
Olfactory Drug Aerosol Delivery with Acoustic Radiation



Abstract
:1. Introduction
- (1)
- to develop a computational model of olfactory drug delivery with acoustic radiation forces in four nasal geometries.
- (2)
- to understand the acoustic responses of varying nasal geometries to pulsating waves from the nostrils.
- (3)
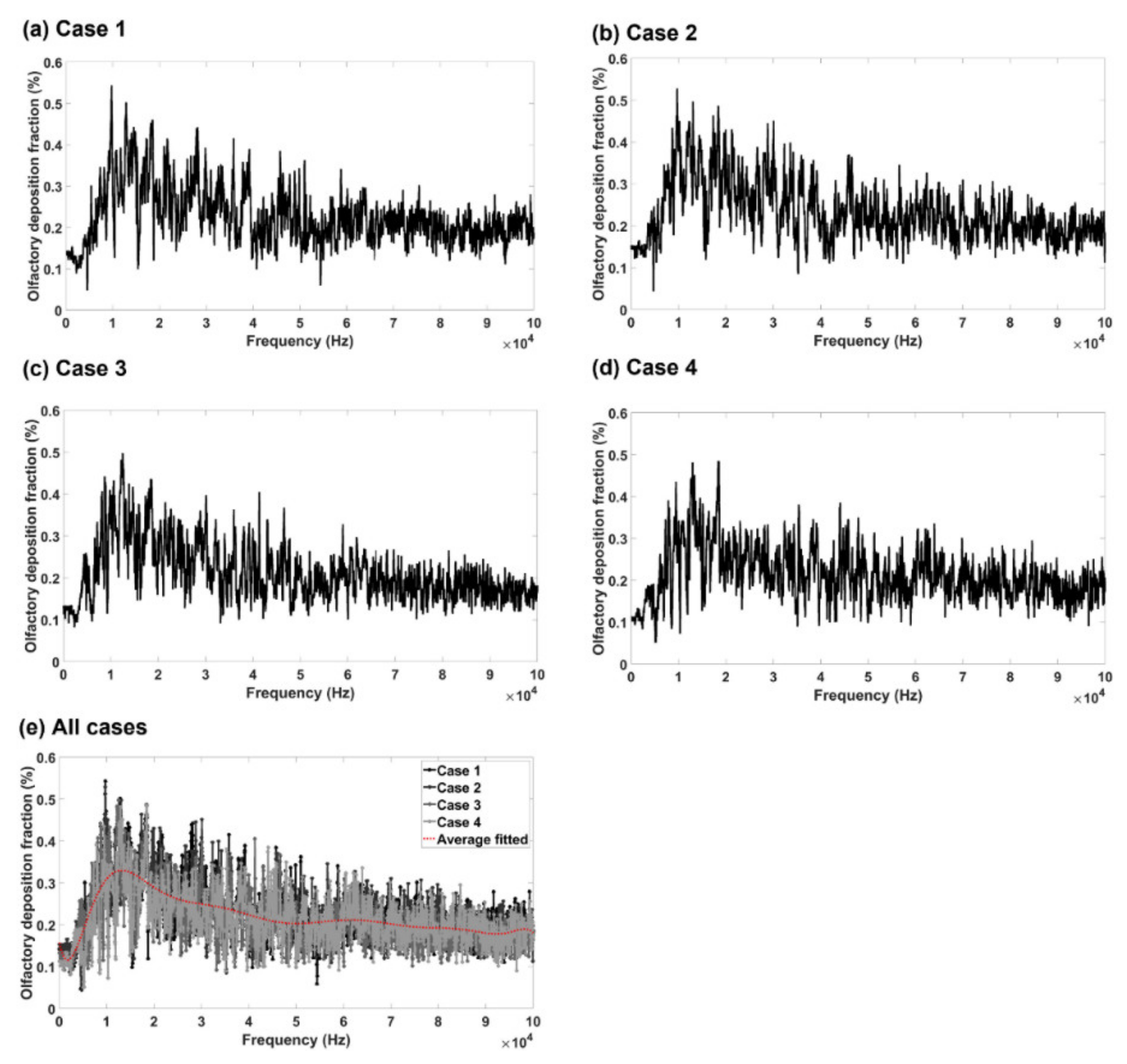
- to predict the olfactory deposition fraction in the four nasal geometries under varying pulsating frequencies ranging from 10 Hz to 100,000 Hz.
