1. Introduction
Worldwide, prostate cancer was the third most common diagnosed malignancy in 2020 [
1]. The survival rates of prostate cancer are subject to the degree of metastasis. The five-year survival of localized prostate cancer is 100%, however, it falls rapidly to 31% in patients with distant metastases [
2].
In the last decade, new treatment options for patients with metastatic, castration resistant prostate cancer (mCRPC) became available, including novel androgen axis drugs (e.g., abiraterone, enzalutamide) and chemotherapy (i.e., docetaxel and cabazitaxel). More recently radioligand therapy with lutetium-177 prostate specific membrane antigen ([
177Lu]Lu-PSMA-617) emerged as a promising treatment for advanced prostate cancer [
3]. Several studies have demonstrated the safety and efficacy (extended overall survival and improved quality of life) of [
177Lu]Lu-PSMA-617 treatment in mCRPC patients [
3,
4,
5]. Although the majority (68%-75%) of the metastatic prostate cancer patients receiving [
177Lu]Lu-PSMA-617 treatment showed some degree of response, some did not benefit [
6].
Earlier studies mostly identified pre-therapeutic clinical and laboratory parameters for the prediction of treatment response (defined as prostate specific antigen (PSA) change) [
7,
8,
9]. Only a sparse literature exists on imaging-derived predictors (defined by pre-treatment with [
68Ga]Ga-PSMA-11 PET/CT), which has showed that low SUV
max and SUV
mean values were negative predictors for treatment response [
10,
11]. Unfortunately, these studies only evaluated treatment response on the patient-level by evaluating biochemical changes (PSA). The use of PSA reduction is the most commonly used in clinic due to its simplicity, however for response evaluation PSA is still under debate and cannot be used as response criterion in a per-lesion analysis [
12]. This study investigated whether imaging-derived factors on baseline [
68Ga]Ga-PSMA-11 PET/CT can potentially predict the response to [
177Lu]Lu-PSMA-617 treatment, in a lesion- and patient-level analysis, in men with mCRPC.
2. Materials and Methods
2.1. Population
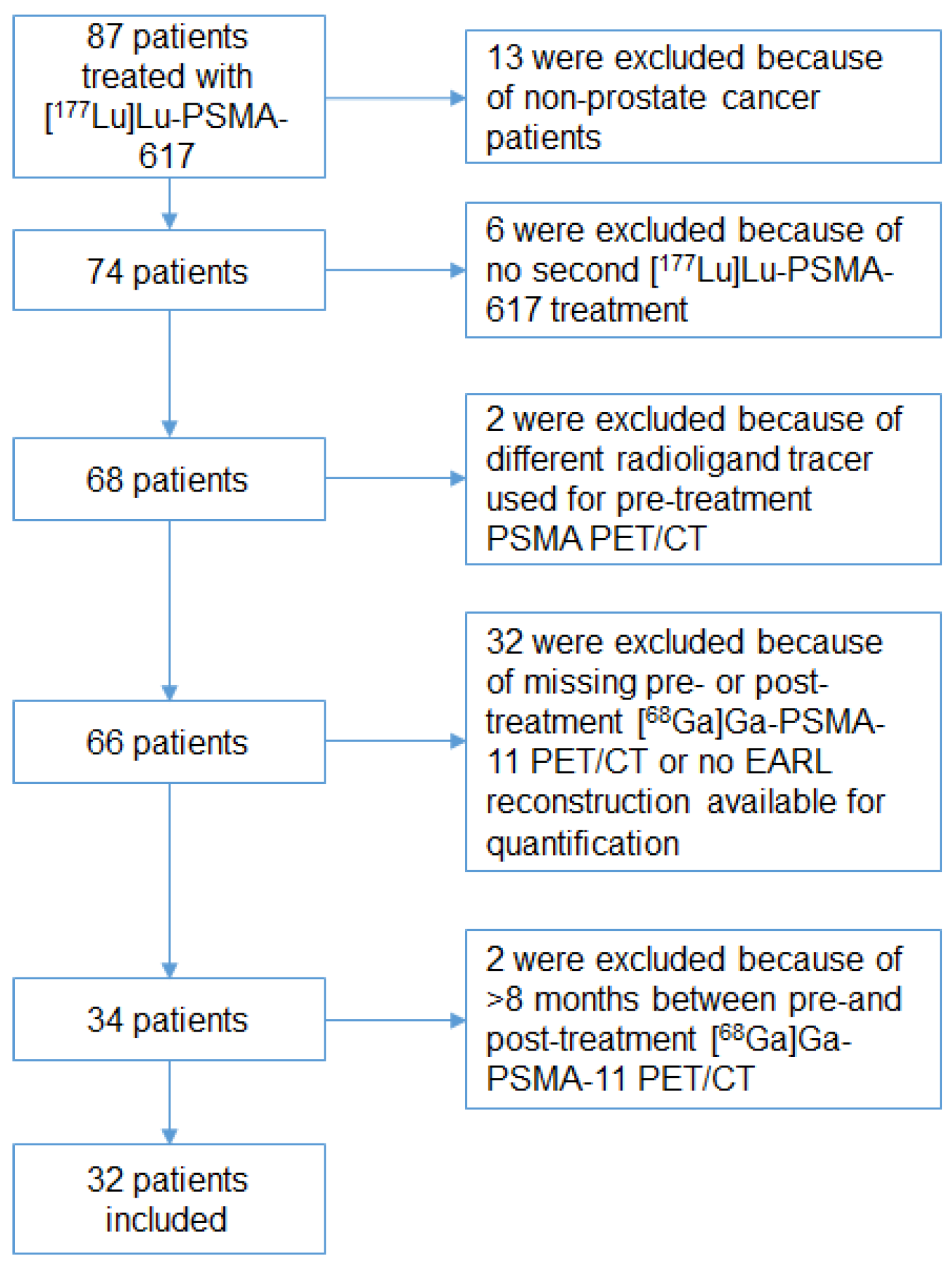
Patients referred for and treated with [
177Lu]Lu-PSMA-617 were identified retrospectively from a single center from March 2017 to November 2019. Patients were included if they had histologically proven mCRPC and had a [
