
Leucine-Rich Alpha-2-Glycoprotein: A Novel Predictor of Diastolic Dysfunction


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Recruitment and Sample Collection
2.2. Angiographic and Echocardiographic Assessment
2.3. Other Measurements
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics and Clinical Characteristics
3.2. Regression Model Analysis of LRG1 for Diastolic Dysfunction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart. J. 2016, 37, 2129–2200. [Google Scholar]
- Paulus, W.J.; Tschöpe, C.; Sanderson, J.E.; Rusconi, C.; Flachskampf, F.A.; Rademakers, F.E.; Marino, P.; Smiseth, O.A.; De Keulenaer, G.; Leite-Moreira, A.; et al. How to diagnose diastolic heart failure: A consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur. Heart J. 2007, 28, 2539–2550. [Google Scholar] [CrossRef] [Green Version]
- Burlew, B.S.; Weber, K.T. Cardiac Fibrosis as a Cause of Diastolic Dysfunction. Herz 2002, 27, 92–98. [Google Scholar] [CrossRef]
- Schellings, M.W.; Pinto, Y.M.; Heymans, S. Matricellular proteins in the heart: Possible role during stress and re-modeling. Cardiovasc. Res. 2004, 64, 24–31. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Song, D.; Dong, J.; Zhu, P.; Liu, J.; Liu, W.; Ma, X.; Zhao, L.; Ling, S. Current Understanding of the Pathophysiology of Myocardial Fibrosis and Its Quantitative Assessment in Heart Failure. Front. Physiol. 2017, 8, 238. [Google Scholar] [CrossRef]
- Jamiel, A.; Ahmed, A.M.; Farah, I.; Al-Mallah, M.H. Correlation between diastolic dysfunction and coronary artery disease on coronary computed tomography angiography. Heart Views 2016, 17, 13–18. [Google Scholar] [CrossRef]
- Pellicori, P.; Ferreira, J.P.; Mariottoni, B.; Rocca, H.B.; Ahmed, F.Z.; Verdonschot, J.; Collier, T.; Cuthbert, J.J.; Petutschnigg, J.; Mujaj, B.; et al. Effects of spironolactone on serum markers of fibrosis in people at high risk of developing heart failure: Rationale, design and baseline characteristics of a proof-of-concept, randomised, precision-medicine, prevention trial. The Heart OMics in AGing (HOMAGE) trial. Eur. J. Heary Fail. 2020, 22, 1711–1723. [Google Scholar]
- Song, W.; Wang, X. The role of TGFβ1 and LRG1 in cardiac remodelling and heart failure. Biophys. Rev. 2015, 7, 91–104. [Google Scholar] [CrossRef] [Green Version]
- Gao, W.; Wu, R.; Yin, J.; Ma, Y.; Guo, J.; Zhong, X.; Huang, D.; Ge, J. Expression and predictive value of leucine rich α-2 glycoprotein in ischemic heart disease. ResearchSquare 2020, preprint. [Google Scholar]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef]
