
The Impact of Treatment with IL-17/IL-23 Inhibitors on Subclinical Atherosclerosis in Patients with Plaque Psoriasis and/or Psoriatic Arthritis: A Systematic Review


 , ,
, ,
Abstract
:1. Introduction
2. Materials & Methods
2.1. Search Strategy and Eligibility Criteria
2.2. Selection Process and Data Extraction
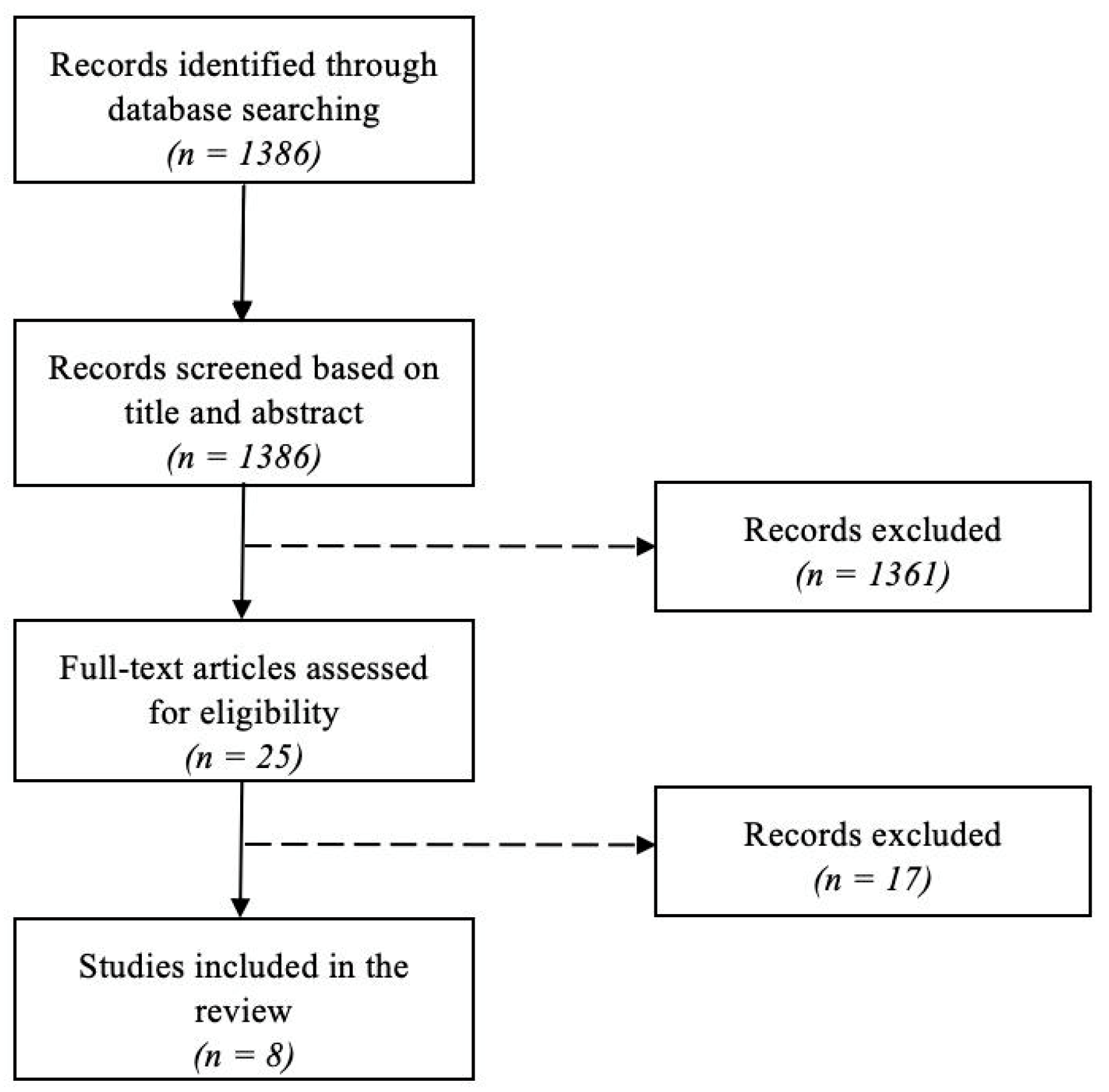
2.3. Study Selection
3. Results of Narrative Review
3.1. Diagnostic Evaluation of Subclinical Atherosclerosis in the Context of Psoriasis
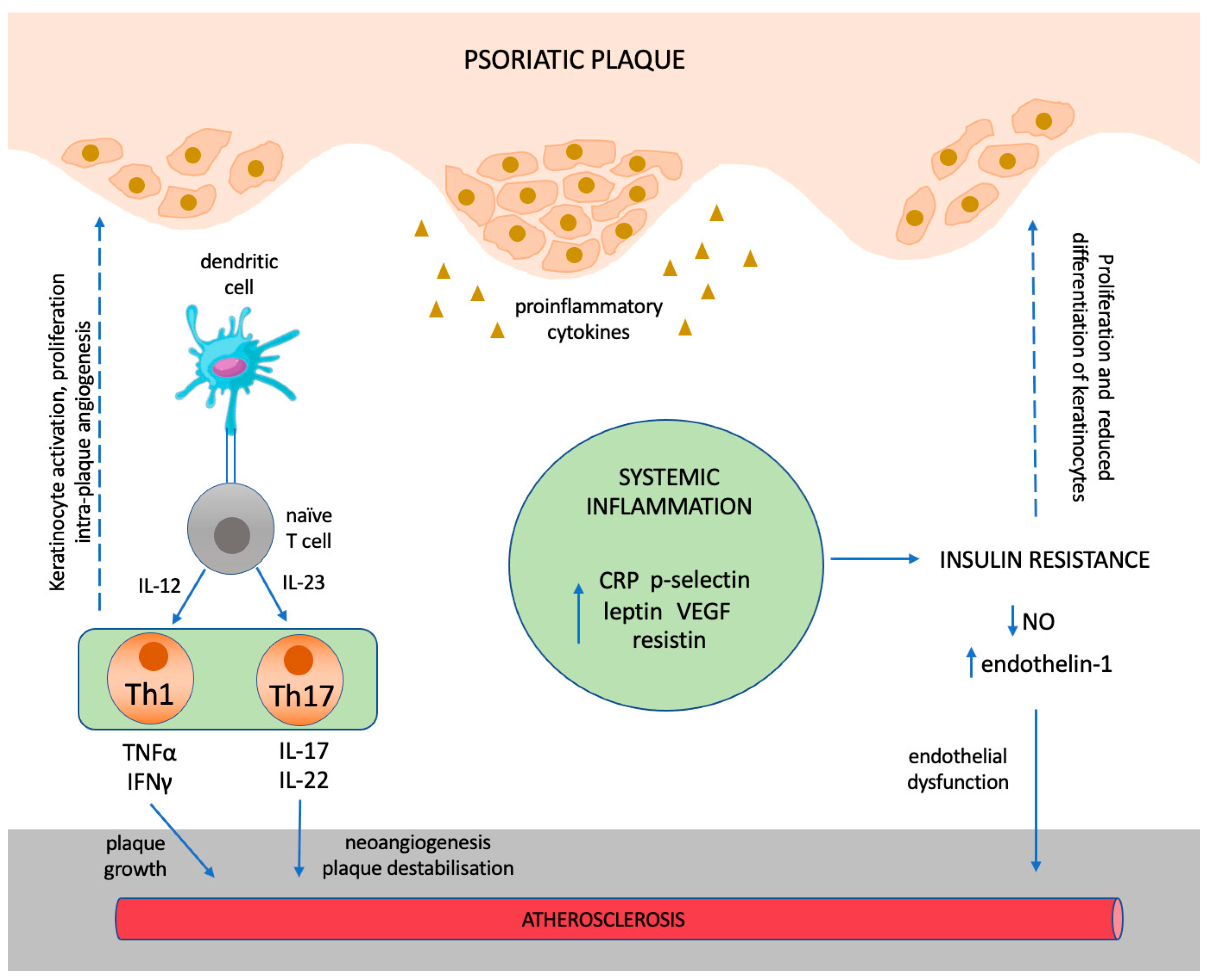
3.2. Shared Pathogenetic Mechanisms between Psoriasis and Atherosclerosis
3.2.1. The “Psoriatic March” Concept
3.2.2. Angiogenesis and Platelet Activation
3.2.3. The Involvement of Th1 and Th17 Immune Responses
4. Results of Systematic Search
Characteristics of Studies Assessing the Impact of Treatment with IL-17 and IL-23 Inhibitors on Subclinical Atherosclerosis in Patients with Psoriasis
5. Discussion and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reich, K. The concept of psoriasis as a systemic inflammation: Implications for disease management. J. Eur. Acad. Dermatol. Venereol. 2012, 26 (Suppl. S2), 3–11. [Google Scholar] [CrossRef] [PubMed]
- Lockshin, B.; Balagula, Y.; Merola, J.F. Interleukin 17, inflammation, and cardiovascular risk in patients with psoriasis. J. Am. Acad. Dermatol. 2018, 79, 345–352. [Google Scholar] [CrossRef] [Green Version]
- Gisondi, P.; Bellinato, F.; Girolomoni, G.; Albanesi, C. Pathogenesis of Chronic Plaque Psoriasis and Its Intersection with Cardio-Metabolic Comorbidities. Front. Pharmacol. 2020, 11, 117. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, H.; Abdulla, J.; Henningsen, K.M.; Skov, L.; Hansen, P.R. Coronary Artery Disease Assessed by Computed Tomography in Patients with Psoriasis: A Systematic Review and Meta-Analysis. Dermatology 2019, 235, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Fang, N.; Jiang, M.; Fan, Y. Association Between Psoriasis and Subclinical Atherosclerosis: A Meta-Analysis. Medicine 2016, 95, e3576. [Google Scholar] [CrossRef]
- Ghazizadeh, R.; Shimizu, H.; Tosa, M.; Ghazizadeh, M. Pathogenic Mechanisms Shared between Psoriasis and Cardiovascular Disease. Int. J. Med. Sci. 2010, 7, 284–289. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Moreno, A.; Ocampo-Candiani, J.; Garza-Rodriguez, V. Psoriasis and Cardiovascular Disease: A Narrative Review. Korean J. Fam. Med. 2021, 42, 345–355. [Google Scholar] [CrossRef]
- Lin, C.P.; Merola, J.F.; Wallace, E.B. Current and emerging biologic and small molecule systemic treatment options for psoriasis and psoriatic arthritis. Curr. Opin. Pharmacol. 2022, 67, 102292. [Google Scholar] [CrossRef]
- Megna, M.; Potestio, L.; Ruggiero, A.; Camela, E.; Fabbrocini, G. Guselkumab is efficacious and safe in psoriasis patients who failed anti-IL17: A 52-week real-life study. J. Dermatol. Treat. 2022, 33, 2560–2564. [Google Scholar] [CrossRef]
- Ruggiero, A.; Fabbrocini, G.; Cinelli, E.; Megna, M. Real world practice indirect comparison between guselkumab and risankizumab: Results from an Italian retrospective study. Dermatol. Ther. 2022, 35, e15214. [Google Scholar] [CrossRef]
- Megna, M.; Tommasino, N.; Potestio, L.; Battista, T.; Ruggiero, A.; Noto, M.; Fabbrocini, G.; Genco, L. Real-world practice indirect comparison between guselkumab, risankizumab, and tildrakizumab: Results from an Italian 28-week retrospective study. J. Dermatol. Treat. 2022, 33, 2813–2820. [Google Scholar] [CrossRef] [PubMed]
- Megna, M.; Potestio, L.; Ruggiero, A.; Camela, E.; Fabbrocini, G. Risankizumab treatment in psoriasis patients who failed anti-IL17: A 52-week real-life study. Dermatol. Ther. 2022, 35, e15524. [Google Scholar] [CrossRef] [PubMed]
- Dufour, J.; Hassan, M.; Netchiporouk, E.; Litvinov, I.V. Recent Advances in Evaluating Impact of Biologic Therapy for Moderate-Severe Psoriasis on Cardiovascular Events and Atherosclerotic Plaque Formation. J. Cutan. Med. Surg. 2020, 24, 209–210. [Google Scholar] [CrossRef] [PubMed]
- González-Cantero, A.; Ortega-Quijano, D.; Álvarez-Díaz, N.; Ballester, M.A.; Jimenez-Gomez, N.; Jaen, P.; González-Cantero, J.; González-Calvin, J.L.; Barderas, M.G.; Shin, D.B.; et al. Impact of Biological Agents on Imaging and Biomarkers of Cardiovascular Disease in Patients with Psoriasis: A Systematic Review and Meta-Analysis of Randomized Placebo-Controlled Trials. J. Investig. Dermatol. 2021, 141, 2402–2411. [Google Scholar] [CrossRef] [PubMed]