68Ga]Ga-PSMA-11 PET/CT before and after two cycles of [
177Lu]Lu-PSMA-617 treatment. The reason why we choose to analyze after two cycles is based on the findings of Ahmadzadehfar et al., who showed that response (PSA decline ≥ 50%) is only or mostly seen after the second cycle of [
177Lu]Lu-PSMA-617 treatment [
13].
Patients were excluded if the interval between the baseline and post treatment [68Ga]Ga-PSMA-11 PET/CT was more than eight months. Blood testing was performed at the time of admission. The PSMA-617 ligand was obtained from ABX GmbH, Radeberg, Germany. A total of 6.0 or 7.4 GBq [177Lu]Lu-PSMA-617 per 40 to 250 μg peptide was administered intravenously for each cycle, with a planned interval of six weeks.
The need for informed consent was waived by the institutions medical ethics committee for this retrospective study.
2.2. Image Acquisition and Reconstruction
Sixty minutes after intravenous administration of 1.5–2.0 MBq/kg [68Ga]Ga-PSMA-11 the imaging was performed from the skull vertex to the mid-thigh (Biograph mCT scanner, Siemens, Erlangen, Germany).
The PET reconstruction was obtained following the EANM Research Ltd. (EARL), Vienna, Austria recommendations although its use for [
68Ga]Ga-PSMA-11 PET/CT interpretation has not been validated yet [
14,
15]. The [
68Ga]Ga-PSMA-11 accumulation was corrected for lean body mass (in SUV
lbm,peak*cm
3) [
16].
2.3. Imaging Analysis
Syngo.via-software (Siemens version 05.01, Erlangen, Germany) was used to establish quantitative image analysis. Based on PERCIST, relevant volumes of interest were (semi)automatically segmented if the standardized uptake value of peak (SUV
peak) was greater than the threshold set by a 3 cm cylindrical volume of interest (VOI) in the aorta with a threshold of 1.5 × aorta peak + 2 × standard deviation [
17]. The activity in the blood pool has been shown to be a well-grounded reference region for [
68Ga]Ga-PSMA-11 imaging interpretation [
18].
Manual adoption was needed if single tumor lesions and organs were not automatically divided based on the set PERCIST criteria.
Segmentations smaller than 0.3 mL where disregarded.
The Syngo.via software only allowed visual validation of a maximum of 50 lesions on the [68Ga]Ga-PSMA-11 PET/CT. It automatically calculated the total amount of [68Ga]Ga-PSMA-11 accumulation of the remaining lesions (>50).