2. Materials and Methods
2.1. Nasal Airway Models
2.2. Numerical Models
2.3. Correlation Analysis
3. Results
3.1. Grid Independence Study
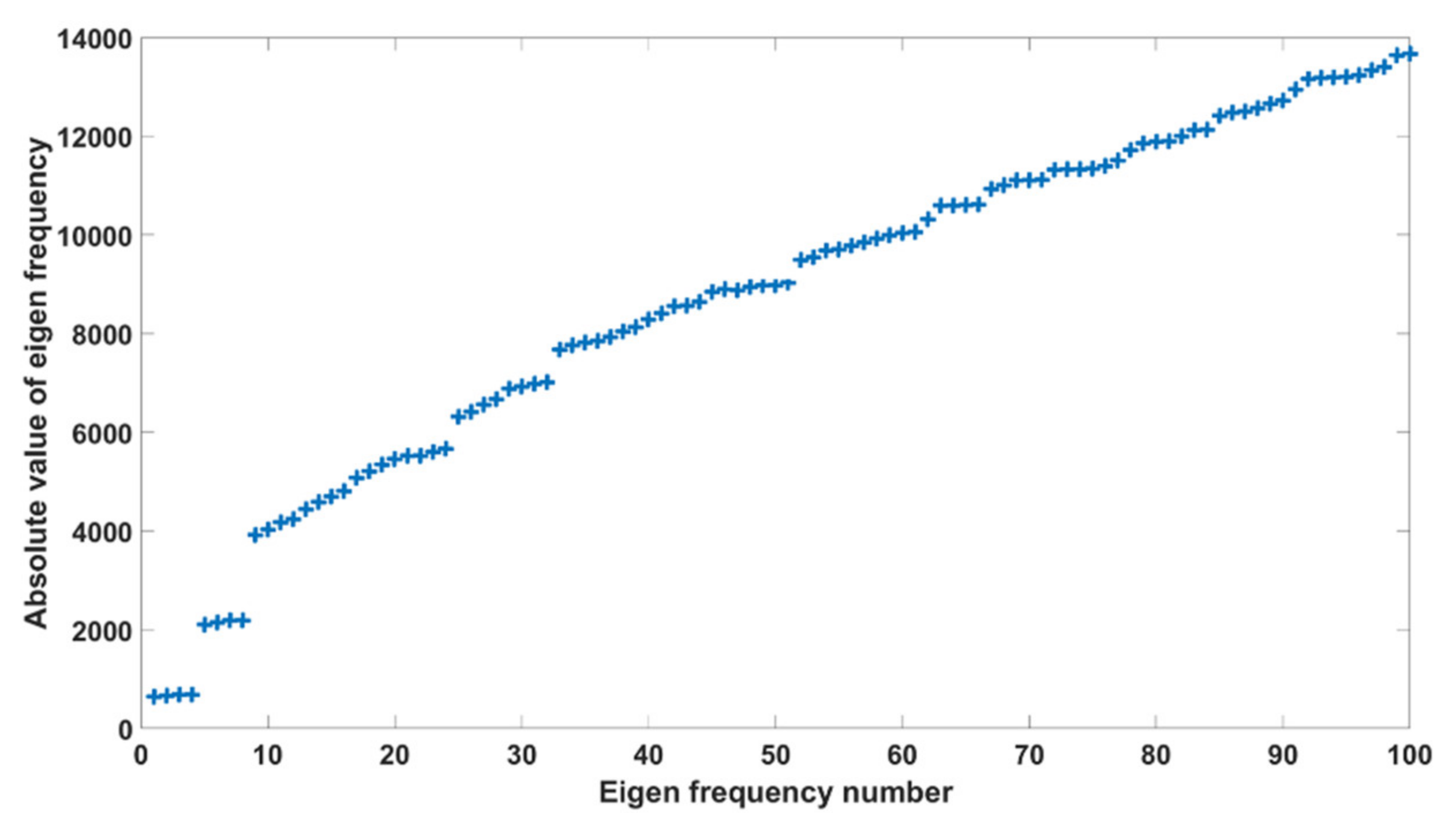
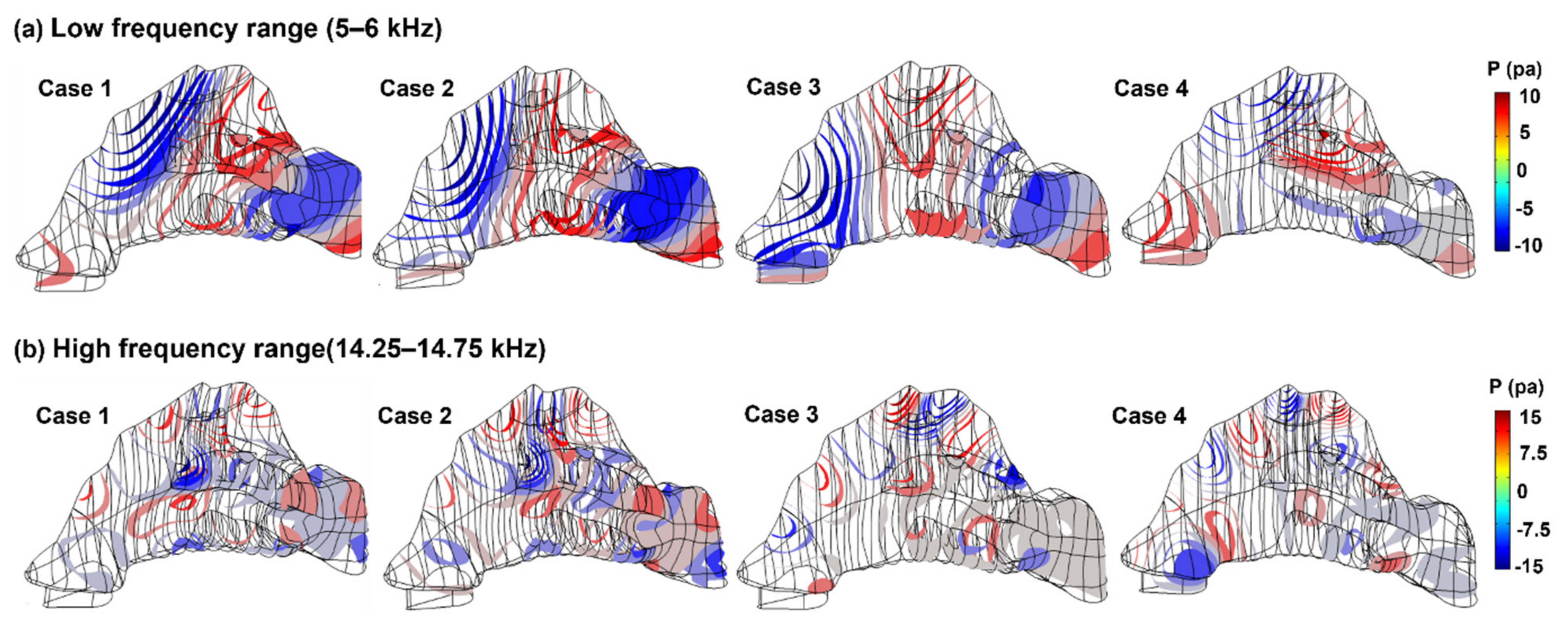
