019, 278, 129–134. [Google Scholar] [CrossRef]
- Blasco, M.J.; Vilagut, G.; Alayo, I.; Almenara, J.; Cebrià, A.I.; Echeburúa, E.; Gabilondo, A.; Gili, M.; Lagares, C.; Piqueras, J.A.; et al. First-onset and persistence of suicidal ideation in university students: A one-year follow-up study. J. Affect. Disord. 2019, 256, 192–204. [Google Scholar] [CrossRef]
- Sar, V.; Akyuz, G.; Kugu, N.; Ozturk, E.; Ertem-Vehid, H. Axis I dissociative disorder comorbidity in borderline personality disorder and reports of childhood trauma. J. Clin. Psychiatry 2006, 67, 1583–1590. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Diordrs, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Peters, J.R.; Upton, B.T.; Baer, R.A. Brief report: Relationships between facets of impulsivity and borderline personality features. J. Pers. Disord. 2013, 27, 547–552. [Google Scholar] [CrossRef]
- Paris, J.; Zweig-Frank, H. A 27-year follow-up of patients with borderline personality disorder. Compr. Psychiatry 2001, 42, 482–487. [Google Scholar] [CrossRef]
- Meaney, R.; Hasking, P.; Reupert, A. Prevalence of Borderline Personality Disorder in University Samples: Systematic Review, Meta-Analysis and Meta-Regression. PLoS ONE 2016, 11, e0155439. [Google Scholar] [CrossRef]
- Chen, T.H.; Hsiao, R.C.; Liu, T.L.; Yen, C.F. Predicting effects of borderline personality symptoms and self-concept and identity disturbances on internet addiction, depression, and suicidality in college students: A prospective study. Kaohsiung J. Med. Sci. 2019, 35, 508–514. [Google Scholar] [CrossRef] [Green Version]
- Paris, J. Suicidality in Borderline Personality Disorder. Medicina 2019, 55, 223. [Google Scholar] [CrossRef] [Green Version]
- Romero-Acosta, K.; Verhelst, S.; Lowe, G.A.; Lipps, G.E.; Restrepo, J.; Fonseca, L. Association Between Suicidal Behaviour and Cannabis and Tranquilizer use, Depression, Aggression and Other Borderline Personality Traits Among Students in Sincelejo, Colombia. Rev. Colomb. Psiquiatr. 2021. [Google Scholar] [CrossRef]
- Andrewes, H.E.; Hulbert, C.; Cotton, S.M.; Betts, J.; Chanen, A.M. Relationships between the frequency and severity of non-suicidal self-injury and suicide attempts in youth with borderline personality disorder. Early Interv. Psychiatry 2019, 13, 194–201. [Google Scholar] [CrossRef]
- Wongpakaran, N.; Wongpakaran, T.; Kittipodjanasit, A.; Chompoosri, P.; Kuntawong, P.; Wedding, D. Predictive factors for suicidal attempts: A case-control study. Perspect Psychiatr. Care 2019, 55, 667–672. [Google Scholar] [CrossRef]
- Angstman, K.B.; Seshadri, A.; Marcelin, A.; Gonzalez, C.A.; Garrison, G.M.; Allen, J.S. Personality Disorders in Primary Care: Impact on Depression Outcomes within Collaborative Care. J. Prim. Care Community Health 2017, 8, 233–238. [Google Scholar] [CrossRef] [Green Version]