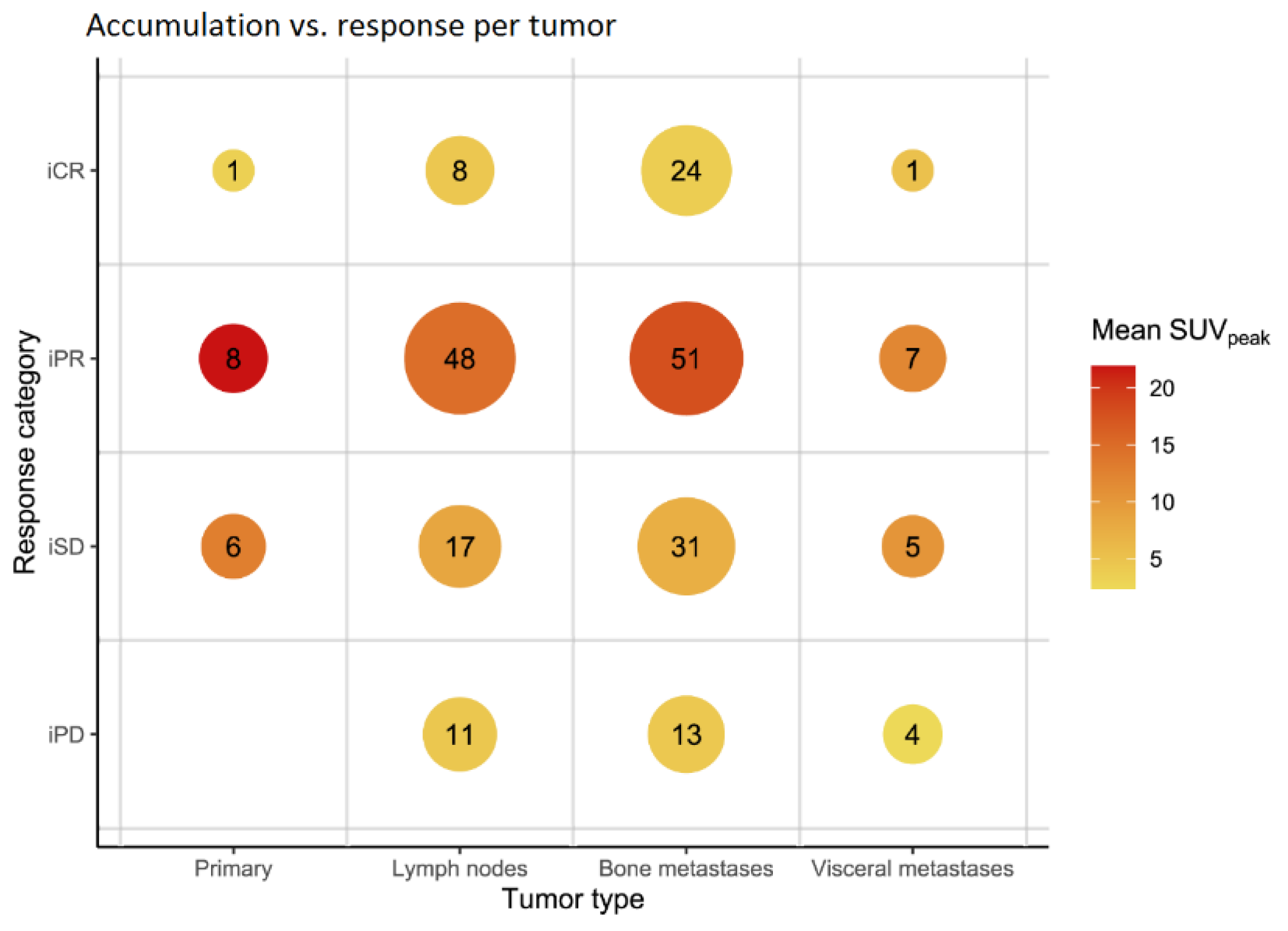
Parameters collected included PSMA tumor volume (PSMA-TV) in mL and TL-PSMA (summation of the entire tumor load within the patient derived from total lesion glycolysis (TLG)). The SUVpeak and SUVmax of the primary prostate tumor (if in situ), and the SUVpeak and SUVmax the two most- and least-avid lesions of three different organ categories (lymph nodes, bone and visceral metastasis) were collected. This approach was chosen in order to collect a wide variety of lesion avidity for the lesion-based analysis.
In accordance with the EARL recommendations, the TL-PSMA was calculated by multiplying the SUV
peak value with the PSMA-TV (SUV
lbm,peak*cm
3) per patient. Although the EARL recommendations are used for 18F-FDG (FDG), the used method for the total lesion glycolysis (TLG) will best represent the in vivo distribution of [
68Ga]Ga-PSMA-11 by calculating the fractional tumor activity [
19,
20,
21].