3.2. Acoustic Eigenfrequency Analysis
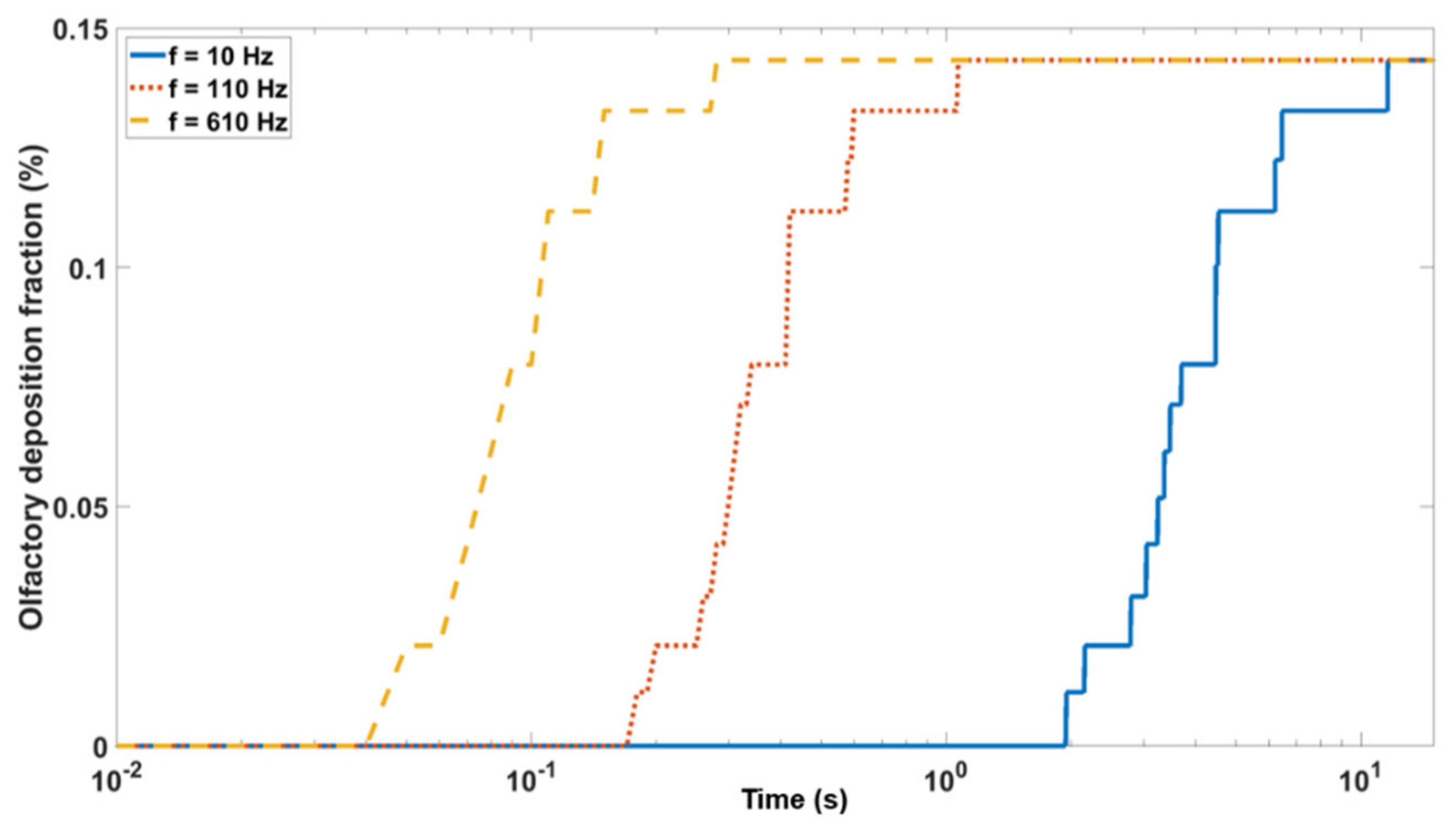
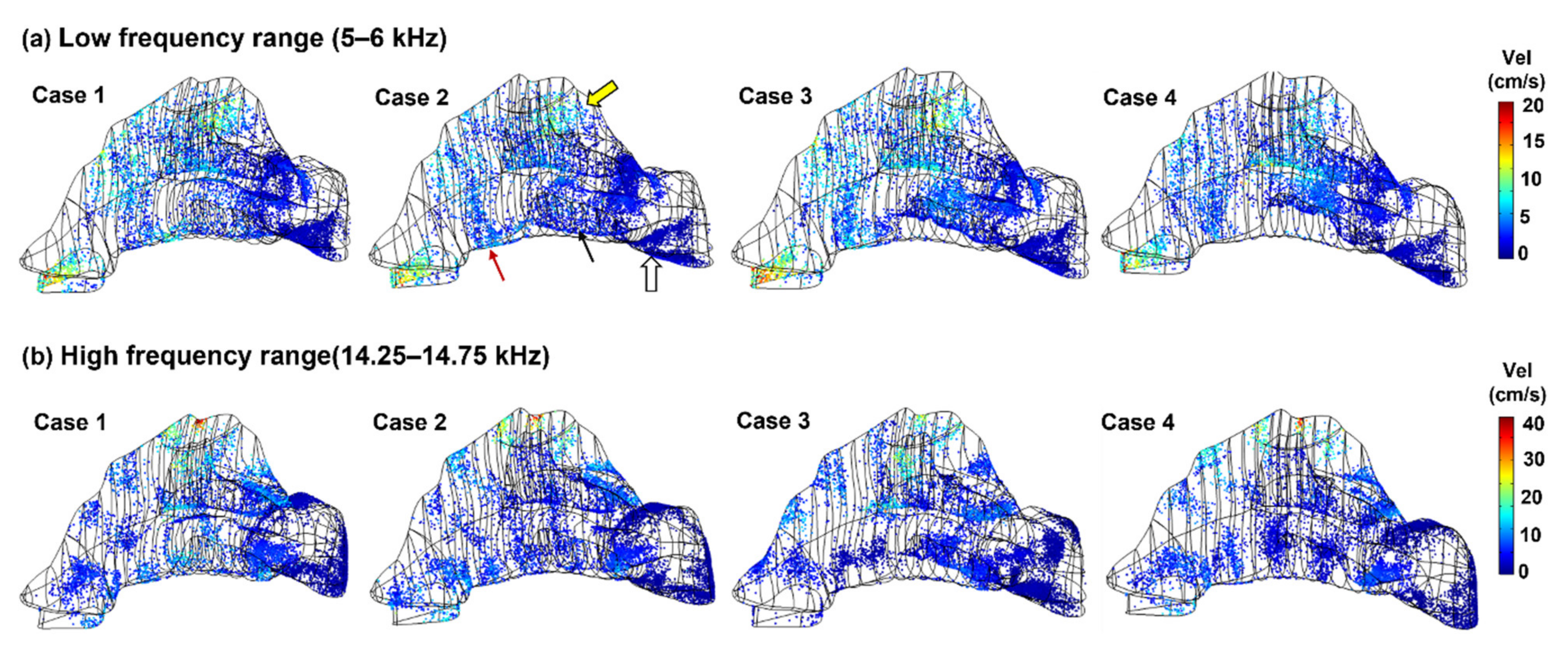
3.3. Olfactory Deposition with Acoustic Radiation Force
4. Discussion
5. Conclusions
- (1)
- Frequency analyses of the nasal cavity revealed that certain eigenfrequencies were particularly associated with the olfactory region and had the potential to deliver more drugs to the olfactory region.