- Galderisi, M.; Cosyns, B.; Edvardsen, T.; Cardim, N.; Delgado, V.; Di Salvo, G.; Donal, E.; Sade, L.E.; Ernande, L.; Garbi, M.; et al. Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: An expert consensus document of the European association of cardiovascular imaging. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1301–1310. [Google Scholar]
- Greenland, P.; Alpert, J.S.; Beller, G.A.; Benjamin, E.J.; Budoff, M.J.; Fayad, Z.A.; Foster, E.; Hlatky, M.A.; Hodgson, J.M.; Kushner, F.G.; et al. 2010 ACCF/AHA Guideline for Assessment of Cardiovascular Risk in Asymptomatic Adults: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2010, 56, e50–e103. [Google Scholar] [CrossRef] [Green Version]
- Lam, C.S.; Lyass, A.; Kraigher-Krainer, E.; Massaro, J.M.; Lee, D.S.; Ho, J.E.; Levy, D.; Redfield, M.M.; Pieske, B.M.; Benjamin, E.J.; et al. Cardiac Dysfunction and Noncardiac Dysfunction as Precursors of Heart Failure With Reduced and Preserved Ejection Fraction in the Community. Circulation 2011, 124, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, H.R.; Axel, L.; Hochman, J.S. Diastolic Dysfunction in Patients With Ischemic Symptoms Without Ob-structive Coronary Artery Disease. Circ. Cardiovasc. Imaging 2014, 7, 420–421. [Google Scholar] [CrossRef] [Green Version]
- Michelsen, M.M.; Pena, A.; Mygind, N.D.; Høst, N.; Gustafsson, I.; Hansen, P.R.; Hansen, H.S.; Kastrup, J.; Prescott, E. Overlap between angina without obstructive coronary artery disease and left ventricular di-astolic dysfunction with preserved ejection fraction. PLoS ONE 2019, 14, e0216240. [Google Scholar] [CrossRef]
- Vasan, R.S.; Xanthakis, V.; Lyass, A.; Andersson, C.; Tsao, C.; Cheng, S.; Aragam, J.; Benjamin, E.J.; Larson, M.G. Epidemiology of Left Ventricular Systolic Dysfunction and Heart Failure in the Framingham Study: An Echocardiographic Study Over 3 Decades. JACC Cardiovasc. Imaging 2018, 11, 1–11. [Google Scholar] [CrossRef]
- Reddy, Y.N.V.; Carter, R.E.; Obokata, M.; Redfield, M.M.; Borlaug, B.A. A Simple, Evidence-Based Approach to Help Guide Diagnosis of Heart Failure With Preserved Ejection Fraction. Circulation 2018, 138, 861–870. [Google Scholar] [CrossRef]
- Paulus, W.J. H(2)FPEF Score: At Last, a Properly Validated Diagnostic Algorithm for Heart Failure With Preserved Ejection Fraction. Circulation 2018, 138, 871–873. [Google Scholar] [CrossRef]
- Anjan, V.Y.; Loftus, T.M.; Burke, M.A.; Akhter, N.; Fonarow, G.C.; Gheorghiade, M.; Shah, S.J. Prevalence, Clinical Phenotype, and Outcomes Associated With Normal B-Type Natriuretic Peptide Levels in Heart Failure With Preserved Ejection Fraction. Am. J. Cardiol. 2012, 110, 870–876. [Google Scholar] [CrossRef] [Green Version]