2.4. Outcomes
The primary outcome of this study was defined as an objective response after two cycles of [
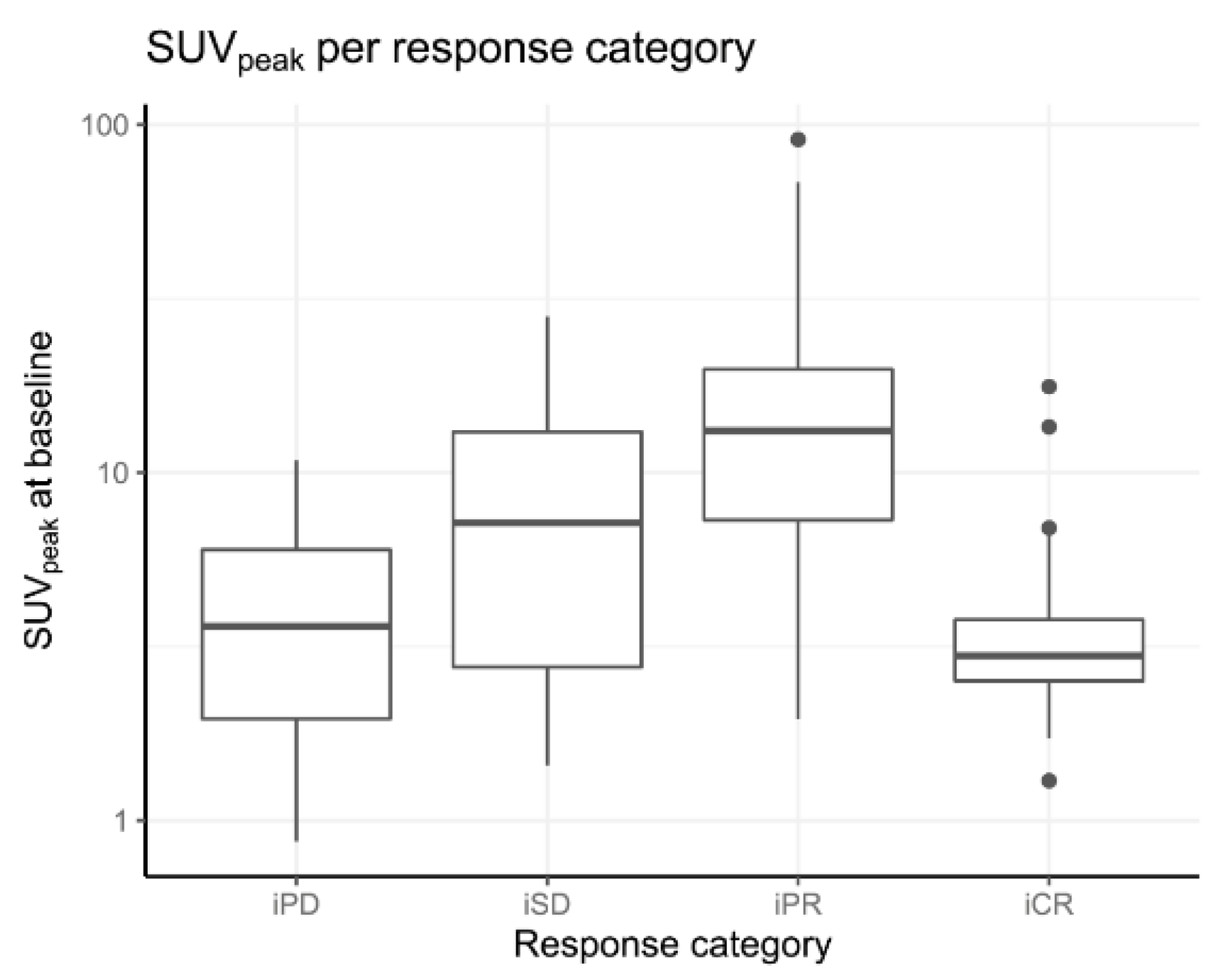
177Lu]Lu-PSMA-617 treatment at the lesion- and patient-level. Response evaluation at the lesion-level was based on PERCIST [
17]: imaging complete response (iCR); complete resolution of PSMA-tracer accumulation in all lesions, imaging partial response (iPR); more than or equal to 30% reduction of SUV
peak, imaging progressive disease (iPD); more than or equal to 30% increase in SUV
peak and imaging stable disease (iSD); not qualifying for iCR, iPR, or iPD. The definition of objective response includes iCR + iPR. For the patient-based analysis, the same methodology was used, except the TL-PSMA was used as the distinctive parameter instead of the SUV
peak, thus objective response at the patient-level was determined as a reduction of TL-PSMA ≥30% and progressive disease was defined as more than or equal to 30% increase in the TL-PSMA and/or the appearance of new lesions.