- (2)
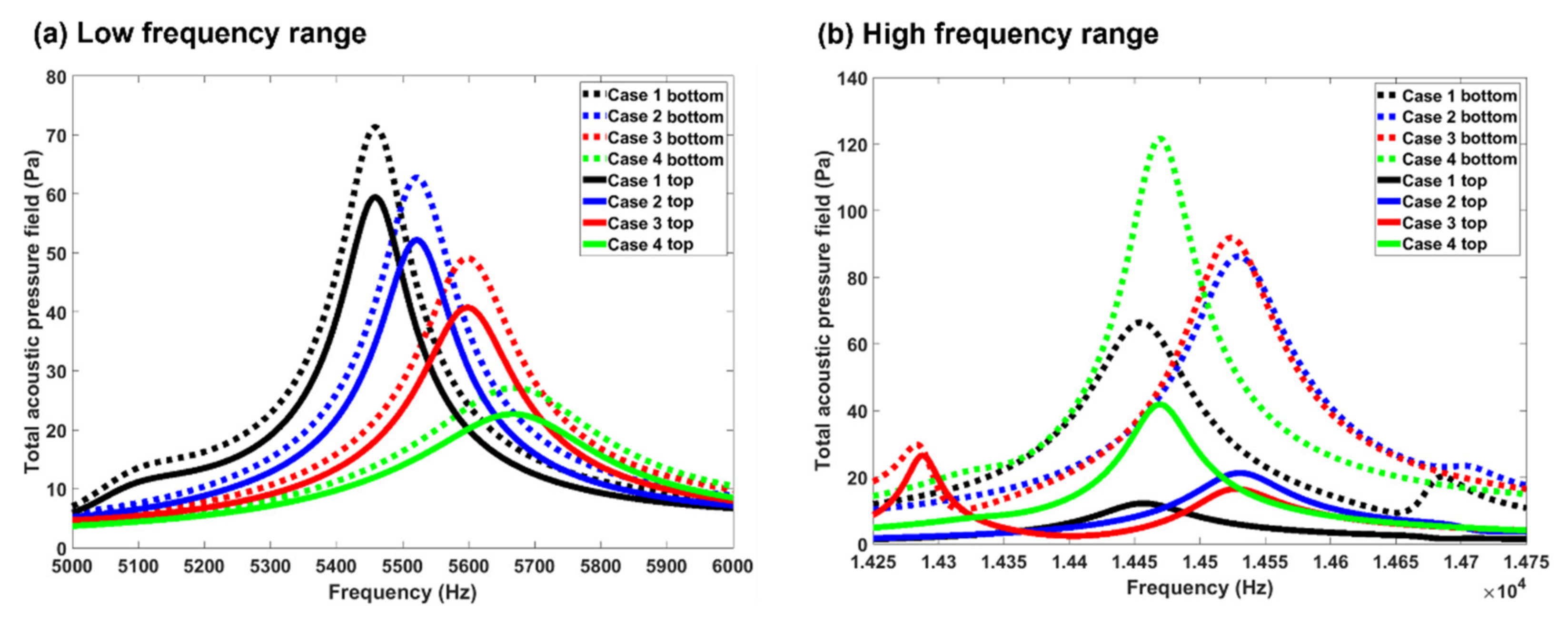
- At high frequencies, the acoustic pressure peaks/valleys were smaller in size and distributed in an alternating manner.
- (3)
- Turbinate shrinking/swelling did not have a significant impact on the magnitude of the olfactory delivery efficiency but would alter the frequency for optimal olfactory delivery.
- (4)
- The olfactory deposition was maximal at 11–15 kHz and decreased at higher frequencies. The olfactory deposition was almost constant for f > 40 kHz.