- Hjuler, K.F.; Bøttcher, M.; Vestergaard, C.; Bøtker, H.E.; Iversen, L.; Kragballe, K. Association Between Changes in Coronary Artery Disease Progression and Treatment with Biologic Agents for Severe Psoriasis. JAMA Dermatol. 2016, 152, 1114–1121. [Google Scholar] [CrossRef]
- Montaudié, H.; Albert-Sabonnadiere, C.; Acquacalda, E.; Fontas, E.; Danré, A.; Roux, C.; Ortonne, J.; Lacour, J.-P.; Euller-Ziegler, L.; Passeron, T. Impact of systemic treatment of psoriasis on inflammatory parameters and markers of comorbidities and cardiovascular risk: Results of a prospective longitudinal observational study. J. Eur. Acad. Dermatol. Venereol. 2013, 28, 1186–1191. [Google Scholar] [CrossRef]
- Mosca, M.; Hong, J.; Hadeler, E.; Hakimi, M.; Brownstone, N.; Liao, W.; Bhutani, T. Psoriasis and Cardiometabolic Comorbidities: An Evaluation of the Impact of Systemic Treatments in Randomized Clinical Trials. Dermatol. Ther. 2021, 11, 1497–1520. [Google Scholar] [CrossRef]
- Piaserico, S.; Osto, E.; Famoso, G.; Zanetti, I.; Gregori, D.; Poretto, A.; Iliceto, S.; Peserico, A.; Tona, F. Treatment with tumor necrosis factor inhibitors restores coronary microvascular function in young patients with severe psoriasis. Atherosclerosis 2016, 251, 25–30. [Google Scholar] [CrossRef]
- Pina, T.; Corrales, A.; Lopez-Mejias, R.; Armesto, S.; Gonzalez-Lopez, M.A.; Gómez-Acebo, I.; Ubilla, B.; Remuzgo-Martínez, S.; Gonzalez-Vela, M.C.; Blanco, R.; et al. Anti-tumor necrosis factor-alpha therapy improves endothelial function and arterial stiffness in patients with moderate to severe psoriasis: A 6-month prospective study. J. Dermatol. 2016, 43, 1267–1272. [Google Scholar] [CrossRef]
- Jókai, H.; Szakonyi, J.; Kontár, O.; Marschalkó, M.; Szalai, K.; Kárpáti, S.; Holló, P. Impact of effective tumor necrosis factor-alfa inhibitor treatment on arterial intima-media thickness in psoriasis: Results of a pilot study. J. Am. Acad. Dermatol. 2013, 69, 523–529. [Google Scholar] [CrossRef]
- Eder, L. TNFa inibitors are associated with reduced indices of subclinical atherosclerosis in patients with psoriatic disease. Arthritis Rheumatol. 2018, 38, 42–49. [Google Scholar]
- Herédi, E.; Végh, J.; Pogácsás, L.; Gáspár, K.; Varga, J.; Kincse, G.; Zeher, M.; Szegedi, A.; Gaál, J. Subclinical cardiovascular disease and it’s improvement after long-term TNF-α inhibitor therapy in severe psoriatic patients. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1531–1536. [Google Scholar] [CrossRef] [PubMed]
- Bissonnette, R.; Harel, F.; Krueger, J.G.; Guertin, M.-C.; Chabot-Blanchet, M.; Gonzalez, J.; Maari, C.; Delorme, I.; Lynde, C.W.; Tardif, J.-C. TNF-α Antagonist and Vascular Inflammation in Patients with Psoriasis Vulgaris: A Randomized Placebo-Controlled Study. J. Investig. Dermatol. 2017, 137, 1638–1645. [Google Scholar] [CrossRef] [PubMed]
- Elnabawi, Y.A.; Oikonomou, E.; Dey, A.K.; Mancio, J.; Rodante, J.A.; Aksentijevich, M.; Choi, H.; Keel, A.; Erb-Alvarez, J.; Teague, H.L.; et al. Association of Biologic Therapy with Coronary Inflammation in Patients with Psoriasis as Assessed by Perivascular Fat Attenuation Index. JAMA Cardiol. 2019, 4, 885–891. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.N.; Shin, D.B.; Joshi, A.A.; Dey, A.K.; Armstrong, A.W.; Duffin, K.C.; Fuxench, Z.C.; Harrington, C.L.; Hubbard, R.A.; Kalb, R.E.; et al. Effect of 2 Psoriasis Treatments on Vascular Inflammation and Novel Inflammatory Cardiovascular Biomarkers: A Randomized Placebo-Controlled Trial. Circ. Cardiovasc. Imaging 2018, 11, e007394. [Google Scholar] [CrossRef] [Green Version]
- Wegner, J.; Karbach, S.; Drosos, I.; Schnorbus, B.; Muxel, S.; Schmidt, F.; Wenzel, P.; Waisman, A.; Münzel, T.; Gori, T.; et al. TNF-α blockade may lead to improvement of vascular function in psoriasis patients. Exp. Dermatol. 2022, 31, 237–241. [Google Scholar] [CrossRef]
- Avgerinou, G.; Tousoulis, D.; Siasos, G.; Oikonomou, E.; Maniatis, K.; Papageorgiou, N.; Praskevopoulos, T.; Miliou, A.; Koumaki, D.; Latsios, G. Anti-tumor necrosis factor α treatment with adalimumab improves significantly endothelial function and decreases inflammatory process in patients with chronic psoriasis. Int. J. Cardiol. 2011, 151, 382–383. [Google Scholar] [CrossRef]