Secondary outcomes included a biochemical response after two cycles of [
177Lu]Lu-PSMA-617 treatment at the patient-level, defined according to the prostate cancer clinical trial working group 2 and 3 [
22,
23]. Response definitions: a partial response (bPR) was more than 50% PSA level reduction; progressive disease (bPD) was more than or equal to 25% increase; and a stable disease (bSD) was less or equal to 50% reduction and less than 25% increase of PSA level.
Additionally, clinical, biochemical, imaging, and hematological parameters (
Table 1 and
Table 2, and
Appendix A Table A1) were gathered to investigate potential predictive factors on a patient-level.
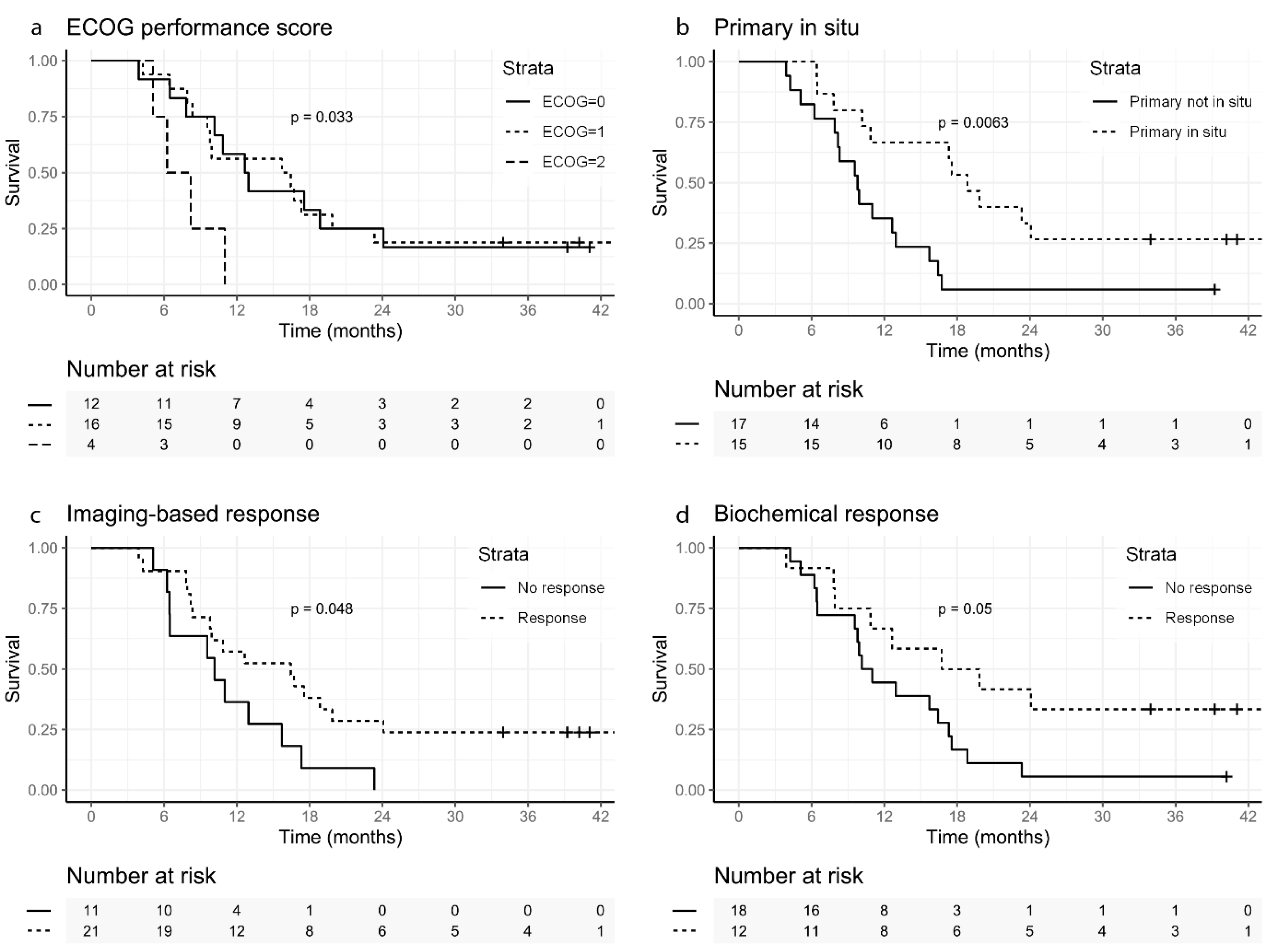
Finally, overall survival (OS), defined as after the first cycle of [177Lu]Lu-PSMA-617 treatment to death from any cause, was analyzed on a patient-level.