- (5)
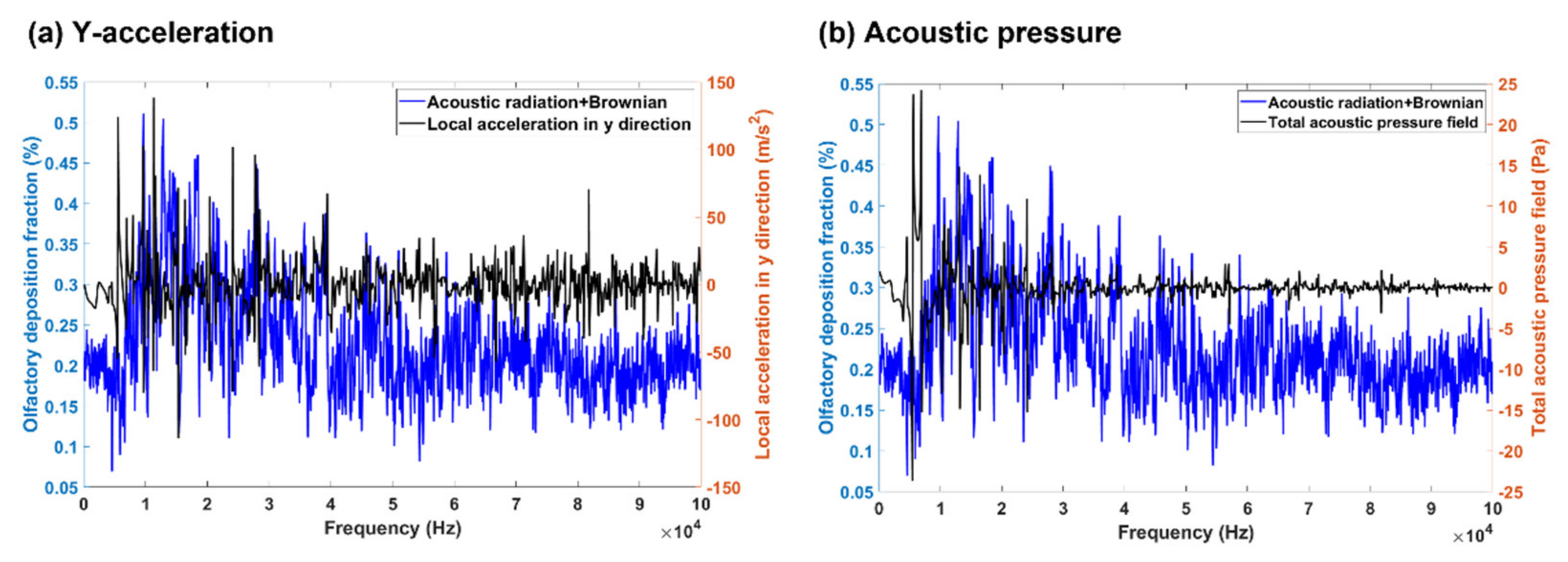
- A higher cross-correlation between the product of pressure and pressure gradient and the olfactory deposition delivery efficiency was found than other acoustic parameters. The nearest peaks belong to the y component of local acceleration, and the minimum unnormalized distance based on dynamic time warping algorithm belongs to the total acoustic pressure field.
- (6)
- Frequency analysis near the olfactory region showed a negative correlation between acoustic pressure and turbinate cross-section.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sheikh, S.; Haque, E.; Mir, S.S. Neurodegenerative Diseases: Multifactorial Conformational Diseases and Their Therapeutic Interventions. J. Neurodegener. Dis. 2013, 2013, 563481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Md, S.; Bhattmisra, S.K.; Zeeshan, F.; Shahzad, N.; Mujtaba, M.A.; Srikanth Meka, V.; Radhakrishnan, A.; Kesharwani, P.; Baboota, S.; Ali, J. Nano-carrier enabled drug delivery systems for nose to brain targeting for the treatment of neurodegenerative disorders. J. Drug Deliv. Sci. Technol. 2018, 43, 295–310. [Google Scholar] [CrossRef]
- Sikich, L.; Kolevzon, A.; King, B.H.; McDougle, C.J.; Sanders, K.B.; Kim, S.J.; Spanos, M.; Chandrasekhar, T.; Trelles, M.D.P.; Rockhill, C.M.; et al. Intranasal oxytocin in children and adolescents with autism spectrum disorder. N. Engl. J. Med. 2021, 385, 1462–1473. [Google Scholar] [CrossRef] [PubMed]
- Bourganis, V.; Kammona, O.; Alexopoulos, A.; Kiparissides, C. Recent advances in carrier mediated nose-to-brain delivery of pharmaceutics. Eur. J. Pharm. Biopharm. 2018, 128, 337–362. [Google Scholar] [CrossRef] [PubMed]
- Lehn, A.; Gelauff, J.; Hoeritzauer, I.; Ludwig, L.; McWhirter, L.; Williams, S.; Gardiner, P.; Carson, A.; Stone, J. Functional neurological disorders: Mechanisms and treatment. J. Neurol. 2016, 263, 611–620. [Google Scholar] [CrossRef]
- Martier, R.; Konstantinova, P. Gene Therapy for Neurodegenerative Diseases: Slowing Down the Ticking Clock. Front. Neurosci. 2020, 14, 580179. [Google Scholar] [CrossRef]
- Tan, M.S.A.; Parekh, H.S.; Pandey, P.; Siskind, D.J.; Falconer, J.R. Nose-to-brain delivery of antipsychotics using nanotechnology: A review. Expert Opin. Drug. Deliv. 2020, 17, 839–853. [Google Scholar] [CrossRef]
- Hanson, L.; Frey, W. Strategies for Intranasal Delivery of Therapeutics for the Prevention and Treatment of NeuroAIDS. J. Neuroimmune Pharmacol. 2007, 2, 81–86. [Google Scholar] [CrossRef]
- Sood, S.; Jain, K.; Gowthamarajan, K. Intranasal therapeutic strategies for management of Alzheimer’s disease. J. Drug. Target. 2014, 22, 279–294. [Google Scholar] [CrossRef]
- Kumar, H.; Mishra, G.; Sharma, A.K.; Gothwal, A.; Kesharwani, P.; Gupta, U. Intranasal drug delivery: A non-invasive approach for the better delivery of neurotherapeutics. Pharm. Nanotechnol. 2017, 5, 203–214. [Google Scholar] [CrossRef]
- Frey, W.H.; Liu, J.; Chen, X.Q.; Thorne, R.G.; Fawcett, J.R.; Ala, T.A.; Rahman, Y.E. Delivery of I-125-NGF to the brain via the olfactory route. Drug Deliv. 1997, 4, 87–92. [Google Scholar] [CrossRef]