- Wongpakaran, N.; Wongpakaran, T.; Boonyanaruthee, V.; Pinyopornpanish, M.; Intaprasert, S. Comorbid personality disorders among patients with depression. Neuropsychiatr. Dis. Treat 2015, 11, 1091–1096. [Google Scholar] [CrossRef] [Green Version]
- Rizk, M.M.; Choo, T.H.; Galfalvy, H.; Biggs, E.; Brodsky, B.S.; Oquendo, M.A.; Mann, J.J.; Stanley, B. Variability in Suicidal Ideation is Associated with Affective Instability in Suicide Attempters with Borderline Personality Disorder. Psychiatry 2019, 82, 173–178. [Google Scholar] [CrossRef]
- Bennett, C.; Melvin, G.A.; Quek, J.; Saeedi, N.; Gordon, M.S.; Newman, L.K. Perceived Invalidation in Adolescent Borderline Personality Disorder: An Investigation of Parallel Reports of Caregiver Responses to Negative Emotions. Child Psychiatry Hum. Dev. 2019, 50, 209–221. [Google Scholar] [CrossRef]
- Zhou, S.J.; Wang, L.L.; Qi, M.; Yang, X.J.; Gao, L.; Zhang, S.Y.; Zhang, L.G.; Yang, R.; Chen, J.X. Depression, Anxiety, and Suicidal Ideation in Chinese University Students During the COVID-19 Pandemic. Front Psychol. 2021, 12, 669833. [Google Scholar] [CrossRef]
- Wang, Y.H.; Shi, Z.T.; Luo, Q.Y. Association of depressive symptoms and suicidal ideation among university students in China: A systematic review and meta-analysis. Medicine 2017, 96, e6476. [Google Scholar] [CrossRef]
- Rungsang, B.; Chaimongkol, N.; Deoisres, W.; Wongnam, P. Suicidal Ideation among Thai Adolescents: An Empirical Test of a Causal Model. Pac. Rim Int. J. Nurs. Res. 2017, 21, 97–107. [Google Scholar]
- Wongpakaran, N.; Wongpakaran, T.; Kuntawong, P. A short screening tool for borderline personality disorder (Short-Bord): Validated by Rasch analysis. Asian J. Psychiatr. 2019, 44, 195–199. [Google Scholar] [CrossRef]
- Zimet, G.D.; Powell, S.S.; Farley, G.K.; Werkman, S.; Berkoff, K.A. Psychometric characteristics of the Multidimensional Scale of Perceived Social Support. J. Pers. Assess 1990, 55, 610–617. [Google Scholar]
- Wongpakaran, N.; Wongpakaran, T. A revised Thai Multi-Dimensional Scale of Perceived Social Support. Span J. Psychol. 2012, 15, 1503–1509. [Google Scholar] [CrossRef] [Green Version]
- Wongpakaran, N.; Wongpakaran, T. The Thai version of the PSS-10: An Investigation of its psychometric properties. BioPsychoSocial Med. 2010, 4, 6. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Quantitative Methods for Analyzing Travel Behaviour of Individuals: Some Recent Developments; Routledge: London, UK, 2021.
- Breet, E.; Kidd, M.; McGregor, N.W.; Stein, D.J.; Lochner, C. Suicide ideation and attempts in obsessive-compulsive disorder. Ann. Clin. Psychiatry 2019, 31, 192–199. [Google Scholar]