- Onsun, N.; Akaslan, T.Ç.; Sallahoglu, K.; Gülcan, A.S.; Bulut, H.; Yabacı, A. Effects of TNF inhibitors and an IL12/23 inhibitor on changes in body weight and adipokine levels in psoriasis patients: A 48-week comparative study. J. Dermatolog. Treat. 2022, 33, 1727–1732. [Google Scholar] [CrossRef]
- Knowles, L.; Nadeem, N.; Chowienczyk, P.J. Do anti-tumour necrosis factor-α biologics affect subclinical measures of atherosclerosis and arteriosclerosis? A systematic review. Br. J. Clin. Pharmacol. 2020, 86, 837–851. [Google Scholar] [CrossRef]
- Egeberg, A.; Gisondi, P.; Carrascosa, J.M.; Warren, R.B.; Mrowietz, U. The role of the interleukin-23/Th17 pathway in cardiometabolic comorbidity associated with psoriasis. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1695–1706. [Google Scholar] [CrossRef] [Green Version]
- Owczarczyk-Saczonek, A.; Placek, W. Interleukin-17 as a factor linking the pathogenesis of psoriasis with metabolic disorders. Int. J. Dermatol. 2017, 56, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zang, J.; Liu, C.; Yan, Z.; Shi, D. Interleukin-17 Links Inflammatory Cross-Talks Between Comorbid Psoriasis and Atherosclerosis. Front. Immunol. 2022, 13, 835671. [Google Scholar] [CrossRef] [PubMed]
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of Cardiovascular Events and All-Cause Mortality with Arterial Stiffness: A Systematic Review and Meta-Analysis. J. Am. Coll. Cardiol. 2010, 55, 1318–1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gisondi, P.; Fantin, F.; Del Giglio, M.; Valbusa, F.; Marino, F.; Zamboni, M.; Girolomoni, G. Chronic Plaque Psoriasis Is Associated with Increased Arterial Stiffness. Dermatology 2009, 218, 110–113. [Google Scholar] [CrossRef]
- Gonzalez-Juanatey, C.; Llorca, J.; Miranda-Filloy, J.A.; Amigo-Diaz, E.; Testa, A.; Garcia-Porrua, C.; Martin, J.; Gonzalez-Gay, M.A. Endothelial dysfunction in psoriatic arthritis patients without clinically evident cardiovascular disease or classic atherosclerosis risk factors. Arthritis Rheum. 2007, 57, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Moroni, L.; Selmi, C.; Angelini, C.; Meroni, P.L. Evaluation of Endothelial Function by Flow-Mediated Dilation: A Comprehensive Review in Rheumatic Disease. Arch. Immunol. Ther. Exp. 2017, 65, 463–475. [Google Scholar] [CrossRef]
- Inaba, Y.; Chen, J.A.; Bergmann, S.R. Prediction of future cardiovascular outcomes by flow-mediated vasodilatation of brachial artery: A meta-analysis. Int. J. Cardiovasc. Imaging 2010, 26, 631–640. [Google Scholar] [CrossRef]
- Martinez-Lopez, A.; Blasco-Morente, G.; Perez-Lopez, I.; Tercedor-Sanchez, J.; Arias-Santiago, S. Studying the effect of systemic and biological drugs on intima-media thickness in patients suffering from moderate and severe psoriasis. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1492–1498. [Google Scholar] [CrossRef]
- Balci, D.; Balci, A.; Karazincir, S.; Ucar, E.; Iyigun, U.; Yalcin, F.; Seyfeli, E.; Inandi, T.; Egilmez, E. Increased carotid artery intima-media thickness and impaired endothelial function in psoriasis. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 1–6. [Google Scholar] [CrossRef]
- Bulbul Sen, B.; Atci, N.; Rifaioglu, E.N.; Ekiz, O.; Kartal, I.; Buyukkaya, E.; Kurt, M.; Karakas, M.F.; Buyukkaya, S.; Akcay, A.B.; et al. Increased epicardial fat tissue is a marker of subclinical atherosclerosis in patients with psoriasis. Br. J. Dermatol. 2013, 169, 1081–1086. [Google Scholar] [CrossRef]
- Dey, A.K.; Joshi, A.A.; Chaturvedi, A.; Lerman, J.B.; Aberra, T.M.; Rodante, J.A.; Teague, H.L.; Harrington, C.L.; Rivers, J.P.; Chung, J.H.; et al. Association Between Skin and Aortic Vascular Inflammation in Patients with Psoriasis: A Case-Cohort Study Using Positron Emission Tomography/Computed Tomography. JAMA Cardiol. 2017, 2, 1013–1018. [Google Scholar] [CrossRef] [PubMed]
- Bissonnette, R.; Tardif, J.C.; Harel, F.; Pressacco, J.; Bolduc, C.; Guertin, M.C. Effects of the tumor necrosis factor-α antagonist adalimumab on arterial inflammation assessed by positron emission tomography in patients with psoriasis: Results of a randomized controlled trial. Circ. Cardiovasc. Imaging 2013, 6, 83–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groenendyk, J.W.; Shukla, P.; Dey, A.K.; Elnabawi, Y.A.; Aksentijevich, M.; Choi, H.; Genovese, L.D.; Harrington, C.L.; Natarajan, B.; Goyal, A.; et al. Association of aortic vascular uptake of 18FDG by PET/CT and aortic wall thickness by MRI in psoriasis: A prospective observational study. Eur. J. Nucl. Med. 2019, 46, 2488–2495. [Google Scholar] [CrossRef] [PubMed]