- Francis, G.; Martinez, J.; Liu, W.; Nguyen, T.; Ayer, A.; Fine, J.; Zochodne, D.; Hanson, L.R.; Frey, W.H.; Toth, C. Intranasal Insulin Ameliorates Experimental Diabetic Neuropathy. Diabetes 2009, 58, 934–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.F.; Fawcett, J.R.; Thorne, R.G.; DeFor, T.A.; Frey, W.H. Intranasal administration of insulin-like growth factor-I bypasses the blood-brain barrier and protects against focal cerebral ischemic damage. J. Neurol. Sci. 2001, 187, 91–97. [Google Scholar] [CrossRef]
- Xi, J.; Barari, K.; Si, X.A.; Abdollahzadeh Jamalabadi, M.Y.; Park, J.H.; Rein, M. Inspiratory leakage flow fraction for surgical masks with varying gaps and filter materials. Phys. Fluids 2022, 34, 041908. [Google Scholar]
- Jain, H.; Prabhakar, B.; Shende, P. Modulation of olfactory area for effective transportation of actives in CNS disorders. J. Drug. Deliv. Sci. Technol. 2022, 68, 103091. [Google Scholar] [CrossRef]
- Kanazawa, T. Brain delivery of small interfering ribonucleic acid and drugs through intranasal administration with nano-sized polymer micelles. Med. Devices 2015, 8, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Kooiman, K.; Vos, H.J.; Versluis, M.; de Jong, N. Acoustic behavior of microbubbles and implications for drug delivery. Adv. Drug. Deliv. Rev. 2014, 72, 28–48. [Google Scholar] [CrossRef]
- Krishan, M.; Gudelsky, G.A.; Desai, P.B.; Genter, M.B. Manipulation of olfactory tight junctions using papaverine to enhance intranasal delivery of gemcitabine to the brain. Drug Deliv. 2014, 21, 8–16. [Google Scholar] [CrossRef] [Green Version]
- Si, X.A.; Xi, J.; Kim, J.; Zhou, Y.; Zhong, H. Modeling of release position and ventilation effects on olfactory aerosol drug delivery. Respir. Physiol. Neurobiol. 2013, 186, 22–32. [Google Scholar] [CrossRef]
- Si, X.A.; Sami, M.; Xi, J. Liquid film translocation significantly enhances nasal spray delivery to olfactory region: A numerical simulation study. Pharmaceutics 2021, 13, 903. [Google Scholar] [CrossRef]
- Xi, J.; Yuan, J.E.; Zhang, Y.; Nevorski, D.; Wang, Z.; Zhou, Y. Visualization and Quantification of Nasal and Olfactory Deposition in a Sectional Adult Nasal Airway Cast. Pharm. Res. 2016, 33, 1527–1541. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.S.; Holmes, T.D.; Gao, J.; Guilmette, R.A.; Li, S.; Surakitbanharn, Y.; Rowlings, C. Characterization of nasal spray pumps and deposition pattern in a replica of the human nasal airway. J. Aerosol. Med. 2001, 14, 267–280. [Google Scholar] [CrossRef] [PubMed]
- Xi, J.; Longest, P.W. Numerical predictions of submicrometer aerosol deposition in the nasal cavity using a novel drift flux approach. Int. J. Heat Mass Transfer 2008, 51, 5562–5577. [Google Scholar] [CrossRef]
- Gubner, J.A. Probability and Random Processes for Electrical and Computer Engineers; Cambridge University Press: Cambridge, UK, 2006; ISBN 978-0-521-86470-1. [Google Scholar]
- Petitjean, F.; Ketterlin, A.; Gançarski, P. A global averaging method for dynamic time warping, with applications to clustering. Pattern Recognit. 2011, 44, 678–693. [Google Scholar] [CrossRef]
- Schroeter, J.D.; Tewksbury, E.W.; Wong, B.A.; Kimbell, J.S. Experimental measurements and computational predictions of regional particle deposition in a sectional nasal model. J. Aerosol Med. Pulm. Drug. Deliv. 2015, 28, 20–29. [Google Scholar] [CrossRef]