- Jiraniramai, S.; Wongpakaran, T.; Angkurawaranon, C.; Jiraporncharoen, W.; Wongpakaran, N. Construct Validity and Differential Item Functioning of the PHQ-9 Among Health Care Workers: Rasch Analysis Approach. Neuropsychiatr Dis. Treat. 2021, 17, 1035–1045. [Google Scholar]
- Mirkovic, B.; Delvenne, V.; Robin, M.; Pham-Scottez, A.; Corcos, M.; Speranza, M. Borderline personality disorder and adolescent suicide attempt: The mediating role of emotional dysregulation. BMC Psychiatry 2021, 21, 393. [Google Scholar] [CrossRef]
- Nisenbaum, R.; Links, P.S.; Eynan, R.; Heisel, M.J. Variability and predictors of negative mood intensity in patients with borderline personality disorder and recurrent suicidal behavior: Multilevel analyses applied to experience sampling methodology. J. Abnorm. Psychol. 2010, 119, 433–439. [Google Scholar] [CrossRef]
- Lew, B.; Huen, J.; Yu, P.; Yuan, L.; Wang, D.-F.; Ping, F.; Abu Talib, M.; Lester, D.; Jia, C.-X. Associations between depression, anxiety, stress, hopelessness, subjective well-being, coping styles and suicide in Chinese university students. PLoS ONE 2019, 14, e0217372. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; Thomas, M.R.; Huntington, J.L.; Lawson, K.L.; Novotny, P.J.; Sloan, J.A.; Shanafelt, T.D. Personal life events and medical student burnout: A multicenter study. Acad. Med. 2006, 81, 374–384. [Google Scholar] [CrossRef]
- Lageborn, C.T.; Ljung, R.; Vaez, M.; Dahlin, M. Ongoing university studies and the risk of suicide: A register-based nationwide cohort study of 5 million young and middle-aged individuals in Sweden, 1993-2011. BMJ Open 2017, 7, e014264. [Google Scholar] [CrossRef] [Green Version]
- Dyrbye, L.N.; West, C.P.; Satele, D.; Boone, S.; Tan, L.; Sloan, J.; Shanafelt, T.D. Burnout among U.S. medical students, residents, and early career physicians relative to the general U.S. population. Acad. Med. 2014, 89, 443–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quarshie, E.N.; Cheataa-Plange, H.V.; Annor, F.; Asare-Doku, W.; Lartey, J.K.S. Prevalence of suicidal behaviour among nursing and midwifery college students in Ghana. Nurs. Open 2019, 6, 897–906. [Google Scholar] [CrossRef]
- Hoying, J.; Melnyk, B.M.; Hutson, E.; Tan, A. Prevalence and Correlates of Depression, Anxiety, Stress, Healthy Beliefs, and Lifestyle Behaviors in First-Year Graduate Health Sciences Students. Worldviews Evid Based Nurs. 2020, 17, 49–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wathelet, M.; Duhem, S.; Vaiva, G.; Baubet, T.; Habran, E.; Veerapa, E.; Debien, C.; Molenda, S.; Horn, M.; Grandgenèvre, P.; et al. Factors Associated with Mental Health Disorders Among University Students in France Confined During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2025591. [Google Scholar] [CrossRef] [PubMed]