- Rumberger, J. Using noncontrast cardiac CT and coronary artery calcification measurements for cardiovascular risk assessment and management in asymptomatic adults. Vasc. Health Risk Manag. 2010, 6, 579–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borsky, P.; Fiala, Z.; Andrys, C.; Beranek, M.; Hamakova, K.; Kremlacek, J.; Malkova, A.; Svadlakova, T.; Krejsek, J.; Palicka, V.; et al. C-reactive protein, chemerin, fetuin-A and osteopontin as predictors of cardiovascular risks in persons with Psoriasis Vulgaris. Physiol. Res. 2021, 70, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Campanati, A.; Ganzetti, G.; Giuliodori, K.; Marra, M.; Bonfigli, A.; Testa, R.; Offidani, A. Serum levels of adipocytokines in psoriasis patients receiving tumor necrosis factor-α inhibitors: Results of a retrospective analysis. Int. J. Dermatol. 2015, 54, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Awad, S.M.; Attallah, D.A.; Salama, R.H.; Mahran, A.M.; Abu El-Hamed, E. Serum levels of psoriasin (S100A7) and koebnerisin (S100A15) as potential markers of atherosclerosis in patients with psoriasis. Clin. Exp. Dermatol. 2018, 43, 262–267. [Google Scholar] [CrossRef]
- Dey, A.K.; Gaddipati, R.; Elnabawi, Y.A.; Ongstad, E.; Goyal, A.; Chung, J.H.; Teague, H.L.; Rodante, J.A.; Sajja, A.A.; Sorokin, A.V.; et al. Association Between Soluble Lectinlike Oxidized Low-Density Lipoprotein Receptor-1 and Coronary Artery Disease in Psoriasis. JAMA Dermatol. 2020, 156, 151–157. [Google Scholar] [CrossRef]
- Niknezhad, N.; Haghighatkhah, H.R.; Zargari, O.; Ghalamkarpour, F.; Younespour, S.; Niknejad, N.; Alikhan, A.; Abdollahimajd, F. High-sensitivity C-reactive protein as a biomarker in detecting subclinical atherosclerosis in psoriasis. Dermatol. Ther. 2020, 33, e13628. [Google Scholar] [CrossRef]
- Pietrzak, A.; Bartosinska, J.; Blaszczyk, R.; Chodorowska, G.; Brzozowski, W.; Hercogova, J.; Donica, H.; Lotti, T. Increased serum level of N-terminal Pro-B-type natriuretic peptide as a possible biomarker of cardiovascular risk in psoriatic patients. J. Eur. Acad. Dermatol. Venereol. 2014, 29, 1010–1014. [Google Scholar] [CrossRef]
- Demirbaş, A.; Kurtipek, G.S.; Tunçez, A.; Akyürek, F.; Demirbaş, G.U. The role of cystatin-C and fetuin-A in the determination of early atherosclerotic risk in psoriasis patients. Dermatol. Ther. 2020, 33, e13898. [Google Scholar] [CrossRef] [PubMed]
- Balta, I.; Balta, S.; Demirkol, S.; Mikhailidis, D.; Celik, T.; Akhan, M.; Kurt, O.; Kurt, Y.; Aydin, I.; Kilic, S. Elevated serum levels of endocan in patients with psoriasis vulgaris: Correlations with cardiovascular risk and activity of disease. Br. J. Dermatol. 2013, 169, 1066–1070. [Google Scholar] [CrossRef] [PubMed]
- Balta, S.; Balta, I.; Mikhailidis, D.P.; Ozturk, C.; Demirkol, S.; Celik, T.; Kilic, S.; Demir, M.; Iyisoy, A. Bilirubin Levels and Their Association with Carotid Intima Media Thickness and High-Sensitivity C-reactive Protein in Patients with Psoriasis Vulgaris. Am. J. Clin. Dermatol. 2014, 15, 137–142. [Google Scholar] [CrossRef]
- Erfan, G.; Guzel, S.; Alpsoy, S.; Rifaioglu, E.N.; Kaya, S.; Kucukyalcın, V.; Topcu, B.; Kulac, M. Serum YKL-40: A potential biomarker for psoriasis or endothelial dysfunction in psoriasis? Mol. Cell Biochem. 2015, 400, 207–212. [Google Scholar] [CrossRef]
- Erturan, I.; Köroğlu, B.K.; Adiloğlu, A.; Ceyhan, A.M.; Akkaya, V.B.; Tamer, N.; Başak, P.Y.; Korkmaz, S.; Ersoy, I.H.; Kılınç, O. Evaluation of serum sCD40L and homocysteine levels with subclinical atherosclerosis indicators in patients with psoriasis: A pilot study. Int. J. Dermatol. 2014, 53, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.A.; Lerman, J.B.; Aberra, T.M.; Afshar, M.; Teague, H.L.; Rodante, J.A.; Krishnamoorthy, P.; Ng, Q.; Aridi, T.Z.; Salahuddin, T.; et al. GlycA Is a Novel Biomarker of Inflammation and Subclinical Cardiovascular Disease in Psoriasis. Circ. Res. 2016, 119, 1242–1253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaiser, H.; Wang, X.; Kvist-Hansen, A.; Krakauer, M.; Gørtz, P.M.; McCauley, B.D.; Skov, L.; Becker, C.; Hansen, P.R. Biomarkers of subclinical atherosclerosis in patients with psoriasis. Sci. Rep. 2021, 11, 21438. [Google Scholar] [CrossRef]