- Djupesland, P.G. Nasal drug delivery devices: Characteristics and performance in a clinical perspective—A review. Drug Deliv. Transl. Res. 2013, 3, 42–62. [Google Scholar] [CrossRef] [Green Version]
- Basu, S.; Holbrook, L.T.; Kudlaty, K.; Fasanmade, O.; Wu, J.; Burke, A.; Langworthy, B.W.; Farzal, Z.; Mamdani, M.; Bennett, W.D.; et al. Numerical evaluation of spray position for improved nasal drug delivery. Sci. Rep. 2020, 10, 10568. [Google Scholar] [CrossRef]
- Vahaji, S.; Shang, Y.; Zhang, Y.; Wong, E.; Rezk, A.; Yeo, L.; Vreugde, S.; Wormald, P.-J.; Singh, N.; Inthavong, K. Optimising Aerosol Delivery for Maxillary Sinus Deposition in a Post-FESS Sinonasal Cavities. Aerosol Air Qual. Res. 2021, 21, 210098. [Google Scholar] [CrossRef]
- Javia, A.; Kore, G.; Misra, A. Polymers in nasal drug delivery: An overview. In Applications of Polymers in Drug Delivery, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 305–332. [Google Scholar]
- Li, C.; Wang, J.; Wang, Y.; Gao, H.; Wei, G.; Huang, Y.; Yu, H.; Gan, Y.; Wang, Y.; Mei, L. Recent progress in drug delivery. Acta Pharm. Sin. B 2019, 9, 1145–1162. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Value | |
|---|---|
| 343 [m/s] | |
| T | 293.15 [K] |
| pA | 1 [atm] |
| 1.24 [kg/m3] | |
| 1000 [kg/m3] | |
| 1 [μm] | |
| 2.2 [GPa] |
| Fine | Normal | Coarse | Coarser | |
|---|---|---|---|---|
| Number of edge elements | 5930 | 4254 | 2855 | 3397 |
| Number of boundary elements | 18,888 | 10,396 | 4484 | 6370 |
| Number of elements | 40,743 | 19,631 | 3652 | 11,343 |
| Minimum element quality | 0.01095 | 0.03195 | 0.01201 | 0.009745 |
| Number of vertex elements | 1057 | 1057 | 1057 | 1057 |
| Error (%) | 0 | 1.66 | 5.09 | 26.30 |
| Parameter | Place | MCC | PD | DTWA |
|---|---|---|---|---|
| Total acoustic pressure field | OL * | 358.3626 | 2850 | 0.0330 |
| Local velocity (RMS) | OL | 76.6382 | 6650 | 0.0484 |
| Instantaneous local acceleration | OL | 111.6919 | 65,500 | 0.0694 |
| Pressure | OL | 370.0679 | 4150 | 0.0334 |
| Pressure × velocity | OL | 13.1760 | 6650 | 0.0688 |
| Local acceleration, y component | OL | 307.4364 | 1600 | 0.0700 |
| Pressure × pressure gradient | OL | 329.0383 | 14,400 | 0.0694 |
| Total acoustic pressure field | N ** | 539.3815 | 14,400 | 0.0694 |
| Local acceleration, x component | N | 238.5432 | 9700 | 0.5424 |
| Local acceleration, y component | N | 306.3583 | 14,400 | 0.0695 |
| Local acceleration, z component | N | 399.8635 | 72,100 | 0.0696 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdollahzadeh Jamalabadi, M.Y.; Xi, J. Olfactory Drug Aerosol Delivery with Acoustic Radiation. Biomedicines 2022, 10, 1347. https://doi.org/10.3390/biomedicines10061347
Abdollahzadeh Jamalabadi MY, Xi J. Olfactory Drug Aerosol Delivery with Acoustic Radiation. Biomedicines. 2022; 10(6):1347. https://doi.org/10.3390/biomedicines10061347
Chicago/Turabian StyleAbdollahzadeh Jamalabadi, Mohammad Yaghoub, and Jinxiang Xi. 2022. "Olfactory Drug Aerosol Delivery with Acoustic Radiation" Biomedicines 10, no. 6: 1347. https://doi.org/10.3390/biomedicines10061347
APA StyleAbdollahzadeh Jamalabadi, M. Y., & Xi, J. (2022). Olfactory Drug Aerosol Delivery with Acoustic Radiation. Biomedicines, 10(6), 1347. https://doi.org/10.3390/biomedicines10061347