- Pramukti, I.; Strong, C.; Sitthimongkol, Y.; Setiawan, A.; Pandin, M.G.R.; Yen, C.F.; Lin, C.Y.; Griffiths, M.D.; Ko, N.Y. Anxiety and Suicidal Thoughts During the COVID-19 Pandemic: Cross-Country Comparative Study Among Indonesian, Taiwanese, and Thai University Students. J. Med. Internet Res. 2020, 22, e24487. [Google Scholar] [CrossRef]
- Tyrer, P.; Mulder, R.; Crawford, M.; Newton-Howes, G.; Simonsen, E.; Ndetei, D.; Koldobsky, N.; Fossati, A.; Mbatia, J.; Barrett, B. Personality disorder: A new global perspective. World Psychiatry Off. J. World Psychiatr. Assoc. (WPA) 2010, 9, 56–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | Mean (SD) or n (%) | |
|---|---|---|
| Age | 20.26 ± 1.4 | |
| Sex | Female | 270 (80.4) |
| Number of years studying | 2.58 ± 1.3 | |
| Academic major | ||
| Health Science | 254 (75.6) | |
| Non-health Science | 82 (24.4) | |
| Monthly allowance (THB) | ||
| <5000 | 182 (54.2) | |
| 5001–10,000 | 123 (36.6) | |
| >10,000 | 31 (9.2) | |
| Satisfaction with monthly allowance | ||
| Yes | 258 (76.8) | |
| No | 78 (23.2) | |
| Psychological variable | ||
| Level of suicidal ideation | ||
| None | 288 (85.71) | |
| Mild | 33 (9.82) | |
| Moderate and severe | 15 (4.46) | |
| SI-Bord | 3.80 ± 2.9 | |
| r-MSPSS | 53.09 ± 12.8 | |
| TPSS | 14.74 ± 6.5 | |
| PHQ-8 | 6.27 ± 4.9 | |
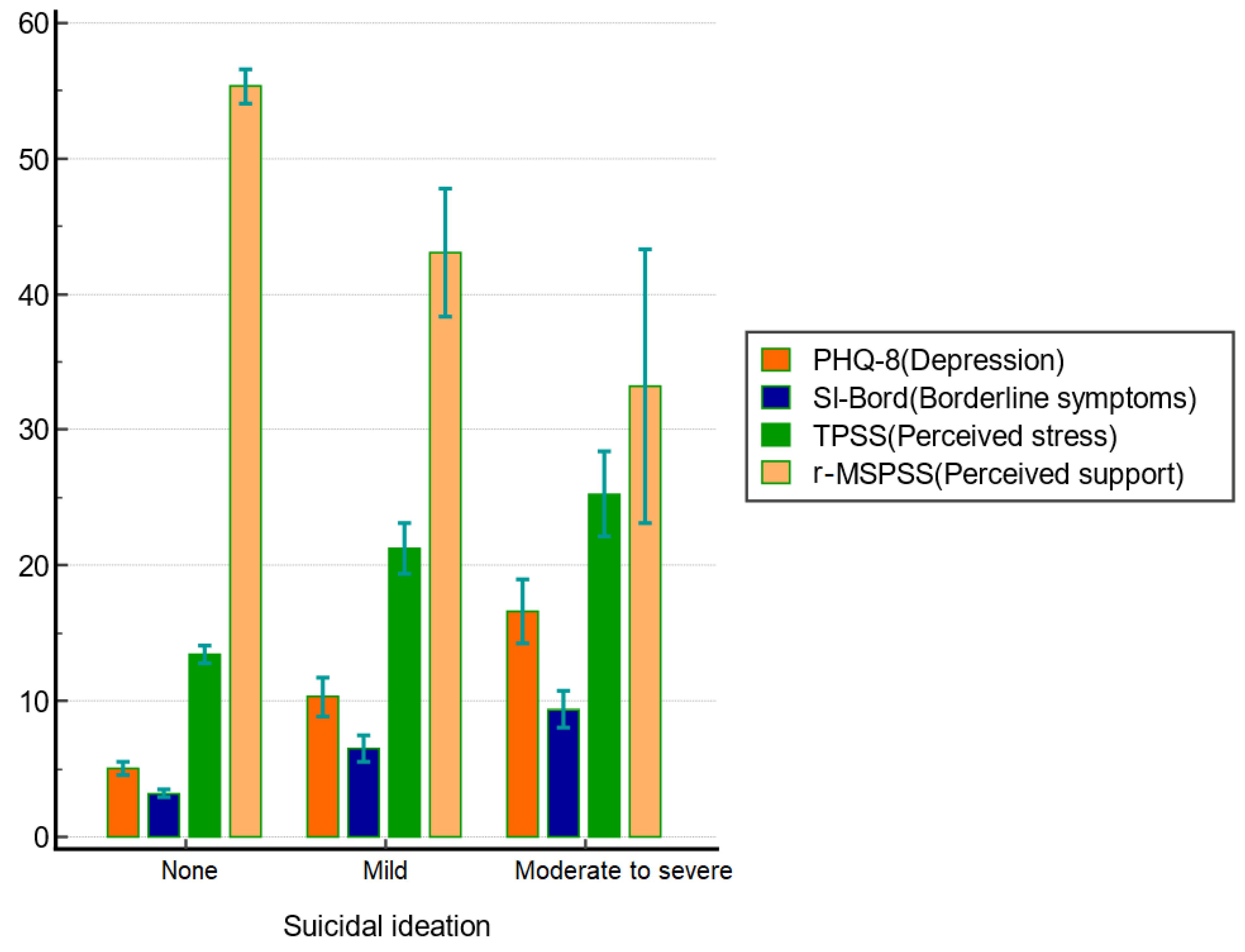
| Level of Suicidal Ideation | Test Difference | ||||
|---|---|---|---|---|---|
| Variable | None | Mild | Moderate/Severe | ||
| N = 288 | N = 33 | N = 15 | |||
| Age | 20.20 ± 1.3 | 20.42 ± 1.7 | 21.07 ± 1.4 | F (2, 333) = 3.06, p = 0.048 | |
| Sex | Female | 236 (87.4) | 25 (9.3) | 9 (3.3) | χ2 = 4.84, df2, p = 0.089 |
| Number of years studying | 2.51 ± 1.2 | 2.85 ± 1.4 | 3.4 ± 1.2 | F (2, 333) = 4.45, p = 0.012 | |
| Academic major | |||||
| Health Science | 229 (90.2) | 19 (7.5) | 6 (2.4) | χ2 = 18.51, df2, p < 0.001 | |
| Non-health Science | 59 (72.0) | 14 (17.1) | 9 (11.0) | ||
| Monthly Allowance (THB) | |||||
| <5000 | 163 (89.6) | 13 (7.1) | 6 (3.3) | χ2 = 6.65, df4, p = 0.155 | |
| 5001–10,000 | 102 (82.9) | 14 (11.4) | 7 (5.7) | ||
| >10,000 | 23 (74.2) | 6 (19.4) | 2 (6.5) | ||
| Satisfaction with monthly allowance | |||||
| Yes | 227 (88.0) | 21 (8.1) | 10 (3.9) | χ2 = 4.73, df2, p = 0.094 | |
| No | 61 (78.2) | 12 (15.4) | 5 (6.4) | ||
| Psychological variable | |||||
| SI-Bord | 3.19 ± 2.5 | 6.52 ± 2.8 | 9.40 ± 2.5 | F (2, 333) = 64.06, p < 0.001 | |
| r-MSPSS | 55.35 ± 10.9 | 43.06 ± 13.2 | 33.20 ± 18.2 | F (2, 333) = 40.09, p < 0.001 | |