- Obokata, M.; Borlaug, B.A. Role of Diastolic Stress Testing in the Evaluation for Heart Failure With Preserved Ejection Fraction: A Simultaneous Invasive-Echocardiographic Study. Circulation 2017, 135, 825–838. [Google Scholar] [CrossRef] [Green Version]
- Paulus, W.J.; Tschöpe, C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J. Am. Coll. Cardiol. 2013, 62, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Amende, I.; Coltart, D.J.; Krayenbuehl, H.P.; Rutishauser, W. Left ventricular contraction and relaxation in patients with coronary heart disease. Eur. J. Cardiol. 1975, 3, 37–45. [Google Scholar]
- Reduto, L.A.; Wickemeyer, W.J.; Young, J.B.; Del Ventura, L.A.; Reid, J.W.; Glaeser, D.H.; Quiñones, M.A.; Miller, R.R. Left ventricular diastolic performance at rest and during exercise in patients with coronary artery disease. Assessment with first-pass radionuclide angiography. Circulation 1981, 63, 1228–1237. [Google Scholar] [CrossRef] [Green Version]
- Mehta, S.K.; Rame, J.E.; Khera, A.; Murphy, S.A.; Canham, R.M.; Peshock, R.M.; de Lemos, J.A.; Drazner, M.H. Left ventricular hypertrophy, subclinical atherosclerosis, and inflammation. Hypertension 2007, 49, 1385–1391. [Google Scholar] [CrossRef] [Green Version]
- Lin, F.Y.; Zemedkun, M.; Dunning, A.; Gomez, M.; Labounty, T.M.; Asim, M.; Horn, E.; Aurigemma, G.; Maurer, M.S.; Roman, M.; et al. Extent and severity of coronary artery disease by coronary CT angiography is associated with elevated left ventricular diastolic pressures and worsening diastolic function. J. Cardiovasc. Comput. Tomogr. 2013, 7, 289–296.e281. [Google Scholar] [CrossRef]
- Mansour, M.J.; Aljaroudi, W.; Mroueh, A.; Hamoui, O.; Honeine, W.; Khoury, N.; Abi Nassif, J.; Chammas, E. Stress-induced Worsening of Left Ventricular Diastolic Function as a Marker of Myocardial Is-chemia. J. Cardiovasc. Echogr. 2017, 27, 45–51. [Google Scholar]
- Serada, S.; Fujimoto, M.; Terabe, F.; Iijima, H.; Shinzaki, S.; Matsuzaki, S.; Ohkawara, T.; Nezu, R.; Nakajima, S.; Kobayashi, T.; et al. Serum leucine-rich alpha-2 glycoprotein is a disease activity biomarker in ulcerative colitis. Inflamm. Bowel Dis. 2012, 18, 2169–2179. [Google Scholar] [CrossRef]
- Zhang, J.; Zhu, L.; Fang, J.; Ge, Z.; Li, X. LRG1 modulates epithelial-mesenchymal transition and angiogenesis in colorectal cancer via HIF-1α activation. J. Exp. Clin. Cancer Res. 2016, 35, 29. [Google Scholar] [CrossRef] [Green Version]