2.5. Statistical Analysis
The software IBM SPSS Statistics version 25.0.0.2 for Windows (IBM, Armonk, NY, USA) and R version 4.0.1 (R Core Team 2020) was used for all analyses (for used R codes see
Supplementary Materials). As accumulation measurements (i.e., SUV
peak and SUV
max) showed positive skewness, a log-transformation was applied before analyses were executed. Several types of analyses were executed to test different hypotheses. A
p-value ≤ 0.05 was considered significant.
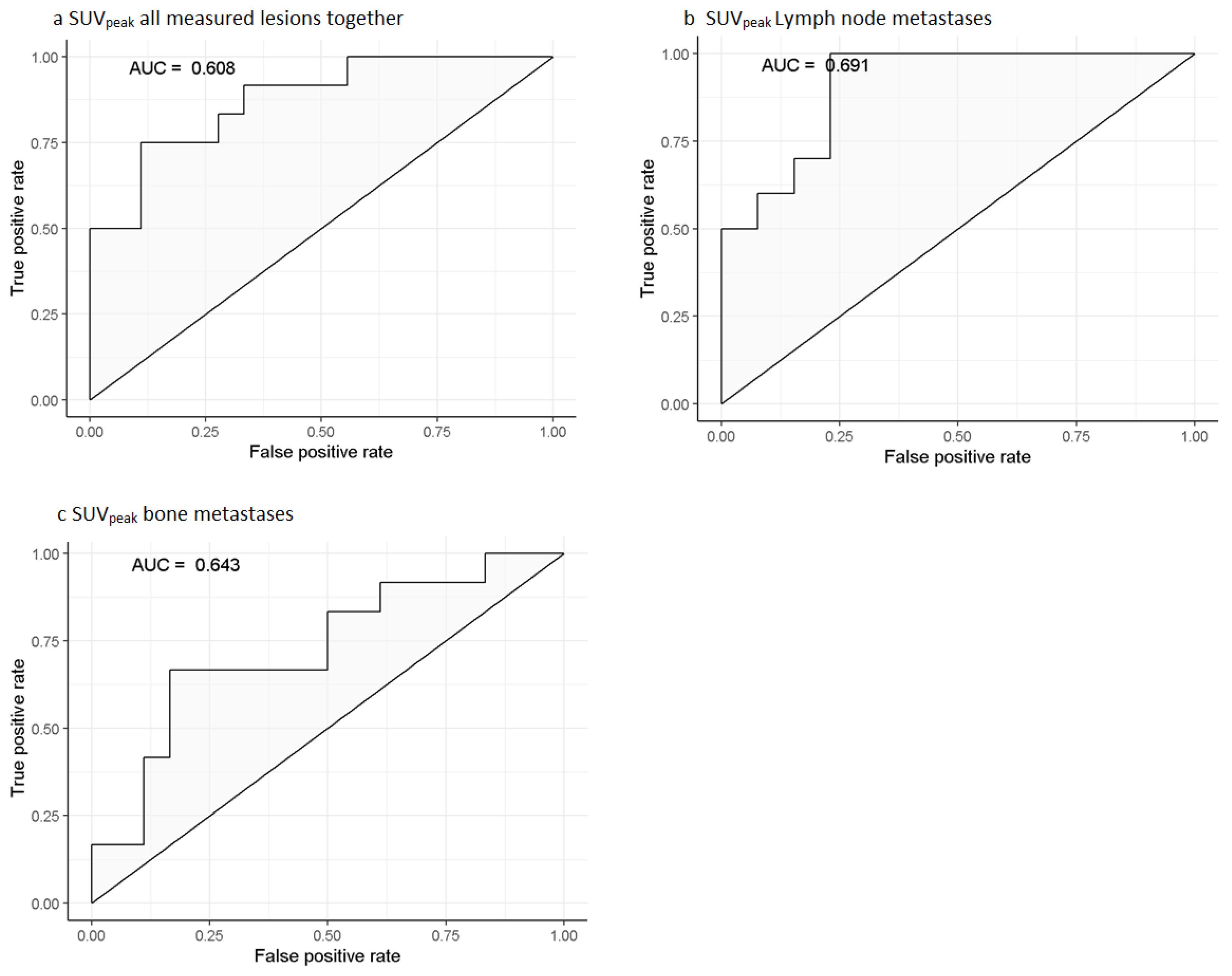
For our primary outcome, the imaging-based response on a lesion-level, Receiver Operating Characteristics (ROC) curve analyses were performed for predicting imaging-based response, including the following variables: SUVpeak/SUVmax all measured lesions together, SUVpeak/SUVmax lymph node metastases and bone metastases. The Youden’s index test and a set minimum specificity of 0.80 were used to determine the optimal cut-off value for binarization of the predictive values.