- Kyriakou, A.; Patsatsi, A.; Sotiriadis, D.; Goulis, D. Effects of treatment for psoriasis on circulating levels of leptin, adiponectin and resistin: A systematic review and meta-analysis. Br. J. Dermatol. 2018, 179, 273–281. [Google Scholar] [CrossRef]
- Boehncke, W.-H.; Boehncke, S.; Tobin, A.-M.; Kirby, B. The “psoriatic march”: A concept of how severe psoriasis may drive cardiovascular comorbidity. Exp. Dermatol. 2011, 20, 303–307. [Google Scholar] [CrossRef]
- Shahidi-Dadras, M.; Haghighatkhah, H.R.; Abdollahimajd, F.; Younespour, S.; Kia, M.P.; Zargari, O. Correlation between vascular endothelial growth factor and subclinical atherosclerosis in patients with psoriasis. Int. J. Dermatol. 2016, 55, 52–59. [Google Scholar] [CrossRef]
- Saleh, H.M.A.; Attia, E.A.S.; Onsy, A.M.; Saad, A.A.; Abd Ellah, M.M.M. Platelet activation: A link between psoriasis per se and subclinical atherosclerosis—A case-control study. Br. J. Dermatol. 2013, 169, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.A.; Montagnani, M.; Kwang, K.K.; Quon, M.J. Reciprocal relationships between insulin resistance and endothelial dysfunction: Molecular and pathophysiological mechanisms. Circulation 2006, 113, 1888–1904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansson, G.K. Inflammation, atherosclerosis, and coronary artery disease. N. Engl. J. Med. 2005, 352, 1685–1695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purzycka-Bohdan, D.; Kisielnicka, A.; Bohdan, M.; Szczerkowska-Dobosz, A.; Sobalska-Kwapis, M.; Nedoszytko, B.; Nowicki, R.J. Analysis of the Potential Genetic Links between Psoriasis and Cardiovascular Risk Factors. Int. J. Mol. Sci. 2021, 22, 9063. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.; Levine, P.H.; Fullerton, A.L.; Forsberg, A.; Duffy, C.P.; Hoogasian, J.J.; Drachman, D.A. Marker Proteins of Platelet Activation in Patients with Cerebrovascular Disease. Arch. Neurol. 1982, 39, 692–695. [Google Scholar] [CrossRef] [PubMed]
- Garbaraviciene, J.; Diehl, S.; Varwig, D.; Bylaite, M.; Ackermann, H.; Ludwig, R.J.; Boehncke, W.-H. Platelet P-selectin reflects a state of cutaneous inflammation: Possible application to monitor treatment efficacy in psoriasis. Exp. Dermatol. 2010, 19, 736–741. [Google Scholar] [CrossRef]
- Von Stebut, E.; Boehncke, W.-H.; Ghoreschi, K.; Gori, T.; Kaya, Z.; Thaci, D.; Schäffler, A. IL-17A in Psoriasis and Beyond: Cardiovascular and Metabolic Implications. Front. Immunol. 2019, 10, 3096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Kaiser, H.; Kvist-Hansen, A.; McCauley, B.D.; Skov, L.; Hansen, P.R.; Becker, C. IL-17 Pathway Members as Potential Biomarkers of Effective Systemic Treatment and Cardiovascular Disease in Patients with Moderate-to-Severe Psoriasis. Int. J. Mol. Sci. 2022, 23, 555. [Google Scholar] [CrossRef]
- Robert, M.; Miossec, P.; Hot, A. The Th17 Pathway in Vascular Inflammation: Culprit or Consort? Front. Immunol. 2022, 13, 888763. [Google Scholar] [CrossRef]
- Simon, T.; Taleb, S.; Danchin, N.; Laurans, L.; Rousseau, B.; Cattan, S.; Montely, J.-M.; Dubourg, O.; Tedgui, A.; Kotti, S.; et al. Circulating levels of interleukin-17 and cardiovascular outcomes in patients with acute myocardial infarction. Eur. Heart J. 2013, 34, 570–577. [Google Scholar] [CrossRef] [Green Version]
- Valaiyaduppu Subas, S.; Mishra, V.; Busa, V.; Antony, I.; Marudhai, S.; Patel, M.; Cancarevic, I. Cardiovascular Involvement in Psoriasis, Diagnosing Subclinical Atherosclerosis, Effects of Biological and Non-Biological Therapy: A Literature Review. Cureus 2020, 12, e11173. [Google Scholar] [CrossRef]
- Gisterå, A.; Robertson, A.-K.L.; Andersson, J.; Ketelhuth, D.F.J.; Ovchinnikova, O.; Nilsson, S.K.; Lundberg, A.M.; Li, M.O.; Flavell, R.A.; Hansson, G.K. Transforming Growth Factor–β Signaling in T Cells Promotes Stabilization of Atherosclerotic Plaques Through an Interleukin-17–Dependent Pathway. Sci. Transl. Med. 2013, 5, 196ra100. [Google Scholar] [CrossRef]
- Gao, Q.; Jiang, Y.; Ma, T.; Zhu, F.; Gao, F.; Zhang, P.; Guo, C.; Wang, Q.; Wang, X.; Ma, C.; et al. A Critical Function of Th17 Proinflammatory Cells in the Development of Atherosclerotic Plaque in Mice. J. Immunol. 2010, 185, 5820–5827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slominski, A.T.; Kim, T.K.; Takeda, Y.; Janjetovic, Z.; Brozyna, A.A.; Skobowiat, C.; Wang, J.; Postlethwaite, A.; Li, W.; Tuckey, R.C.; et al. RORα and RORγ are expressed in human skin and serve as receptors for endogenously produced noncalcemic 20-hydroxy- and 20,23-dihydroxyvitamin D. FASEB J. 2014, 28, 2775–2789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campione, E.; Cosio, T.; Di Prete, M.; Lanna, C.; Dattola, A.; Bianchi, L. Experimental Pharmacological Management of Psoriasis. J. Exp. Pharmacol. 2021, 13, 725–737. [Google Scholar] [CrossRef] [PubMed]