- Bos, S.; Phillips, M.; Watts, G.F.; Verhoeven, A.J.; Sijbrands, E.J.; Ward, N.C. Novel protein biomarkers associated with coronary artery disease in statin-treated patients with familial hypercholesterolemia. J. Clin. Lipidol. 2017, 11, 682–693. [Google Scholar] [CrossRef]
- Feng-Jung, Y. MON-056 Leucine-Rich a-2-Glycoprotein 1 increased Peripheral arterial occlusive disease risk in end-stage renal disease. Kidney Int. Rep. 2019, 4, S327. [Google Scholar] [CrossRef]
- Yang, F.-J.; Hsieh, C.-Y.; Shu, K.-H.; Chen, I.-Y.; Pan, S.-Y.; Chuang, Y.-F.; Chiu, Y.-L.; Yang, W.-S. Plasma Leucine-Rich α-2-Glycoprotein 1 Predicts Cardiovascular Disease Risk in End-Stage Renal Disease. Sci. Rep. 2020, 10, 5988. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Abraham, S.; McKenzie, J.A.G.; Jeffs, N.; Swire, M.; Tripathi, V.B.; Luhmann, U.F.O.; Lange, C.A.K.; Zhai, Z.; Arthur, H.M.; et al. LRG1 promotes angiogenesis by modulating endothelial TGF-β signalling. Nature 2013, 499, 306–311. [Google Scholar] [CrossRef] [Green Version]
- Celik, T.; Yuksel, U.C.; Fici, F.; Celik, M.; Yaman, H.; Kilic, S.; Iyisoy, A.; Dell’Oro, R.; Grassi, G.; Yokusoglu, M.; et al. Vascular inflammation and aortic stiffness relate to early left ventricular diastolic dysfunction in pre-hypertension. Blood Press 2013, 22, 94–100. [Google Scholar] [CrossRef]
- Liu, C.; Lim, S.T.; Teo, M.H.Y.; Tan, M.S.Y.; Kulkarni, M.D.; Qiu, B.; Li, A.; Lal, S.; Dos Remedios, C.G.; Tan, N.S.; et al. Collaborative Regulation of LRG1 by TGF-β1 and PPAR-β/δ Modulates Chronic Pressure Over-load-Induced Cardiac Fibrosis. Circ. Heart Fail 2019, 12, e005962. [Google Scholar] [CrossRef]
- Watson, C.J.; Ledwidge, M.T.; Phelan, D.; Collier, P.; Byrne, J.C.; Dunn, M.J.; McDonald, K.M.; Baugh, J.A. Proteomic Analysis of Coronary Sinus Serum Reveals Leucine-Rich α2-Glycoprotein as a Novel Biomarker of Ventricular Dysfunction and Heart Failure. Circ. Heart Fail. 2011, 4, 188–197. [Google Scholar] [CrossRef] [Green Version]
- Yang, F.; Liu, Y.-H.; Yang, X.-P.; Xu, J.; Kapke, A.; Carretero, O.A. Myocardial Infarction and Cardiac Remodelling in Mice. Exp. Physiol. 2002, 87, 547–555. [Google Scholar] [CrossRef]
- Kumagai, S.; Nakayama, H.; Fujimoto, M.; Honda, H.; Serada, S.; Ishibashi-Ueda, H.; Kasai, A.; Obana, M.; Sakata, Y.; Sawa, Y.; et al. Myeloid cell-derived LRG attenuates adverse cardiac remodelling after myocardial infarction. Cardiovasc. Res. 2015, 109, 272–282. [Google Scholar] [CrossRef] [Green Version]