Mixed-effects models with SUVpeak/SUVmax as the independent variable, imaging-based response (dichotomized or as categorical variable) as the dependent variable, and a random intercept of SUVpeak and SUVmax per patient was used to model the effect of imaging-based response on the SUVpeak and SUVmax values. The random intercept was added to the model to incorporate the anticipated between-patient variation in SUVpeak and SUVmax levels. The remaining dependent relation between the imaging-based response and SUVpeak or SUVmax was then modelled as a fixed effect. PSMA-TV in the patient and metastasis type were added to the model as a confounder. In order to test the hypothesis that type of metastasis (i.e., lymph node, bone and visceral metastases) was of influence on the relationship between the individual pre-treatment accumulation and imaging-based response per lesion, metastasis type was added as an interaction to the model, both as a categorical variable and as a dichotomized variable in separate models.
For the imaging-based response on a patient-level, the maximum SUVpeak and SUVmax values in primary tumor or metastases (lymph node, bone, and visceral metastases) were tested for a relationship with response in logistic regression analysis. This approach was also used for the secondary outcome, biochemical response.
Several variables were tested in logistic regression analysis, univariately, while correcting for tumor load by including baseline PSMA-TV in each model. Each model was tested using likelihood ratio tests, comparing the model including the variable with a model only including baseline PSMA-TV.
Overall survival analysis was done using Cox-proportional hazard models, and Kaplan–Meier survival curves were constructed. The ISUP Gleason score, ECOG performance score, extent of disease, and imaging parameters were included in Cox-proportional hazard regression.
4. Discussion
This study evaluated the potential of imaging-derived factors on [68Ga]Ga-PSMA-11 PET/CT to predict the response in a lesion- and a patient-based analysis, in men with mCRPC receiving two cycles of [177Lu]Lu-PSMA-617 treatment. In the lesion-level analysis, a clear relationship was found between pre-therapeutic accumulation (SUVpeak and SUVmax) and imaging-based response on [68Ga]Ga-PSMA-11 PET/CT with no preference or difference for either, primary tumor, lymph node, bone or visceral metastasis.
Interestingly, in the lesion-level analysis, a contradictory lower SUVpeak at baseline was seen in lesions with iCR. An explanation might be the threshold method based on PERCIST and lesion selection criteria in this study. If, at follow-up imaging, the lesion SUVpeak was under the threshold, it was set to zero (being iCR), even when visually some accumulation might still be present. An additional explanation can be found in the set threshold and making the accumulation of the least avid lesion depended on the blood pool activity. However, to address a large number of lesions with a wide variety of intensities, this approach was deliberately chosen to gain more insight in lesion-based response. A third explanation is the influence of partial volume effect on small lesions, potentially overestimating objective response.
In the clinical setting, a difference was noticed in the objective response between different lesion types (e.g., prostate, lymph node, bone or visceral), however, the results of this study show no difference between lesion type (
Figure 4 and
Figure 5). Thus, making a distinction between lesion types seems irrelevant for patient selection prior to
177Lu-PSMA-617. To the best knowledge of the authors, this is the first study evaluating the response on individual lesion-level with imaging-derived predictive factors on [
68Ga]Ga-PSMA-11 PET/CT, thus no comparison with existing literature can be made.