| TPSS | 13.42 ± 5.8 | 21.24 ± 5.3 | 25.27 ± 5.6 | F (2, 333) = 54.51, p < 0.001 | |
| PHQ-8 | 5.01 ± 4.1 | 10.33 ± 4.0 | 16.6 ± 4.2 | F (2, 333) = 74.46, p < 0.001 | |
| Estimate | S.E. | Wald | df | p-Value | 95% Confidence Interval | ||
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| Age | 0.224 | 0.111 | 4.041 | 1 | 0.044 | 0.006 | 0.442 |
| Year | 0.319 | 0.120 | 7.035 | 1 | 0.008 | 0.083 | 0.555 |
| Health Science | 1.299 | 0.321 | 16.337 | 1 | 0.000 | 0.669 | 1.929 |
| PHQ-8 | 0.332 | 0.040 | 69.018 | 1 | 0.000 | 0.254 | 0.410 |
| TPSS | 0.276 | 0.035 | 60.647 | 1 | 0.000 | 0.207 | 0.346 |
| SI-Bord | 0.482 | 0.059 | 65.733 | 1 | 0.000 | 0.365 | 0.598 |
| r-MSPSS | −0.086 | 0.012 | 49.698 | 1 | 0.000 | −0.110 | −0.062 |
| Estimate | S.E. | Wald | df | p-Value | 95% Confidence Interval | |||
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | Odds Ratio (95% CI) | ||||||
| Age | −0.074 | 0.251 | 0.087 | 1 | 0.768 | −0.567 | 0.419 | 0.93 (0.59–1.46) |
| Year | 0.130 | 0.279 | 0.218 | 1 | 0.640 | −0.417 | 0.677 | 1.14 (0.67–1.93) |
| Health Science | 0.700 | 0.396 | 3.115 | 1 | 0.078 | −0.077 | 1.476 | 2.01 (0.93–4.36) |
| PHQ-8 | 0.149 | 0.053 | 7.800 | 1 | 0.005 | 0.044 | 0.253 | 1.16 (1.05–1.22) |
| TPSS | 0.104 | 0.045 | 5.297 | 1 | 0.021 | 0.015 | 0.193 | 1.11 (1.01–1.22) |
| SI-Bord | 0.170 | 0.080 | 4.476 | 1 | 0.034 | 0.013 | 0.328 | 1.19 (1.01–1.40) |
| r-MSPSS | −0.033 | 0.015 | 4.575 | 1 | 0.032 | −0.062 | −0.003 | 0.97 (0.94–1.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wongpakaran, N.; Oon-Arom, A.; Karawekpanyawong, N.; Lohanan, T.; Leesawat, T.; Wongpakaran, T. Borderline Personality Symptoms: What Not to Be Overlooked When Approaching Suicidal Ideation among University Students. Healthcare 2021, 9, 1399. https://doi.org/10.3390/healthcare9101399
Wongpakaran N, Oon-Arom A, Karawekpanyawong N, Lohanan T, Leesawat T, Wongpakaran T. Borderline Personality Symptoms: What Not to Be Overlooked When Approaching Suicidal Ideation among University Students. Healthcare. 2021; 9(10):1399. https://doi.org/10.3390/healthcare9101399
Chicago/Turabian StyleWongpakaran, Nahathai, Awirut Oon-Arom, Nuntaporn Karawekpanyawong, Trustsavin Lohanan, Thanakorn Leesawat, and Tinakon Wongpakaran. 2021. "Borderline Personality Symptoms: What Not to Be Overlooked When Approaching Suicidal Ideation among University Students" Healthcare 9, no. 10: 1399. https://doi.org/10.3390/healthcare9101399
APA StyleWongpakaran, N., Oon-Arom, A., Karawekpanyawong, N., Lohanan, T., Leesawat, T., & Wongpakaran, T. (2021). Borderline Personality Symptoms: What Not to Be Overlooked When Approaching Suicidal Ideation among University Students. Healthcare, 9(10), 1399. https://doi.org/10.3390/healthcare9101399