- Brożyna, A.A.; Żmijewski, M.A.; Linowiecka, K.; Kim, T.; Slominski, R.M.; Slominski, A.T. Disturbed expression of vitamin D and retinoic acid-related orphan receptors α and γ and of megalin in inflammatory skin diseases. Exp. Dermatol. 2022, 31, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Uceda, D.E.; Dey, A.K.; Abdelrahman, K.M.; Aksentijevich, M.; Rodante, J.A.; Elnabawyi, Y.A.; Reddy, A.; Keel, A.; Erb-Alvarez, J.; et al. Treatment of Psoriasis with Biologic Therapy Is Associated with Improvement of Coronary Artery Plaque Lipid-Rich Necrotic Core: Results from a Prospective, Observational Study. Circ. Cardiovasc. Imaging 2020, 13, e011199. [Google Scholar] [CrossRef]
- Elnabawi, A.Y.; Dey, A.K.; Goyal, A.; Groenendyk, J.W.; Chung, J.H.; Belur, A.D.; Rodante, J.; Harrington, C.L.; Teague, H.L.; Baumer, Y.; et al. Coronary artery plaque characteristics and treatment with biologic therapy in severe psoriasis: Results from a prospective observational study. Cardiovasc. Res. 2019, 115, 721–728. [Google Scholar] [CrossRef]
- Gelfand, J.M.; Shin, D.B.; Duffin, K.C.; Armstrong, A.W.; Blauvelt, A.; Tyring, S.K.; Menter, A.; Gottlieb, S.; Lockshin, B.N.; Simpson, E.L.; et al. A Randomized Placebo-Controlled Trial of Secukinumab on Aortic Vascular Inflammation in Moderate-to-Severe Plaque Psoriasis (VIP-S). J. Investig. Dermatol. 2020, 140, 1784–1793. [Google Scholar] [CrossRef]
- Makavos, G.; Ikonomidis, I.; Andreadou, I.; Varoudi, M.; Kapniari, I.; Loukeri, E.; Theodoropoulos, K.; Pavlidis, G.; Triantafyllidi, H.; Thymis, J.; et al. Effects of Interleukin 17A Inhibition on Myocardial Deformation and Vascular Function in Psoriasis. Can. J. Cardiol. 2020, 36, 100–111. [Google Scholar] [CrossRef]
- Marovt, M.; Marko, P.B.; Pirnat, M.; Ekart, R. Effect of biologics targeting interleukin-23/-17 axis on subclinical atherosclerosis: Results of a pilot study. Clin. Exp. Dermatol. 2020, 45, 560–564. [Google Scholar] [CrossRef] [PubMed]
- Piros, É.A.; Szabó, Á.; Rencz, F.; Brodszky, V.; Szalai, K.; Galajda, N.; Szilveszter, B.; Dósa, E.; Merkely, B.; Holló, P. Impact of Interleukin-17 Inhibitor Therapy on Arterial Intima-media Thickness among Severe Psoriatic Patients. Life 2021, 11, 919. [Google Scholar] [CrossRef] [PubMed]
- Von Stebut, E.; Reich, K.; Thaçi, D.; Koenig, W.; Pinter, A.; Körber, A.; Rassaf, T.; Waisman, A.; Mani, V.; Yates, D.; et al. Impact of Secukinumab on Endothelial Dysfunction and Other Cardiovascular Disease Parameters in Psoriasis Patients over 52 Weeks. J. Investig. Dermatol. 2019, 139, 1054–1062. [Google Scholar] [CrossRef] [Green Version]
- Kamata, M.; Tada, Y. Efficacy and Safety of Biologics for Psoriasis and Psoriatic Arthritis and Their Impact on Comorbidities: A Literature Review. Int. J. Mol. Sci. 2020, 21, 1690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerdes, S.; Pinter, A.; Papavassilis, C.; Reinhardt, M. Effects of secukinumab on metabolic and liver parameters in plaque psoriasis patients. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 533–541. [Google Scholar] [CrossRef] [Green Version]
- Lebwohl, M. Does Treatment of Psoriasis Reduce Cardiovascular Comorbidities? J. Investig. Dermatol. 2017, 137, 1612–1613. [Google Scholar] [CrossRef]
- Marsche, G.; Holzer, M.; Wolf, P. Antipsoriatic treatment extends beyond the skin: Recovering of high-density lipoprotein function. Exp. Dermatol. 2014, 23, 701–704. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.N.; Huang, Y.H. Changes in metabolic parameters in psoriatic patients treated with secukinumab. Ther. Adv. Chronic Dis. 2020, 11, 2040622320944777. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.; Leonardi, C.L.; Krueger, J.G.; Kimball, A.B.; Strober, B.E.; Gordon, K.B.; Langley, R.G.; de Lemos, J.A.; Daoud, Y.; Blankenship, D.; et al. Association between biologic therapies for chronic plaque psoriasis and cardiovascular events: A meta-analysis of randomized controlled trials. JAMA 2011, 306, 864–871. [Google Scholar] [CrossRef]