On the patient-level, the pre-therapeutic imaging-derived predictive factor, SUV
peak of the most avid metastases was significantly associated with the imaging-based response (TL-PSMA ≥ 30% reduction). No other study has evaluated the imaging-based response based on PERCIST. Hofman et al. [
5] and Sartor et al. [
3], however, used the RECIST criteria, but in comparison to PERCIST (which looks at accumulation reduction); RECIST only uses single dimension size changes and has severe limitations in measuring bone or bone marrow disease [
17]. On the other hand, evaluating tumor response with [
68Ga]Ga-PSMA-11 PET/CT (via the same mechanism of the treatment itself) can also be debated, as potential non-PSMA avid disease will not be evaluated.
There are studies evaluating imaging-derived predictive factors with biochemical response as outcome, although the results are contradictory. Some did not find any significant imaging-derived predictive factor (e.g., SUV
max and SUV
mean, total tumor load, number of metastatic lesions, and sites of disease) for biochemical response [
11,
24], while some did (e.g., SUV
max < 45 of the most avid lesion, SUV
mean) [
10,
25]. An explanation can be found in the difference in the number of cycles used, population size, the used therapeutic radiopharmaceuticals, and the amount of activity, thereby making their results difficult to compare and to interpret.
In the survival analyses, patients with an ECOG performance score of zero and one had a significant better OS than patients with an ECOG performance score of two, in line with previous findings [
7]. Furthermore, patients with a biochemical response (>50% PSA reduction) had a better OS, compared to biochemical non-responders. This is in contrast to the findings of Ahmadzadehfar et al. [
7] and Rahbar et al. [
9], who did not find a significant difference in 100 and 104 mCRPC patients treated with [
177Lu]Lu-PSMA-617 between biochemical responders and non-responders concerning OS. The difference can possibly be explained by differences in sample size, population heterogeneity and selection bias by the range in the number of given [
177Lu]Lu-PSMA-617 cycles in both studies: namely two to six in this study versus one to eight cycles.
This study has several limitations: first, the retrospective design and resulting missing data. Second, the small sample size (
Figure 1) and population heterogeneity limits the ability to draw definite conclusions on patient-based analyses. But in the lesion-based analysis, the sample size was a total of 237 lesions, however, only the two most avid and two least avid lesions were selected to address many lesions with a wide variety of intensities, introducing a selection bias. Third, no volumes of the individual lesions were measured, introducing bias by partial volume effects. This could have influenced the response rate on the lesion-level analysis, as a lower PSMA-TV with the same SUV
peak is more prone for iCR than a higher PSMA-TV with the same SUV
peak. On the patient-level, however, baseline TL-PSMA and PSMA-TV had no significant influence on the imaging-based response rate. Fourth, PERCIST for the lesion-based response evaluation is not validated for PSMA PET/CT. However, it is already broadly available in clinical practice and easy to apply [
15,
17].
Other studies used a maximum intensity threshold with SUV
max for tumor segmentation [
20,
26]. In this study, we chose to use SUV
peak adapted from PERCIST for tumor segmentation as this limits the influence of noise on quantification [
27].
In current practice, patients are only eligible for [
177Lu]Lu-PSMA-617 treatment if sufficient tracer accumulation is observed on PSMA PET/CT. However, the definition of sufficient tracer accumulation is still a topic of discussion. Currently, it is based on literature on peptide receptor radionuclide therapy (PRRT), as was also used in the VISION trial [
28,
29,
30]: accumulation in tumor sites must at least be higher than physiological accumulation in normal liver tissue, to ensure a certain efficacy. The included patients in this study all met this specific criterion. Still, there were some non-responders (iPD and bPD) in this study (5/32; 16% and 5/30; 17%), in line with the findings in the VISION trial [
3], thereby indicating that the decision whether or not an individual patient is eligible for [
177Lu]Lu-PSMA-617 based on the visual assessment of accumulation alone compared to healthy liver tissue accumulation remains questionable. The results in this study indicate that tracer accumulation based on SUV
peak (>14.87) or SUV
max (>19.08) in a lesion can be helpful to determine if a certain lesion will or will not respond, based on a broadly available, internationally accredited image reconstruction method (EARL) [
14]. In case, when all or the majority of metastases within a patient are below these thresholds, an alternative treatment may be more beneficial, subsequently, improving patient selection for
177Lu-PSMA-617 based on available pre-treatment [
68Ga]Ga-PSMA-11 imaging.
The results of this study illustrate the potential of response prediction by pre-treatment [68Ga]Ga-PSMA-11 PET/CT quantification, using widely available image reconstruction parameters (EARL) and software packages enabling (semi-automated) PERCIST assessments. The findings of this study need to be validated in larger cohorts and future prospective studies.


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