- Yadav, M.; Palmerini, T.; Caixeta, A.; Madhavan, M.V.; Sanidas, E.; Kirtane, A.J.; Stone, G.W.; Généreux, P. Prediction of coronary risk by SYNTAX and derived scores: Synergy between percutaneous coronary intervention with taxus and cardiac surgery. J. Am. Coll. Cardiol. 2013, 62, 1219–1230. [Google Scholar] [CrossRef] [Green Version]
- Yin, X.; Subramanian, S.; Hwang, S.J.; O’Donnell, C.J.; Fox, C.S.; Courchesne, P.; Muntendam, P.; Gordon, N.; Adourian, A.; Juhasz, P.; et al. Protein biomarkers of new-onset cardiovascular disease: Prospective study from the systems approach to biomarker research in cardiovascular disease initiative. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 939–945. [Google Scholar] [CrossRef] [Green Version]
- Lakhani, I.; Wong, M.V.; Hung, J.K.F.; Gong, M.; Bin Waleed, K.; Xia, Y.; Lee, S.; Roever, L.; Liu, T.; Tse, G.; et al. Diagnostic and prognostic value of serum C-reactive protein in heart failure with preserved ejection fraction: A systematic review and meta-analysis. Heart Fail. Rev. 2020, 26, 1141–1150. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Diastolic Function | p-Value | |
|---|---|---|---|
| No-DD (n = 47) | DD (n = 47) | ||
| Age (years) | 62.04 ± 11.35 | 63.53 ± 12.16 | 0.323 |
| Gender | |||
| Male | 27 (57.40) | 31 (66.00) | 0.396 |
| Female | 20 (42.60) | 16 (34.00) | |
| Race | |||
| Malay | 14 (29.80) | 18 (38.3) | 0.228 |
| Chinese | 21 (44.7) | 13 (27.7) | |
| Indian | 12 (25.50) | 16 (34.0) | |
| Number of coronary lesion(s) | |||
| 0 | 8 (17.00) | 4 (8.50) | <0.001 ** |
| 1 | 20 (42.60) | 3 (6.40) | |
| 2 | 11 (23.40) | 10 (21.30) | |
| 3 | 8 (17.00) | 30 (63.80) | |
| Diastolic dysfunction grading | |||
| Grade 1 | NA | 38 (80.9) | |
| Grade 2 | NA | 5 (10.6) | |
| Grade 3 | NA | 4 (8.5) | |
| LRG1 levels (ng/mL) | 8 (4) | 14 (8) | <0.001 ** |
| SYNTAX | 7 (17) | 24.5 (15) | <0.001 ** |
| Laboratory tests | |||
| Hemoglobin (g/dL) | 13.2 (1.5) | 13.3 (1.5) | 0.758 |
| Urea (mmol/L) | 5.5 (3.6) | 6.6 (3.9) | 0.037 * |
| Creatinine (mcmol/L) | 78 (28) | 90 (48) | 0.018 * |
| Risk Factors | |||
| Diabetes Mellitus | |||
| Non-diabetic | 38 (80.9) | 26 (55.3) | 0.008 ** |
| Diabetic | 9 (19.1) | 21 (44.7) | |
| Lipid Profile | |||
| Total cholesterol (mmol/L) | 4 (1.8) | 4.5 (1.3) | 0.117 |
| Triglyceride (mmol/L) | 1 (0.8) | 1.2 (0.7) | 0.604 |
| LDL (mmol/L) | 2.24 (1.33) | 3 (1.47) | 0.031 * |
| HDL (mmol/L) | 1.07 (0.5) | 1.08 (0.38) | 0.678 |
| Hyperlipidemia | |||
| No | 40 (85.10) | 37 (78.70) | 0.421 |
| Yes | 7 (14.90) | 10 (21.30) | |
| Hypertension | |||
| <140/90 mmHg | 27 (57.4) | 31 (66.0) | 0.396 |
| >140/90 mmHg | 20 (42.6) | 16 (34.0) | |
| Smoking | |||