- Poizeau, F.; Nowak, E.; Kerbrat, S.; Le Nautout, B.; Droitcourt, C.; Drici, M.D.; Sbidian, E.; Guillot, B.; Bachelez, H.; Ait-Oufella, H.; et al. Association Between Early Severe Cardiovascular Events and the Initiation of Treatment with the Anti-Interleukin 12/23p40 Antibody Ustekinumab. JAMA Dermatol. 2020, 156, 1208–1215. [Google Scholar] [CrossRef]
- Kleinrensink, N.J.; Pouw, J.N.; Leijten, E.F.A.; Takx, R.A.P.; Welsing, P.M.J.; de Keizer, B.; Jong, P.A.; Foppen, B. Increased vascular inflammation on PET/CT in psoriasis and the effect of biologic treatment: Systematic review and meta-analysis. Clin. Transl. Imaging 2022, 10, 225–235. [Google Scholar] [CrossRef]
- Nast, A.; Smith, C.; Spuls, P.I.; Valle, G.A.; Bata-Csörgö, Z.; Boonen, H.; De Jong, E.; Garcia-Doval, I.; Gisondi, P.; Kaur-Knudsen, D.; et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis Vulgaris—Part 1: Treatment and monitoring recommendations. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2461–2498. [Google Scholar] [CrossRef] [PubMed]
- Nast, A.; Smith, C.; Spuls, P.I.; Valle, G.A.; Bata-Csörgö, Z.; Boonen, H.; De Jong, E.; Garcia-Doval, I.; Gisondi, P.; Kaur-Knudsen, D.; et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis Vulgaris—Part 2: Specific clinical and comorbid situations. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 281–317. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Search Terms | Results |
|---|---|
| Cardiovascular | 2,051,829 |
| Coronary disease | 355,309 |
| Atherosclerosis | 165,432 |
| Cardiovascular OR coronary disease OR atherosclerosis | 2,286,796 |
| Psoriasis | 59,808 |
| Psoriatic arthritis | 12,928 |
| psoriasis OR psoriatic arthritis | 62,289 |
| Biologics | 7,336,51 |
| Interleukin 17 inhibitor | 2846 |
| Interleukin 23 inhibitor | 1077 |
| Secukinumab | 1734 |
| Brodalumab | 473 |
| Ixekizumab | 875 |
| Guselkumab | 473 |
| Rizankizumab | 296 |
| Biologics OR interleukin 17 inhibitor OR interleukin 23 inhibitor OR secukinumab OR brodalumab OR ixekizumab OR guselkumab OR rizankizumab | 7,337,887 |
| (cardiovascular OR atherosclerosis OR coronary disease) AND (psoriasis OR psoriatic arthritis) AND (biologics OR interleukin 17 inhibitor OR interleukin 23 inhibitor OR secukinumab OR brodalumab OR ixekizumab OR guselkumab OR rizankizumab) | 1386 |
| Marker | Diagnostic Method | Comments |
|---|---|---|
| Assessment of functional alterations | ||
| Pulse wave velocity | High resolution B-mode ultrasound | Gold standard measurement of arterial stiffness |
| Flow-mediated dilatation | High resolution B-mode ultrasound | assesses stimulus-activated (mainly nitric oxide-dependent) vasodilation, normally performed in the brachial artery, some studies have also used the radial and femoral arteries |
| Assessment of structural alterations | ||
| Intima media thickness | High resolution B-mode ultrasound | -carotid, branchial, femoral (more informative), thickening of the intima precedes the development of plaque and stenosis |
| Coronary artery calcium (CAC score) | Non-contrast coronary artery calcium CT | Measures the amount of calcium in coronary arteries, indicates cardiovascular disease, assists in cardiovascular risk assessment |
| Coronary plaque characterization | Coronary CTA | e.g., total coronary plaque burden, non-calcified coronary plaque burden, high risk plaque prevalence |
| Lipid-rich necrotic core | Coronary CTA | High risk coronary plaque feature, histopathologic correlate of low-attenuation plaque |
| Perivascular fat attenuation index | Coronary CTA | Quantification of coronary inflammation, may predict the risk of developing atherosclerosis |
| Aortic vascular inflammation | FDG PET scan | Marker of subclinical vascular disease, predictive of future major cardiovascular events |
| Epicardial fat thickness | Native CT, MRI, TTE | Epicardial adipose tissue functions as a lipid store that secrets hormones/cytokines etc., may be related with disease duration |
| Soluble biomarkers | ||
| N-terminal pro B-type natriuretic peptide (NT-proBNP), homocysteine, sCD40L, soluble lectin-like oxidized low-density lipoprotein receptor-1 (sLOX-1), leptin, high sensitivity C-reactive protein (hs-CRP), fetuin-A, cystatin-C, osteopontin, chemerin, GlycA, endocan, vascular endothelial growth factor (VEGF), YKL-40, leptin, fetuin-A, cystatin-C, psoriasin, koebnerisin | ||
| First Author, Year | Study Type | n | Intervention | Follow Up | Assessed Marker of Subclinical Atherosclerosis | Results |
|---|---|---|---|---|---|---|
| Choi et al., 2020 [77] | Prospective, cohort | 209 | Group A (n = 124): biologic therapy (anti-TNFa, anti-IL12/23, anti-IL-17) Group B (n = 85): non biologic therapy (topical, light, systemic therapy) | 1 year | Lipid-rich necrotic core assessed by CTA | -Favorable modification of lipid-rich necrotic core in patients under biologics -No significant difference between different biologic groups |
| Elnabawi et al., 2019 [24] | Prospective, cohort | 134 | Group A (n = 82): anti-TNFα, anti-IL-12/23, anti-IL17) Group B (n = 52): non biologic therapy (topical, light therapy) | 1 year | Perivascular fat attenuation index assessed by coronary CTA | -Significant decrease in median fat attenuation index only in biologic group -Similar changes between different biologic groups |
| Elnabawi et al., 2019 [78] | Prospective, cohort | 121 | Group A (n = 89): biologic therapy (anti-TNFa, anti-IL-12/23, anti-IL-17) Group B (n = 32): non biologic therapy (topical/light therapy) | 1 year | Coronary plaque burden and plaque subcomponents (calcified vs. non-calcified) assessed by coronary CTA | Favorable modulation of coronary plaque indices |
| Gelfand et al., 2020 (VIP-S) [79] | RCT | 91 | 12-week period [Secukinumab (n = 46) vs. placebo (n = 45)] followed by a 40-week period [secukinumab (n = 86)] | 1 year | Aortic vascular inflammation assessed by FDG-PET/CT | Non-statistically significant −0.75% reduction in target-to-blood at week 12 and at week 52 |
| Makavos et al., 2020 [80] | Prospective, cohort | 150 | Secukinumab (n = 50) vs. cyclosporine (n = 50) vs. methotrexate (n = 50) | 1 year | GLS, GLSR, GLSRE, LVtwist and untwisting, CFR, PWV, MDA, PC | Greater improvement of all markers in secukinumab group |
| Marovt et al., 2020 [81] | Prospective, cohort | 15 | Ustekinumab (n = 4) vs. secukinumab (n = 10) vs. ixekizumab (n = 1) | 6 months | PWV, IMT | No significant changes in all groups |
| Piros et al., 2021 [82] | Prospective, cohort | 31 | Secukinumab (n = 20) vs. ixekizumab (n = 11) | 6 months | IMT | Significant reduction of IMT |
| von Stebut et al., 2019 (CARIMA) [83] | RCT | 151 | Secukinumab 300 mg for 52 weeks (n = 48) vs. secukinumab 150 mg for 52 weeks (n = 54) vs. placebo for 12 weeks followed by secukinumab 300 mg for 40 weeks (n = 26) vs. placebo for 12 weeks followed by secukinumab 150 mg for 40 weeks (n = 23) | 1 year | FMD | Non-significant difference in FMD until week 12; significantly improved FMD in patients receiving secukinumab 300 mg for 52 weeks |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsiogka, A.; Gregoriou, S.; Stratigos, A.; Soulaidopoulos, S.; Rompoti, N.; Panagakis, P.; Papoutsaki, M.; Kostakis, P.; Kontochristopoulos, G.; Tsioufis, K.; et al. The Impact of Treatment with IL-17/IL-23 Inhibitors on Subclinical Atherosclerosis in Patients with Plaque Psoriasis and/or Psoriatic Arthritis: A Systematic Review. Biomedicines 2023, 11, 318. https://doi.org/10.3390/biomedicines11020318
Tsiogka A, Gregoriou S, Stratigos A, Soulaidopoulos S, Rompoti N, Panagakis P, Papoutsaki M, Kostakis P, Kontochristopoulos G, Tsioufis K, et al. The Impact of Treatment with IL-17/IL-23 Inhibitors on Subclinical Atherosclerosis in Patients with Plaque Psoriasis and/or Psoriatic Arthritis: A Systematic Review. Biomedicines. 2023; 11(2):318. https://doi.org/10.3390/biomedicines11020318
Chicago/Turabian StyleTsiogka, Aikaterini, Stamatios Gregoriou, Alexander Stratigos, Stergios Soulaidopoulos, Natalia Rompoti, Pantelis Panagakis, Marina Papoutsaki, Panagiotis Kostakis, George Kontochristopoulos, Konstantinos Tsioufis, and et al. 2023. "The Impact of Treatment with IL-17/IL-23 Inhibitors on Subclinical Atherosclerosis in Patients with Plaque Psoriasis and/or Psoriatic Arthritis: A Systematic Review" Biomedicines 11, no. 2: 318. https://doi.org/10.3390/biomedicines11020318
APA StyleTsiogka, A., Gregoriou, S., Stratigos, A., Soulaidopoulos, S., Rompoti, N., Panagakis, P., Papoutsaki, M., Kostakis, P., Kontochristopoulos, G., Tsioufis, K., Campanati, A., Offidani, A., Vlachopoulos, C., & Rigopoulos, D. (2023). The Impact of Treatment with IL-17/IL-23 Inhibitors on Subclinical Atherosclerosis in Patients with Plaque Psoriasis and/or Psoriatic Arthritis: A Systematic Review. Biomedicines, 11(2), 318. https://doi.org/10.3390/biomedicines11020318