| Non-smoker | 24 (51.10) | 27 (57.40) | 0.204 |
| Current smoker | 20 (42.60) | 20 (42.60) | |
| Ex-smoker | 3 (6.40) | 0 (0.00) | |
| Medication use | |||
| Perindopril | 27 (57.4) | 21 (44.7) | 0.216 |
| Beta Blocker | 26 (55.3) | 20 (42.6) | 0.302 |
| Frusemide | 6 (12.8) | 2 (4.3) | 0.139 |
| Spironolactone | 0 (0) | 1 (2.1) | 0.315 |
| Metformin | 9 (19.1) | 19 (40.4) | 0.024 * |
| Gliclazide | 3 (6.4) | 7 (14.9) | 0.181 |
| Insulin | 6 (12.8) | 8 (17.0) | 0.562 |
| Index | No-DD | DD | p Value | Effect Size |
|---|---|---|---|---|
| Median (IQR) | Median (IQR) | |||
| LAVI | 28 (3) | 35 (2) | <0.001 | 1.54 |
| TR velocity | 2.1 (0.4) | 2.9 (0.1) | <0.001 | 2.7 |
| Septal e′ | 7.8 (1.5) | 6.7 (1.5) | <0.001 | 1.42 |
| Lateral e′ | 12 (3.3) | 9.8 (1.1) | <0.001 | 1.33 |
| E/e′ | 12 (2) | 15 (1) | <0.001 | 1.64 |
| EF (%) | 67 (21) | 60 (14) | 0.069 | 0.8 |
| Variables | Unadjusted OR | p-Value | Adjusted OR | p-Value |
|---|---|---|---|---|
| [95% CI] | [95% CI] | |||
| LRG1 | 1.26 | <0.001 | 1.32 ** | <0.001 |
| [1.23–1.42] | [1.14–1.53] | |||
| SYNTAX | 1.1 | - | 1.08 ** | 0.007 |
| [1.06–1.16] | [1.02–1.14] | |||
| Creatinine | 1.02 | - | 1.04 ** | 0.005 |
| [1.01–1.04] | [1.01–1.06] | |||
| DM | 3.41 | - | 6.93 ** | 0.006 |
| [1.35–8.61] | [1.76–27.34] |
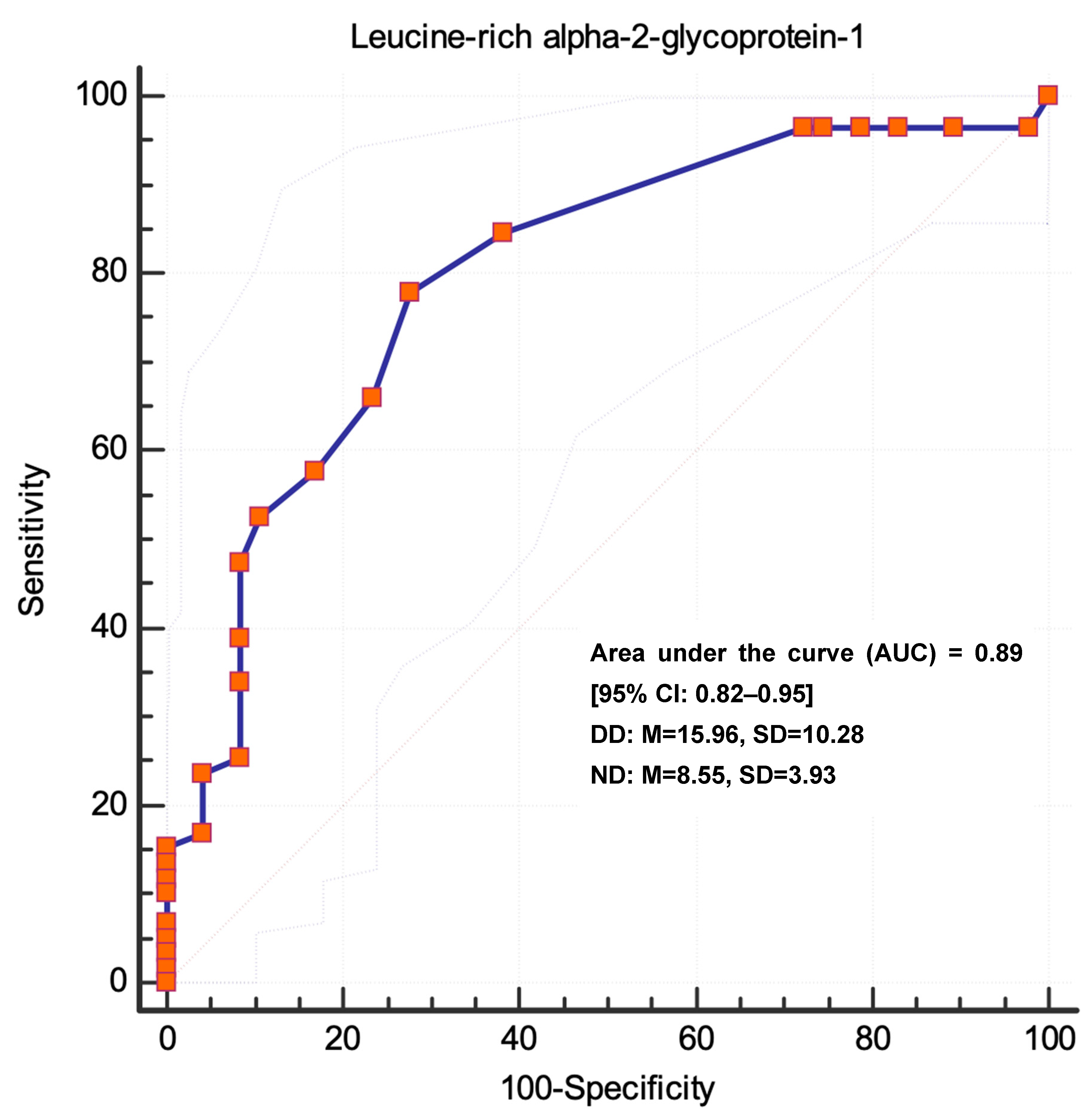
| Predictive Performance of Regression Model | Pairwise Comparison of ROC Curves | ||||
|---|---|---|---|---|---|
| Model | AUC [95% CI] | Standard Error | p-Value | z | p-Value |
| Unadjusted Model | 0.79 [0.70–0.87] | 0.04 | <0.001 *** | 2.356 | 0.0185 |
| Adjusted Model | 0.89 [0.82–0.95] | 0.03 | <0.001 *** | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loch, A.; Tan, K.L.; Danaee, M.; Idris, I.; Ng, M.L. Leucine-Rich Alpha-2-Glycoprotein: A Novel Predictor of Diastolic Dysfunction. Biomedicines 2023, 11, 944. https://doi.org/10.3390/biomedicines11030944
Loch A, Tan KL, Danaee M, Idris I, Ng ML. Leucine-Rich Alpha-2-Glycoprotein: A Novel Predictor of Diastolic Dysfunction. Biomedicines. 2023; 11(3):944. https://doi.org/10.3390/biomedicines11030944
Chicago/Turabian StyleLoch, Alexander, Kok Leng Tan, Mahmoud Danaee, Iskandar Idris, and Mei Li Ng. 2023. "Leucine-Rich Alpha-2-Glycoprotein: A Novel Predictor of Diastolic Dysfunction" Biomedicines 11, no. 3: 944. https://doi.org/10.3390/biomedicines11030944
APA StyleLoch, A., Tan, K. L., Danaee, M., Idris, I., & Ng, M. L. (2023). Leucine-Rich Alpha-2-Glycoprotein: A Novel Predictor of Diastolic Dysfunction. Biomedicines, 11(3), 944. https://doi.org/10.3390/biomedicines11030944